Embed Size (px)
Citation preview

0165-4608/98/$19.00PII S0165-4608(98)00036-3
Cancer Genet Cytogenet 106:11–17 (1998)
Elsevier Science Inc., 1998655 Avenue of the Americas, New York, NY 10010
Interphase Cytogenetics of Esophageal Adenocarcinoma and Precursor Lesions
Diane L. Persons, Wendy S. Croughan, Kristen A. Borelli,and Rachel Cherian
ABSTRACT:
Limited information is currently available on chromosomal abnormalities in esophagealadenocarcinoma and associated premalignant lesions. In this study, numeric changes affecting chromo-somes 4, 6, 7, 8, 9, 10, 11, 12, 17, 18, X, and Y were analyzed by using fluorescence in situ hybridization(FISH) with chromosome-specific centromere DNA probes in 12 esophageal adenocarcinomas. In addi-tion,
TP53
overexpression, measured by immunohistochemistry, and amplification of
HER-2/neu
andC-
MYC
, detected by FISH, were analyzed within the same tumors. The most common numeric abnor-malities detected were gains of chromosomes 12 (8 cases), 6 (7 cases), 7 (7 cases), and 11 (6 cases). Thetotal number of abnormal chromosomes varied from 0 to 10, with an average of 4.6 per case. Overex-pression of
TP53
was present in 9 of 12 cases. No correlation was noted between the degree of aneusomyand
TP53
overexpression. In contrast,
HER-2/neu
amplification was present in two cases, both withlarge numbers of aneusomic chromosomes. Amplification of C-
MYC
was detected in only one case thathad a moderate number of numeric abnormalities. In a subset of cases in which premalignant lesionswere examined, aneusomy was found to be an early change, frequently present in both Barrett’s esopha-gus and dysplastic regions. In contrast, gene amplification and
TP53
overexpression were restricted tomore advanced areas of dysplasia and malignancy. Screening larger cohorts of patients with Barrett’sesophagus or dysplasia for numeric abnormalities of chromosomes 6, 7, 11, and 12 may determinewhether any of these abnormalities are predictive markers of progression to malignancy. © ElsevierScience Inc., 1998
INTRODUCTION
Most esophageal adenocarinomas are thought to arise fromBarrett’s esophagus [1]. Barrett’s esophagus is a columnarepithelial metaplastic change resulting from persistentdamage to the squamous epithelial lining of the loweresophagus [2]. There is a 30- to 40-fold increased risk of de-veloping esophageal adenocarcinoma in Barrett’s esopha-gus [3]. Early diagnosis of dysplasia or invasive adenocar-cinoma is crucial for optimal treatment. Progression fromthe metaplastic columnar epithelium through dysplasticchanges to adenocarcinoma most likely entails a series ofgenetic alterations [4]. Recognition of specific geneticchanges that could identify the subset of patients with
Barrett’s esophagus who will progress to adenocarcinomawould be very important. A few studies have describedcytogenetic changes in esophageal adenocarcinoma and inBarrett’s esophagus [5–8]. In addition,
TP53
abnormalitiesand other gene amplification or overexpression have beendescribed as potential markers in esophageal carcinomaand its precursor [9–13].
Fluorescence in situ hybridization (FISH), with the useof chromosome-specific
a
-satellite DNA probes, is a rapidmethod for determining the numeric complement of spe-cific chromosomes within metaphase and interphase nu-clei [14]. FISH has become a useful tool in determiningcommon numeric abnormalities in solid tumors, whichare often difficult to examine by conventional cytogenet-ics. Several types of solid tumors have been studied byFISH, including prostate [15] and bladder carcinoma [16,17]. In contrast with conventional cytogenetics, culture ar-tifacts are avoided by FISH; therefore all abnormalities de-tected are indicative only of in vivo chromosome changes.In addition, FISH can be performed on paraffin-embeddedtissue, allowing retrospective studies.
