Embed Size (px)
Citation preview

IS ETHNICITY AN INDEPENDENT PREDICTOR OF PROSTATE CANCERRECURRENCE AFTER RADICAL PROSTATECTOMY?
GARY D. GROSSFELD,* DAVID M. LATINI, TRACY DOWNS, DEBORAH P. LUBECK,*SHILPA S. MEHTA* AND PETER R. CARROLL†
From the Department of Urology, Program in Urologic Oncology, Urology Outcomes Research Group and University of California-SanFrancisco/Mount Zion Cancer Center, University of California-San Francisco, San Francisco, California, and TAP Pharmaceutical
Products, Inc., Lake Forest, Illinois
ABSTRACT
Purpose: Prostate cancer incidence and mortality are higher in black than in white Americanmen. We determined whether ethnicity is an independent predictor of disease recurrence in menundergoing radical prostatectomy.
Materials and Methods: We studied 1,468 patients who underwent radical prostatectomy atthe University of California, San Francisco or as part of the Cancer of the Prostate StrategicUrological Research Endeavor database, a longitudinal disease registry of patients with prostatecancer. Preoperative characteristics, including age, race, prostate specific antigen (PSA) atdiagnosis, clinical T stage, biopsy Gleason score and percent positive prostate biopsies at diag-nosis were determined in each patient. Disease recurrence was defined as PSA 0.2 ng./ml. orgreater on 2 consecutive occasions after radical prostatectomy or second cancer treatment at least6 months after surgery. Cox proportional hazards analysis was performed to determine indepen-dent predictors of time to disease recurrence. To control for pretreatment disease characteristicssimultaneously patients were assigned to previously described risk groups based on clinicaltumor stage, PSA at diagnosis and biopsy Gleason score. The likelihood of disease recurrence perrisk group stratified according to ethnicity was determined using the Kaplan-Meier method andcompared using the log rank test. Additional multivariate analysis was performed in the subsetof patients enrolled in Cancer of the Prostate Strategic Urological Research Endeavor on whomeducation and income information was available.
Results: Disease recurred in 304 of the 1,468 patients (21%). Black ethnicity, serum PSA atdiagnosis, biopsy Gleason score and percent positive prostate biopsies were independent predic-tors of recurrence on multivariate analysis. Black ethnicity remained an independent predictorof disease recurrence in the multivariate model after stratifying patients into risk groups(p � 0.0007). Ethnicity was most important in patients at high risk, in whom estimated 5-yeardisease-free survival was 65% and 28% in white and black men, respectively. Education, incomeand ethnicity correlated highly. When education and income were entered into the multivariatemodel, ethnicity was no longer an independent predictor of outcome after prostatectomy.
Conclusions: Ethnicity appears to be an independent predictor of disease recurrence afteradjusting for pretreatment measures of disease extent in patients undergoing radical prostatec-tomy. It appears to be particularly important in those with high risk disease characteristics.However, black ethnicity, education and income are highly correlated variables, suggesting thatsociodemographic factors may contribute to the poorer outcomes in black patients even afteradjusting for differences in pretreatment disease characteristics.
KEY WORDS: prostate; prostatic neoplasms; blacks; questionnaires; neoplasm recurrence, local
Black ethnicity is a well-known risk factor for prostatecancer diagnosis and mortality.1–3 Black American men areapproximately 1.5-fold more likely to be diagnosed with and2.5-fold more likely to die of prostate cancer than their whitecounterparts.3 Previous studies have shown that black menpresent with more adverse disease characteristics than whitemen, including higher serum prostate specific antigen (PSA)at diagnosis,4 more advanced clinical tumor stage and higher
grade disease.5–7 This scenario may lead to differences ininitial treatment with a lower rate of definitive local treat-ment and higher rate of initial androgen deprivation in blackthan in white patients.7
Several theories have been proposed to explain these dif-ferences, including earlier onset of more extensive disease inblack men,8 genetic and molecular differences in the races ,9
differences in hormone metabolism,10 dietary factors5 anddelayed or limited access to health care for black versuswhite Americans.11 While there is evidence to support each ofthese theories, no single cause for racial differences in pros-tate cancer incidence or mortality is accepted. In fact, it islikely that multiple factors contribute to this discrepancy.
When considering differences in black and white men withprostate cancer, an important distinction to make is whetherthe more aggressive phenotype in black patients is the result
Accepted for publication July 5, 2002.Supported by National Institutes of Health/National Cancer
Institute University of California-San Francisco Special Program ofResearch Excellence Grant Number 1 p50 c89520 and TAPPharmaceutical Products.
* Financial interest and/or other relationship with TAPPharmaceuticals.
† Financial interest and/or other relationship with AblationTechnologies, Astra Zeneca, Southwest Oncology Group and TAPPharmaceuticals.
