Embed Size (px)
Citation preview
Cancer Genetics and Cytogenetics 137 (2002) 146–149
0165-4608/02/$ – see front matter © 2002 Elsevier Science Inc. All rights reserved.PII: S0165-4608(02)00559-9
Isolated cardiac recurrence of acute lymphoblastic leukemia characterized by t(11;19) two years after unrelated allogeneic bone marrow transplantation
Tonya L. Wright
a
, Peter G. Bardy
a
, Patrick Disney
b
, Sarah Moore
c
, Noemi Horvath
a,c,
*
a
Department of Hematology, Royal Adelaide Hospital, Adelaide, Australia
b
Department of Cardiology, Royal Adelaide Hospital, Adelaide, Australia
c
SA Cancer Cytogenetics Unit, Institute of Medical and Veterinary Science, Adelaide, Australia
Received 31 December 2001; received in revised form 21 February 2002; accepted 22 February 2002
Abstract
A 33-year-old male presented with acute lymphoblastic leukemia (ALL) characterized by translocation(11;19)(q23;p13.3). He received an allogeneic bone marrow transplant from a matched unrelated donor.Two years later his disease relapsed with an isolated intracardiac mass, presenting as right heart failure.He had no evidence of concomitant relapse in the bone marrow. Tumor cytogenetics revealed clonal evo-lution with the karyotype 46,XY,t(3;16)(q23;p13),t(11;19)(q23;p13.3), the chromosome 16 breakpoint in-volving the band where the genes for multidrug resistance-associated protein and CREB binding proteinare known to reside. To our knowledge, this is the first report of an isolated extramedullary relapse of
ALL in the heart. © 2002 Elsevier Science Inc. All rights reserved.
1. Introduction
The translocation (11;19) seen in this patient has been re-ported to result in
MLL-ENL
gene fusion and is generallyassociated with a poor outcome [1]. Most patients with thisvariety of genetic lesion have M4 or M5 acute myeloid leu-kemia, c-acute lymphoblastic leukemia (ALL), pro-B ALL,or pre-B ALL. A smaller number are shown to have T-ALL,and it appears, from the relatively small number of patientsstudied, that this group has a good response to therapy withlong first remissions and better survival [1,2].
For those patients who do not achieve complete remis-sion, however, allogeneic bone marrow transplantation (BMT)may still provide a curative option, although a significantpercentage of adults with ALL relapse following BMT. Re-lapse at an extramedullary site with sparing of the marrow isunusual. We report a patient with an isolated cardiac recur-rence of ALL presenting as right heart failure, 2 years aftertransplant. The heart has not previously been reported in theliterature as a site of extramedullary relapse, and the mecha-nism underlying selection of this site remains unknown. Cy-togenetic analysis of our patient’s tumor revealed the t(11;19)
(q23;p13.3) and clonal evolution with a second transloca-tion not previously reported in ALL. The contribution ofthis aberration to the pattern of relapse is unknown. The op-timal treatment of isolated extramedullary relapse remainscontroversial.
2. Case report
A 33-year-old caucasian male presented in September1998 with cervical lymphadenopathy and leukocytosis. Histotal white cell count was 173
�
10
9
/L, with 86% circulatingblasts. Bone marrow biopsy diagnosed early T precursorALL, L2 in the French–American–British classification.Cytogenetic analysis revealed the t(11;19)(q23;p13.3) andflow cytometry demonstrated the T cell phenotype (CD3
�
,CD4
�
, CD5
�
, CD7
�
, CD8
�
, CD34
�
). He was treated withleukapheresis before commencing chemotherapy accordingto the LaLa94 protocol (unpublished observations). Sinceonly a partial remission was achieved with induction che-motherapy, he was not a suitable candidate for autologousBMT. He subsequently received a matched unrelated donorBMT in December 1998. The conditioning regimen con-sisted of cyclophosphamide (total 120 mg/kg in 2 doses)and total body irradiation (13.2Gy in 8 fractions). Cy-closporin and methotrexate were given for graft-versus-hostdisease (GVHD) prophylaxis. Transplantation was compli-cated by grade 2 skin GVHD, confirmed by skin biopsy.Bone marrow biopsy 31 days after transplant confirmed tri-
* Corresponding author. SA Cancer Cytogenetics Unit, Institute ofMedical & Veterinary Science, Division of Hematology, PO Box 14, Run-dle Mall, Adelaide 5000, Australia. Tel.:
�
61-8-8222-3550; fax:
�
61-8-8222- 3162.
E-mail address
: [email protected] (N. Horvath).