The goal of this study was to identify common numericchromosome abnormalities in esophageal adenocarcinoma
From the Department of Pathology and Laboratory Medicine,University of Kansas Medical Center (D. L. P., W. S. C., K. A. B.),Kansas City, Kansas, USA; and the Department of Pathology, Vet-erans Administration Hospital (R. C.), Kansas City, Missouri,USA.
Address reprint requests to: Diane L. Persons, M.D., 1213 Clin-ical Laboratory, University of Kansas Medical Center, 3901 Rain-bow Blvd., Kansas City, Kansas 66160-7232.
Received September 1, 1997; accepted February 12, 1998.

12
D. L. Persons et al.
by using chromosome-specific centromere probes andFISH. In addition, amplification of
HER-2/neu
and C
-MYC
and overexpression of
TP53
were examined. After identifi-cation of the most commonly abnormal chromosomes,analysis of premalignant lesions in tissue sections from asubset of cases was performed to determine the stage ofprogression at which the genetic abnormality arose.
MATERIALS AND METHODS
Tissue Samples
Specimens of paraffin-embedded esophageal adenocarci-nomas and corresponding premalignant lesions were ob-tained from the University of Kansas Medical Center (Kan-sas City, KS) and the Veterans Administration Hospital(Kansas City, MO). Tissue samples for the initial aneu-somy study were prepared from sections obtained fromparaffin-embedded tissue blocks from 12 esophageal ade-nocarcinoma cases. Isolated nuclei were prepared fromtwo to four 40-
m
sections of tissue. Areas of tumor weremicrodissected to enrich for more than 75% tumor cells.The microdissected sections were deparaffinized withthree 10-minute washes in xylene and rehydrated with two5-minute washes in absolute ethanol and two 5-minutewashes in dH
2
O. A nuclear suspension was prepared byincubating the sections in 2 mL of an 8.5 mg/mL pepsinsolution (Sigma P-7012, St. Louis, MO; 8.5 mg/mL in 0.9%NaCl, pH 1.5) at 37
8
C for 2.5 hours. The digested materialwas filtered through 40-
m
m nylon mesh (Tetko, BriarcliffManor, NY), washed twice in phosphate-buffered saline(PBS), resuspended in 200–500
m
L of PBS, and droppedonto slides. The cell suspension was spread over an areaof approximately 22
3
22 mm and oven dried at 60
8
C for10 minutes. Subsequent comparison of premalignant le-sions with invasive lesions was performed on 5-
m
sectionsfrom the corresponding case. The 5-
m
paraffin-embeddedtissue sections were deparaffinized in xylene
3
3 and de-hydrated in ETOH. The tissue was digested with 4 mg/mLpepsin for 10 minutes at 37
8
C. Slides were then washedfor 5 minutes each in H
2
O and 2
3
SSC.
Fluorescence In Situ Hybridization
Denaturation of both tissue sections and isolated nucleiwas performed in 70% formamide, at 70
8
C for 5 minutes.Slides were quenched in 70% cold ETOH, dehydrated,and air dried. Hybridization mixtures and probes for chro-mosome enumeration probes (CEP) X, Y, 4, 6, 7, 8, 9, 10,11, 12, 17, and 18, along with probe for
HER-2/neu
andC
-MYC
were obtained from Vysis, Inc. (Downers Grove,IL). Probes were denatured at 70
8
C for 5 minutes. The de-natured probes were added to the slide of denatured tissueor cells, hybridized overnight, and finally washed for 2minutes in 0.4
3
SSC at 70
8
C. Nuclei were counterstainedwith 1
m
g/mL 4
9
,6-diamidino-2-phenylindole dihydro-chloride (DAPI) in the antifade
p
-phenylenediamine dihy-drochloride.
