Embed Size (px)
Citation preview

Insulin-like Growth Factor IIin Gynecological Cancers: A PreliminaryStudy
INTRODUCTION
Insulin-like growth factor (IGF) system is one of thegrowth factor systems that modulates steroid hormoneactions in the endometrium through autocrine/para-crine mechanisms.1,2 IGF-I and IGF-II stimulateproliferation and differentiation and maintain differ-entiated cell functions in several cell types in vitro. Forexample, endometrial stromal cells produce IGF-I andIGF-II as well as high-affinity IGF-binding proteins(IGFBP), whereas epithelial cells and, to a lesserextent, stromal cells contain cell membrane receptorsfor IGF. Estrogen stimulates IGF-I gene expression,and IGF-II gene expression is associated with endome-trial differentiation. The messenger RNA (mRNA)
of six high-affinity IGFBPs is expressed in humanendometrium. Suppression of IGF-I action by IGFBP-1 may be one of the molecular mechanisms accountingfor progestagenic and anti-estrogenic effects of levo-norgestrel in the endometrium.1,2 IGF-II is present introphoblast cells and in placenta and the levels are highduring fetal circulation.3,4
Of late, an awareness of the IGF system playing amajor role in carcinogenesis has resulted from thedocumentation of IGF-I mRNA or protein up-regu-lation in many cancers.5 The IGF-II mRNA expres-sion is up-regulated in an adrenocortical tumor cellline.6 Elevated levels of serum IGF-I have beenobserved in patients with lung, breast, and prostatecancers.7 The association between IGF-I and prostate
American Journal of Reproductive Immunology
Mathur SP, Landen CP, Datta SM, Hoffman MC, Mathur RS,Young RC. Insulin-like Growth Factor II in Gynecological Cancers: APrelim- inary Study. AJRI 2003; 49:113–119 � Blackwell Munksgaard,2003
PROBLEM: We have previously reported elevated serum levels ofcervical human papilloma viral proteins E6 and E7 and serum insulin-like growth factor II (IGF-II) in women with cervical cancer andadvanced cervical intraepithelial neoplasia. As most women withcervical cancer have elevated levels of serum IGF-II, we sought todetermine whether the cervical cancer and lymph node biopsies fromthese women demonstrated increased production of IGF-II and whetherthis elevation was also present in ovarian and endometrial cancers.METHOD OF STUDY: We used the semi-quantitative immunofluo-rescent antibody assay established in our laboratory to identify thelevels of IGF-II in 21 cervical cancers (seven with matching lymphnodes), 18 benign cervical biopsies, 13 endometrial cancers, 15 benignendometrial biopsies, 5 ovarian cancers, and 15 benign ovarian biopsies.RESULTS: The immunofluorescent IGF-II levels (relative intensityper pixel) were the highest in cervical cancers; they were significantlyhigher than in matched controls. IGF-II levels were not higher inovarian cancers and only slightly elevated in endometrial cancers. Thepresence of IGF-II in pelvic lymph nodes of women with cervicalcancer paralleled with those in the cervical cancers. Interestingly, wecould identify small nests of metastases of malignant cells in the nodes(pauci-cellular metastasis) by using IGF-II as the marker.CONCLUSION: We propose that measurement and identification ofIGF-II in the cervical biopsy may be a sensitive method of detectingcervical cancer and metastatic spread in the lymph nodes.
Subbi P. Mathur, Charles P. Landen,Susan M. Datta, M. CamilleHoffman, Rajesh S. Mathur, andRoger C. YoungDepartment of Obstetrics and Gynecology,Medical University of South Carolina,Charleston, SC, USA
Key words:Cervix neoplasms, endometrium neoplasms, insulin-likegrowth factors, ovary neoplasms
Address reprint requests to Professor Subbi P. Mathur,Division of Gynecological Oncology,Department of Obstetrics and Gynecology,Medical University of South Carolina,96 Jonathan Lucas Street,Suite 634, Charleston,SC 29425, USA.E-mail: [email protected]
Submitted May 7, 2002;accepted June 3, 2002.
