Embed Size (px)
Citation preview

Interventional Oncology Liver Directed TherapyAugust 24 2018
Ryan M Davis MD
Assistant Professor of Clinical Radiology
Vascular and Interventional Radiology
University of Missouri - Columbia
2
Disclosures
None
3
Liver Directed Therapy
- Thermal Ablation- Primary or metastatic lesions lt3cm
- Chemoembolization- Intermediate stage primary or metastatic disease- Bridge to transplant
- Y90 Radioembolization- Multifocal primary or metastatic disease- Bridge to transplant or resection
4
Effect of Heat on Soft Tissue
bull In thermal tumor ablation therapy energy is applied to heat and kills focal malignancies (coagulation necrosis)
bull Energy must be delivered throughout the lesion
5
gt105⁰C
60-100 ⁰C
46-52 ⁰C
Boiling vaporization and charring
(carbonization)
Near instantaneous protein coagulation leading
to coagulation necrosis
Irreversible cellular damage
Goldberg SN et al AJR Am J Roentgenol 2000 174(2)323-31
MICROWAVE SYSTEMS OVERVIEW
HOW MICROWAVE SYSTEMS WORK
bull Antenna(s) placed intonear targetbull Use CTUS guidance
bull Electromagnetic field (915 MHz or 245 GHz) rapidly oscillates water molecules generating heat
bull Electromagnetic field heatingThe electromagnetic field can penetrate all biologic tissues including dehydratedcharred tissue created during ablation
10
6
ENERGY CAN BE APPLIED CONTINUOUSLY DESPITE CHANGES IN TISSUE
EFFECTIVE IN ALL SOFT TISSUE TYPES
IMPROVED PERIVASCULAR PERFORMANCE VS RF = LESS HEAT SINK EFFECT
MICROWAVE SYSTEMS OVERVIEW
7
8
9
13mo Post MWA
10
TACE
bull Intermediate stage HCCbull Unresectable
bull Neuroendocrine Mets
bull mCRC (irinotecan)
bull Ocular Melanoma ()
bull Cholangiocarcinoma ()
bull RCC ()
11
Basics
bull Inoperable primary vs secondary hepatic tumorsbull Induces local ischemia and prolonged chemo exposure
to tumor
bull BCLC stage B (Extended for bridging to transplant or Stage C if local portal invasion)
bull Conventional TACE versus DEB-TACE
bull Efficacy for HCC confirmed with 2 randomized trials and several metaanalysis
bull Role for mCRC (irinotecan) reduced recently downgraded in NCCN guidelines to 3
12
Chemoembolization
bull Lancet 2002 May 18359(9319)1734-9
bull Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial
bull Llovet JM1 Real MI Montantildea X Planas R CollS Aponte J Ayuso C Sala M Muchart J Solagrave R RodeacutesJ Bruix J Barcelona Liver Cancer Group
bull Survival benefit at 1 and 2 years of 82 and 63 for chemoembolization and 63 and 27 for control
13
14
4mo Post TACE
15
Yttrium-90 Radioembolization
bull Hepatic mCRC
bull Non-resectable HCC
bull Cholangiocarcinoma
bull Breast CA mets
bull Neuroendocrine Tumor
16
About Yttrium 90 microspheres
bull Yttrium 90 is a pure beta emitter with a half life of 268 days or 642 hours
bull 94 of the radiation is decayed in 11 days
17
Rationale for SIRT
bull Preferential blood supply to tumorbull Parenchyma is 30 arterial and 70
portal supplybull Metastases are nearly 100 arterial
bull Preferential vasculaturebull Microvasculature of hepatic tumor is
3-200x more dense than surrounding normal parenchyma
bull CRC cells are radiosensitivebull Radiation works synergistically with
radiation-sensitizing chemotherapy drugs
bull Targeted to the tumorbull Allows treatment of multiple and
large tumors not amenable to external beam radiation therapy or ablation
18
Benefits of SIRT
bull Provide a localized radiation therapy delivering a dose of internal radiation up to 40x higher than conventional external beam therapy
bull Healthy liver tissue remain relatively unaffected2
bull 90 of patients experience ltGrade 3 adverse events
bull Outpatient Procedure
bull Typically involves two treatments over 6 weeks
bull Most patients return home 4-6 hours after the treatment
19
Products
bull Y-90 Glass Microspheres (TheraSpheres)bull 1999 granted Humanitarian Device Exemption for
use in unresectable HCC
bull Requires only safety not effectiveness data
bull Y-90 Resin Microspheres (Sir-Spheres)bull 2002 FDA grants Pre Market Approval for mCRC
bull Sufficient evidence that device is safe and effective for intended use
20
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48
Ryan M Davis MD
Assistant Professor of Clinical Radiology
Vascular and Interventional Radiology
University of Missouri - Columbia
2
Disclosures
None
3
Liver Directed Therapy
- Thermal Ablation- Primary or metastatic lesions lt3cm
- Chemoembolization- Intermediate stage primary or metastatic disease- Bridge to transplant
- Y90 Radioembolization- Multifocal primary or metastatic disease- Bridge to transplant or resection
4
Effect of Heat on Soft Tissue
bull In thermal tumor ablation therapy energy is applied to heat and kills focal malignancies (coagulation necrosis)
bull Energy must be delivered throughout the lesion
5
gt105⁰C
60-100 ⁰C
46-52 ⁰C
Boiling vaporization and charring
(carbonization)
Near instantaneous protein coagulation leading
to coagulation necrosis
Irreversible cellular damage
Goldberg SN et al AJR Am J Roentgenol 2000 174(2)323-31
MICROWAVE SYSTEMS OVERVIEW
HOW MICROWAVE SYSTEMS WORK
bull Antenna(s) placed intonear targetbull Use CTUS guidance
bull Electromagnetic field (915 MHz or 245 GHz) rapidly oscillates water molecules generating heat
bull Electromagnetic field heatingThe electromagnetic field can penetrate all biologic tissues including dehydratedcharred tissue created during ablation
10
6
ENERGY CAN BE APPLIED CONTINUOUSLY DESPITE CHANGES IN TISSUE
EFFECTIVE IN ALL SOFT TISSUE TYPES
IMPROVED PERIVASCULAR PERFORMANCE VS RF = LESS HEAT SINK EFFECT
MICROWAVE SYSTEMS OVERVIEW
7
8
9
13mo Post MWA
10
TACE
bull Intermediate stage HCCbull Unresectable
bull Neuroendocrine Mets
bull mCRC (irinotecan)
bull Ocular Melanoma ()
bull Cholangiocarcinoma ()
bull RCC ()
11
Basics
bull Inoperable primary vs secondary hepatic tumorsbull Induces local ischemia and prolonged chemo exposure
to tumor
bull BCLC stage B (Extended for bridging to transplant or Stage C if local portal invasion)
bull Conventional TACE versus DEB-TACE
bull Efficacy for HCC confirmed with 2 randomized trials and several metaanalysis
bull Role for mCRC (irinotecan) reduced recently downgraded in NCCN guidelines to 3
12
Chemoembolization
bull Lancet 2002 May 18359(9319)1734-9
bull Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial
bull Llovet JM1 Real MI Montantildea X Planas R CollS Aponte J Ayuso C Sala M Muchart J Solagrave R RodeacutesJ Bruix J Barcelona Liver Cancer Group
bull Survival benefit at 1 and 2 years of 82 and 63 for chemoembolization and 63 and 27 for control
13
14
4mo Post TACE
15
Yttrium-90 Radioembolization
bull Hepatic mCRC
bull Non-resectable HCC
bull Cholangiocarcinoma
bull Breast CA mets
bull Neuroendocrine Tumor
16
About Yttrium 90 microspheres
bull Yttrium 90 is a pure beta emitter with a half life of 268 days or 642 hours
bull 94 of the radiation is decayed in 11 days
17
Rationale for SIRT
bull Preferential blood supply to tumorbull Parenchyma is 30 arterial and 70
portal supplybull Metastases are nearly 100 arterial
bull Preferential vasculaturebull Microvasculature of hepatic tumor is
3-200x more dense than surrounding normal parenchyma
bull CRC cells are radiosensitivebull Radiation works synergistically with
radiation-sensitizing chemotherapy drugs
bull Targeted to the tumorbull Allows treatment of multiple and
large tumors not amenable to external beam radiation therapy or ablation
18
Benefits of SIRT
bull Provide a localized radiation therapy delivering a dose of internal radiation up to 40x higher than conventional external beam therapy
bull Healthy liver tissue remain relatively unaffected2
bull 90 of patients experience ltGrade 3 adverse events
bull Outpatient Procedure
bull Typically involves two treatments over 6 weeks
bull Most patients return home 4-6 hours after the treatment
19
Products
bull Y-90 Glass Microspheres (TheraSpheres)bull 1999 granted Humanitarian Device Exemption for
use in unresectable HCC
bull Requires only safety not effectiveness data
bull Y-90 Resin Microspheres (Sir-Spheres)bull 2002 FDA grants Pre Market Approval for mCRC
bull Sufficient evidence that device is safe and effective for intended use
20
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