Analysis of Interphase In Situ Hybridization
Hybridization signals were enumerated within 200 inter-phase nuclei per specimen. Criteria for analysis of nuclei
have been previously described [18]. Overlapping nucleiand nuclei lacking any hybridization signals were ex-cluded from analysis. Individual signals were recorded foreach nucleus. Analysis and photography was performedon fluorescence microscopes equipped with a triple-passfilter for simultaneous detection of SpectrumGreen, Spec-trumOrange, and DAPI (DAPI/Green/Orange, Vysis, Inc.,Downers Grove, IL) or a dual-pass filter (DAPI/Orange) fordetection of SpectrumOrange and DAPI. Photographs wereobtained with Kodak Ektachrome Elite 400 (EastmanKodak, Rochester, NY).
TP53 Immunostaining
Rabbit anti-human
TP53
antibody (DO-1, Immunotech,Westbrook, ME) was used as the primary antibody. Theantibody was detected by using a DAB secondary detec-tion kit (Bio Tek Solutions; CMS, Houston, TX) accordingto the manufacturer’s instructions. Cells were counter-stained with ethyl green. Immunostaining was consideredpositive when more than 10% of cells had 2
1
or 3
1
nu-clear staining intensity (1
1
, weak staining; 2
1
, moderatestaining; 3
1
, strong staining).
RESULTS
Numeric chromosome abnormalities determined by FISHon isolated nuclei from 12 cases of esophageal adenocarci-noma are summarized in Table 1. All centromere probesavailable from Vysis, Inc. at the initiation of the study—namely, X, Y, 4, 6, 7, 8, 9, 10, 11, 12, 17, and 18—wereused to screen the tumors to identify the most commonaneusomic (gained or lost) chromosomes. In the isolatednuclei part of the study, significant aneusomy was definedas greater than 25% of 200 nuclei with more than two sig-nals (gain) or fewer than two signals (loss). Evaluation ofseveral normal control specimens of isolated nuclei fromnormal gastric mucosa suggested that a 10% cutoff (meanplus two standard deviations) might be applicable for dif-ferentiating aneusomic tumor nuclei from normal nuclei(data not shown). However, essentially all tumor speci-mens showed between 5 and 15% aneusomy for mostprobes. These findings most likely represent nonclonal ab-
Table 1
Numeric chromosome abnormalities as determined by FISH
Case Partial Karyotype
a
1 No abnormalities2
2
Y,
1
4,
1
7,
1
83
1
11,
1
12,
1
184
2
Y,
1
6,
1
11,
1
125
1
Y,
1
6
1
7,
1
9,
1
11,
1
12,
1
17,
1
186
1
127
1
X,
1
6,
1
7,
2
8,
1
9,
1
10,
1
11,
1
12,
1
17,
1
188
1
X,
1
4,
1
6,
1
9,
1
10,
1
12,
1
17,
1
189
1
6,
1
7,
1
17,
1
18
10
1
7,
1
811
1
X,
1
6,
1
7,
1
8,
1
11,
1
12,
1
1712
1
X,
1
6,
1
7,
1
11,
1
12,
1
17
a
Chromosomes examined: X, Y, 4, 6, 7, 8, 9, 10, 11, 12, 17, and 18.

FISH Analysis in Esophageal Adenocarcinoma
13
normalities or small abnormal subclones. Because the pri-mary objective of the initial part of this study was to de-fine major clonal abnormalities in these tumors, a 25%cutoff was chosen. With this cutoff, small populations ofaneusomic cells, indicating tumor heterogeneity or techni-cal artifact, were not considered major abnormal clones.The total number of abnormal chromosomes per case var-ied from 0 to 10, with an average of 4.6 aneusomic chro-mosomes per case (Fig. 1). Overall, gain in chromosomecopy number was more frequent than loss of a chromo-some (Fig. 2). In some of the cases with numerous chromo-some gains, tetraploidization had most likely taken place.The only losses detected included the Y chromosome (2cases) and chromosome 8 (1 case). Of the 12 chromosomesexamined, gains of chromosomes 12 (8 cases), 6 (7 cases),and 11 (6 cases) were most commonly observed.
