Embed Size (px)
Citation preview
Isolation & Quarantine FacilitiesAssessment & Recommendations
Assessment Process
Literature Review CD I&Q Definitions WA Administrative Code (WAC) Individual I&Q Conditions
and Principles Potential Disease Agent Characteristics – CDC CDC Infection Control and I&Q Guidance
Interviews Preparedness, CHS, CD-EPI, CBPH, Contracts, Risk
Communications Staffs Research and Review Facility Options Analyze Facility Pros and Cons Develop Recommendations
I&Q Facilities Parameters
Preliminary Objective: Find 300 rooms 100 in each King County Emergency Coordination Zone
Plan for Individual Level I&Q NOT Community Level
Disease Agents Considered: Executive Order 13295 Quarantinable Diseases
AND CDC Category A Bioterrorism Threats
OR Diseases with Potential for Pandemic Spread
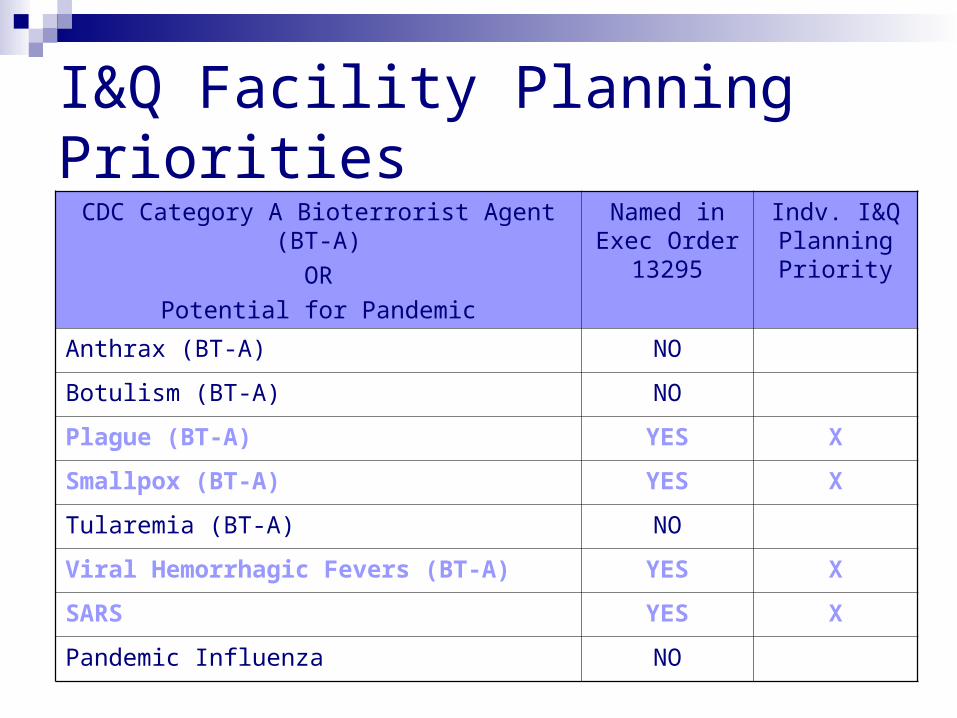
I&Q Facility Planning PrioritiesCDC Category A Bioterrorist Agent (BT-A)
OR Potential for Pandemic
Named in Exec Order
13295
Indv. I&Q Planning Priority
Anthrax (BT-A) NO
Botulism (BT-A) NO
Plague (BT-A) YES X
Smallpox (BT-A) YES X
Tularemia (BT-A) NO
Viral Hemorrhagic Fevers (BT-A) YES X
SARS YES X
Pandemic Influenza NO
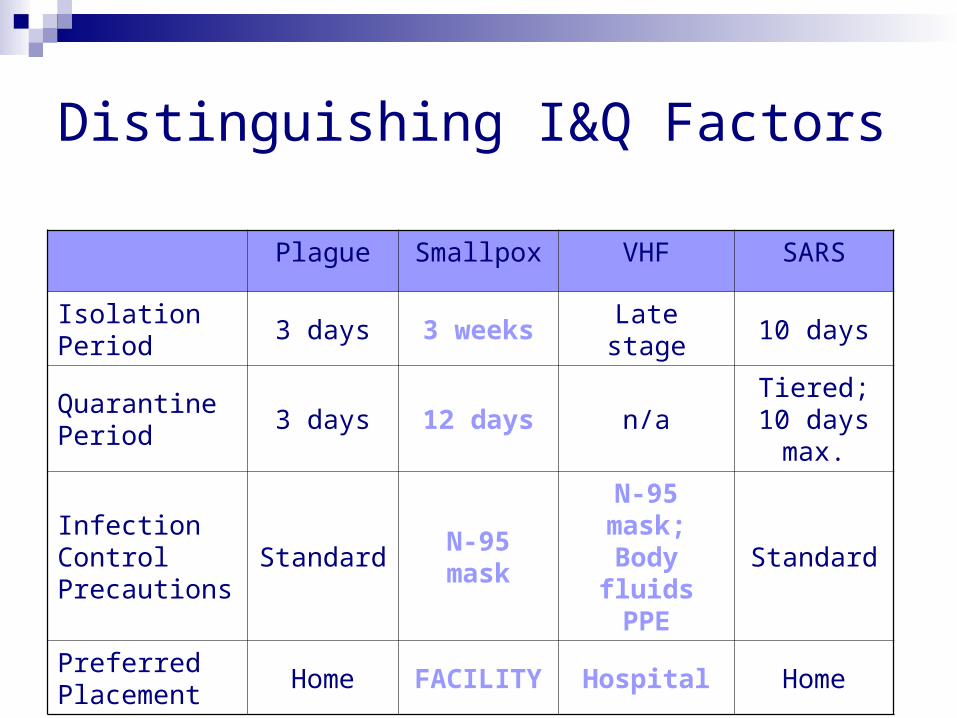
Distinguishing I&Q Factors
Plague Smallpox VHF SARS
Isolation Period
3 days 3 weeks Late stage 10 days
Quarantine Period
3 days 12 days n/aTiered; 10 days max.
Infection Control Precautions
StandardN-95 mask
N-95 mask; Body
fluids PPE
Standard
Preferred Placement
Home FACILITY Hospital Home

I&Q Facilities Considerations Separate rooms/wings ideal; wards OK in large events Adherence to standard and airborne precautions Adequate water, electricity, heating, cooling, ventilation Maintain a clean and quality facility Easy to coordinate and deliver services (accessibility) Attend to physical, emotional, mental, spiritual needs
communications, comfort, entertainment, acceptability I&Q periods could be as long as 3 weeks
comfortable, functional, securable Compatible with Community Level Quarantine measures
e.g. limit the movement of people; social isolation
A Note on Effectiveness
Quarantine need not be 100% complete to be effective
Voluntary Quarantine is our desired outcome Involuntary Quarantine is resource intensive
Maximum utilization of scarce CD-EPI and/or IQRC resources Law Enforcement and Court System Involvement Requires a More Secure Facility
Recommendations are biased in favor of “publicly acceptable” facilities Motels or similar familiar and comfortable home-like
environments In large events, clean temporary structures vs.