Disclosures
None
3
Liver Directed Therapy
- Thermal Ablation- Primary or metastatic lesions lt3cm
- Chemoembolization- Intermediate stage primary or metastatic disease- Bridge to transplant
- Y90 Radioembolization- Multifocal primary or metastatic disease- Bridge to transplant or resection
4
Effect of Heat on Soft Tissue
bull In thermal tumor ablation therapy energy is applied to heat and kills focal malignancies (coagulation necrosis)
bull Energy must be delivered throughout the lesion
5
gt105⁰C
60-100 ⁰C
46-52 ⁰C
Boiling vaporization and charring
(carbonization)
Near instantaneous protein coagulation leading
to coagulation necrosis
Irreversible cellular damage
Goldberg SN et al AJR Am J Roentgenol 2000 174(2)323-31
MICROWAVE SYSTEMS OVERVIEW
HOW MICROWAVE SYSTEMS WORK
bull Antenna(s) placed intonear targetbull Use CTUS guidance
bull Electromagnetic field (915 MHz or 245 GHz) rapidly oscillates water molecules generating heat
bull Electromagnetic field heatingThe electromagnetic field can penetrate all biologic tissues including dehydratedcharred tissue created during ablation
10
6
ENERGY CAN BE APPLIED CONTINUOUSLY DESPITE CHANGES IN TISSUE
EFFECTIVE IN ALL SOFT TISSUE TYPES
IMPROVED PERIVASCULAR PERFORMANCE VS RF = LESS HEAT SINK EFFECT
MICROWAVE SYSTEMS OVERVIEW
7
8
9
13mo Post MWA
10
TACE
bull Intermediate stage HCCbull Unresectable
bull Neuroendocrine Mets
bull mCRC (irinotecan)
bull Ocular Melanoma ()
bull Cholangiocarcinoma ()
bull RCC ()
11
Basics
bull Inoperable primary vs secondary hepatic tumorsbull Induces local ischemia and prolonged chemo exposure
to tumor
bull BCLC stage B (Extended for bridging to transplant or Stage C if local portal invasion)
bull Conventional TACE versus DEB-TACE
bull Efficacy for HCC confirmed with 2 randomized trials and several metaanalysis
bull Role for mCRC (irinotecan) reduced recently downgraded in NCCN guidelines to 3
12
Chemoembolization
bull Lancet 2002 May 18359(9319)1734-9
bull Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial
bull Llovet JM1 Real MI Montantildea X Planas R CollS Aponte J Ayuso C Sala M Muchart J Solagrave R RodeacutesJ Bruix J Barcelona Liver Cancer Group
bull Survival benefit at 1 and 2 years of 82 and 63 for chemoembolization and 63 and 27 for control
13
14
4mo Post TACE
15
Yttrium-90 Radioembolization
bull Hepatic mCRC
bull Non-resectable HCC
bull Cholangiocarcinoma
bull Breast CA mets
bull Neuroendocrine Tumor
16
About Yttrium 90 microspheres
bull Yttrium 90 is a pure beta emitter with a half life of 268 days or 642 hours
bull 94 of the radiation is decayed in 11 days
17
Rationale for SIRT
bull Preferential blood supply to tumorbull Parenchyma is 30 arterial and 70
portal supplybull Metastases are nearly 100 arterial
bull Preferential vasculaturebull Microvasculature of hepatic tumor is
3-200x more dense than surrounding normal parenchyma
bull CRC cells are radiosensitivebull Radiation works synergistically with
radiation-sensitizing chemotherapy drugs
bull Targeted to the tumorbull Allows treatment of multiple and
large tumors not amenable to external beam radiation therapy or ablation
18
Benefits of SIRT
bull Provide a localized radiation therapy delivering a dose of internal radiation up to 40x higher than conventional external beam therapy
bull Healthy liver tissue remain relatively unaffected2
bull 90 of patients experience ltGrade 3 adverse events
bull Outpatient Procedure
bull Typically involves two treatments over 6 weeks
bull Most patients return home 4-6 hours after the treatment
19
Products
bull Y-90 Glass Microspheres (TheraSpheres)bull 1999 granted Humanitarian Device Exemption for
use in unresectable HCC
bull Requires only safety not effectiveness data
bull Y-90 Resin Microspheres (Sir-Spheres)bull 2002 FDA grants Pre Market Approval for mCRC
bull Sufficient evidence that device is safe and effective for intended use
20
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48
Liver Directed Therapy
- Thermal Ablation- Primary or metastatic lesions lt3cm
- Chemoembolization- Intermediate stage primary or metastatic disease- Bridge to transplant
- Y90 Radioembolization- Multifocal primary or metastatic disease- Bridge to transplant or resection
4
Effect of Heat on Soft Tissue
bull In thermal tumor ablation therapy energy is applied to heat and kills focal malignancies (coagulation necrosis)
bull Energy must be delivered throughout the lesion
5
gt105⁰C
60-100 ⁰C
46-52 ⁰C
Boiling vaporization and charring
(carbonization)
Near instantaneous protein coagulation leading
to coagulation necrosis
Irreversible cellular damage
Goldberg SN et al AJR Am J Roentgenol 2000 174(2)323-31
MICROWAVE SYSTEMS OVERVIEW
HOW MICROWAVE SYSTEMS WORK
bull Antenna(s) placed intonear targetbull Use CTUS guidance
bull Electromagnetic field (915 MHz or 245 GHz) rapidly oscillates water molecules generating heat
bull Electromagnetic field heatingThe electromagnetic field can penetrate all biologic tissues including dehydratedcharred tissue created during ablation
10
6
ENERGY CAN BE APPLIED CONTINUOUSLY DESPITE CHANGES IN TISSUE
EFFECTIVE IN ALL SOFT TISSUE TYPES
IMPROVED PERIVASCULAR PERFORMANCE VS RF = LESS HEAT SINK EFFECT
MICROWAVE SYSTEMS OVERVIEW
7
8
9
13mo Post MWA
10
TACE
bull Intermediate stage HCCbull Unresectable
bull Neuroendocrine Mets
bull mCRC (irinotecan)
bull Ocular Melanoma ()
bull Cholangiocarcinoma ()
bull RCC ()
11
Basics
bull Inoperable primary vs secondary hepatic tumorsbull Induces local ischemia and prolonged chemo exposure
to tumor
bull BCLC stage B (Extended for bridging to transplant or Stage C if local portal invasion)
bull Conventional TACE versus DEB-TACE
bull Efficacy for HCC confirmed with 2 randomized trials and several metaanalysis
bull Role for mCRC (irinotecan) reduced recently downgraded in NCCN guidelines to 3
12
Chemoembolization
bull Lancet 2002 May 18359(9319)1734-9
bull Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial
bull Llovet JM1 Real MI Montantildea X Planas R CollS Aponte J Ayuso C Sala M Muchart J Solagrave R RodeacutesJ Bruix J Barcelona Liver Cancer Group
bull Survival benefit at 1 and 2 years of 82 and 63 for chemoembolization and 63 and 27 for control
13
14
4mo Post TACE
15
Yttrium-90 Radioembolization
bull Hepatic mCRC
bull Non-resectable HCC
bull Cholangiocarcinoma
bull Breast CA mets
bull Neuroendocrine Tumor
16
About Yttrium 90 microspheres
bull Yttrium 90 is a pure beta emitter with a half life of 268 days or 642 hours
bull 94 of the radiation is decayed in 11 days
17
Rationale for SIRT
bull Preferential blood supply to tumorbull Parenchyma is 30 arterial and 70
portal supplybull Metastases are nearly 100 arterial
bull Preferential vasculaturebull Microvasculature of hepatic tumor is
3-200x more dense than surrounding normal parenchyma
bull CRC cells are radiosensitivebull Radiation works synergistically with
radiation-sensitizing chemotherapy drugs
bull Targeted to the tumorbull Allows treatment of multiple and
large tumors not amenable to external beam radiation therapy or ablation
18
Benefits of SIRT
bull Provide a localized radiation therapy delivering a dose of internal radiation up to 40x higher than conventional external beam therapy
bull Healthy liver tissue remain relatively unaffected2
bull 90 of patients experience ltGrade 3 adverse events
bull Outpatient Procedure
bull Typically involves two treatments over 6 weeks
bull Most patients return home 4-6 hours after the treatment
19
Products
bull Y-90 Glass Microspheres (TheraSpheres)bull 1999 granted Humanitarian Device Exemption for
use in unresectable HCC
bull Requires only safety not effectiveness data
bull Y-90 Resin Microspheres (Sir-Spheres)bull 2002 FDA grants Pre Market Approval for mCRC
bull Sufficient evidence that device is safe and effective for intended use
20
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