0022-5347/02/1686-2510/0 Vol. 168, 2510–2515, December 2002THE JOURNAL OF UROLOGY® Printed in U.S.A.Copyright © 2002 by AMERICAN UROLOGICAL ASSOCIATION, INC.® DOI: 10.1097/01.ju.0000036493.19691.e0
2510

of genetic and/or molecular differences in the races or simplyof socioeconomic factors, such as poorer use of or access toquality health care. If molecular or genetic differences causeincreased prostate cancer progression in black men, basicscience research aimed at identifying these factors would becritical. In contrast, if attitudes with respect to health careand cancer screening or limited access to, quality or use ofhealth care prove to be major causes for adverse outcomes inblack men with prostate cancer, intervention strategies de-signed to change these behaviors and health care policiesshould be implemented.
We determined whether ethnicity remains an independentpredictor of disease recurrence in patients undergoing radi-cal prostatectomy after adjusting for important sociodemo-graphic and pretreatment clinical disease characteristics.Patients were recruited from urology practices representingall regions of the United States to decrease the impact ofgeographical differences on treatment outcome. In this waywe removed as many potential confounding factors as possi-ble to determine the impact of ethnicity on outcome afterprostatectomy.
MATERIALS AND METHODS
Study population. The study population included 1,468men with biopsy proved prostate cancer who underwent rad-ical prostatectomy at University of California-San Franciscoor as a participant in the Cancer of the Prostate StrategicUrological Research Endeavor (CaPSURE) database, a lon-gitudinal observational disease registry of patients withprostate cancer recruited through a network of urologists at35 community and academic urology practice sites distrib-uted throughout the United States. This series represents aconsecutive series of patients undergoing radical prostatec-tomy between December 1986 and April 2001 at University ofCalifornia-San Francisco and between January 1989 andDecember 1998 in CaPSURE on whom complete pretreat-ment clinical data were available. Patients were excludedfrom analysis if they received neoadjuvant androgen depri-vation or radiation before radical prostatectomy, or if adju-vant treatment (radiation or androgen deprivation) was ad-ministered within 6 months of surgery. Institutional reviewboard approval for the project was obtained at each studysite.
Outcomes measured. The primary end point of analysiswas disease recurrence after radical prostatectomy. Diseaserecurrence was defined by detectable serum PSA after sur-gery or second cancer treatment administered more than 6months after radical prostatectomy. Biochemical disease re-currence was defined as serum PSA 0.2 ng./ml. or greater on2 occasions after surgery. Although complete postoperativePSA data were available on all University of California-SanFrancisco patients, some CaPSURE patients were enrolled inthe database despite a considerable interval since diagnosisand treatment. Because PSA values were not routinely re-corded for the period between diagnosis and enrollment, se-rial PSA data were not complete on all CaPSURE patients.Thus, in some cases disease recurrence was based secondprostate cancer treatment, such as radiotherapy or androgendeprivation, delivered more than 6 months after radical pros-tatectomy. Previous studies have shown that such treatmentcan be used as a surrogate marker of disease recurrence inthis patient population.12
Data analysis. Baseline demographic and preoperativeclinical disease characteristics were determined in the over-all study group. Demographic information included age, eth-nicity and year of surgery in all patients, while informationon income and education was available on the subset enrolledin CaPSURE. Ethnicity was categorized as white, black orother. Preoperative disease characteristics included clinicalT stage, as assigned by the treating urologist according to the
1992 American Joint Committee on Cancer (AJCC) TNMstaging system, serum PSA at diagnosis, and primary andsecondary Gleason patterns in the diagnostic biopsy speci-men. The percent positive prostate biopsies at diagnosis wascalculated as the number of biopsies positive for cancer di-vided by the total number of prostate biopsies obtained. Coxproportional hazards multivariate analysis was performed todetermine whether ethnicity was an independent predictor oftime to disease recurrence after adjusting for preoperativeclinical and demographic differences in black and white men.Because we were interested in determining whether ethnic-ity and other measures of socioeconomic status contributedsignificantly to the model of time to disease recurrence usingclinical characteristics, we used a hierarchical modeling ap-proach. Patient age, serum PSA at diagnosis, Gleason scoreand percent positive biopsies were all considered continuousvariables in this multivariate analysis. These variables aswell as clinical tumor stage were forced into the model, whileblack ethnicity was allowed to enter in stepwise fashion onlyif it was determined to be a significant independent predictorof recurrence. Clinical stage T1 and white ethnicity wereconsidered the reference groups for these variables on mul-tivariate analysis.