Nine of the 12 tumors overexpressed
TP53
by immuno-histochemical staining. Tumors that overexpressed
TP53
had between 1 and 10 aneusomic chromosomes and in-cluded those tumors with amplified
HER-2/neu
and C
-MYC
(Fig. 1). Therefore, there was no correlation between
TP53
overexpression and degree of aneusomy. In contrast,
Her-2/neu
was amplified in two cases, both of which had sig-nificant numbers of aneusomic chromosomes. The singletumor in which C
-MYC
was amplified had a moderate de-gree of aneusomy (6 abnormal chromosomes).
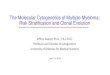
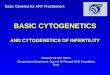
Figure 3 illustrates FISH performed on tissue sectionsof case 12 for evaluation of chromosome 6 aneusomy innormal gastric tissue, Barrett’s esophagus, dysplastic Bar-rett’s, and invasive tumor. No nuclei contained more thantwo signals in the normal tissue. However, 17% of the Bar-rett’s nuclei, 22% of the dysplastic nuclei, and 34% of thetumor nuclei had more than two signals (Fig. 4). Addi-tional interphase analysis performed on tissue sectionsfrom case 12 and 7 are shown in Figure 4. Gains of chro-
mosomes 6 and 12 were observed in 17–21% of nucleiwithin the Barrett’s esophagus area and a substantial num-ber of nuclei within the dysplastic areas in these twocases. In contrast, amplification of C
-MYC
was not ob-served in the Barrett’s region in case 12 but was present inmost of the dysplastic and tumor nuclei.
Her-2/neu
ampli-fication also was not present in Barrett’s esophagus butwas seen in 3% of dysplastic nuclei and most of the tumornuclei in case 7. Precursor lesions were not available forevaluation of
Her-2/neu
amplification in case 8. Precursorlesions examined in cases 2 (chromosome 8), 9 (chromo-somes 6 and 7), 10 (chromosome 8), and 11 (chromosome6) had less than 10% aneusomic nuclei (data not shown).However, in each of these instances, there was an in-creased number of abnormal nuclei compared with nor-mal tissue.
Overexpression of
TP53
was not observed in any casesof Barrett’s esophagus but was seen in 4 of 6 cases of dys-plasia associated with the eight tumors that overexpressed
TP53
(Table 2). There was no evidence of aneusomy,
Her-2/neu
or C
-MYC
amplification, or
TP53
overexpression inrandom sections from adjacent normal gastric or esoph-ageal squamous tissue in any of the 12 cases.
DISCUSSION
The development of malignancy in Barrett’s esophagus,in the progression from metaplasia to dysplasia to adeno-carcinoma, is undoubtedly associated with genetic changesat each step. The number of studies addressing chromo-somal alterations in Barrett’s esophagus or in adenocarci-noma arising from this lesion are limited [5–8]. To date,the most extensive study examined 37 adenocarcinomasof the esophagus, of which 22 arose in Barrett’s esophagus[8]. Losses of chromosomes 4, 18, 21, and Y and gain of
Figure 1 Total number of aneusomic chromosomes per case. Cases with Her-2/neu or C-MYC amplification areindicated along with those with TP53 overexpression (*).

14 D. L. Persons et al.
chromosomes 14 and 20 were the most frequent numericchanges. Rearrangements were most often observed in 1p,3q, 11p, and 22p. Two of eight Barrett’s esophagus speci-mens were also found to have clonal chromosome abnor-
malities in this study. Garewal et al. [5] examined 10 casesof Barrett’s esophagus, 9 of which had clonal abnormali-ties. The most common findings were loss of chromo-somes, in particular chromosomes 5 and 7 (1 case) and
Figure 2 Chromosome-specific aneusomy (number of cases with gain or loss) in 12 esophageal carcinomas.
Figure 3 Chromosome 6 aneusomy in case 12: normal copy number (2 signals) in gastric control (A); aneusomy(.2 signals) in Barrett’s esophagus (B); dysplasia (C); and tumor (D). SpectrumOrange CEP 6 and DAPI counter-stain, 3600.