AJRI 2003; 49: 113–119Copyright � Blackwell Munksgaard, 2003
ISSN 8755-8920
AMERICAN JOURNAL OF REPRODUCTIVE IMMUNOLOGY VOL. 49, 2003

cancer risk has also been consistently observed inboth cohort and case-control studies.8 IGF-1, but notIGF-II, levels are increased in the plasma of patientswith prostate cancer.9 Three studies suggested arelationship between IGF-I and breast cancer.10–12
Other cohort studies show that pre-menopausalwomen in the highest tertile of IGF-I had a threefoldincrease in the risk of breast cancer compared withthose in the lowest tertile.13
IGF-II is a 7,500 molecular weight, 67 amino acidpeptide which mediates some of the actions of growthhormone.14 It is secreted as a pro-hormone consistingof A, C, B, D, and E chains.15 The mature IGF-IIpeptide consists of A, C, and B chains and isstructurally homologous to IGF-I and proinsulin. Itis secreted by the liver and by target tissues such ascervix and endometrium, where it serves a paracrinerole. IGF-II in circulation is bound to IGFBP-5, IGF-BP3 and to an acid-labile sub-unit.16,17 IGF-II mRNAexpression is normally highest during fetal life anddeclines after birth. The proportion of unbound IGF-II in the circulation of normal men and women is lessthan 5%.14
By using human papilloma virus (HPV)-negativecervical cancer cell line HT-3, Steller et al.18 found anincrease in IGF-II mRNA following epidermalgrowth factor (EGF) stimulation. However, they didnot detect any increase in IGF-I mRNA. Theyhypothesized that autocrine production of IGF-IIand over-expression of the IGF-1 receptor in cervicalcancer may participate in the mitogenic signaling ofEGF.19 Other data suggest that IGF-II gene abnor-malities may be present in cervical cancer.20 In anearlier study, presence of IGF-II in cervical cancercell culture supernatants was indirectly assessed byusing a radio-receptor assay.21 Relaxation of IGF-IIgene imprinting in human gynecologic tumors hasbeen reported.22Increased IGF-I levels and decreasedIGFBP-1 have been shown in post-menopausalwomen with endometrial cancer.23
Our earlier studies have shown:
1. supernatants of both HPV-positive and -negativecervical cancer cell lines incubated with differentconcentrations of EGF or nicotine had elevatedlevels of EGF-receptor (EGF-R) and IGF-II in adose-dependent manner;24
2. elevated levels of EGF-R and HPV E6 and E7proteins in cervical cancer and cervical intraepithel-ial neoplasia;25
3. more importantly, serum levels of IGF-II, but not ofIGF-I, were elevated (almost fourfold higher thanthe levels in normal menstruating women)26 incervical cancer and advanced cervical intraepithelialneoplasia;27 and
4. serum IGF-II levels were significantly decreased inwomen with cervical cancer after therapy.27
In the present study, we sought to determinewhether IGF-II could be detected in tissue specimensof cervical, ovarian, and endometrial cancers. Further-more, we attempt to correlate relative levels of IGF-IIin these specimens by using semi-quantitative immu-nofluorescence techniques.
MATERIALS AND METHODS
MaterialsWe studied the immunofluorescent levels (relativeintensity per pixel) of IGF-II in archival biopsysamples from 21 cervical cancers, 18 benign cervicalsections, 13 endometrial cancers, 15 normal endome-trial sections, 5 ovarian cancers and 15 benign ovariansections in this preliminary study. We also studiedmatching lymph nodes and cervical cancers from sevenpatients with cervical cancer.The paraffin sections were treated by the protocol
developed in the laboratory.25,26 Briefly, paraffin sec-tions were de-paraffinized by passing the slides throughxylene, 100% ethyl alcohol, 90% ethyl alcohol, 80%ethyl alcohol, 70% ethyl alcohol, 50% ethyl alcohol,10% ethyl alcohol, and finally, deionized glass distilledwater. The slides were heated for 1 min in boilingantigen-unmasking citrate buffer solution and washedin cold phosphate-buffered saline.