deteriorated structures
I&Q Facility Options Considered Public Facilities “Mothballed” Public Facilities Existing Structures:
Community health centers, nursing homes, treatment centers, apartments, schools, dormitories, hotels
Temporary Structures: Trailers, modular units, barracks, tents, bubble systems,
field hospitals, RVs, youth camps, fire fighter shelters Emergency Declaration of Dedicated Facility:
Hospital, separate hospital building, hotel
Motel Option
Certain motels best address CDC guidance Separate rooms and restrooms Independent air circulation
Allows for client privacy and self-sufficiency Significant factor in long-term periods
Currently used for TB isolation
PRO: High chance for acceptability CON: Post-event stigma of site
HHS – Contingency Stations
Placed inside existing structure
Modular: 50 bed units, up to 250 per station
Includes beds and supplies Available through SNS
4 hours for quarantine (plane) 12 hours for mass care
PRO: Eliminates need for local supply stocking/storage CON: Potential for Post-Event Stigmatization of host
facility
Alaska Structures Tents
Medical Shelter is 650 square feet Erected in 30 minutes or less Soft wall, aluminum frame Modular, expandable Positive pressure ventilation Able to isolate between shelters and
hallways
PRO: Could accommodate HHS-CS option CON: water, electrical hook-up needed; may
require pre-purchase of tent
Sprung Tents
Quickly assembled 30 ft to 300 ft long 30 year guarantee Large, open space Can be placed on any flat surface
PRO: Could accommodate HHS-CS
CON: water, electrical hook-up needed; may require pre-purchase of tent
Mobile Field Hospital Option
Large scale solution May be able to secure one
from military State of Connecticut Model
Serves as alternate hospital facility
PRO: Could accommodate HHS-CS option CON: purchase, storage, site, water,
electrical hook-up are all needed
Pros for Each Option
Motel: High chance for public acceptance Best meets CDC criteria
HHS – CS: Large scale, flexible Eliminates need for local purchase and storage
of supplies Field Hospital:
Large scale, flexible Acute care is possible
Cons for Each Option
Motel: Public stigmatization after event major concern
HHS – CS: Public stigmatization of host facility Common ventilation system, no privacy
Field Hospital: Stocking and staffing - expensive Common ventilation system, no privacy
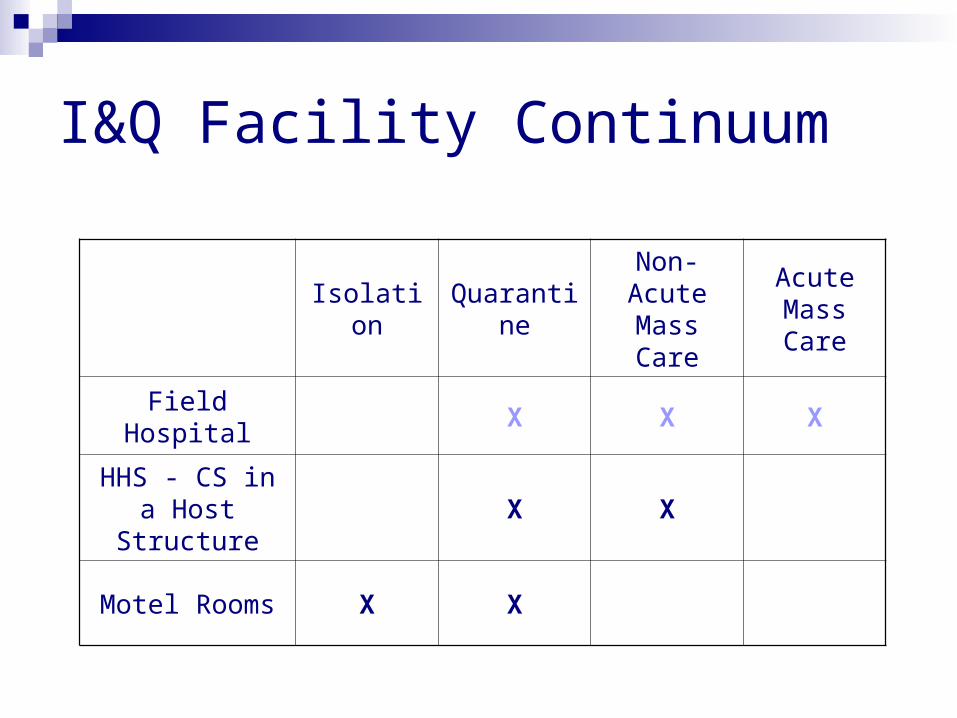
I&Q Facility Continuum
IsolationQuaranti
ne
Non-Acute Mass Care
Acute Mass Care
Field Hospital X X X
HHS - CS in a Host Structure
X X
Motel Rooms X X
I&Q Facility RecommendationsDevelop a Continuum of Options: Partner with Motels (TB Model) Accommodate HHS – Contingency Stations
Temporary Tents Emergency Declaration of “Designated
Facility” Hospital Wing Hotel
Action Steps
Secure motel agreements (1 underway) Secure HHS-CS accommodation facility
agreements Prepare a list of potential “Designated Facility”
options Develop an Operational Plans
Site specific as secured Generic to be used at any site designated in the event





