FISH Analysis in Esophageal Adenocarcinoma 15
chromosome Y (7 cases). Three cases of Barrett’s esopha-gus were examined by Raskind et al. [6]. Clonal abnormal-ities were found to be present in areas of Barrett’s mucosaand in surrounding regions of histologically normal mu-cosa. The clones persisted when the disease progressed toeither high-grade dysplasia or adenocarcinoma.
Although only limited knowledge exists concerning thecytogenetic abnormalities associated with Barrett’s esoph-
agus and adenocarcinoma of the esophagus, flow cytomet-ric techniques have demonstrated correlations betweenaneuploidy and histologic diagnosis. Several studies havedemonstrated the association of aneuploidy with ad-vanced degrees of dysplasia and with adenocarcinoma[19–21]. However, the flow cytometric method for analysisof ploidy is limited to detection of total DNA contentchanges of greater than 4% [22]. Inasmuch as the largest
Figure 4 Aneusomy and gene amplification in adenocarcinoma and precursor lesions (case 7, left; case 12,right). Abbreviations: CEP, chromosome enumeration probe; N, normal tissue; B, Barrett’s esophagus; D, dysplasia;T, tumor.

16 D. L. Persons et al.
chromosome (chromosome 1) consists of approximately5% of the total DNA content, it is possible to have gainsand losses of multiple smaller chromosomes that would beundetected by flow cytometric analysis. FISH has previ-ously been shown to be a more sensitive method than flowcytometry for detection of aneuploidy [15]. In addition,FISH performed on paraffin-embedded tissue has severaladvantages over conventional cytogenetic methods per-formed on fresh tissue. One advantage, the ability to visu-ally differentiate tumor and normal nuclei, allows verifi-cation of normal results. In contrast, a normal cytogeneticresult may indicate analysis of normal cells and failure oftumor cells to grow. As an example, in the study byMenke-Pluymers et al. [8], a number of cases had normalcytogenetic results but had abnormal DNA indexes byflow cytometry. FISH analysis also reveals an accuraterepresentation of the proportion of genetic abnormalitiesthat are present in vivo and is not dependent on thegrowth variability of different clones in an in vitro envi-ronment. The major limitation of using centromere-spe-cific probes and FISH analysis is that structural rearrange-ments of chromosomes cannot be detected.
Using FISH and probes for chromosomes 7, 8, 17, andY, Krishnadath et al. [23] found overrepresentation ofchromosome 8 (2 cases) and loss of chromosomes 17 (2cases) and Y (3 cases) in an examination of five esophagealcarcinomas. In the present study, we used 12 chromo-some-specific probes and examined a larger number ofesophageal carcinomas. We found that gains of chromo-somes 6, 7, 11, and 12 were the most frequent numeric ab-normalities. At least one of these chromosomes wasgained in all 11 abnormal cases. In a subgroup of Barrett’sesophagus cases, aneusomy of these chromosomes wasfrequently detected, suggesting that aneusomy is an earlyevent in tumorigenesis. Gains of chromosomes 7 and 12have been frequently observed in both gastric and coloncarcinoma [24–26]. We also observed the loss of the Ychromosome in 2 of our cases. The loss of the Y chromo-some has been one of the most frequently reported nu-meric changes in esophageal adenocarcinoma and in Bar-rett’s esophagus [5, 23].
The TP53 gene has been shown to be abnormal in a sig-nificant proportion of esophageal cancers as well as intheir precursors (9, 27]. Wang et al. [10] also described ar-eas of nonneoplastic esophageal mucosa that contained
mutant TP53 by immunohistochemical methods. In con-trast, although a large percentage of adenocarcinomasoverexpressed TP53 in our study (9 of 12 tumors) and 4cases with dysplasia were positive, no evidence of overex-pression was noted in Barrett’s esophagus or in normalmucosa. Likewise, amplification of HER-2/neu and C-MYChave been identified in both gastric and esophageal adeno-carcinomas [11, 12, 28]. Similar to TP53 overexpression,amplification of HER-2/neu or C-MYC was limited to tu-mor or dysplastic nuclei in 3 amplified cases. These re-sults indicate that gene amplification and TP53 overex-pression were not early events in our case cohort.
