Embed Size (px)
Citation preview
Romanian Journal of Morphology and Embryology 2009, 50(4):583–587
OORRIIGGIINNAALL PPAAPPEERR
Irritated seborrheic keratosis with coarse keratohyalin granules
A. FERNANDEZ-FLORES
Service of Anatomic Pathology, Hospital El Bierzo Service of Cellular Pathology, Clinica Ponferrada, Ponferrada, Spain
Abstract Aims: The viral etiology of certain types of seborrheic keratosis (SK) has been a controversial subject in literature, with different molecular results. On the contrary, to the molecular approach, some have suggested that certain types of SK are indeed warts, due to their morphologic features. We decided to investigate the presence of coarse keratohyalin granules in cases of irritated SK. Material, Methods and Results: We examined the last 60 cases with such a diagnosis in our Service of Anatomic Pathology and found these granules in eight cases (7.5%). The granules were evidenced in squamous eddies in four cases, while they were seen in foci of hypergranulosis from the top part of the epidermis in five cases. These granules were evidenced in a few foci in three cases while they were seen in multiple foci in five cases. In these eight cases, we also looked for other morphologic signs suggesting a viral origin, such as papilated, exo-endophytic configuration, parakeratosis at the tips of digitations, dilated vessels in the papillae and koilocytes. While six cases presented at least any of these other features, in two of the eight cases (25%), the only clue suggesting a viral origin was the evidence of the thick granules of keratohyalin. Conclusions: We discuss the meaning of such a finding as described in literature, and conclude that it should be a specific feature to look out for, in cases of irritated SK, in order to exclude a diagnosis of verruca vulgaris. Keywords: irritated seborrheic keratosis, inverted follicular keratosis, human papillomavirus, keratohyalin granules, verruca
vulgaris, viral wart.
Introduction
The subject on the viral origin of seborrheic keratosis (SK) is controversial. For some, inverted follicular kera-tosis would actually be a viral wart [1]. While the term inverted follicular keratosis has been equaled to irritated SK by many [2–4], this is not a universally accepted assertion: some clearly distinguish SK (a tumor which sometimes can be irritated) from an inverted follicular keratosis (a type of wart) [1]. The molecular studies, which could be of help in such a debate, have added some controversy to the subject, with contradictory results when cases of SK have been studied for papillo-mavirus infection [5–17]. On the contrary, some teams have relied on the more traditional histopathologic features to claim the viral nature of inverted follicular keratosis [1]. We