Effect of Heat on Soft Tissue
bull In thermal tumor ablation therapy energy is applied to heat and kills focal malignancies (coagulation necrosis)
bull Energy must be delivered throughout the lesion
5
gt105⁰C
60-100 ⁰C
46-52 ⁰C
Boiling vaporization and charring
(carbonization)
Near instantaneous protein coagulation leading
to coagulation necrosis
Irreversible cellular damage
Goldberg SN et al AJR Am J Roentgenol 2000 174(2)323-31
MICROWAVE SYSTEMS OVERVIEW
HOW MICROWAVE SYSTEMS WORK
bull Antenna(s) placed intonear targetbull Use CTUS guidance
bull Electromagnetic field (915 MHz or 245 GHz) rapidly oscillates water molecules generating heat
bull Electromagnetic field heatingThe electromagnetic field can penetrate all biologic tissues including dehydratedcharred tissue created during ablation
10
6
ENERGY CAN BE APPLIED CONTINUOUSLY DESPITE CHANGES IN TISSUE
EFFECTIVE IN ALL SOFT TISSUE TYPES
IMPROVED PERIVASCULAR PERFORMANCE VS RF = LESS HEAT SINK EFFECT
MICROWAVE SYSTEMS OVERVIEW
7
8
9
13mo Post MWA
10
TACE
bull Intermediate stage HCCbull Unresectable
bull Neuroendocrine Mets
bull mCRC (irinotecan)
bull Ocular Melanoma ()
bull Cholangiocarcinoma ()
bull RCC ()
11
Basics
bull Inoperable primary vs secondary hepatic tumorsbull Induces local ischemia and prolonged chemo exposure
to tumor
bull BCLC stage B (Extended for bridging to transplant or Stage C if local portal invasion)
bull Conventional TACE versus DEB-TACE
bull Efficacy for HCC confirmed with 2 randomized trials and several metaanalysis
bull Role for mCRC (irinotecan) reduced recently downgraded in NCCN guidelines to 3
12
Chemoembolization
bull Lancet 2002 May 18359(9319)1734-9
bull Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial
bull Llovet JM1 Real MI Montantildea X Planas R CollS Aponte J Ayuso C Sala M Muchart J Solagrave R RodeacutesJ Bruix J Barcelona Liver Cancer Group
bull Survival benefit at 1 and 2 years of 82 and 63 for chemoembolization and 63 and 27 for control
13
14
4mo Post TACE
15
Yttrium-90 Radioembolization
bull Hepatic mCRC
bull Non-resectable HCC
bull Cholangiocarcinoma
bull Breast CA mets
bull Neuroendocrine Tumor
16
About Yttrium 90 microspheres
bull Yttrium 90 is a pure beta emitter with a half life of 268 days or 642 hours
bull 94 of the radiation is decayed in 11 days
17
Rationale for SIRT
bull Preferential blood supply to tumorbull Parenchyma is 30 arterial and 70
portal supplybull Metastases are nearly 100 arterial
bull Preferential vasculaturebull Microvasculature of hepatic tumor is
3-200x more dense than surrounding normal parenchyma
bull CRC cells are radiosensitivebull Radiation works synergistically with
radiation-sensitizing chemotherapy drugs
bull Targeted to the tumorbull Allows treatment of multiple and
large tumors not amenable to external beam radiation therapy or ablation
18
Benefits of SIRT
bull Provide a localized radiation therapy delivering a dose of internal radiation up to 40x higher than conventional external beam therapy
bull Healthy liver tissue remain relatively unaffected2
bull 90 of patients experience ltGrade 3 adverse events
bull Outpatient Procedure
bull Typically involves two treatments over 6 weeks
bull Most patients return home 4-6 hours after the treatment
19
Products
bull Y-90 Glass Microspheres (TheraSpheres)bull 1999 granted Humanitarian Device Exemption for
use in unresectable HCC
bull Requires only safety not effectiveness data
bull Y-90 Resin Microspheres (Sir-Spheres)bull 2002 FDA grants Pre Market Approval for mCRC
bull Sufficient evidence that device is safe and effective for intended use
20
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48
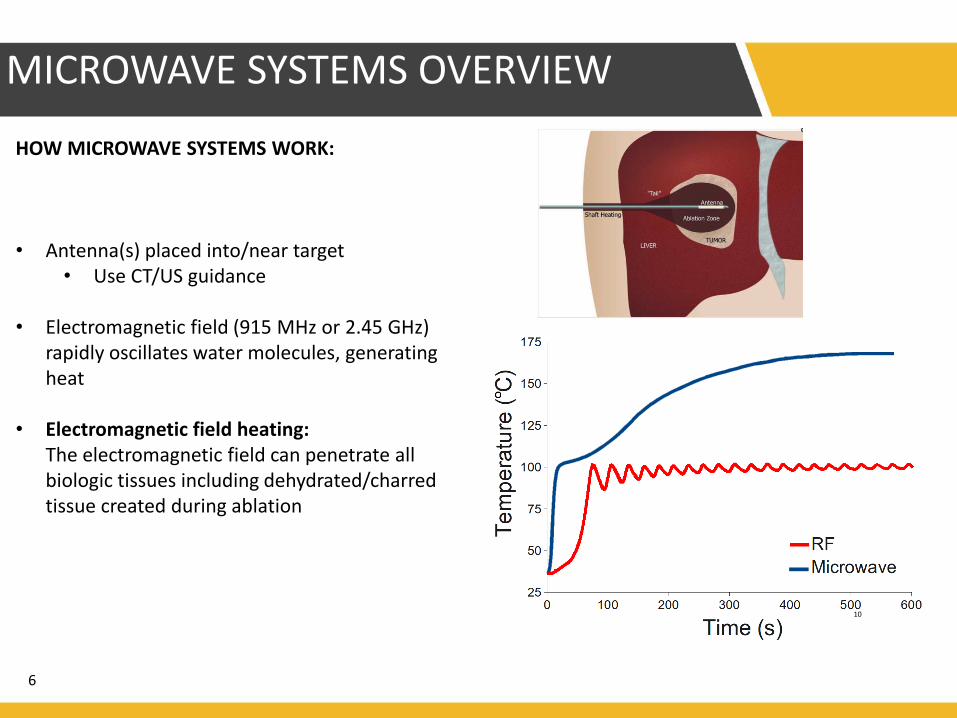
MICROWAVE SYSTEMS OVERVIEW
HOW MICROWAVE SYSTEMS WORK
bull Antenna(s) placed intonear targetbull Use CTUS guidance
bull Electromagnetic field (915 MHz or 245 GHz) rapidly oscillates water molecules generating heat
bull Electromagnetic field heatingThe electromagnetic field can penetrate all biologic tissues including dehydratedcharred tissue created during ablation
10
6
ENERGY CAN BE APPLIED CONTINUOUSLY DESPITE CHANGES IN TISSUE
EFFECTIVE IN ALL SOFT TISSUE TYPES
IMPROVED PERIVASCULAR PERFORMANCE VS RF = LESS HEAT SINK EFFECT
MICROWAVE SYSTEMS OVERVIEW
7
8
9
13mo Post MWA
10
TACE
bull Intermediate stage HCCbull Unresectable
bull Neuroendocrine Mets
bull mCRC (irinotecan)
bull Ocular Melanoma ()
bull Cholangiocarcinoma ()
bull RCC ()
11
Basics
bull Inoperable primary vs secondary hepatic tumorsbull Induces local ischemia and prolonged chemo exposure
to tumor
bull BCLC stage B (Extended for bridging to transplant or Stage C if local portal invasion)
bull Conventional TACE versus DEB-TACE
bull Efficacy for HCC confirmed with 2 randomized trials and several metaanalysis
bull Role for mCRC (irinotecan) reduced recently downgraded in NCCN guidelines to 3
12
Chemoembolization
bull Lancet 2002 May 18359(9319)1734-9
bull Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial
bull Llovet JM1 Real MI Montantildea X Planas R CollS Aponte J Ayuso C Sala M Muchart J Solagrave R RodeacutesJ Bruix J Barcelona Liver Cancer Group
bull Survival benefit at 1 and 2 years of 82 and 63 for chemoembolization and 63 and 27 for control
13
14
4mo Post TACE
15
Yttrium-90 Radioembolization
bull Hepatic mCRC
bull Non-resectable HCC
bull Cholangiocarcinoma
bull Breast CA mets
bull Neuroendocrine Tumor
16
About Yttrium 90 microspheres
bull Yttrium 90 is a pure beta emitter with a half life of 268 days or 642 hours
bull 94 of the radiation is decayed in 11 days
17
Rationale for SIRT
bull Preferential blood supply to tumorbull Parenchyma is 30 arterial and 70
portal supplybull Metastases are nearly 100 arterial
bull Preferential vasculaturebull Microvasculature of hepatic tumor is
3-200x more dense than surrounding normal parenchyma
bull CRC cells are radiosensitivebull Radiation works synergistically with
radiation-sensitizing chemotherapy drugs
bull Targeted to the tumorbull Allows treatment of multiple and
large tumors not amenable to external beam radiation therapy or ablation
18
Benefits of SIRT
bull Provide a localized radiation therapy delivering a dose of internal radiation up to 40x higher than conventional external beam therapy
bull Healthy liver tissue remain relatively unaffected2
bull 90 of patients experience ltGrade 3 adverse events
bull Outpatient Procedure
bull Typically involves two treatments over 6 weeks
bull Most patients return home 4-6 hours after the treatment
19
Products
bull Y-90 Glass Microspheres (TheraSpheres)bull 1999 granted Humanitarian Device Exemption for
use in unresectable HCC
bull Requires only safety not effectiveness data
bull Y-90 Resin Microspheres (Sir-Spheres)bull 2002 FDA grants Pre Market Approval for mCRC
bull Sufficient evidence that device is safe and effective for intended use
20
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