Immunofluorescent Quantification of IGF-IIin Tissue SectionsWe applied a semi-quantitative immunofluorescentantibody assay24,25 to identify IGF-II levels in squa-mous epithelium of cervical tissues. We used anantibody to human IGF-II, raised in goat (ICNBiomedicals, Lisle, IL, USA), as the primary antibody.Fluorescein isothio-cyanate-conjugated anti-goat IgGantibody (ICN Biomedicals) was used as the secondaryantibody.The intensity of immunofluorescence was measured
by digitized image analysis using an Axioplan researchmicroscope (Carl Zeiss Inc., Jena, Germany) equippedwith a 100-W mercury light source and a 100 · plan-neufluar nal. 3 objective. The images were capturedwith a Dage CCD 100 integrating camera (Dage-MTI,Ann Arbor, MI, USA) and a Flashpoint 128 CaptureBoard (Integral Technologies, Lafayette, IN, USA).Image capture and processing were done on a DualPentium Pro 200 Imaging Workstation (Dell Comput-ers, Austin, TX, USA) by using Image-Pro Plussoftware (Media Cybernetics, Silver Springs, MD,USA). The settings were left constant through the
114 / MATHUR ET AL.
� BLACKWELL MUNKSGAARD, 2003

processing of all the images. Cells with maximumpositive intensity measured 250–260 units of relativeintensity per pixel and the negative areas measured 40–60 units in light intensity. Small areas of squamousepithelial cells were outlined and the fluorescent inten-sity was assessed in pixels, without bias in each area,until the whole relevant field was covered. Two observ-ers analyzed at least 20 fields for each tissue. Meanvalues of these observations for each microscopic fieldwere obtained by using the Image-Pro software. Thevalues for IGF-II (relative intensity per pixel) obtainedin each patient were entered in the database forstatistical analysis. The quality control measures aredescribed elsewhere.24–26 The location of positive cellswas matched on a hematoxylin–eosin-stained sectionand the nature of carcinogenicity of the cell wasassessed.
Statistical Analysis of DataValues for IGF-II were compared between the controlsand patients in each group as well as between cancercells and normal cells in the same section, usingStudent’s t-test. Linear regression analysis was used tocompare the levels in the cervical cancer tissue withthose in lymph nodes from the same patients.
RESULTS
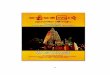
IGF-II, as determined by semi-quantitative immuno-fluorescent antibody assay, was significantly higher insquamous epithelial cervical cancer cells than in normalcervical epithelial cells in the same sections. It was also
higher in cervical cancer cells than in squamous epithel-ials cells from the cervix of normal women. The levelswere the highest in cervical cancer and the lowest inovarian cancers (Table I, Fig. 1). The levels in endome-trial cancers were slightly elevated but did not approachthe values seen in cervical cancers.The lymph nodes from women with known cervical
cancer were also investigated for the presence ofIGF-II. The lymph nodes were divided into twocategories, namely, histologically positive and his-tologically negative. IGF-II values were determinedfor each category. The IGF-II levels were highlycorrelatable (P < 0.0001) between cervical cancersand lymph nodes from the same patients (Table II,Fig. 2).
DISCUSSION
Ovarian Cancers. We found no difference in the valuesof IGF-II when comparing ovarian cancer tissues withnormal ovary. Thus, in spite of most ovarian and cer-vical cancers being epithelial in origin, our data suggestdifferent mechanisms of malignant cell proliferation.Endometrial Cancers. Our data demonstrate signifi-cant differences in IGF-II levels between the malig-nant endometrium of cancer patients and normalendometrium. While these data suggest that IGF-IImay be involved in the proliferative mechanisms ofendometrial cancer, the values are not sufficientlyhigh to be of clinical use.Cervical Cancers. Consistent with our previousobservations, IGF-II appears to be over-expressedby cervical cancer cells. This observation perhaps maybe exploited to improve cervical cancer screening, forevaluation of the extent of the disease, or as a meansto monitor therapy.In spite of the recommendation for annual Pap
smear screening, cervical cancer remains a majorgynecologic malignancy in this country and claims14,500 new cases and 4,800 lives every year.28 It hasbeen estimated that at least 25% of women with high-grade intraepithelial neoplasia are not being identifiedduring routine gynecological examination. Because ofthe relatively low sensitivity and specificity of the Papsmear,29 the currently used decision tree is relativelycostly and inefficient in finding high-grade neoplasia.30
For cervical cancer, though surgical therapy is suc-cessful many times, detection of metastasis requiresextensive dissection. Furthermore, it is estimated thatmore than 10,000 malignant cells are required in alymph node to identify metastasis and occult lymphaticspread.31 A rapid tissue or blood test that will identifythose women who are at risk for developing recurrentcervical cancer will be valuable.