In conclusion, aneusomy was found to be an earlychange, frequently present in both Barrett’s esophagus anddysplastic regions in the subset of cases in which prema-lignant lesions were examined. In contrast, gene amplifi-cation and TP53 overproduction were restricted to moreadvanced areas of dysplasia and malignancy. Future stud-ies screening large cohorts of patients with Barrett’sesophagus or dysplasia for numeric abnormalities of chro-mosomes 6, 7, 11, and 12 may determine whether any ofthese abnormalities are predictive of progression to malig-nancy. The combination of histologic evaluation andaneusomy analysis performed by FISH may be used toidentify those patients with Barrett’s esophagus whowould benefit from more frequent clinical evaluation forearly detection of adenocarcinoma.
REFERENCES
1. DeMeester TR (1993): Barrett’s esophagus. Surgery 113:239–241.
2. Spechler SJ, Goyal RK (1987): Barrett’s esophagus. N Engl JMed 315:362–371.
3. van der Veen AH, Dees J, Blackensteijn JD, Van BlankensteijnM (1989): Adenocarcinoma in Barrett’s esophagus: an over-rated risk. Gut 30:14–18.
4. Chejfec G, Schnell T, Sontag S (1992): Barrett’s esophagus: apreneoplastic disorder. Am J Clin Pathol 98:5–7.
5. Garewal HS, Sampliner R, Liu Y, Trent JM (1989): Chromo-somal rearrangement in Barrett’s esophagus: a premalignantlesion of esophageal adenocarcinoma. Cancer Genet Cytoge-net 42:281–296.
6. Raskind WH, Norwood T, Levine DS, Haggitt RC, Rabino-vitch PS, Reid BJ (1992): Persistent clonal areas and clonalexpansion in Barrett’s esophagus. Cancer Res 52:2946–2950.
7. Rodriguez E, Rao PH, Ladonyi M, Altorki N, Chaganti RSK(1990); 11p13–15 is a specific region of chromosomal rear-rangement in gastric and esophageal adenocarcinoma. Can-cer Res 50:6410–6416.
8. Menke-Pluymers MBE, van Drunen E, Vissers KJ, MulderAH, Tilanus HW, Hagemeijer A (1996): Cytogenetic analysisof Barrett’s mucosa and adenocarcinoma of the distal esopha-gus and cardia. Cancer Genet Cytogenet 90:109–117.
9. Casson AG, Mukhopadhyay T, Cleary KR, Ro JY, Levin B,Roth JA (1991): P53 gene mutations in Barrett’s epitheliumand esophageal cancer. Cancer Res 51:4495–4499.
10. Wang L-D, Hong J-Y, Qui S-L, Gao H, Yang CS (1993): Accu-mulation of p53 protein in human esophageal precancerouslesions: a possible early biomarker for carcinogenesis. CancerRes 53:1783–1787.
11. Houldsworth J, Cordon-Cardo C, Ladanyi M, Kelsen DP,
Table 2 TP53 overexpression
Case Normal Barrett’s Dysplasia Tumor
1 2 2 1 1
5 2 ND ND 1
6 2 ND ND 1
7 2 2 2 1
8 2 ND ND 1
9 2 2 1 1
10 2 2 2 1
11 2 2 1 1
12 2 2 1 1
Abbreviation: ND, not done, no Barrett’s or dysplasia present.

FISH Analysis in Esophageal Adenocarcinoma 17
Chaganti RSK (1990): Gene amplification in gastric andesophageal adenocarcinomas. Cancer Res 50:6417–6422.
12. Al-Kasspooles M, Moore JH, Orringer MB, Beer DG (1993):Amplification and over-expression of the EGFR and erbB-2genes in human esophageal adenocarcinomas. Int J Cancer54:213–219.