decided to investigate the presence of coarse keratohyalin granules (which has been associated to viral infection in cutaneous pathology) in cases of irritated SK. Although some have previously studied the “hyperkeratosis” in cases of inverted follicular keratosis [1], this latter term does not equal “coarse keratohyalin granules”: hyper-keratosis refers only to the thickness of the granular layer, as well as to the number of granules [18], but not to the thickness, the regularity or the shape of the granules themselves.
Material and Methods
We examined the slides of the most recent 60 diag-noses of irritated SK that had been signed in our Service of Anatomic Pathology. In all the cases, we evaluated the type of keratohyalin granules. They were classified as
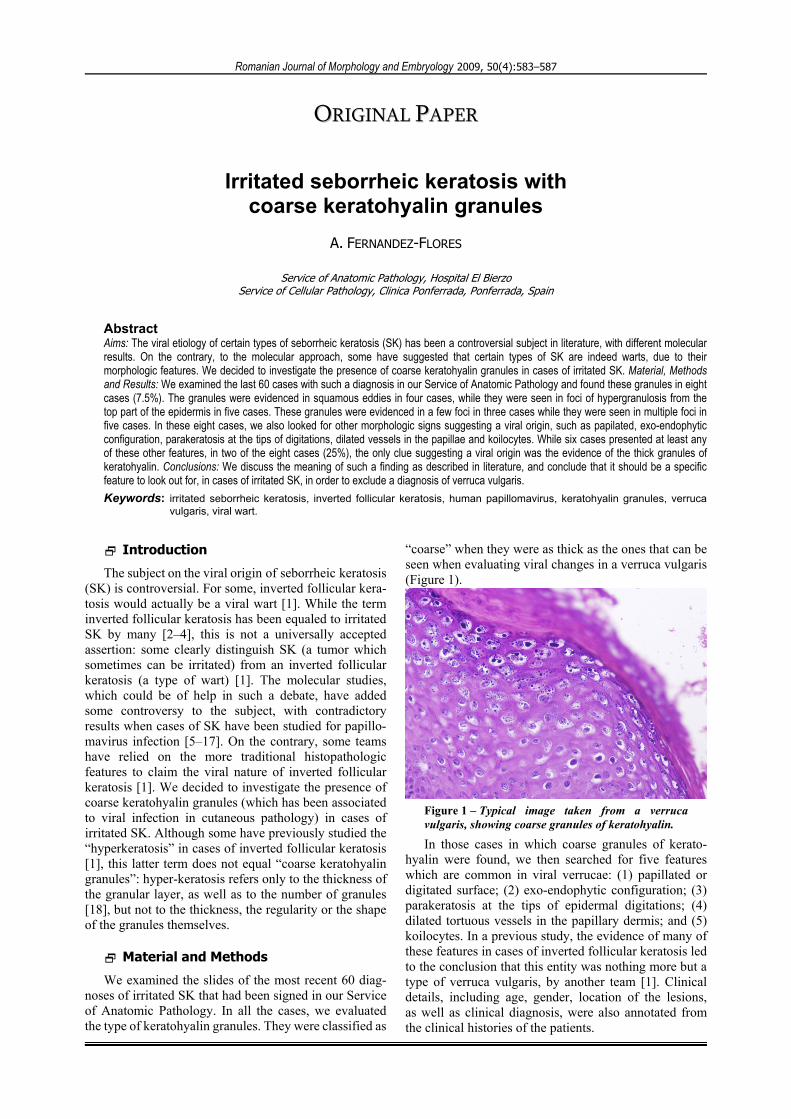
“coarse” when they were as thick as the ones that can be seen when evaluating viral changes in a verruca vulgaris (Figure 1).
Figure 1 – Typical image taken from a verruca vulgaris, showing coarse granules of keratohyalin.
In those cases in which coarse granules of kerato-hyalin were found, we then searched for five features which are common in viral verrucae: (1) papillated or digitated surface; (2) exo-endophytic configuration; (3) parakeratosis at the tips of epidermal digitations; (4) dilated tortuous vessels in the papillary dermis; and (5) koilocytes. In a previous study, the evidence of many of these features in cases of inverted follicular keratosis led to the conclusion that this entity was nothing more but a type of verruca vulgaris, by another team [1]. Clinical details, including age, gender, location of the lesions, as well as clinical diagnosis, were also annotated from the clinical histories of the patients.
A. Fernandez-Flores
584
Results
From the 60 cases evaluated, we found coarse granules of keratohyalin in eight cases (7.5%).
Table 1 shows the clinical details of the patients from which these biopsies were obtained, including the locations of the lesions, as well as the clinical diagnoses.
Table 1 – Clinical details of the patients from whom the biopsies were studied. SK: seborrheic keratosis; BCC: basal cell carcinoma; CND: clinically not diagnosed
Case no. Gender Age Location Clinical diagnosis1. F 85 Back SK 2. M 60 Face SK 3. M 68 Face SK 4. F 78 Eyelid SK 5. F 71 Forehead SK vs. BCC 6. M 78 Chest CND 7. M 83 Face SK 8. F 61 Back SK
Cases no. 1, 5 and 8 accomplished all the criteria that are described in classic books for irritated SK [2]. On the contrary, as it will be mentioned below, we re-diagnosed cases no. 3 and 6 as verruca vulgaris, due to the many morphologic clues that suggested such a diagnosis. In cases no. 4 and 7, features of SK coexisted with some features suggesting a viral wart (Table 2).