TABLE I. IGF-II Levels (Mean � S.D. Relative Intensity per
Pixel) in the Cervical Cancer (CC), Cervical Cancer Normal
Tissue (CCN), Benign Cervix (BC), Ovarian Cancer (OC),
Ovarian Cancer Normal Tissue (OCN), Benign Ovary (BO),
Endometrial Cancer (EC), Endometrial Cancer Normal
Tissue (ECN), and Benign Endometrium (BE)
Group Mean � S.D.
P value
versus benign
CC (n ¼ 21) 180.9 � 23.4 < 0.00001
CCN (n ¼ 21) 69.0 � 14.9 N.S.
BC (n ¼ 18) 67.7 � 3.1 –
OC (n ¼ 4) 77.1 � 4.4 N.S.
OCN (n ¼ 5) 69.2 � 2.8 N.S.
BO (n ¼ 15) 69.6 � 3.3 –
EC (n ¼ 13) 95.1 � 18.9 0.025
ECN (n ¼ 13) 87.5 � 15.7 N.S.
BE (n ¼ 15) 65.2 � 10.8 –
Cut-off level for a positive finding (mean � 2 S.D. of benign cer-vix ¼ 99).
IGF-II IN GYNECOLOGICAL CANCERS / 115
AMERICAN JOURNAL OF REPRODUCTIVE IMMUNOLOGY VOL. 49, 2003

Pap smears and screening patients for HPV havecontributed to benefit women with cervical cancer.However, we need an additional screening test that willenable us to accurately pinpoint malignant cell prolif-eration and, more importantly, help us to monitortherapy efficacy in these patients. The reasons are asfollows:
• Not all women with abnormal Pap smear or positiveHPV testing progress to cervical cancer.
• Sensitivity of a Pap test is at best estimated to be51%, which is somewhat improved by liquid prepPap test.
• There are a large number of patients for whomthere is clearly a need for something more than
Fig. 1. IGF-II in (A) normal cervix, (B) cervical cancer, (C) normal endometrium, (D) endometrial cancer, (E) normal ovary, and (F) ovarian
cancer.
116 / MATHUR ET AL.
� BLACKWELL MUNKSGAARD, 2003

the Pap test, such as those with atypical squa-mous cells of undetermined significance/AGUS.32 The latter patients often do not get the
medical attention that they need and have to waitfor repeat tests before clinical therapy can beinitiated.
Fig. 2. IGF-II in paired cervical cancer and
lymph node sections from the same patient.
(A, C, E, G, and I) from cervical cancer and
(B, D, F, H, and J) from lymph nodes of the
same patient.
IGF-II IN GYNECOLOGICAL CANCERS / 117
AMERICAN JOURNAL OF REPRODUCTIVE IMMUNOLOGY VOL. 49, 2003

• Also, these tests cannot be used to follow-up ontherapy efficacy on women with cervical cancer afterthey have been treated, because of the paucity ofcervical tissue available for biopsy.
• Only 80–85% of women with cervical cancer areinfected with HPV (HPV typing is not routinelydone in all clinical institutions) and there is a highdegree of observer variability in Pap smears.
Our finding of elevated levels of IGF-II duringcervical cancer and in the serum of women withcervical cancer (the first one in the literature) isexciting, specific to cervical cancer, and supports thefeasibility of using these tests to diagnose thepresence of cervical cancer. Screening the lymphnode biopsies for the presence of increased IGF-IIwill help us identify small metastases of cervicalcancer, which may otherwise be missed by micro-scopic examination. We call these metastases to bepauci-cellular metastases. Supplementing Pap smearwith IGF-II testing will be a value-added screeningfor cervical cancer.It appears that IGF-II plays a major role in cellular
proliferation in cervical cancer. Because of its closeassociation with IGFBP 1–532–35 and the recentlydiscovered binding protein vibronectin,36 we can inferthat the heightened levels of cervical and serum IGF-IIin cervical cancer patients will be matched by altera-tions in the IGFBPs and receptor repertoire.