ENERGY CAN BE APPLIED CONTINUOUSLY DESPITE CHANGES IN TISSUE
EFFECTIVE IN ALL SOFT TISSUE TYPES
IMPROVED PERIVASCULAR PERFORMANCE VS RF = LESS HEAT SINK EFFECT
MICROWAVE SYSTEMS OVERVIEW
7
8
9
13mo Post MWA
10
TACE
bull Intermediate stage HCCbull Unresectable
bull Neuroendocrine Mets
bull mCRC (irinotecan)
bull Ocular Melanoma ()
bull Cholangiocarcinoma ()
bull RCC ()
11
Basics
bull Inoperable primary vs secondary hepatic tumorsbull Induces local ischemia and prolonged chemo exposure
to tumor
bull BCLC stage B (Extended for bridging to transplant or Stage C if local portal invasion)
bull Conventional TACE versus DEB-TACE
bull Efficacy for HCC confirmed with 2 randomized trials and several metaanalysis
bull Role for mCRC (irinotecan) reduced recently downgraded in NCCN guidelines to 3
12
Chemoembolization
bull Lancet 2002 May 18359(9319)1734-9
bull Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial
bull Llovet JM1 Real MI Montantildea X Planas R CollS Aponte J Ayuso C Sala M Muchart J Solagrave R RodeacutesJ Bruix J Barcelona Liver Cancer Group
bull Survival benefit at 1 and 2 years of 82 and 63 for chemoembolization and 63 and 27 for control
13
14
4mo Post TACE
15
Yttrium-90 Radioembolization
bull Hepatic mCRC
bull Non-resectable HCC
bull Cholangiocarcinoma
bull Breast CA mets
bull Neuroendocrine Tumor
16
About Yttrium 90 microspheres
bull Yttrium 90 is a pure beta emitter with a half life of 268 days or 642 hours
bull 94 of the radiation is decayed in 11 days
17
Rationale for SIRT
bull Preferential blood supply to tumorbull Parenchyma is 30 arterial and 70
portal supplybull Metastases are nearly 100 arterial
bull Preferential vasculaturebull Microvasculature of hepatic tumor is
3-200x more dense than surrounding normal parenchyma
bull CRC cells are radiosensitivebull Radiation works synergistically with
radiation-sensitizing chemotherapy drugs
bull Targeted to the tumorbull Allows treatment of multiple and
large tumors not amenable to external beam radiation therapy or ablation
18
Benefits of SIRT
bull Provide a localized radiation therapy delivering a dose of internal radiation up to 40x higher than conventional external beam therapy
bull Healthy liver tissue remain relatively unaffected2
bull 90 of patients experience ltGrade 3 adverse events
bull Outpatient Procedure
bull Typically involves two treatments over 6 weeks
bull Most patients return home 4-6 hours after the treatment
19
Products
bull Y-90 Glass Microspheres (TheraSpheres)bull 1999 granted Humanitarian Device Exemption for
use in unresectable HCC
bull Requires only safety not effectiveness data
bull Y-90 Resin Microspheres (Sir-Spheres)bull 2002 FDA grants Pre Market Approval for mCRC
bull Sufficient evidence that device is safe and effective for intended use
20
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48
8
9
13mo Post MWA
10
TACE
bull Intermediate stage HCCbull Unresectable
bull Neuroendocrine Mets
bull mCRC (irinotecan)
bull Ocular Melanoma ()
bull Cholangiocarcinoma ()
bull RCC ()
11
Basics
bull Inoperable primary vs secondary hepatic tumorsbull Induces local ischemia and prolonged chemo exposure
to tumor
bull BCLC stage B (Extended for bridging to transplant or Stage C if local portal invasion)
bull Conventional TACE versus DEB-TACE
bull Efficacy for HCC confirmed with 2 randomized trials and several metaanalysis
bull Role for mCRC (irinotecan) reduced recently downgraded in NCCN guidelines to 3
12
Chemoembolization
bull Lancet 2002 May 18359(9319)1734-9
bull Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial
bull Llovet JM1 Real MI Montantildea X Planas R CollS Aponte J Ayuso C Sala M Muchart J Solagrave R RodeacutesJ Bruix J Barcelona Liver Cancer Group
bull Survival benefit at 1 and 2 years of 82 and 63 for chemoembolization and 63 and 27 for control
13
14
4mo Post TACE
15
Yttrium-90 Radioembolization
bull Hepatic mCRC
bull Non-resectable HCC
bull Cholangiocarcinoma
bull Breast CA mets
bull Neuroendocrine Tumor
16
About Yttrium 90 microspheres
bull Yttrium 90 is a pure beta emitter with a half life of 268 days or 642 hours
bull 94 of the radiation is decayed in 11 days
17
Rationale for SIRT
bull Preferential blood supply to tumorbull Parenchyma is 30 arterial and 70
portal supplybull Metastases are nearly 100 arterial
bull Preferential vasculaturebull Microvasculature of hepatic tumor is
3-200x more dense than surrounding normal parenchyma
bull CRC cells are radiosensitivebull Radiation works synergistically with
radiation-sensitizing chemotherapy drugs
bull Targeted to the tumorbull Allows treatment of multiple and
large tumors not amenable to external beam radiation therapy or ablation
18
Benefits of SIRT
bull Provide a localized radiation therapy delivering a dose of internal radiation up to 40x higher than conventional external beam therapy
bull Healthy liver tissue remain relatively unaffected2
bull 90 of patients experience ltGrade 3 adverse events
bull Outpatient Procedure
bull Typically involves two treatments over 6 weeks
bull Most patients return home 4-6 hours after the treatment
19
Products
bull Y-90 Glass Microspheres (TheraSpheres)bull 1999 granted Humanitarian Device Exemption for
use in unresectable HCC
bull Requires only safety not effectiveness data
bull Y-90 Resin Microspheres (Sir-Spheres)bull 2002 FDA grants Pre Market Approval for mCRC
bull Sufficient evidence that device is safe and effective for intended use
20
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

9
13mo Post MWA
10
TACE
bull Intermediate stage HCCbull Unresectable
bull Neuroendocrine Mets
bull mCRC (irinotecan)
bull Ocular Melanoma ()
bull Cholangiocarcinoma ()
bull RCC ()
11
Basics
bull Inoperable primary vs secondary hepatic tumorsbull Induces local ischemia and prolonged chemo exposure
to tumor
bull BCLC stage B (Extended for bridging to transplant or Stage C if local portal invasion)
bull Conventional TACE versus DEB-TACE
bull Efficacy for HCC confirmed with 2 randomized trials and several metaanalysis
bull Role for mCRC (irinotecan) reduced recently downgraded in NCCN guidelines to 3
12
Chemoembolization
bull Lancet 2002 May 18359(9319)1734-9
bull Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial
bull Llovet JM1 Real MI Montantildea X Planas R CollS Aponte J Ayuso C Sala M Muchart J Solagrave R RodeacutesJ Bruix J Barcelona Liver Cancer Group
bull Survival benefit at 1 and 2 years of 82 and 63 for chemoembolization and 63 and 27 for control
13
14
4mo Post TACE
15
Yttrium-90 Radioembolization
bull Hepatic mCRC
bull Non-resectable HCC
bull Cholangiocarcinoma
bull Breast CA mets
bull Neuroendocrine Tumor
16
About Yttrium 90 microspheres
bull Yttrium 90 is a pure beta emitter with a half life of 268 days or 642 hours
bull 94 of the radiation is decayed in 11 days
17
Rationale for SIRT
bull Preferential blood supply to tumorbull Parenchyma is 30 arterial and 70
portal supplybull Metastases are nearly 100 arterial
bull Preferential vasculaturebull Microvasculature of hepatic tumor is
3-200x more dense than surrounding normal parenchyma
bull CRC cells are radiosensitivebull Radiation works synergistically with
radiation-sensitizing chemotherapy drugs
bull Targeted to the tumorbull Allows treatment of multiple and
large tumors not amenable to external beam radiation therapy or ablation
18
Benefits of SIRT
bull Provide a localized radiation therapy delivering a dose of internal radiation up to 40x higher than conventional external beam therapy
bull Healthy liver tissue remain relatively unaffected2
bull 90 of patients experience ltGrade 3 adverse events
bull Outpatient Procedure
bull Typically involves two treatments over 6 weeks
bull Most patients return home 4-6 hours after the treatment
19
Products
bull Y-90 Glass Microspheres (TheraSpheres)bull 1999 granted Humanitarian Device Exemption for
use in unresectable HCC
bull Requires only safety not effectiveness data
bull Y-90 Resin Microspheres (Sir-Spheres)bull 2002 FDA grants Pre Market Approval for mCRC
bull Sufficient evidence that device is safe and effective for intended use
20
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

13mo Post MWA
10
TACE
bull Intermediate stage HCCbull Unresectable
bull Neuroendocrine Mets
bull mCRC (irinotecan)
bull Ocular Melanoma ()
bull Cholangiocarcinoma ()
bull RCC ()
11
Basics
bull Inoperable primary vs secondary hepatic tumorsbull Induces local ischemia and prolonged chemo exposure
to tumor
bull BCLC stage B (Extended for bridging to transplant or Stage C if local portal invasion)
bull Conventional TACE versus DEB-TACE
bull Efficacy for HCC confirmed with 2 randomized trials and several metaanalysis
bull Role for mCRC (irinotecan) reduced recently downgraded in NCCN guidelines to 3
12
Chemoembolization
bull Lancet 2002 May 18359(9319)1734-9
bull Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial
bull Llovet JM1 Real MI Montantildea X Planas R CollS Aponte J Ayuso C Sala M Muchart J Solagrave R RodeacutesJ Bruix J Barcelona Liver Cancer Group
bull Survival benefit at 1 and 2 years of 82 and 63 for chemoembolization and 63 and 27 for control
13
14
4mo Post TACE
15
Yttrium-90 Radioembolization
bull Hepatic mCRC
bull Non-resectable HCC
bull Cholangiocarcinoma
bull Breast CA mets
bull Neuroendocrine Tumor
16
About Yttrium 90 microspheres
bull Yttrium 90 is a pure beta emitter with a half life of 268 days or 642 hours
bull 94 of the radiation is decayed in 11 days
17
Rationale for SIRT
bull Preferential blood supply to tumorbull Parenchyma is 30 arterial and 70
portal supplybull Metastases are nearly 100 arterial
bull Preferential vasculaturebull Microvasculature of hepatic tumor is
3-200x more dense than surrounding normal parenchyma
bull CRC cells are radiosensitivebull Radiation works synergistically with
radiation-sensitizing chemotherapy drugs
bull Targeted to the tumorbull Allows treatment of multiple and
large tumors not amenable to external beam radiation therapy or ablation
18
Benefits of SIRT
bull Provide a localized radiation therapy delivering a dose of internal radiation up to 40x higher than conventional external beam therapy
bull Healthy liver tissue remain relatively unaffected2
bull 90 of patients experience ltGrade 3 adverse events
bull Outpatient Procedure
bull Typically involves two treatments over 6 weeks
bull Most patients return home 4-6 hours after the treatment
19
Products
bull Y-90 Glass Microspheres (TheraSpheres)bull 1999 granted Humanitarian Device Exemption for
use in unresectable HCC
bull Requires only safety not effectiveness data
bull Y-90 Resin Microspheres (Sir-Spheres)bull 2002 FDA grants Pre Market Approval for mCRC
bull Sufficient evidence that device is safe and effective for intended use
20
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