The significance of ethnicity on the likelihood of diseaserecurrence was further investigated by assigning patients topreviously described risk groups based on serum PSA atdiagnosis, clinical tumor stage and biopsy Gleason score.13
This technique enabled the adjustment of pretreatment dis-ease characteristics simultaneously. We defined risk as low—serum PSA less than 10 ng./ml., total biopsy Gleason score 6or less and 1992 AJCC clinical stage T1c or T2a disease,intermediate—a serum PSA at diagnosis of 10.1 to 20 ng./ml.,total biopsy Gleason score 7 or 1992 AJCC clinical stage T2bdisease and high—serum PSA greater than 20 ng./ml., totalbiopsy Gleason 8 to 10 or 1992 AJCC clinical stage T2c or T3disease. Risk group with low risk as the reference group,patient age and percent positive biopsies were entered intothe Cox model with black ethnicity allowed to enter only if itwas a statistically significant independent predictor of timeto disease recurrence. The likelihood of disease recurrenceper risk group stratified according to ethnicity was deter-mined using the Kaplan-Meier method and compared by thelog rank test.
Additional Cox proportional hazards multivariate analysiswas performed using the subset of 975 CaPSURE patients onwhom education and income information was available. Thisanalysis was performed in a manner similar to those de-scribed with clinical and sociodemographic characteristics,including education and income, entered into the model.Education level of high school diploma or less and a house-hold income of $0 to $30,000 were used as the referencegroups for analysis. Statistical significance was considered at� � 0.05. All data were analyzed using commercially avail-able software.
RESULTS
Median followup after surgery in all patients was 3.1years. Disease recurred in 304 of the 1,468 men (21%).Increasing serum PSA defined recurrence in 59% of whiteand 66% of black men with recurrence after prostatectomy,while second cancer treatment defined recurrence in 41% and34%, respectively (p � 0.4). Tables 1 and 2 list baselinesociodemographic and clinical disease characteristics of theoverall study group based on disease status at last followup.There were significant differences in patient age, ethnicity,educational level, household income, serum PSA at diagno-sis, biopsy Gleason score, clinical tumor stage, percent posi-tive prostate biopsies and risk group classification in menwith and without disease recurrence (tables 1 and 2).
Table 3 lists clinical and sociodemographic characteristics
ETHNICITY IS PREDICTOR OF PROSTATE CANCER RECURRENCE 2511
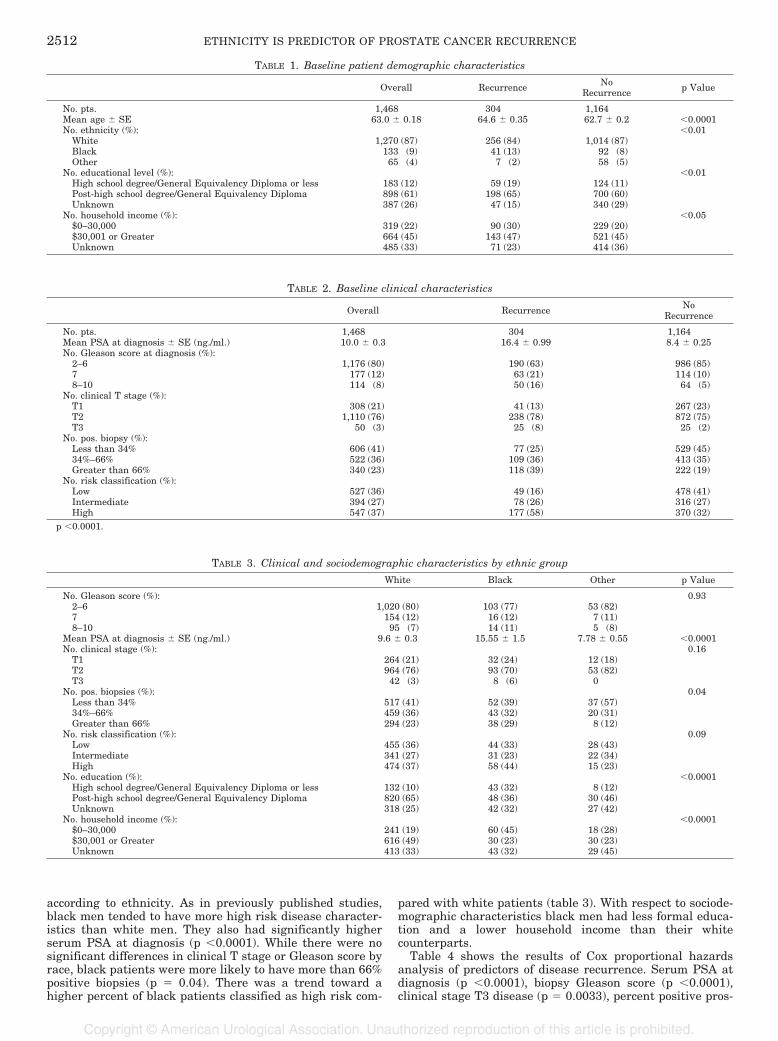
according to ethnicity. As in previously published studies,black men tended to have more high risk disease character-istics than white men. They also had significantly higherserum PSA at diagnosis (p �0.0001). While there were nosignificant differences in clinical T stage or Gleason score byrace, black patients were more likely to have more than 66%positive biopsies (p � 0.04). There was a trend toward ahigher percent of black patients classified as high risk com-
pared with white patients (table 3). With respect to sociode-mographic characteristics black men had less formal educa-tion and a lower household income than their whitecounterparts.