Table 2 – Morphologic features suggestive of a viral etiology which were found in the eight cases of irritated SK with coarse keratohyalin granules that we found in our study
Case 1 2 3 4 5 6 7 8 1. Papilated or digitated surface + - + + - + + - 2. Exo-endophytic configuration - - + + - + + - 3. Parakeratosis at the tips of epidermal digitations + - + + - + - +
4. Dilated tortuous vessels in the papillary dermis - - + - - + + -
5. Koilocytes - - - - - - - - Total number of morphologic
features found 2 0 4 3 0 4 3 1
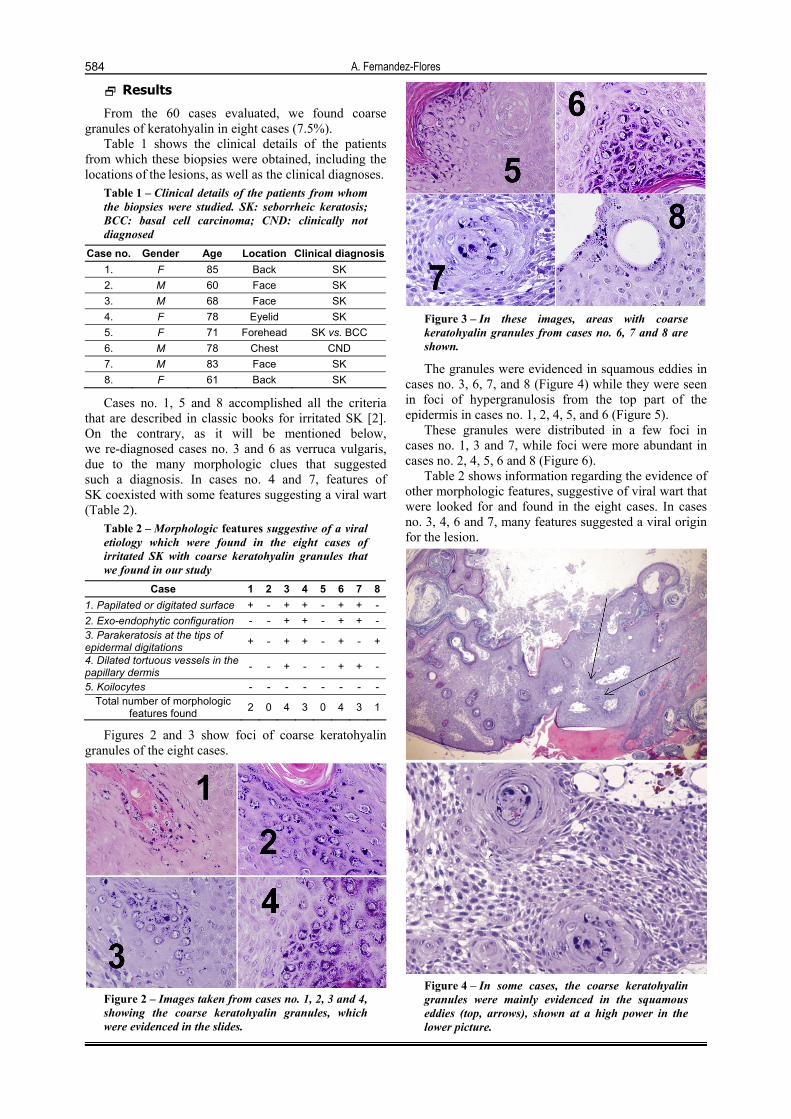
Figures 2 and 3 show foci of coarse keratohyalin granules of the eight cases.
Figure 2 – Images taken from cases no. 1, 2, 3 and 4, showing the coarse keratohyalin granules, which were evidenced in the slides.