TACE
bull Intermediate stage HCCbull Unresectable
bull Neuroendocrine Mets
bull mCRC (irinotecan)
bull Ocular Melanoma ()
bull Cholangiocarcinoma ()
bull RCC ()
11
Basics
bull Inoperable primary vs secondary hepatic tumorsbull Induces local ischemia and prolonged chemo exposure
to tumor
bull BCLC stage B (Extended for bridging to transplant or Stage C if local portal invasion)
bull Conventional TACE versus DEB-TACE
bull Efficacy for HCC confirmed with 2 randomized trials and several metaanalysis
bull Role for mCRC (irinotecan) reduced recently downgraded in NCCN guidelines to 3
12
Chemoembolization
bull Lancet 2002 May 18359(9319)1734-9
bull Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial
bull Llovet JM1 Real MI Montantildea X Planas R CollS Aponte J Ayuso C Sala M Muchart J Solagrave R RodeacutesJ Bruix J Barcelona Liver Cancer Group
bull Survival benefit at 1 and 2 years of 82 and 63 for chemoembolization and 63 and 27 for control
13
14
4mo Post TACE
15
Yttrium-90 Radioembolization
bull Hepatic mCRC
bull Non-resectable HCC
bull Cholangiocarcinoma
bull Breast CA mets
bull Neuroendocrine Tumor
16
About Yttrium 90 microspheres
bull Yttrium 90 is a pure beta emitter with a half life of 268 days or 642 hours
bull 94 of the radiation is decayed in 11 days
17
Rationale for SIRT
bull Preferential blood supply to tumorbull Parenchyma is 30 arterial and 70
portal supplybull Metastases are nearly 100 arterial
bull Preferential vasculaturebull Microvasculature of hepatic tumor is
3-200x more dense than surrounding normal parenchyma
bull CRC cells are radiosensitivebull Radiation works synergistically with
radiation-sensitizing chemotherapy drugs
bull Targeted to the tumorbull Allows treatment of multiple and
large tumors not amenable to external beam radiation therapy or ablation
18
Benefits of SIRT
bull Provide a localized radiation therapy delivering a dose of internal radiation up to 40x higher than conventional external beam therapy
bull Healthy liver tissue remain relatively unaffected2
bull 90 of patients experience ltGrade 3 adverse events
bull Outpatient Procedure
bull Typically involves two treatments over 6 weeks
bull Most patients return home 4-6 hours after the treatment
19
Products
bull Y-90 Glass Microspheres (TheraSpheres)bull 1999 granted Humanitarian Device Exemption for
use in unresectable HCC
bull Requires only safety not effectiveness data
bull Y-90 Resin Microspheres (Sir-Spheres)bull 2002 FDA grants Pre Market Approval for mCRC
bull Sufficient evidence that device is safe and effective for intended use
20
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

Basics
bull Inoperable primary vs secondary hepatic tumorsbull Induces local ischemia and prolonged chemo exposure
to tumor
bull BCLC stage B (Extended for bridging to transplant or Stage C if local portal invasion)
bull Conventional TACE versus DEB-TACE
bull Efficacy for HCC confirmed with 2 randomized trials and several metaanalysis
bull Role for mCRC (irinotecan) reduced recently downgraded in NCCN guidelines to 3
12
Chemoembolization
bull Lancet 2002 May 18359(9319)1734-9
bull Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial
bull Llovet JM1 Real MI Montantildea X Planas R CollS Aponte J Ayuso C Sala M Muchart J Solagrave R RodeacutesJ Bruix J Barcelona Liver Cancer Group
bull Survival benefit at 1 and 2 years of 82 and 63 for chemoembolization and 63 and 27 for control
13
14
4mo Post TACE
15
Yttrium-90 Radioembolization
bull Hepatic mCRC
bull Non-resectable HCC
bull Cholangiocarcinoma
bull Breast CA mets
bull Neuroendocrine Tumor
16
About Yttrium 90 microspheres
bull Yttrium 90 is a pure beta emitter with a half life of 268 days or 642 hours
bull 94 of the radiation is decayed in 11 days
17
Rationale for SIRT
bull Preferential blood supply to tumorbull Parenchyma is 30 arterial and 70
portal supplybull Metastases are nearly 100 arterial
bull Preferential vasculaturebull Microvasculature of hepatic tumor is
3-200x more dense than surrounding normal parenchyma
bull CRC cells are radiosensitivebull Radiation works synergistically with
radiation-sensitizing chemotherapy drugs
bull Targeted to the tumorbull Allows treatment of multiple and
large tumors not amenable to external beam radiation therapy or ablation
18
Benefits of SIRT
bull Provide a localized radiation therapy delivering a dose of internal radiation up to 40x higher than conventional external beam therapy
bull Healthy liver tissue remain relatively unaffected2
bull 90 of patients experience ltGrade 3 adverse events
bull Outpatient Procedure
bull Typically involves two treatments over 6 weeks
bull Most patients return home 4-6 hours after the treatment
19
Products
bull Y-90 Glass Microspheres (TheraSpheres)bull 1999 granted Humanitarian Device Exemption for
use in unresectable HCC
bull Requires only safety not effectiveness data
bull Y-90 Resin Microspheres (Sir-Spheres)bull 2002 FDA grants Pre Market Approval for mCRC
bull Sufficient evidence that device is safe and effective for intended use
20
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

Chemoembolization
bull Lancet 2002 May 18359(9319)1734-9
bull Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial
bull Llovet JM1 Real MI Montantildea X Planas R CollS Aponte J Ayuso C Sala M Muchart J Solagrave R RodeacutesJ Bruix J Barcelona Liver Cancer Group
bull Survival benefit at 1 and 2 years of 82 and 63 for chemoembolization and 63 and 27 for control
13
14
4mo Post TACE
15
Yttrium-90 Radioembolization
bull Hepatic mCRC
bull Non-resectable HCC
bull Cholangiocarcinoma
bull Breast CA mets
bull Neuroendocrine Tumor
16
About Yttrium 90 microspheres
bull Yttrium 90 is a pure beta emitter with a half life of 268 days or 642 hours
bull 94 of the radiation is decayed in 11 days
17
Rationale for SIRT
bull Preferential blood supply to tumorbull Parenchyma is 30 arterial and 70
portal supplybull Metastases are nearly 100 arterial
bull Preferential vasculaturebull Microvasculature of hepatic tumor is
3-200x more dense than surrounding normal parenchyma
bull CRC cells are radiosensitivebull Radiation works synergistically with
radiation-sensitizing chemotherapy drugs
bull Targeted to the tumorbull Allows treatment of multiple and
large tumors not amenable to external beam radiation therapy or ablation
18
Benefits of SIRT
bull Provide a localized radiation therapy delivering a dose of internal radiation up to 40x higher than conventional external beam therapy
bull Healthy liver tissue remain relatively unaffected2
bull 90 of patients experience ltGrade 3 adverse events
bull Outpatient Procedure
bull Typically involves two treatments over 6 weeks
bull Most patients return home 4-6 hours after the treatment
19
Products
bull Y-90 Glass Microspheres (TheraSpheres)bull 1999 granted Humanitarian Device Exemption for
use in unresectable HCC
bull Requires only safety not effectiveness data
bull Y-90 Resin Microspheres (Sir-Spheres)bull 2002 FDA grants Pre Market Approval for mCRC
bull Sufficient evidence that device is safe and effective for intended use
20
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

14
4mo Post TACE
15
Yttrium-90 Radioembolization
bull Hepatic mCRC
bull Non-resectable HCC
bull Cholangiocarcinoma
bull Breast CA mets
bull Neuroendocrine Tumor
16
About Yttrium 90 microspheres
bull Yttrium 90 is a pure beta emitter with a half life of 268 days or 642 hours
bull 94 of the radiation is decayed in 11 days
17
Rationale for SIRT
bull Preferential blood supply to tumorbull Parenchyma is 30 arterial and 70
portal supplybull Metastases are nearly 100 arterial
bull Preferential vasculaturebull Microvasculature of hepatic tumor is
3-200x more dense than surrounding normal parenchyma
bull CRC cells are radiosensitivebull Radiation works synergistically with
radiation-sensitizing chemotherapy drugs
bull Targeted to the tumorbull Allows treatment of multiple and
large tumors not amenable to external beam radiation therapy or ablation
18
Benefits of SIRT
bull Provide a localized radiation therapy delivering a dose of internal radiation up to 40x higher than conventional external beam therapy
bull Healthy liver tissue remain relatively unaffected2
bull 90 of patients experience ltGrade 3 adverse events
bull Outpatient Procedure
bull Typically involves two treatments over 6 weeks
bull Most patients return home 4-6 hours after the treatment
19
Products
bull Y-90 Glass Microspheres (TheraSpheres)bull 1999 granted Humanitarian Device Exemption for
use in unresectable HCC
bull Requires only safety not effectiveness data
bull Y-90 Resin Microspheres (Sir-Spheres)bull 2002 FDA grants Pre Market Approval for mCRC
bull Sufficient evidence that device is safe and effective for intended use
20
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48
4mo Post TACE
15
Yttrium-90 Radioembolization
bull Hepatic mCRC
bull Non-resectable HCC
bull Cholangiocarcinoma
bull Breast CA mets
bull Neuroendocrine Tumor
16
About Yttrium 90 microspheres
bull Yttrium 90 is a pure beta emitter with a half life of 268 days or 642 hours
bull 94 of the radiation is decayed in 11 days
17
Rationale for SIRT
bull Preferential blood supply to tumorbull Parenchyma is 30 arterial and 70
portal supplybull Metastases are nearly 100 arterial
bull Preferential vasculaturebull Microvasculature of hepatic tumor is
3-200x more dense than surrounding normal parenchyma
bull CRC cells are radiosensitivebull Radiation works synergistically with
radiation-sensitizing chemotherapy drugs
bull Targeted to the tumorbull Allows treatment of multiple and
large tumors not amenable to external beam radiation therapy or ablation
18
Benefits of SIRT
bull Provide a localized radiation therapy delivering a dose of internal radiation up to 40x higher than conventional external beam therapy
bull Healthy liver tissue remain relatively unaffected2
bull 90 of patients experience ltGrade 3 adverse events
bull Outpatient Procedure
bull Typically involves two treatments over 6 weeks
bull Most patients return home 4-6 hours after the treatment
19
Products
bull Y-90 Glass Microspheres (TheraSpheres)bull 1999 granted Humanitarian Device Exemption for
use in unresectable HCC
bull Requires only safety not effectiveness data
bull Y-90 Resin Microspheres (Sir-Spheres)bull 2002 FDA grants Pre Market Approval for mCRC
bull Sufficient evidence that device is safe and effective for intended use
20
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48
Yttrium-90 Radioembolization
bull Hepatic mCRC
bull Non-resectable HCC
bull Cholangiocarcinoma
bull Breast CA mets
bull Neuroendocrine Tumor
16
About Yttrium 90 microspheres
bull Yttrium 90 is a pure beta emitter with a half life of 268 days or 642 hours
bull 94 of the radiation is decayed in 11 days
17
Rationale for SIRT
bull Preferential blood supply to tumorbull Parenchyma is 30 arterial and 70
portal supplybull Metastases are nearly 100 arterial
bull Preferential vasculaturebull Microvasculature of hepatic tumor is
3-200x more dense than surrounding normal parenchyma
bull CRC cells are radiosensitivebull Radiation works synergistically with
radiation-sensitizing chemotherapy drugs
bull Targeted to the tumorbull Allows treatment of multiple and
large tumors not amenable to external beam radiation therapy or ablation
18
Benefits of SIRT
bull Provide a localized radiation therapy delivering a dose of internal radiation up to 40x higher than conventional external beam therapy
bull Healthy liver tissue remain relatively unaffected2
bull 90 of patients experience ltGrade 3 adverse events
bull Outpatient Procedure
bull Typically involves two treatments over 6 weeks
bull Most patients return home 4-6 hours after the treatment
19
Products
bull Y-90 Glass Microspheres (TheraSpheres)bull 1999 granted Humanitarian Device Exemption for
use in unresectable HCC
bull Requires only safety not effectiveness data
bull Y-90 Resin Microspheres (Sir-Spheres)bull 2002 FDA grants Pre Market Approval for mCRC
bull Sufficient evidence that device is safe and effective for intended use
20
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