T.L. Wright et al. / Cancer Genetics and Cytogenetics 137 (2002) 146–149
147
lineage engraftment and normal karyotype. He remainedwell for 22 months.
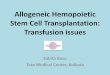
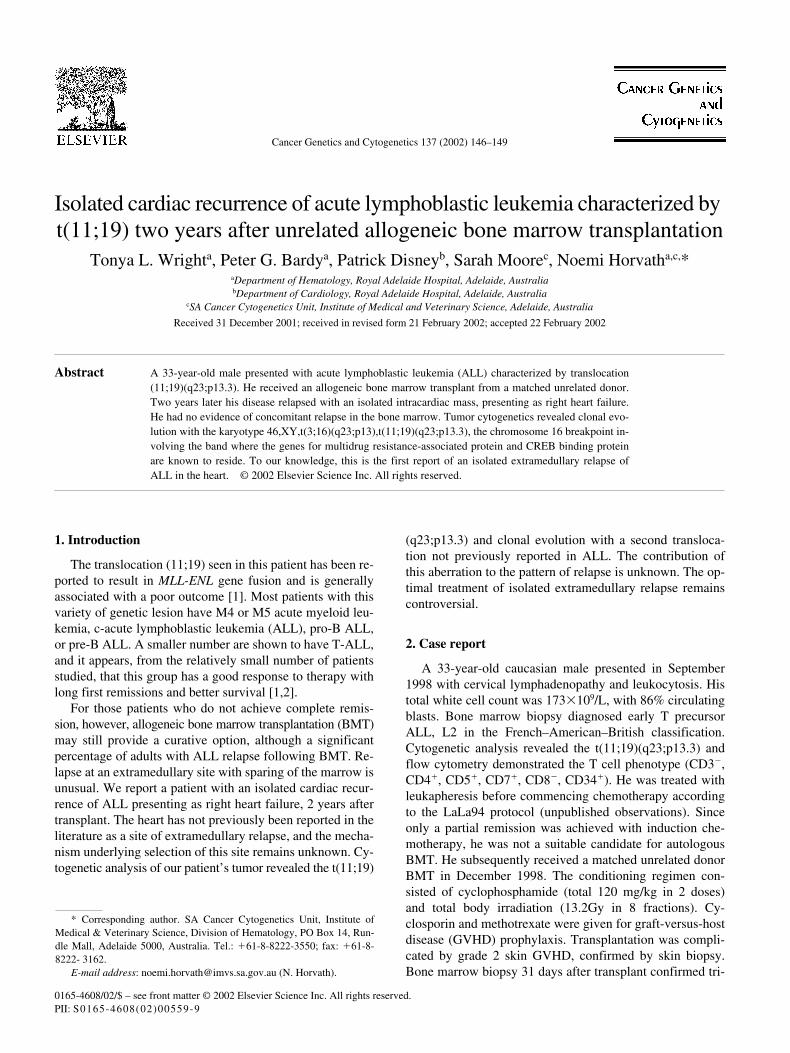
In October 2000, he was admitted to a Surgical Unit forinvestigation of abdominal pain. Laparotomy was normalapart from a small amount of ascites. Analysis of the asciticfluid revealed a high neutrophil count but no bacterialgrowth, suggesting spontaneous bacterial peritonitis par-tially treated by pre-operative antibiotics. Following surgeryhe developed ascites and marked peripheral edema. Clinicalexamination revealed an elevated JVP and a faint cardiacmurmur. Right heart failure was suspected. Echocardio-graphy revealed a large tumor in the right atrium arisingfrom the interatrial septum, and obstructing the tricuspidvalve (Fig. 1). Cardiac surgery was performed, however,complete excision was not possible due to deep invasion ofthe septum. Histology of the tumor was consistent with re-lapsed T cell ALL. Cytogenetic analysis of the tumor re-vealed clonal evolution, with the presence of the t(11;19)and an additional t(3;16)(q23;p13) (Fig. 2). There was noevidence of bone marrow relapse on morphologic or lym-phocyte surface marker examination. Cytogenetic analysisof the bone marrow revealed the normal karyotype. Imagingdid not reveal any other sites of disease relapse. Radiother-apy to the heart was commenced, and was well tolerated.Systemic treatment was not given due to his poor perfor-mance status. He remains well and free of hematopoietic re-lapse at 14 months.
3. Discussion
Leukemic relapse can present as either hematopoietic(involving bone marrow and peripheral blood), or ex-tramedullary (involving other sites) [3]. Extramedullary re-lapse of ALL in adults after allogeneic BMT rarely occurswithout concomitant hematopoietic relapse [4]. The centralnervous system and testes, so called sanctuary sites, are thepredominant sites of isolated extramedullary disease. Only afew reports have documented relapse at other isolated sites,including liver and uterus, pancreas and retroperitoneum,pericardium and mediastinum, breast, lung, pleura, boneand soft tissue, intestine, nasopharynx, sinus, skin, ovary,eye and kidney [3–10].