Figure 3 – In these images, areas with coarse keratohyalin granules from cases no. 6, 7 and 8 are shown.
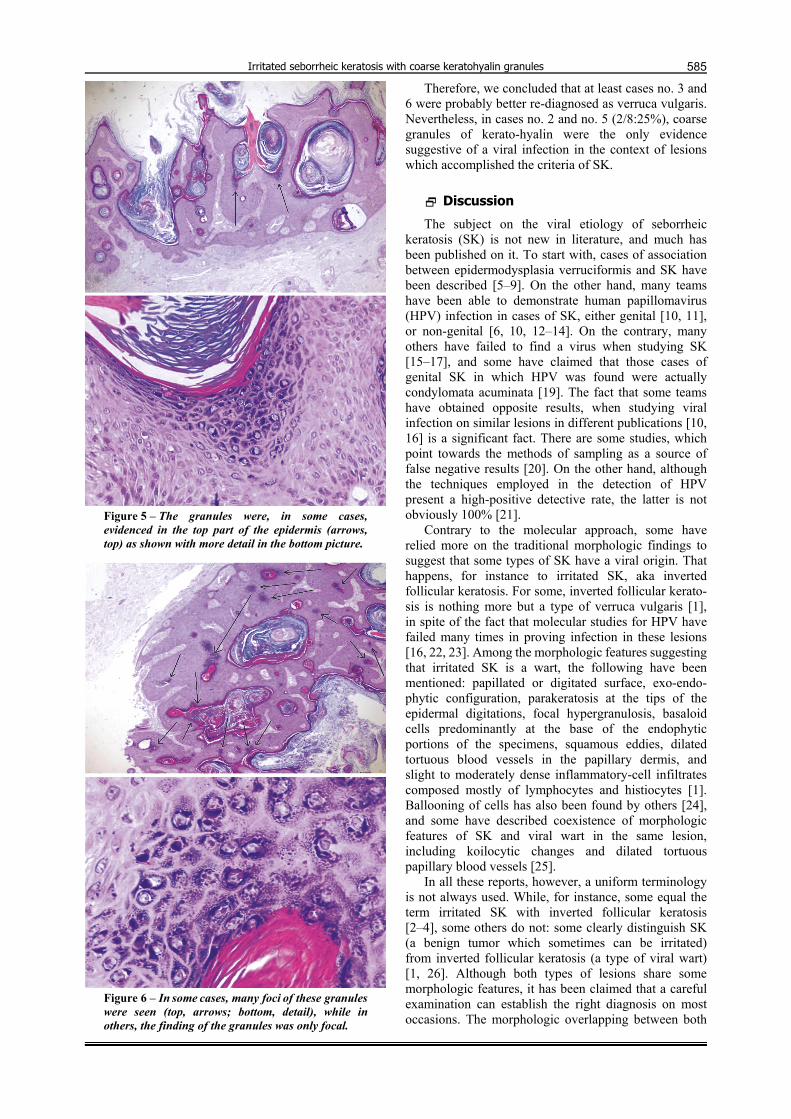
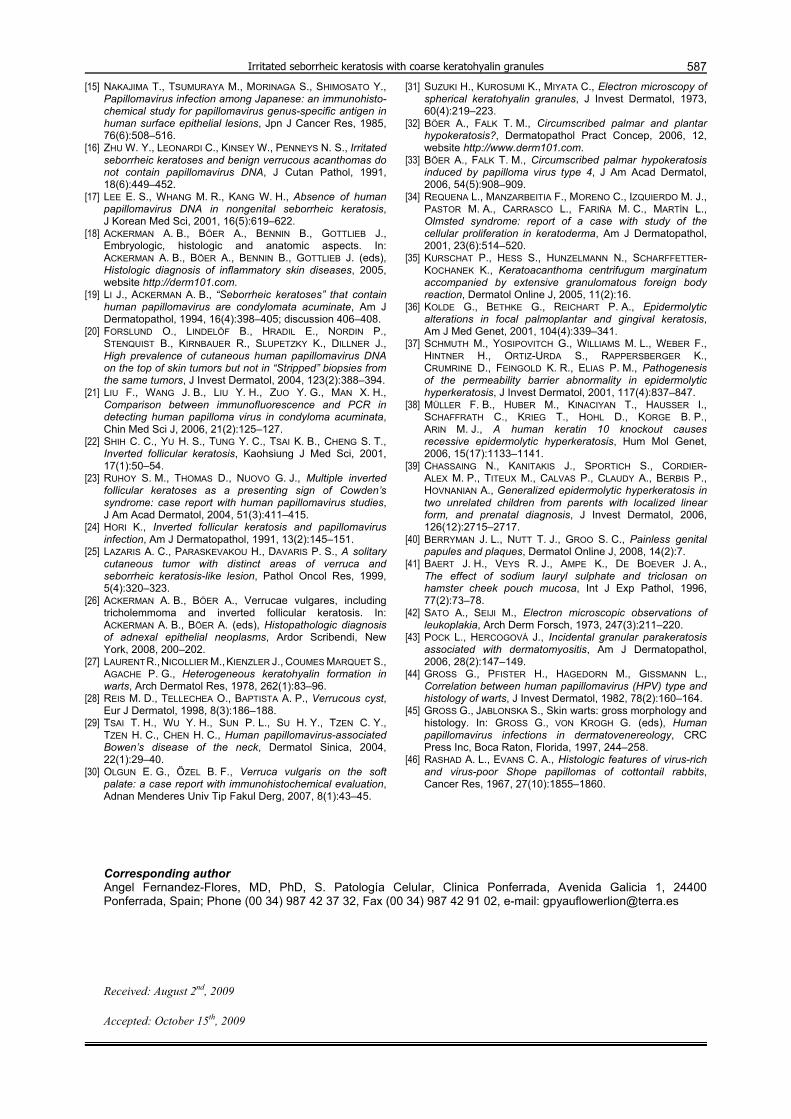
The granules were evidenced in squamous eddies in cases no. 3, 6, 7, and 8 (Figure 4) while they were seen in foci of hypergranulosis from the top part of the epidermis in cases no. 1, 2, 4, 5, and 6 (Figure 5).
These granules were distributed in a few foci in cases no. 1, 3 and 7, while foci were more abundant in cases no. 2, 4, 5, 6 and 8 (Figure 6).
Table 2 shows information regarding the evidence of other morphologic features, suggestive of viral wart that were looked for and found in the eight cases. In cases no. 3, 4, 6 and 7, many features suggested a viral origin for the lesion.