About Yttrium 90 microspheres
bull Yttrium 90 is a pure beta emitter with a half life of 268 days or 642 hours
bull 94 of the radiation is decayed in 11 days
17
Rationale for SIRT
bull Preferential blood supply to tumorbull Parenchyma is 30 arterial and 70
portal supplybull Metastases are nearly 100 arterial
bull Preferential vasculaturebull Microvasculature of hepatic tumor is
3-200x more dense than surrounding normal parenchyma
bull CRC cells are radiosensitivebull Radiation works synergistically with
radiation-sensitizing chemotherapy drugs
bull Targeted to the tumorbull Allows treatment of multiple and
large tumors not amenable to external beam radiation therapy or ablation
18
Benefits of SIRT
bull Provide a localized radiation therapy delivering a dose of internal radiation up to 40x higher than conventional external beam therapy
bull Healthy liver tissue remain relatively unaffected2
bull 90 of patients experience ltGrade 3 adverse events
bull Outpatient Procedure
bull Typically involves two treatments over 6 weeks
bull Most patients return home 4-6 hours after the treatment
19
Products
bull Y-90 Glass Microspheres (TheraSpheres)bull 1999 granted Humanitarian Device Exemption for
use in unresectable HCC
bull Requires only safety not effectiveness data
bull Y-90 Resin Microspheres (Sir-Spheres)bull 2002 FDA grants Pre Market Approval for mCRC
bull Sufficient evidence that device is safe and effective for intended use
20
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48
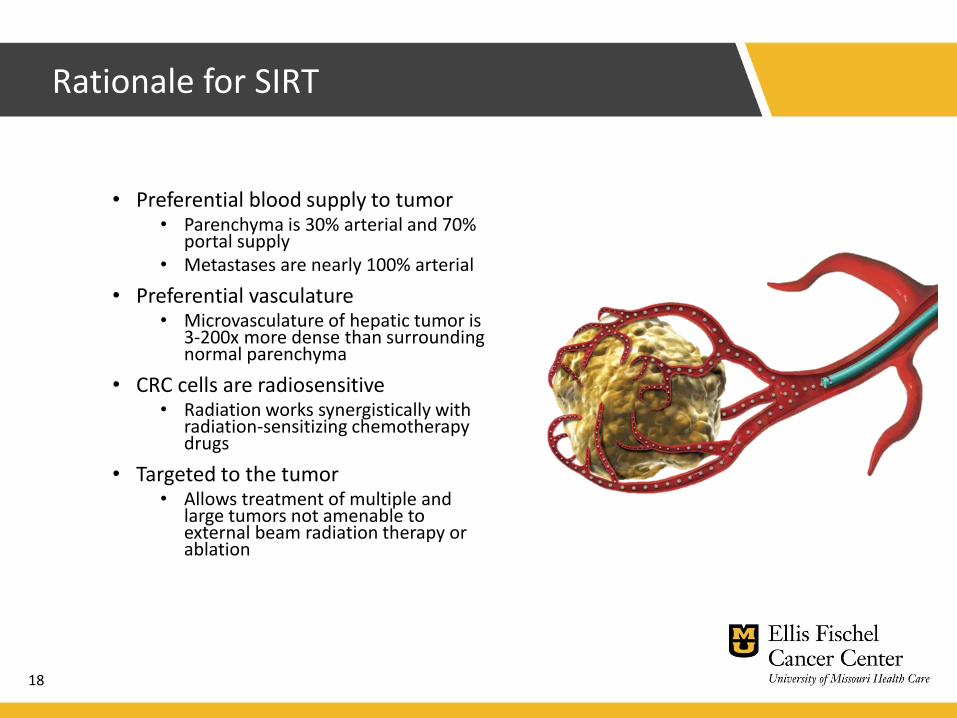
Rationale for SIRT
bull Preferential blood supply to tumorbull Parenchyma is 30 arterial and 70
portal supplybull Metastases are nearly 100 arterial
bull Preferential vasculaturebull Microvasculature of hepatic tumor is
3-200x more dense than surrounding normal parenchyma
bull CRC cells are radiosensitivebull Radiation works synergistically with
radiation-sensitizing chemotherapy drugs
bull Targeted to the tumorbull Allows treatment of multiple and
large tumors not amenable to external beam radiation therapy or ablation
18
Benefits of SIRT
bull Provide a localized radiation therapy delivering a dose of internal radiation up to 40x higher than conventional external beam therapy
bull Healthy liver tissue remain relatively unaffected2
bull 90 of patients experience ltGrade 3 adverse events
bull Outpatient Procedure
bull Typically involves two treatments over 6 weeks
bull Most patients return home 4-6 hours after the treatment
19
Products
bull Y-90 Glass Microspheres (TheraSpheres)bull 1999 granted Humanitarian Device Exemption for
use in unresectable HCC
bull Requires only safety not effectiveness data
bull Y-90 Resin Microspheres (Sir-Spheres)bull 2002 FDA grants Pre Market Approval for mCRC
bull Sufficient evidence that device is safe and effective for intended use
20
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

Benefits of SIRT
bull Provide a localized radiation therapy delivering a dose of internal radiation up to 40x higher than conventional external beam therapy
bull Healthy liver tissue remain relatively unaffected2
bull 90 of patients experience ltGrade 3 adverse events
bull Outpatient Procedure
bull Typically involves two treatments over 6 weeks
bull Most patients return home 4-6 hours after the treatment
19
Products
bull Y-90 Glass Microspheres (TheraSpheres)bull 1999 granted Humanitarian Device Exemption for
use in unresectable HCC
bull Requires only safety not effectiveness data
bull Y-90 Resin Microspheres (Sir-Spheres)bull 2002 FDA grants Pre Market Approval for mCRC
bull Sufficient evidence that device is safe and effective for intended use
20
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48
Products
bull Y-90 Glass Microspheres (TheraSpheres)bull 1999 granted Humanitarian Device Exemption for
use in unresectable HCC
bull Requires only safety not effectiveness data
bull Y-90 Resin Microspheres (Sir-Spheres)bull 2002 FDA grants Pre Market Approval for mCRC
bull Sufficient evidence that device is safe and effective for intended use
20
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48
SIR-Spheres Y-90 resin microspheres
Product Characteristics
bull Microsphere Material Biocompatible Polymer
bull Isotope Yttrium-90 permanently bound to the microsphere
bull Diameter ~325 microm
bull Specific Gravity 108 mgmL
bull Number of Particles per Vial 40-80 million
21
22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