No reports to our knowledge have documented an intra-cardiac mass as an isolated extramedullary recurrence.Savasan et al. [6] reported pericardial relapse with infiltra-tion of myocardium and mediastinum. In this case, relapseoccurred at the initial site of bulky disease, and was attrib-uted to failure of local eradication. In our patient the mecha-nism of relapse is unclear. Cardiac involvement was not ap-parent at diagnosis, and there was no prior history of cardiacabnormality. It would seem unlikely for the heart to act as asanctuary site, as exposure to chemotherapeutic agents ishigh. It has been previously suggested that the graft-versus-leukemia (GVL) effect may be stronger in the marrow thanin peripheral tissues, preferentially allowing extramedullary
Fig. 1. Transthoracic echocardiogram (short axis parasternal view) demonstrating ALL tumor mass (MASS) arising from inter-atrial septum (IAS) and occu-pying most of the right atrium (RA). Real time echocardiography showed interference with tricuspid valve (TV) function. LA: left atrium.

148
T.L. Wright et al. / Cancer Genetics and Cytogenetics 137 (2002) 146–149
relapse [10]. This differential GVL effect may be due to alack of effector cells or cytokines capable of inducing thisbeneficial response in peripheral tissue [4]. The extent ofGVL effect from allogeneic BMT correlates with the degreeof GVHD. GVHD is not commonly reported in the myocar-dium, hence the heart may be a relative haven from the ac-tions of donor T lymphocytes. If this is the case, cardiac re-lapse should occur much more frequently.
An alternative mechanism for extramedullary relapsemay be the development of a second leukemic clone, de-rived from either recipient or donor cells. Leukemic re-lapses from donor cell origin are rare, and most have oc-curred late after BMT, and have been attributed to totalbody irradiation [11]. In our patient, persistence of the ini-tial t(11;19) (q23;p13.3) suggests recurrence of the originalrecipient malignant clone.
Cytogenetic analysis of our patient’s cardiac tumor re-vealed clonal evolution with the emergence of a new t(3;16)(q23;p13). Whether the conditioning chemoradiotherapycontributes to further genetic mutation, as previously sug-gested, is uncertain [12]. Secondary chromosomal abnor-malities in acute leukemias are not uncommon and appear tobe nonrandom. This may suggest that they are responsiblefor important phenotypic features of the tumor cell popula-tion and promote drug resistance or disease progression [13].Interestingly, 16p13 is the site of the multidrug resistance-associated protein gene (MRP) and of the CREB bindingprotein gene. Translocation of the former gene could resultin up-regulation of its expression and hence protect the
evolved clone from chemotherapy [14]. Translocation of thelatter gene has previously been observed in hematologicneoplasms [15,16], some of which are secondary to chemo-therapy [16]. It is still unclear as to why the myocardiumwas selected as the site of relapse, though it is conceivablethat the secondary translocation in our patient has played arole in its selection.
The optimal management of isolated extramedullary re-currence is still debated. Generally, treatment consists of lo-cal radiotherapy and/or chemotherapy [7,10]. Our patientwas treated with radiotherapy alone, because of poor perfor-mance status. Chemotherapy remains a future option, assystemic relapse eventually occurs in most patients. Otheroptions with variable success rates include salvage BMTand donor lymphocyte infusion [10–12,17]. Predictive fac-tors for successful treatment of relapse after BMT are longinterval between transplant and relapse, and isolated ex-tramedullary disease [12]. While clonal evolution appears tobe associated with shorter overall survival, it does not pre-dict for shorter duration from relapse to death [18].
References
[1] Moorman AV, Hagermeijer A, Charrin C, Rieder H. Secker-WalkerLM. The translocations t(11;19)(q23;p13.1) and t(11;19)(q23;p13.3):a cytogenetic and clinical profile of 53 patients. Leukemia 1998;12:805–10.
[2] Huret JL, Brizard A, Slater R, Charrin C, Bertheas MF, Guilhot F,Hahlen K, Kroes W, van Leeuwen E, Schoot EV, Tanzer J, Hage-meijer A. Cytogenetic heterogeneity in t(11;19) acute leukemia: clin-
Fig. 2. Tumor karyotype at extramedullary relapse of ALL: 46,XY,t(3;16)(q23;p13),t(11;19)(q23;p13.3). Thick arrows indicate the derivative chromosomesfrom the t(11;19), while thin arrows indicate the chromosomes involved in the t(3;16).