Table 4 shows the results of Cox proportional hazardsanalysis of predictors of disease recurrence. Serum PSA atdiagnosis (p �0.0001), biopsy Gleason score (p �0.0001),clinical stage T3 disease (p � 0.0033), percent positive pros-
TABLE 1. Baseline patient demographic characteristics
Overall Recurrence NoRecurrence p Value
No. pts. 1,468 304 1,164Mean age � SE 63.0 � 0.18 64.6 � 0.35 62.7 � 0.2 �0.0001No. ethnicity (%): �0.01
White 1,270 (87) 256 (84) 1,014 (87)Black 133 (9) 41 (13) 92 (8)Other 65 (4) 7 (2) 58 (5)
No. educational level (%): �0.01High school degree/General Equivalency Diploma or less 183 (12) 59 (19) 124 (11)Post-high school degree/General Equivalency Diploma 898 (61) 198 (65) 700 (60)Unknown 387 (26) 47 (15) 340 (29)
No. household income (%): �0.05$0–30,000 319 (22) 90 (30) 229 (20)$30,001 or Greater 664 (45) 143 (47) 521 (45)Unknown 485 (33) 71 (23) 414 (36)
TABLE 2. Baseline clinical characteristics
Overall Recurrence NoRecurrence
No. pts. 1,468 304 1,164Mean PSA at diagnosis � SE (ng./ml.) 10.0 � 0.3 16.4 � 0.99 8.4 � 0.25No. Gleason score at diagnosis (%):
2–6 1,176 (80) 190 (63) 986 (85)7 177 (12) 63 (21) 114 (10)8–10 114 (8) 50 (16) 64 (5)
No. clinical T stage (%):T1 308 (21) 41 (13) 267 (23)T2 1,110 (76) 238 (78) 872 (75)T3 50 (3) 25 (8) 25 (2)
No. pos. biopsy (%):Less than 34% 606 (41) 77 (25) 529 (45)34%–66% 522 (36) 109 (36) 413 (35)Greater than 66% 340 (23) 118 (39) 222 (19)
No. risk classification (%):Low 527 (36) 49 (16) 478 (41)Intermediate 394 (27) 78 (26) 316 (27)High 547 (37) 177 (58) 370 (32)
p �0.0001.
TABLE 3. Clinical and sociodemographic characteristics by ethnic group
White Black Other p Value
No. Gleason score (%): 0.932–6 1,020 (80) 103 (77) 53 (82)7 154 (12) 16 (12) 7 (11)8–10 95 (7) 14 (11) 5 (8)
Mean PSA at diagnosis � SE (ng./ml.) 9.6 � 0.3 15.55 � 1.5 7.78 � 0.55 �0.0001No. clinical stage (%): 0.16
T1 264 (21) 32 (24) 12 (18)T2 964 (76) 93 (70) 53 (82)T3 42 (3) 8 (6) 0
No. pos. biopsies (%): 0.04Less than 34% 517 (41) 52 (39) 37 (57)34%–66% 459 (36) 43 (32) 20 (31)Greater than 66% 294 (23) 38 (29) 8 (12)
No. risk classification (%): 0.09Low 455 (36) 44 (33) 28 (43)Intermediate 341 (27) 31 (23) 22 (34)High 474 (37) 58 (44) 15 (23)
No. education (%): �0.0001High school degree/General Equivalency Diploma or less 132 (10) 43 (32) 8 (12)Post-high school degree/General Equivalency Diploma 820 (65) 48 (36) 30 (46)Unknown 318 (25) 42 (32) 27 (42)
No. household income (%): �0.0001$0–30,000 241 (19) 60 (45) 18 (28)$30,001 or Greater 616 (49) 30 (23) 30 (23)Unknown 413 (33) 43 (32) 29 (45)