Figure 4 – In some cases, the coarse keratohyalin granules were mainly evidenced in the squamous eddies (top, arrows), shown at a high power in the lower picture.
Irritated seborrheic keratosis with coarse keratohyalin granules
585
Figure 5 – The granules were, in some cases, evidenced in the top part of the epidermis (arrows, top) as shown with more detail in the bottom picture.
Figure 6 – In some cases, many foci of these granules were seen (top, arrows; bottom, detail), while in others, the finding of the granules was only focal.
Therefore, we concluded that at least cases no. 3 and 6 were probably better re-diagnosed as verruca vulgaris. Nevertheless, in cases no. 2 and no. 5 (2/8:25%), coarse granules of kerato-hyalin were the only evidence suggestive of a viral infection in the context of lesions which accomplished the criteria of SK.
Discussion
The subject on the viral etiology of seborrheic keratosis (SK) is not new in literature, and much has been published on it. To start with, cases of association between epidermodysplasia verruciformis and SK have been described [5–9]. On the other hand, many teams have been able to demonstrate human papillomavirus (HPV) infection in cases of SK, either genital [10, 11], or non-genital [6, 10, 12–14]. On the contrary, many others have failed to find a virus when studying SK [15–17], and some have claimed that those cases of genital SK in which HPV was found were actually condylomata acuminata [19]. The fact that some teams have obtained opposite results, when studying viral infection on similar lesions in different publications [10, 16] is a significant fact. There are some studies, which point towards the methods of sampling as a source of false negative results [20]. On the other hand, although the techniques employed in the detection of HPV present a high-positive detective rate, the latter is not obviously 100% [21].
Contrary to the molecular approach, some have relied more on the traditional morphologic findings to suggest that some types of SK have a viral origin. That happens, for instance to irritated SK, aka inverted follicular keratosis. For some, inverted follicular kerato-sis is nothing more but a type of verruca vulgaris [1], in spite of the fact that molecular studies for HPV have failed many times in proving infection in these lesions [16, 22, 23]. Among the morphologic features suggesting that irritated SK is a wart, the following have been mentioned: papillated or digitated surface, exo-endo-phytic configuration, parakeratosis at the tips of the epidermal digitations, focal hypergranulosis, basaloid cells predominantly at the base of the endophytic portions of the specimens, squamous eddies, dilated tortuous blood vessels in the papillary dermis, and slight to moderately dense inflammatory-cell infiltrates composed mostly of lymphocytes and histiocytes [1]. Ballooning of cells has also been found by others [24], and some have described coexistence of morphologic features of SK and viral wart in the same lesion, including koilocytic changes and dilated tortuous papillary blood vessels [25].
In all these reports, however, a uniform terminology is not always used. While, for instance, some equal the term irritated SK with inverted follicular keratosis [2–4], some others do not: some clearly distinguish SK (a benign tumor which sometimes can be irritated) from inverted follicular keratosis (a type of viral wart) [1, 26]. Although both types of lesions share some morphologic features, it has been claimed that a careful examination can establish the right diagnosis on most occasions. The morphologic overlapping between both

A. Fernandez-Flores
586
lesions has led some to suggest the term “SK-like viral wart” [6].
The purpose of our study, rather than abounding on the subject of molecular detection of HPV in SK, was simply to look for evidence of a type of keratin (thick keratohyalin granules) that has commonly been associated with viral infection [27–29], and which is present even when virae infect mucosae [30].
In normal human skin, keratohyalin granules are amorphous, irregular and mildly varying in size [31] (from 0.2 to 4.5 micrae), but not thick or coarse. These thick granules have been found in some diseases, which were first alleged to be non-infectious, but in which, recently papillomavirus is claimed to be involved, such as palmar and plantar hypokeratosis [32, 33]. On the other hand, there are examples of epidermal alterations with coarse keratohyalin granules in which a HPV infection is either non-suspected or not yet investigated: Olmsted syndrome [34], kerato-acanthoma centrifugum marginatum [35], epidermolytic hyperkeratosis [36, 40], chemical aggression [41], premalignant lesions [42], or dermatomyositis [43]. Therefore, we are aware that an evidence of coarse keratohyalin granules is not pathognomonic of viral infection, but rather of an alteration of the normal keratinization process. Nevertheless, since irritated SK presents some other changes suggestive of a virus many times, we think that thick keratohyalin granules would also have such a meaning in this context.