22
mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

mCRC Liver Metastases and Mortality
bull Liver is the most common site of distant metastatic disease1-12
- 50 develop hepatic mets
- 10-25 considered resectable
bull Liver failure due to hepatic metastases is the most common cause of death among patients with mCRC13
bull Chemotherapy induced parenchymal damage also significantly contributes to liver failure1-12
Protecting healthy parenchyma while effectively treating liver metastases is a key goal when treating
patients with liver dominant metastases
23
1 McMillan DC McArdle CS Surg Oncol 200716(1)3-5 2 Sharma RA et al J Clin Oncol 200725(9)1099-1106 3 Van den Eynde M Hendlisz A Rev Recent Clin Trials 20094(1)56-62 4 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology Colon Cancer Version 32015 httpwwwnccnorgprofessionalsphysician_glspdfcolonpdf 5 Ye LC et al J Clin Oncol 201331(16)1931-1938 6 Burke D Allen-Marsh TG Postgrad Med J 1996 72 464-469 7 Penna C Nordlinger B Surg Clin N Am 2002 82 1075-1090 8 Brown AE et al Surg Clin N Am 2010 90 839-852 9 Fowler KJ et al Ann Surg Oncol 2013 201185-1193 10 Mahnken AH et al Radiology 2013266(2)407-430 11 Helling TS Martin M Ann SurgOncol 201421501-506 12 Shimura T et al J Gastrointest Cancer 2011 4268-72 13 Cho M Gong J amp Fakih M The state of regional therapy in the management of metastatic colorectal cancer to the liver Expert Rev Anticancer Ther 13 Jan 2016
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48
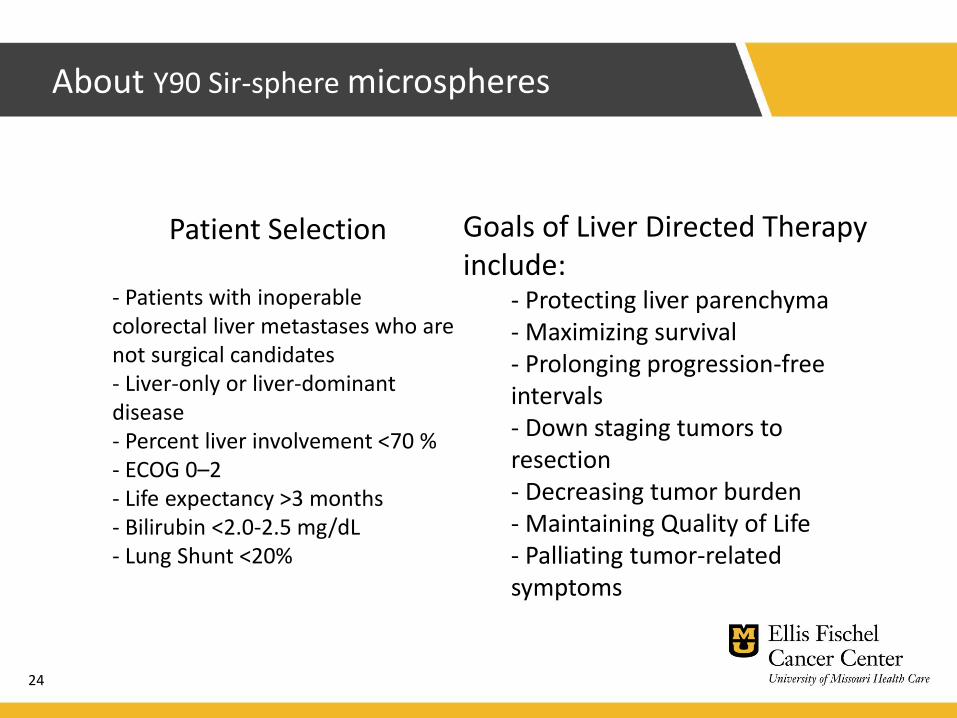
About Y90 Sir-sphere microspheres
24
- Patients with inoperable colorectal liver metastases who are not surgical candidates - Liver-only or liver-dominant disease- Percent liver involvement lt70 - ECOG 0ndash2 - Life expectancy gt3 months- Bilirubin lt20-25 mgdL- Lung Shunt lt20
Goals of Liver Directed Therapy include
- Protecting liver parenchyma- Maximizing survival- Prolonging progression-free intervals- Down staging tumors to resection- Decreasing tumor burden- Maintaining Quality of Life- Palliating tumor-related symptoms
Patient Selection
mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

mCRC Survival Chemo
25
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48
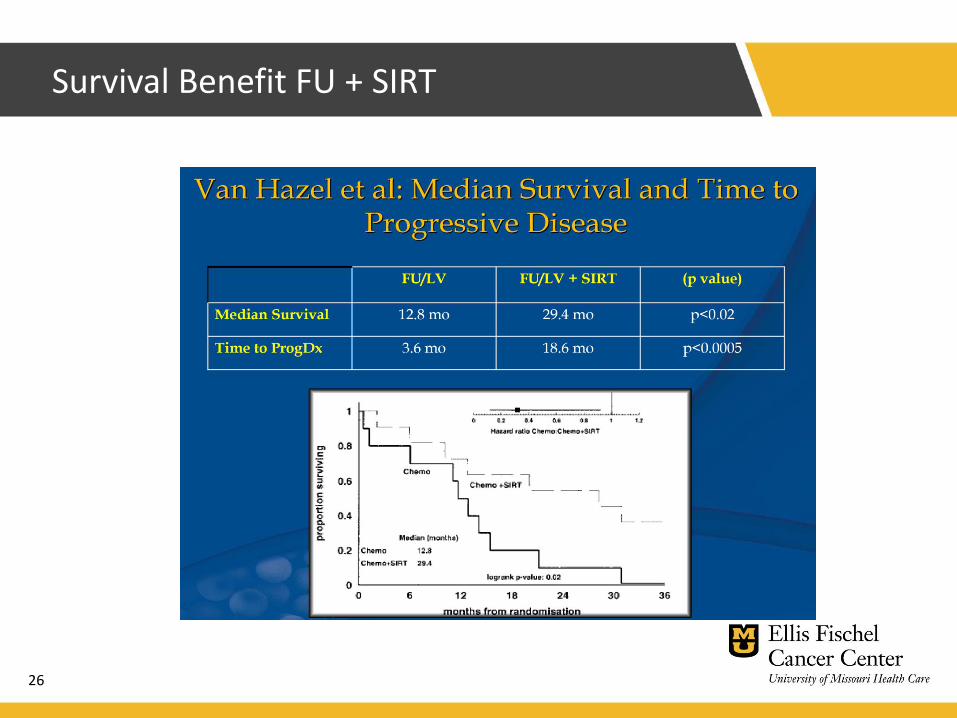
Survival Benefit FU + SIRT
26
SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

SIRFLOX
bull Randomized controlled trial radioembolization as an adjuvant to first-line chemotherapy for metastatic CRC was examined
bull Chemotherapy-naive patients with liver-dominant colorectal liver metastases (530 patients) were randomized to a group receiving FOLFOX with or without bevacizumab and a group receiving FOLFOX with or without bevacizumab and radioembolization
bull There was an 8-mo increase in liver-progressionndashfree survival in the radioembolization arm (21 vs 13 mo)
bull However there was no difference in overall progression-free survival
27
SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

SIRFLOX Study Design
28
Prospective open-label multicenter international RCT
Primary endpoint Progression-Free Survival
Eligible Patients
bull Nonresectable liver-
only or liver-dominant
mCRC
bull No prior chemo for
advanced disease
bull WHO Performance
Status 0ndash1
Stratified by
bull Presence of extra-
hepatic metastases
bull Degree of liver
involvement
bull Intended use of
bevacizumab
bull Institution
Randomized
11
N=530
mFOLFOX6 (+ bevacizumab)
mFOLFOX6 (+ bevacizumab)
SIR-Spheres Y-90 resin
microspheres
n=263 enrolled
n=267 enrolled
Bevacizumab allowed at investigatorrsquos
discretion per institutional practice
ANZ Australia New Zealand EME Europe amp Middle East mFOLFOX6 (modified FOLFOX6) leucovorin fluorouracil oxaliplatin mCRC metastatic colorectal cancer RCT randomized controlled trial US United States WHO World Health Organization
van Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
ANZ 280 (53)
EME 191 (36) US 59 (11)
SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

SIRFLOX Study Design
29
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
205months
SIR-Spheres Y-90 resin
microspheres significantly
extend PFS in the liver
with a 31 reduction in risk
of progression in the liver
+ 79 months
HR 069(95 CI 055ndash090)
P=002126months
FOLFOX
(+ Bev)
(n=263)
Progression-Free Survival in the Liver
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

Me
dia
n P
FS
in
th
e L
ive
r (m
on
ths
)
24
18
12
6
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=159)
211months + 87 months
HR 064(95 CI 048ndash086)
P=003124months
FOLFOX
(+ Bev)
(n=159)
PFS in the LiverLiver-Only and Liver + Extra-hepatic Metastases
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=108)
167months
+ 41 months
HR 077(95 CI 054ndash109)
P=147126months
FOLFOX
(+ Bev)
(n=104)
Liver-Only Metastases Liver + Extrahepatic Metastases
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

Bevacizumab allowed at investigatorrsquos discretion per institutional practicevan Hazel GA et al J Clin Oncol 2016 34 1723ndash1731
Pe
rce
nt
()
8
6
4
2
0FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
60
19
FOLFOX
(+ Bev)
(n=263)
3 x CR rateP=020
Complete Response Rate
Pe
rce
nt
()
80
60
40
20
0
Objective Response Rate
FOLFOX (+ Bev)
+ SIR-Spheres
microspheres
(n=267)
787
688
FOLFOX
(+ Bev)
(n=263)
+ 99 ORRP=042
SIR-Spheres Y-90 resin microspheres
Significantly Increase CR Rate and ORR in the Liver
SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

SIRFLOX OS
33
Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

Right Sided Colon Ca
34
Treatment Data on SIR-Spheresreg Y-90 Resin Microspheres for Patients with Liver Metastases from Right-Sided Primary Colon Cancer
A post-hoc analysis of data from the 739-patient SIRFLOX and FOXFIRE Global studies indicates that adding SIRT with liver-directed SIR-Spheresreg Y-90 resin microspheres to standard first-line mFOLFOX6 chemotherapy for liver-only or liver-dominant metastatic colorectal cancer (mCRC) in patients with right-sided primary (RSP) tumours led to a statistically significant and clinically meaningful 49-month median overall survival benefit (Hazard Ratio [HR] 064 [95 CI 046-089] p=0007) This translates into a 36 reduction in the risk of death at any given time compared to patients who received chemotherapy alone[1]
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48
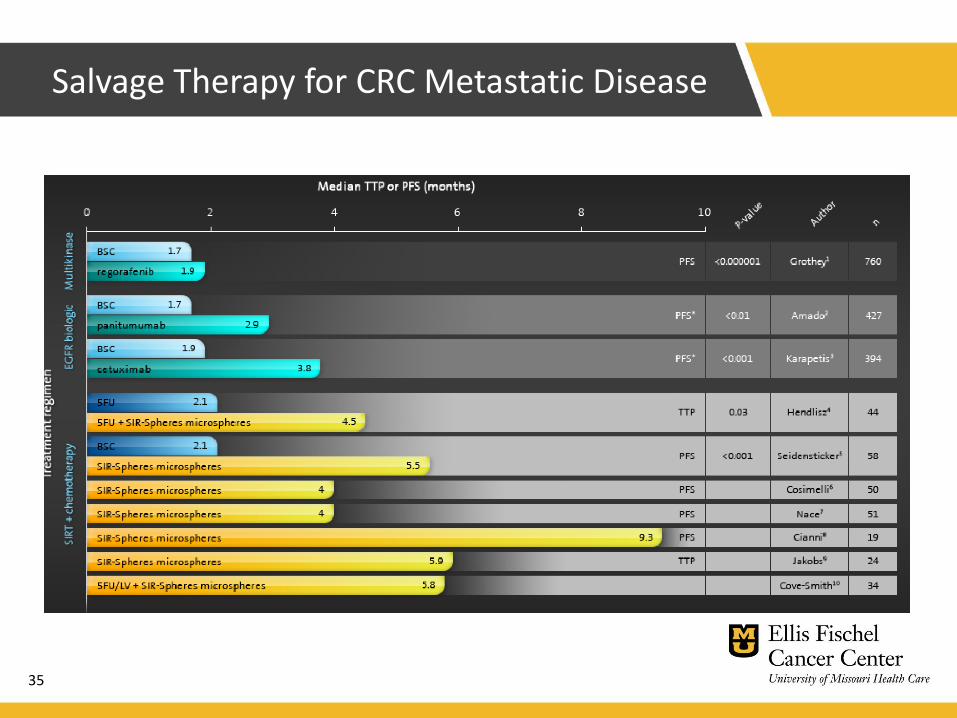
Salvage Therapy for CRC Metastatic Disease
35
Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