ETHNICITY IS PREDICTOR OF PROSTATE CANCER RECURRENCE2512
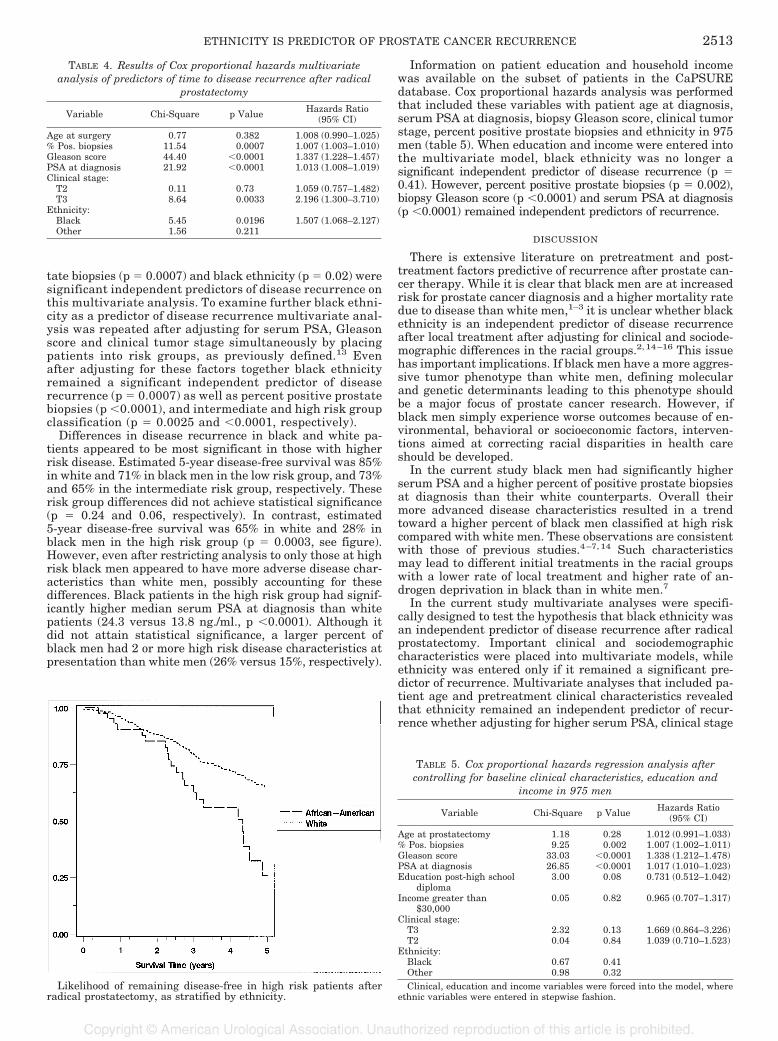
tate biopsies (p � 0.0007) and black ethnicity (p � 0.02) weresignificant independent predictors of disease recurrence onthis multivariate analysis. To examine further black ethni-city as a predictor of disease recurrence multivariate anal-ysis was repeated after adjusting for serum PSA, Gleasonscore and clinical tumor stage simultaneously by placingpatients into risk groups, as previously defined.13 Evenafter adjusting for these factors together black ethnicityremained a significant independent predictor of diseaserecurrence (p � 0.0007) as well as percent positive prostatebiopsies (p �0.0001), and intermediate and high risk groupclassification (p � 0.0025 and �0.0001, respectively).
Differences in disease recurrence in black and white pa-tients appeared to be most significant in those with higherrisk disease. Estimated 5-year disease-free survival was 85%in white and 71% in black men in the low risk group, and 73%and 65% in the intermediate risk group, respectively. Theserisk group differences did not achieve statistical significance(p � 0.24 and 0.06, respectively). In contrast, estimated5-year disease-free survival was 65% in white and 28% inblack men in the high risk group (p � 0.0003, see figure).However, even after restricting analysis to only those at highrisk black men appeared to have more adverse disease char-acteristics than white men, possibly accounting for thesedifferences. Black patients in the high risk group had signif-icantly higher median serum PSA at diagnosis than whitepatients (24.3 versus 13.8 ng./ml., p �0.0001). Although itdid not attain statistical significance, a larger percent ofblack men had 2 or more high risk disease characteristics atpresentation than white men (26% versus 15%, respectively).
Information on patient education and household incomewas available on the subset of patients in the CaPSUREdatabase. Cox proportional hazards analysis was performedthat included these variables with patient age at diagnosis,serum PSA at diagnosis, biopsy Gleason score, clinical tumorstage, percent positive prostate biopsies and ethnicity in 975men (table 5). When education and income were entered intothe multivariate model, black ethnicity was no longer asignificant independent predictor of disease recurrence (p �0.41). However, percent positive prostate biopsies (p � 0.002),biopsy Gleason score (p �0.0001) and serum PSA at diagnosis(p �0.0001) remained independent predictors of recurrence.