It should also be mentioned how these granules in the epidermis have been related to some viral types and not to others. For instance, while they are described in HPV-2-associated cutaneous lesions [44, 45], they are not seen in HPV-4, -7, -3, -10, -27, or -28 infections [45]. The changes in the granular layer of biopsies infected by HPV-2, for instance, include “condensed keratohyalin granule of various shapes, sizes, and stainability” [45], which are easily recognized by the pathologist when evaluating many cases of verruca vulgaris. This thick keratohyalin has also been related to the amount of viral organisms, with bigger granules in virus-rich papillomas [46]. We found coarse kerato-hyalin granules in 7.5% of our cases of irritated SK: in that respect, it is interesting to mention that HPV-2 has been found in up to 14.4% of non-genital KS cases [14].
Thick keratohyalin granules are not commonly mentioned when referring to irritated KS. It should be clarified that while some authors have investigated “hypergranulosis” in inverted follicular keratosis [1], such a term does not equal thick keratohyalin granules. Hyperkergranulosis just refers to the thickness of the granular layer, as well as to the number of granules [18], but it does not refer to the thickness, the regularity or the shape of the granules themselves.
In our opinion, from our cases, some were easily re-diagnosed as verruca vulgaris, due to the amount of morphologic features suggestive of a wart. Nevertheless, as commented above, at least in some of the cases, coarse keratohyalin granules were the only feature suggestive of such a viral origin. Admitting a viral etiology for these cases would, for instance, explain why HPV is found in only part of the irritated SKs
investigated, but not in all. It would also suggest, at least, two different mechanisms of formation of irritated SK: from a non-infectious, yet unknown cause (i.e., solar lentigo), and from a viral infection. It would also support the concept of a “SK-like viral wart” [6], in which the coarse granules would be the “only” histo-pathologic feature, which could give a clue regarding its viral origin. This remarks the importance of paying attention to the appearance of the keratohyalin granules in any irritated SK. Even if focal, we believe that they are a clue suggestive of a viral origin for the lesion.
Conclusions
Our conclusion is that coarse granules of kerato-hyalin should be a morphologic clue to look for, in any case of irritated SK, and when present, even if only focal, to consider the alternative diagnosis of verruca vulgaris.
References [1] SPIELVOGEL R. L., AUSTIN C., ACKERMAN A. B., Inverted
follicular keratosis is not a specific keratosis but a verruca vulgaris (or seborrheic keratosis) with squamous eddies, Am J Dermatopathol, 1983, 5(5):427–442.
[2] BRENN T., MCKEE P. H., Tumors of the surface epithelium. In: MCKEE P. H., CALONJE E., GRANTER S. R. (eds), Pathology of the skin with clinical correlations, 3rd edition, Elsevier Mosby, Philadelphia, 2005, 1112–1240.
[3] LEVER W. F., Inverted follicular keratosis is an irritated seborrheic keratosis, Am J Dermatopathol, 1983, 5(5):474.
[4] SIM-DAVIS D., MARKS R., WILSON-JONES E., The inverted follicular keratosis. A surprising variant of seborrheic wart, Acta Derm Venereol, 1976, 56(5):337–344.
[5] SANDBANK M., HODAK E., ROTEM A., BEN-DAVID E., The heterogeneity of tumours associated with epidermo-dysplasia verruciformis, Acta Derm Venereol, 1987, 67(1):79–82.
[6] JACYK W. K., DREYER L., DE VILLIERS E. M., Seborrheic keratoses of black patients with epidermodysplasia verruciformis contain human papillomavirus DNA, Am J Dermatopathol, 1993, 15(1):1–6.
[7] TOMASINI C., ALOI F., PIPPIONE M., Seborrheic keratosis-like lesions in epidermodysplasia verruciformis, J Cutan Pathol, 1993, 20(3):237–241.
[8] RONCALLI DE OLIVEIRA W., NETO C. F., RADY P. L., TYRING S. K., Seborrheic Keratosis-like lesions in patients with epidermodysplasia verruciformis, J Dermatol, 2003, 30(1):48–53.
[9] FOONG H. B., IBRAHIMI O. A., ELPERN D. J., TYRING S., RADY P., CARLSON J. A., Multiple facial seborrheic keratosis-like lesions in a young woman with epidermodysplasia verruciformis, Int J Dermatol, 2008, 47(5):476–478.
[10] ZHU W. Y., LEONARDI C., PENNEYS N. S., Detection of human papillomavirus DNA in seborrheic keratosis by poly-merase chain reaction, J Dermatol Sci, 1992, 4(3):166–171.
[11] BAI H., CVIKO A., GRANTER S., YUAN L., BETENSKY R. A., CRUM C. P., Immunophenotypic and viral (human papillo-mavirus) correlates of vulvar seborrheic keratosis, Hum Pathol, 2003, 34(6):559–564.