13. Stemmermann G, Heffelfinger SC, Noffsinger A, Hui YZ,Miller MA, Fenolio-Preiser CM (1994): The molecular biol-ogy of esophageal and gastric cancer and their precursors:oncogenes, tumor suppressor genes, and growth factors. HumPathol 25:968–981.
14. Pinkel D, Straume T, Gray JW (1986): Cytogenetic analysisusing quantitative, high-sensitivity, fluorescence hybridiza-tion. Proc Natl Acad Sci USA 83:2934–2938.
15. Persons DL, Kazuhiro T, Gibney DJ, Katzmann JA, LieberMM, Jenkins RB (1994): Comparison of fluorescence in situhybridization with flow cytometry and static image analysisin ploidy analysis of paraffin-embedded prostate adenocarci-noma. Hum Pathol 25:678–683.
16. Hopman AHN, Moesker O, Smeets AWGB, Pauwels RPE,Vooijs GP, Ramaekers FCS (1991): Numerical chromosome 1,7, 9, and 11 aberrations in bladder cancer detected by in situhybridization. Cancer Res 51:644–649.
17. Waldman FM, Carroll PR, Kershmann R, Cohen MB, FieldFG, Mayall BH (1991): Centromeric copy number of chromo-some 7 is strongly correlated with tumor grade and labelingindex in human bladder cancer. Cancer Res 51:3807–3811.
18. Persons DL, Robinson RA, Hsu PH, Seelig SA, Borell TJ,Hartmann LC, Jenkins RB (1996): Chromosome-specificaneusomy in carcinoma of the breast. Clin Cancer Res 2:883–888.
19. Reid BJ (1991): Barrett’s esophagus and esophageal adenocar-cinoma. Gastroenterol Clin North Am 20:817–834.
20. Reid BJ, Blount PL, Rubin CE, Levine DS, Haggitt RC, Rabino-
vitch PS (1992): Flow-cytometric and histological progres-sion to malignancy in Barrett’s esophagus: prospectiveendoscopic surveillance of a cohort. Gastroenterology 102:1212–1219.
21. Sciallero S, Giaretti W, Bonelli L, Geido E, Rapallo A, ConioM, Ravelli P, Lombardo L, Lapertosa G, Aste H (1993): DNAcontent analysis of Barrett’s esophagus by flow cytometry.Endoscopy 25:648–651.
22. Koss LG, Czerniak B, Herz F (1989): Flow cytometric mea-surements of DNA and other cell components in humantumors: a critical appraisal. Hum Pathol 20:528–548.
23. Krishnadath KK, Tilanus HW, Alers JC, Mulder AH, vanDekken H (1994): Detection of genetic changes in Barrett’sadenocarcinoma and Barrett’s esophagus by DNA in situhybridization and immunohistochemistry. Cytometry 15:176–184.
24. Ochi H, Douglass HO, Sandberg AA (1986): Cytogenetic stud-ies in primary gastric cancer. Cancer Genet Cytogenet 22:295–307.
25. Bardi G, Johansson B, Pandis N, Bak-Jensen E, Orndal C,Heim S, Mandahl N, Andren-Sandberg A, Mitelman F (1992):Cytogenetic aberrations in colorectal adenocarcinomas andtheir correlation with clinicopathological features. Cancer 71:306–314.
26. Xiao S, Wei W, Leng X, Shi Y, Liu Q, Li P (1992): Direct chro-mosome analysis of seven primary colorectal carcinomas.Cancer Genet Cytogenet 62:32–39.
27. Ramel S, Reid BJ, Sanchez CA, Blount PL, Levine DS, NeshatK, Haggitt RC, Dean PJ, Thor K, Rabinovich PS (1992): Evalu-ation of p53 protein expression in Barrett’s esophagus bytwo-parameter flow cytometry. Gastroenterology 102:1220–1228.
28. Shibuya M, Yokota J, Ueyama Y (1985): Amplification andexpression of a cellular oncogene (c-myc) in human gastricadenocarcinoma cells. Mol Cell Biol 5:414–418.