DISCUSSION
There is extensive literature on pretreatment and post-treatment factors predictive of recurrence after prostate can-cer therapy. While it is clear that black men are at increasedrisk for prostate cancer diagnosis and a higher mortality ratedue to disease than white men,1–3 it is unclear whether blackethnicity is an independent predictor of disease recurrenceafter local treatment after adjusting for clinical and sociode-mographic differences in the racial groups.2, 14–16 This issuehas important implications. If black men have a more aggres-sive tumor phenotype than white men, defining molecularand genetic determinants leading to this phenotype shouldbe a major focus of prostate cancer research. However, ifblack men simply experience worse outcomes because of en-vironmental, behavioral or socioeconomic factors, interven-tions aimed at correcting racial disparities in health careshould be developed.
In the current study black men had significantly higherserum PSA and a higher percent of positive prostate biopsiesat diagnosis than their white counterparts. Overall theirmore advanced disease characteristics resulted in a trendtoward a higher percent of black men classified at high riskcompared with white men. These observations are consistentwith those of previous studies.4–7, 14 Such characteristicsmay lead to different initial treatments in the racial groupswith a lower rate of local treatment and higher rate of an-drogen deprivation in black than in white men.7
In the current study multivariate analyses were specifi-cally designed to test the hypothesis that black ethnicity wasan independent predictor of disease recurrence after radicalprostatectomy. Important clinical and sociodemographiccharacteristics were placed into multivariate models, whileethnicity was entered only if it remained a significant pre-dictor of recurrence. Multivariate analyses that included pa-tient age and pretreatment clinical characteristics revealedthat ethnicity remained an independent predictor of recur-rence whether adjusting for higher serum PSA, clinical stage
TABLE 4. Results of Cox proportional hazards multivariateanalysis of predictors of time to disease recurrence after radical
prostatectomy
Variable Chi-Square p Value Hazards Ratio(95% CI)
Age at surgery 0.77 0.382 1.008 (0.990–1.025)% Pos. biopsies 11.54 0.0007 1.007 (1.003–1.010)Gleason score 44.40 �0.0001 1.337 (1.228–1.457)PSA at diagnosis 21.92 �0.0001 1.013 (1.008–1.019)Clinical stage:
T2 0.11 0.73 1.059 (0.757–1.482)T3 8.64 0.0033 2.196 (1.300–3.710)
Ethnicity:Black 5.45 0.0196 1.507 (1.068–2.127)Other 1.56 0.211
Likelihood of remaining disease-free in high risk patients afterradical prostatectomy, as stratified by ethnicity.
TABLE 5. Cox proportional hazards regression analysis aftercontrolling for baseline clinical characteristics, education and
income in 975 men
Variable Chi-Square p Value Hazards Ratio(95% CI)
Age at prostatectomy 1.18 0.28 1.012 (0.991–1.033)% Pos. biopsies 9.25 0.002 1.007 (1.002–1.011)Gleason score 33.03 �0.0001 1.338 (1.212–1.478)PSA at diagnosis 26.85 �0.0001 1.017 (1.010–1.023)Education post-high school
diploma3.00 0.08 0.731 (0.512–1.042)
Income greater than$30,000
0.05 0.82 0.965 (0.707–1.317)
Clinical stage:T3 2.32 0.13 1.669 (0.864–3.226)T2 0.04 0.84 1.039 (0.710–1.523)
Ethnicity:Black 0.67 0.41Other 0.98 0.32Clinical, education and income variables were forced into the model, where
ethnic variables were entered in stepwise fashion.
ETHNICITY IS PREDICTOR OF PROSTATE CANCER RECURRENCE 2513

and biopsy Gleason score in black men separately or togetherby placing patients into risk groups. These data suggest thatdifferences in outcome after radical prostatectomy in blackand white men were not only a matter of more advanceddisease at presentation. Results of similar analyses in differ-ent patient groups have varied. Although some investigatorshave reported that black ethnicity is no longer an indepen-dent predictor of disease recurrence and/or survival afteradjusting for differences in clinical disease characteristics inthe races at presentation,14 others agree with our findings inthis regard.2, 15
Racial differences in outcome appeared to be most signifi-cant in patients who presented with high risk disease char-acteristics. Estimated 5-year disease-free survival in whiteand black men with high risk disease was 65% and 28%,respectively. This risk group was the only one in which racialdifferences in disease recurrence attained statistical signifi-cance. Analysis of the high risk group showed that black menhad significantly higher PSA at diagnosis. A similar percentof black and white men were classified at high risk based ona biopsy Gleason score of 8 to 10. Although it did not achievestatistical significance, a higher percent of black patients had2 or more high risk factors compared with white patients(26% versus 15%), suggesting that even in the high riskgroup black men may still have more adverse disease char-acteristics.