Salvage Therapy for CRC Metastatic Disease
36
NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

NCCN Guidelines Recommend SIR-Spheres Y90 Resin
Microspheres for Treatment of mCRC 2a Designation
37
Expert panel reaches uniform consensus that yttrium-90 microspheres is an appropriate option for patients with colorectal liver metastases ndash Interventional Oncology
httpwwwinterventionaloncology360comcontentnccn-guidelines-
recommend-sir-spheres-y90-resin-microspheres-treatment-metastatic-
colorectal
NCCN Categories of Evidence and ConsensusCategory 1 Based upon high-level evidence there is a uniform NCCN consensus that the intervention is appropriateCategory 2a Based upon lower-level evidence there is a uniform NCCN consensus that intervention is appropriateCategory 2b Based upon lower-level evidence there is a NCCN consensus that the intervention is appropriateCategory 3 Based upon lower level of evidence there is major NCCN disagreement that the intervention is appropriate
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48
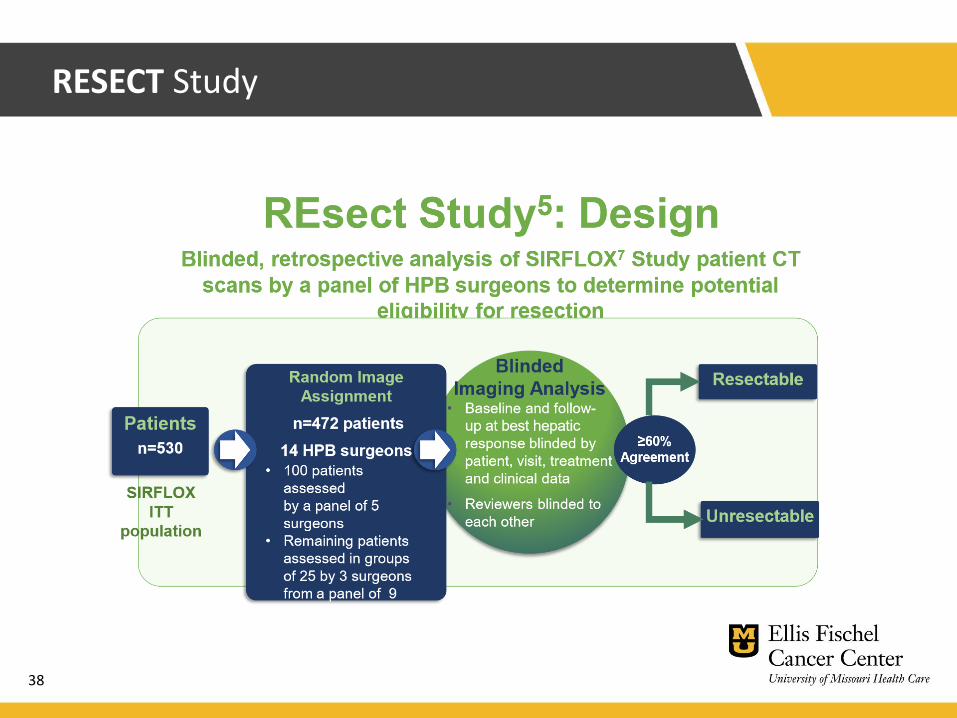
RESECT Study
38
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48
RESECT Study
39
- Surgeonsrsquo blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study present at 12th Annual European-African HPB meeting
- While resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study the increase was significantly more pronounced in patients receiving the combination treatment
- 381 of these were resectable on the basis of their liver CT scan at follow-up compared to 289 of the patients receiving chemotherapy only (plt00001)
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48
bull Retrospective study 2017 ASO
bull 100 Patients who had SIRT with resin microspheres from 16 centers
bull 71 had resection 29 Liver transplant
bull Grade 3 + adverse complications and any grade liver failure in 24 resection group and 7 transplant group
bull 63 occurred in extended resection group (gt5 segments)
bull 125-23 grade 3 complications in non-SIRT patients
bull 4 Deaths gt 6 segments resected multiple comorbidities
bull Study concludes mortality rates complication rates and LF rates
Is it Safe
40
SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

SIR-Spheres Y-90 resin microspheres Vs TACEDEB
41
Mechanisms of Actionbull TACEDEB Designed to
impede blood flow potentially resulting in PES
bull SIR-Spheres Y-90 resin microspheres Designed to travel deep into the tumor bed and deliver beta radiation directly to the tumor and not impede blood flow
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48
Advantages over TACE in HCC
bull TACE well established by two 2002 studies for inoperable intermediate stage HCC
bull Exceeds TACE in TTP of disease
bull Better toxicity profile
bull Better post treatment quality of life
bull Effective with more advanced disease
bull May use in patients is PVT bull Relative contraindication in TACEbull Similar survival to sorafenib (13 vs 11mo) but up to half TARE
patients downstaged for transplant
bull May have survival benefit (39mo vs 31 mo in BCLC B and C patients)
bull Retrospective
42
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48
Procedure
43
Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

Procedure
44
Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

Dose Calculation
45
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48
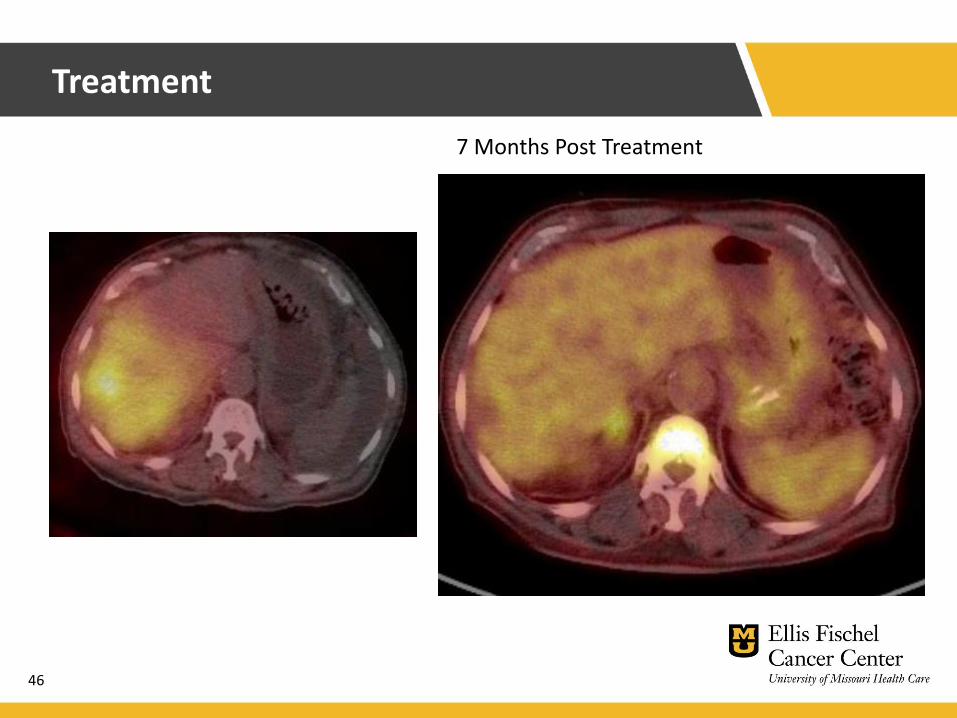
Treatment
46
7 Months Post Treatment
References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48

References
bull Goldberg SN Gazelle GS Mueller PR Thermal ablation therapy for focal malignancy a unified approach to underlying principlestechniques and diagnostic imaging guidance AJR Am J Roentgenol 2000 Feb174(2)323-31
bull Kallini et al Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma Adv Ther 2016 httplinkspringercomarticle1010072Fs12325-016-0324-7
bull Kritzinger et al Hepatic embolotherapy in interventional oncology Technology techniques and applications Clin Radiology 2012 httpwwwsciencedirectcomsciencearticlepiiS0009926012003704
bull Lencioni et al Chemoembolization of Hepatocellular Carcinoma Semin Intervent Radiol 2013 httpwwwncbinlmnihgovpmcarticlesPMC3700789pdfsir30003pdf
bull Llovet JM et al Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectablehepatocellular carcinoma a randomized controlled trial Lancet 2002 May18 359(9319) 1734-9
bull Pardo F et al The Post-Sir-Spheres Study Retrospective Analysis of Safety Following Resection or Transplant in Patients Previously Treated with SIRT with Y90 Resin Microspheres Annals of Surgical Oncology 2017 Sep 24 (9) 2465-2473
bull Salem R et al Radioembolization with 90Yttrium Microspheres a state-of-the-art bbachytherapy treatment for primary and secondary liver malignancies part 1 technical and methodologic considerations J Vasc Interv Radiol 17(8)1251-78 2006
bull Salem R et al Radioembolization with 90yttrium microspheres a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies Part 2 special topics J Vasc Interv Radiol 17(9)1425-39 2006
bull van Hazel GA et al SIRFLOX Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus mFOLFOX6 (plus or minus bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer J Clin Oncol 34(15)1723-31 2016
bull Wells et al Liver Ablation Best Practice Radiol Clin N Am 2015 httpwwwsciencedirectcomsciencearticlepiiS0033838915001050
47
Thank you
48
Thank you
48