[12] ZHAO Y. K., LIN Y. X., LUO R. Y., HUANG X. Y., LIU M. Z., XIA M., JIN H., Human papillomavirus (HPV) infection in seborrheic keratosis, Am J Dermatopathol, 1989, 11(3):209–212.
[13] TSAMBAOS D., MONASTIRLI A., KAPRANOS N., GEORGIOU S., PASMATZI E., STRATIGOS A., KOUTSELINI H., BERGER H., Detection of human papillomavirus DNA in nongenital seborrhoeic keratoses, Arch Dermatol Res, 1995, 287(6):612–615.
[14] GUSHI A., KANEKURA T., KANZAKI T., EIZURU Y., Detection and sequences of human papillomavirus DNA in non-genital seborrhoeic keratosis of immunopotent individuals, J Dermatol Sci, 2003, 31(2):143–149.
Irritated seborrheic keratosis with coarse keratohyalin granules
587[15] NAKAJIMA T., TSUMURAYA M., MORINAGA S., SHIMOSATO Y.,
Papillomavirus infection among Japanese: an immunohisto-chemical study for papillomavirus genus-specific antigen in human surface epithelial lesions, Jpn J Cancer Res, 1985, 76(6):508–516.
[16] ZHU W. Y., LEONARDI C., KINSEY W., PENNEYS N. S., Irritated seborrheic keratoses and benign verrucous acanthomas do not contain papillomavirus DNA, J Cutan Pathol, 1991, 18(6):449–452.
[17] LEE E. S., WHANG M. R., KANG W. H., Absence of human papillomavirus DNA in nongenital seborrheic keratosis, J Korean Med Sci, 2001, 16(5):619–622.
[18] ACKERMAN A. B., BÖER A., BENNIN B., GOTTLIEB J., Embryologic, histologic and anatomic aspects. In: ACKERMAN A. B., BÖER A., BENNIN B., GOTTLIEB J. (eds), Histologic diagnosis of inflammatory skin diseases, 2005, website http://derm101.com.
[19] LI J., ACKERMAN A. B., “Seborrheic keratoses” that contain human papillomavirus are condylomata acuminate, Am J Dermatopathol, 1994, 16(4):398–405; discussion 406–408.
[20] FORSLUND O., LINDELÖF B., HRADIL E., NORDIN P., STENQUIST B., KIRNBAUER R., SLUPETZKY K., DILLNER J., High prevalence of cutaneous human papillomavirus DNA on the top of skin tumors but not in “Stripped” biopsies from the same tumors, J Invest Dermatol, 2004, 123(2):388–394.
[21] LIU F., WANG J. B., LIU Y. H., ZUO Y. G., MAN X. H., Comparison between immunofluorescence and PCR in detecting human papilloma virus in condyloma acuminata, Chin Med Sci J, 2006, 21(2):125–127.
[22] SHIH C. C., YU H. S., TUNG Y. C., TSAI K. B., CHENG S. T., Inverted follicular keratosis, Kaohsiung J Med Sci, 2001, 17(1):50–54.
[23] RUHOY S. M., THOMAS D., NUOVO G. J., Multiple inverted follicular keratoses as a presenting sign of Cowden’s syndrome: case report with human papillomavirus studies, J Am Acad Dermatol, 2004, 51(3):411–415.
[24] HORI K., Inverted follicular keratosis and papillomavirus infection, Am J Dermatopathol, 1991, 13(2):145–151.
[25] LAZARIS A. C., PARASKEVAKOU H., DAVARIS P. S., A solitary cutaneous tumor with distinct areas of verruca and seborrheic keratosis-like lesion, Pathol Oncol Res, 1999, 5(4):320–323.
[26] ACKERMAN A. B., BÖER A., Verrucae vulgares, including tricholemmoma and inverted follicular keratosis. In: ACKERMAN A. B., BÖER A. (eds), Histopathologic diagnosis of adnexal epithelial neoplasms, Ardor Scribendi, New York, 2008, 200–202.
[27] LAURENT R., NICOLLIER M., KIENZLER J., COUMES MARQUET S.,
AGACHE P. G., Heterogeneous keratohyalin formation in warts, Arch Dermatol Res, 1978, 262(1):83–96.
[28] REIS M. D., TELLECHEA O., BAPTISTA A. P., Verrucous cyst, Eur J Dermatol, 1998, 8(3):186–188.
[29] TSAI T. H., WU Y. H., SUN P. L., SU H. Y., TZEN C. Y., TZEN H. C., CHEN H. C., Human papillomavirus-associated Bowen’s disease of the neck, Dermatol Sinica, 2004, 22(1):29–40.