While these analyses were adjusted for differences in clin-ical disease characteristics and age between patient groups,they did not account for the complex sociodemographic dif-ferences in black and white men that may limit access to oruse of health care services. Previously others have attemptedto remove financial barriers to care by studying black pa-tients in equal access health care systems, such as theVeterans Administration or military health care system.Unfortunately such studies failed to show consistently im-proved outcomes in black patients that were equivalent tothose of their white counterparts.16, 17 Therefore, it is likelythat improving health care use is more complex than simplyremoving financial barriers. Minority race, low socioeconomicstatus, advanced age, unemployment, patient behavior andattitude, geographic location, availability of transportation,family and other support systems, individual awareness andeducation appear to limit health care use by black men.18
Studies in men with low income show that illiteracy may alsobe a significant barrier to prostate cancer diagnosis,19 whileothers show that black men often refuse to participate inscreening programs because of concerns on the potentialrisks associated with treatment if prostate cancer were de-tected.20
Although we were clearly unable to consider all factorsthat contribute to health care use, the current results sup-port a complex interaction among ethnicity, income and ed-ucation in black men treated for prostate cancer. When edu-cation and income were entered into the multivariateanalysis of the subgroup of patients enrolled in CaPSURE,black ethnicity was no longer a significant predictor of dis-ease recurrence. There appeared to be a strong correlationamong ethnicity, education and income with none of thesefactors attaining statistical significance as an independentpredictor of outcome when all variables were considered.Such results suggest that sociodemographic factors may con-tribute to the poorer outcome in black patients after radicalprostatectomy. It is likely that educational and income dif-ferences in the racial groups only reflect part of the story withother important cultural differences regarding attitudes to-ward screening and preventive care, access to quality healthcare and health care use also contributing to poorer outcomesin black men with prostate cancer. We believe that theseresults warrant additional research in larger patient popu-lations to distinguish better the influence of individual socio-economic factors on outcome after prostate cancer treatment.
Important limitations of this study must be acknowledged.Data were obtained retrospectively. Despite adjusting forclinical and sociodemographic differences in racial groups onmultivariate analyses unrecognized biases may have oc-curred that could have influenced our results. Although pa-tients were enrolled from 35 urology practices locatedthroughout the United States, most American patients wererecruited at 5 sites. This factor may have limited how thedata may be generalized and introduced unrecognized bias inpatient selection, treatment and outcome. Serial PSA datawere not available on all patients enrolled in CaPSURE. As aresult, disease recurrence was defined by second prostatecancer treatment in 40% of patients with recurrence afterprostatectomy. This incidence was similar in black and whitemen (34% and 41%, respectively, p � 0.4). Nevertheless,physician and patient bias as well as geographic differencesin prostate cancer care may influence the delivery of second-ary cancer treatment. Although we attempted to determinethe cause of racial differences in outcome after radical pros-tatectomy by adjusting for differences in sociodemographiccharacteristics in racial groups, it is impossible to account fordifferences in attitudes, behavior, family support and indi-vidual bias. We had information on education and income ina subset of patients that appeared to be significantly associ-ated with ethnicity. In fact, the association was so strong thatit was difficult to determine which factor, if any, was mostimportant for determining treatment related outcome. Toovercome this limitation a different type of analysis, such asmatched pair analysis, may be necessary to determine betterwhether ethnicity remains an important predictor of outcomeafter controlling for education or income. We are in the pro-cess of designing such an analysis.
CONCLUSIONS
On multivariate analyses and after adjusting for patientage and important clinical disease characteristics black eth-nicity remained an independent predictor of disease recur-rence after radical prostatectomy. This finding was truewhether serum PSA at diagnosis, clinical tumor stage andbiopsy Gleason grade were adjusted for separately or to-gether by assigning patients to previously described riskgroups. Ethnicity as a predictor of outcome appeared to bemost important in patients with high risk disease character-istics, of whom white men had significantly higher estimated5-year disease-free survival than black men. After addingpatient education and income into the multivariate model,black ethnicity was no longer a predictor of disease-free sur-vival. Black ethnicity, education and income were highlycorrelated variables, suggesting that sociodemographic dif-ferences in the races may contribute to poorer outcomes inblack patients after radical prostatectomy. These findingswarrant additional investigation in other patient groups us-ing statistical methods designed to separate the influence ofthese highly correlated variables. Such research may assistinvestigators in designing appropriate interventions to im-prove prostate cancer outcomes in high risk patient groups.