T.L. Wright et al. / Cancer Genetics and Cytogenetics 137 (2002) 146–149
149
ical, hematological and cytogenetic analyses of 48 patients—updatedpublished cases and 16 new observations. Leukemia 1993;7:152–60.
[3] Cormier MG, Armin A, Daneshgari F, Castelli M. Unusual extramed-ullary relapse of acute lymphoblastic leukaemia in a bone marrowtransplant patient. J Surg Onc 1987;36:290–4.
[4] Au WY, Lie AKW, Liang R, Kwong YL. Isolated extramedullary re-lapse of acute lymphoblastic leukaemia after allogeneic bone marrowtransplantation. Bone Marrow Transplant 1999;24:1137–40.
[5] Facon T, Jouet JP, Fenaux P, Walter MP, Lai JL, Jabinet JL, Cham-bon JP, Bauters F. Isolated pericardial and mediastinal relapse fol-lowing allogeneic bone marrow transplantation for acute lymphoblas-tic leukaemia. Transplantation 1991;51:1125–6.
[6] Savasan S, Abella E, Karanes C, Ravindranath Y. Recurrent breastrelapses in a patient with acute lymphoblastic leukaemia following al-logeneic bone marrow transplantation. Acta Haematol 1998;99:95–7.
[7] Ueda S, Kanamori H, Sasaki S, Yamazaki E, Tamura T, MatsuzakiM, Motomura S, Mohri H, Okubo T. Isolated extramedullary relapsein a knee joint after allogeneic bone marrow transplantation for PhALL. Bone Marrow Transplant 1998;21:319–21.
[8] Lee KH, Lee JH, Kim S, Lee JS, Kim SH, Kim WK. High frequencyof extramedullary relapse of acute leukaemia after allogeneic bonemarrow transplantation. Bone Marrow Transplant 2000;26:147–52.
[9] Hinkle AS, Dinndorf PA, Bulas DI, Kapur S. Relapse of acute lym-phoblastic leukaemia in the inferior rectus muscle of the eye. Cancer1994;73:1757–60.
[10] Chong G, Byrnes G, Szer J, Grigg A. Extramedullary relapse after al-logeneic bone marrow transplantation for haematological malignancy.Bone Marrow Transplant 2000;26:1011–15.
[11] Giralt SA, Champlin RE. Leukaemia relapse after allogeneic bonemarrow transplantation: a review. Blood 1994;84:3603–12.
[12] Frassoni F, Barrett AJ, Granena A, Ernst P, Garthon G, Kolb HJ,Prentice HG, Vernant JP, Zwaan FE, Gratwohl A. Relapse after allo-geneic bone marrow transplantation for acute leukaemia: a survey bythe EBMT of 117 cases. Br J Haem 1986;70:317–20.
[13] Johansson B, Mertens F, Mitelman F. Secondary chromosomal ab-normalities in acute leukaemias. Leukemia 1996;8:953–62.
[14] Viguié F. MRP (multidrug resistance-associated protein). Atlas GenetCytogenet Oncol Haematol. 1998. Available at: http://infobiogen.fr/services/chromcancer/Genes/MRPID106.html. Assessed December2001.
[15] Borrow J, Stanton VP Jr, Andresen JM, Becher R, Behm FG, ChaantiRS, Civiv CI, Disteche C, Dube I, Frschauf AM, Horsman D, MitelmanF, Volinia S, Watmore AE, Housman DE. The translocation t(8;16)(p11;p13) of acute myeloid leukaemia fuses a putative acetyltrans-ferase to the CREB-binding protein. Nat Genet 1996;14:34.
[16] Rowley JD, Reshmi S, Sobulo O, Musvee T, Anastasi R, Raimondi S,Schneider NR, Barredo JC, Cantu ES, Schlegelgerger B, Behm F,Doggett NA, Borrow J, Zelenik-Le N. All patients with the t(11;16)(q23;p13.3) that involves MLL and CBP have treatment-related he-matologic disorders. Blood 1997;90:535–41.
[17] Au WY, Kwong YL, Lie AK, Ma SK, Liang R. Extramedullary re-lapse of leukaemia following allogeneic bone marrow transplanta-tion. Hematol Oncol 1999;17:45–52.
[18] Chucrallah AE, Stass SA, Huh YO, Albitar M, Kantarjian HM. Adultacute lymphoblastic leukaemia at relapse-cytogenetic, immunophe-notypic and molecular changes. Cancer 1995;76:985–991.