[30] OLGUN E. G., ÖZEL B. F., Verruca vulgaris on the soft palate: a case report with immunohistochemical evaluation, Adnan Menderes Univ Tip Fakul Derg, 2007, 8(1):43–45.
[31] SUZUKI H., KUROSUMI K., MIYATA C., Electron microscopy of spherical keratohyalin granules, J Invest Dermatol, 1973, 60(4):219–223.
[32] BÖER A., FALK T. M., Circumscribed palmar and plantar hypokeratosis?, Dermatopathol Pract Concep, 2006, 12, website http://www.derm101.com.
[33] BÖER A., FALK T. M., Circumscribed palmar hypokeratosis induced by papilloma virus type 4, J Am Acad Dermatol, 2006, 54(5):908–909.
[34] REQUENA L., MANZARBEITIA F., MORENO C., IZQUIERDO M. J., PASTOR M. A., CARRASCO L., FARIÑA M. C., MARTÍN L., Olmsted syndrome: report of a case with study of the cellular proliferation in keratoderma, Am J Dermatopathol, 2001, 23(6):514–520.
[35] KURSCHAT P., HESS S., HUNZELMANN N., SCHARFFETTER-KOCHANEK K., Keratoacanthoma centrifugum marginatum accompanied by extensive granulomatous foreign body reaction, Dermatol Online J, 2005, 11(2):16.
[36] KOLDE G., BETHKE G., REICHART P. A., Epidermolytic alterations in focal palmoplantar and gingival keratosis, Am J Med Genet, 2001, 104(4):339–341.
[37] SCHMUTH M., YOSIPOVITCH G., WILLIAMS M. L., WEBER F., HINTNER H., ORTIZ-URDA S., RAPPERSBERGER K., CRUMRINE D., FEINGOLD K. R., ELIAS P. M., Pathogenesis of the permeability barrier abnormality in epidermolytic hyperkeratosis, J Invest Dermatol, 2001, 117(4):837–847.
[38] MÜLLER F. B., HUBER M., KINACIYAN T., HAUSSER I., SCHAFFRATH C., KRIEG T., HOHL D., KORGE B. P., ARIN M. J., A human keratin 10 knockout causes recessive epidermolytic hyperkeratosis, Hum Mol Genet, 2006, 15(17):1133–1141.
[39] CHASSAING N., KANITAKIS J., SPORTICH S., CORDIER- ALEX M. P., TITEUX M., CALVAS P., CLAUDY A., BERBIS P., HOVNANIAN A., Generalized epidermolytic hyperkeratosis in two unrelated children from parents with localized linear form, and prenatal diagnosis, J Invest Dermatol, 2006, 126(12):2715–2717.
[40] BERRYMAN J. L., NUTT T. J., GROO S. C., Painless genital papules and plaques, Dermatol Online J, 2008, 14(2):7.
[41] BAERT J. H., VEYS R. J., AMPE K., DE BOEVER J. A., The effect of sodium lauryl sulphate and triclosan on hamster cheek pouch mucosa, Int J Exp Pathol, 1996, 77(2):73–78.
[42] SATO A., SEIJI M., Electron microscopic observations of leukoplakia, Arch Derm Forsch, 1973, 247(3):211–220.
[43] POCK L., HERCOGOVÁ J., Incidental granular parakeratosis associated with dermatomyositis, Am J Dermatopathol, 2006, 28(2):147–149.
[44] GROSS G., PFISTER H., HAGEDORN M., GISSMANN L., Correlation between human papillomavirus (HPV) type and histology of warts, J Invest Dermatol, 1982, 78(2):160–164.
[45] GROSS G., JABLONSKA S., Skin warts: gross morphology and histology. In: GROSS G., VON KROGH G. (eds), Human papillomavirus infections in dermatovenereology, CRC Press Inc, Boca Raton, Florida, 1997, 244–258.
[46] RASHAD A. L., EVANS C. A., Histologic features of virus-rich and virus-poor Shope papillomas of cottontail rabbits, Cancer Res, 1967, 27(10):1855–1860.
Corresponding author Angel Fernandez-Flores, MD, PhD, S. Patología Celular, Clinica Ponferrada, Avenida Galicia 1, 24400 Ponferrada, Spain; Phone (00 34) 987 42 37 32, Fax (00 34) 987 42 91 02, e-mail: [email protected] Received: August 2nd, 2009
Accepted: October 15th, 2009





