REFERENCES
1. Farkas, A., Schneider, D., Perrotti, M., Cummings, K. B. andWard, W. S.: National trends in the epidemiology of prostatecancer, 1973 to 1994: evidence for the effectiveness of prostate-specific antigen screening. Urology, 52: 444, 1998
2. Pienta, K. J., Demers, R., Hoff, M., Kau, T. Y., Montie, J. E. andSeverson, R. K.: Effect of age and race on the survival of menwith prostate cancer in the Metropolitan Detroit tricountyarea, 1973 to 1987. Urology, 45: 93, 1995
3. Powell, I. J.: Prostate cancer in the African American: is this adifferent disease? Semin Urol Oncol, 16: 221, 1998
4. Moul, J. W., Sesterhenn, I. A., Connelly, R. R., Douglas, T.,Srivastava, S., Mostofi, F. K. et al: Prostate-specific antigenvalues at the time of prostate cancer diagnosis in African-
ETHNICITY IS PREDICTOR OF PROSTATE CANCER RECURRENCE2514
American men. JAMA, 274: 1277, 19955. Amling, C. L., Kane, C. J., Riffenburgh, R. H., Ward, J. F.,
Roberts, J. L., Lance, R. S. et al: Relationship between obesityand race in predicting adverse pathologic variables in patientsundergoing radical prostatectomy. Urology, 58: 723, 2001
6. Fowler, J. E., Jr. and Bigler, S. A : A prospective study of theserum prostate specific antigen concentrations and Gleasonhistologic scores of black and white men with prostate carci-noma. Cancer, 86: 836, 1999
7. Lubeck, D. P., Kim, H., Grossfeld, G., Ray, P., Penson, D. F.,Flanders, S. C. et al: Health related quality of life differencesbetween black and white men with prostate cancer: data fromthe cancer of the prostate strategic urologic research endeavor.J Urol, 166: 2281, 2001
8. Sakr, W. A., Haas, G. P., Cassin, B. F., Pontes, J. E. andCrissman, J. D.: The frequency of carcinoma and intraepithe-lial neoplasia of the prostate in young male patients. J Urol,150: 379, 1993
9. Giovannucci, E., Stampfer, M. J., Krithivas, K., Brown, M., Dahl,D., Brufsky, A. et al: The CAG repeat within the androgenreceptor gene and its relationship to prostate cancer. Proc NatlAcad Sci USA, 94: 3320, 1997
10. Ross, R. K., Pike, M. C., Coetzee, G. A., Reichardt, J. K., Yu,M. C., Feigelson, H. et al: Androgen metabolism and prostatecancer: establishing a model of genetic susceptibility. CancerRes, 58: 4497, 1998
11. Ndubuisi, S. C., Kofie, V. Y., Andoh, J. Y. and Schwartz, E. M.:Black-white differences in the stage at presentation of pros-tate cancer in the District of Columbia. Urology, 46: 71, 1995
12. Grossfeld, G. D., Chang, J. J., Broering, J. M., Miller, D. P., Yu,J., Flanders, S. C. et al: Does the completeness of prostatesampling predict outcome for patients undergoing radical
prostatectomy?: data from the CAPSURE database. Urology,56: 430, 2000
13. D’Amico, A. V., Whittington, R., Malkowicz, S. B., Schultz, D.,Fondurulia, J., Chen, M. H. et al: Clinical utility of the per-centage of positive prostate biopsies in defining biochemicaloutcome after radical prostatectomy for patients with clini-cally localized prostate cancer. J Clin Oncol, 18: 1164, 2000
14. Eastham, J. A. and Kattan, M. W.: Disease recurrence in blackand white men undergoing radical prostatectomy for clinicalstage T1–T2 prostate cancer. J Urol, 163: 143, 2000
15. Fowler, J. E., Jr., Bigler, S. A., Bowman, G. and Kilambi, N. K.:Race and cause specific survival with prostate cancer: influ-ence of clinical stage, Gleason score, age and treatment.J Urol, 163: 137, 2000
16. Moul, J. W., Douglas, T. H., McCarthy, W. F. and McLeod, D. G.:Black race is an adverse prognostic factor for prostate cancerrecurrence following radical prostatectomy in an equal accesshealth care setting. J Urol, 155: 1667, 1996
17. Powell, I. J., Schwartz, K. and Hussain, M.: Removal of thefinancial barrier to health care: does it impact on prostatecancer at presentation and survival? A comparative studybetween black and white men in a Veterans Affairs system.Urology, 46: 825, 1995
18. Mandelblatt, J. S., Yabroff, K. R. and Kerner, J. F.: Equitableaccess to cancer services: a review of barriers to quality care.Cancer, 86: 2378, 1999
19. Bennett, C. L., Ferreira, M. R., Davis, T. C., Kaplan, J.,Weinberger, M., Kuzel, T. et al: Relation between literacy,race, and stage of presentation among low-income patientswith prostate cancer. J Clin Oncol, 16: 3101, 1998
20. Robinson, S. B., Ashley, M. and Haynes, M. A.: Attitudes ofAfrican Americans regarding screening for prostate cancer.J Natl Med Assoc, 88: 241, 1996
ETHNICITY IS PREDICTOR OF PROSTATE CANCER RECURRENCE 2515





