AcknowledgementsThis research was supported by the Medical Univer-sity of South Carolina Research Grant UDAK223600 24859 4123, Summer Student ResearchProgram, and by National Cancer Institute Grant 1R21 CA 92085-01. The authors wish to thankthe thoughtful guidance of Dr. Jim Nicholson,
Director, Image Analysis Laboratory, Departmentof Pathology and Laboratory Medicine, during theimage analysis of cells.
REFERENCES
1. Rutanen EM: Insulin-like growth factors and insulin-likegrowth factor binding proteins in the endometrium.Effect of intrauterine levonorgestrel delivery. HumReprod 2000; 15(3 Suppl):173–181.
2. Werner H, Adamo M, Roberts CT Jr., LeRoith D:Molecular and cellular aspects of insulin-like growthfactor action. Vitam Horm 1994; 48:1–58.
3. Han VK, Carter AM: Spatial and temporal patternsof expression of messenger RNA for insulin-likegrowth factors and their binding proteins in the placentaof man and laboratory animals. Placenta 2000;21(4):289–305.
4. de los Rios P, Hill DJ: Cellular localization and expres-sion of insulin-like growth factors (IGFs) and IGFbinding proteins within the epiphyseal growth plate ofthe ovine fetus: possible functional implications. Can JPhysiol Pharmacol 1999; 77(4):235–249.
5. Camacho-Hubner C: Insulin-like growth factor-bindingproteins and neoplasia: an overview. Growth Horm IGFRes 2000; 10(A Suppl):S14–S15.
6. Logie A, Boulle N, Gaston V, Perin L, Boudou P,Le Bouc Y, Gicquel C: Autocrine role of IGF-II inproliferation of human adrenocortical carcinoma NCIH295R cell line. J Mol Endocrinol 1999; 23(1):23–32.
7. Yu H, Berkel H: Insulin-like growth factors and cancer.J La State Med Soc 2001; 151:218–223.
8. Wolk A, Mantzoros CS, Andersson SO, Lu CM, CookNR: Insulin-like growth factor I and prostate cancerrisk: a population-based case-control study. J NatlCancer Inst 1998; 90:911–915.
9. Chan JM, Stampfer MJ, Giovannucci E: Plasma insulin-like growth factor I and prostate cancer risk: a pros-pective study. Science 1998; 279:563–566.
10. Peyrat JP, Bonneterre J, Hecquet B: Plasma insulin-likegrowth factor I (IGF-I) concentrations in human breastcancer. Eur J Cancer 1993; 29:492–497.
11. Bruning PF, van Doorn J, Bonfrer JMG, Ringeling AM,Rikken B: Insulin-like growth factor-binding protein 3 isdecreased in early stage operable premenopausal breastcancer. Int J Cancer 1995; 2:266–270.
12. Hankinson SE, Willett WC, Colditz GA, Hunter DJ,Michand DS, Rosner B, Speizer FE, Pollack M: Circu-lating concentrations of insulin-like growth factor I andrisk of breast cancer. Lancet 1998; 351:1393–1396.
13. Bohlike K, Cramer DW, Trichopoulos D, Davis DL:Insulin-like growth factor-I in relation to premenopausalductal carcinoma in situ of the breast. Epidemiology1998; 9:570–573.
14. Doughaday WH, Rohwein P: Insulin-like growth factorsI and II. Peptide, messenger ribonucleic acid and genestruction, serum and tissue concentrations. Endocr Rev1989; 10:68–91.
15. Bell GI, Merryweather JP, Sanchez-Pescodor R, Stem-pian MM, Priestley L, Scott J, Roll LB: Sequence of acDNA clone encoding human preproinsulin-like growthfactor II. Nature 1984; 310:775–777.
TABLE II. Levels of IGF-II (Relative Intensity per Pixel) in
the Cervical Cancer and Matching Nodes from Women with
Cervical Cancer
No.
Cervical
cancer
Node
cancer cells
Node
normal cells
1 199.0 146.9 68.6
2 208.3 92.5 50.4
3 179.3 79.7 80.6
4 144.2 86.7 52.4
5 162.4 100.6 60.6
6 143.8 90.5 44.3
7 184.7 137.8 49.1
Mean 174.5 105.0 58.0
S.D. 20.9 21.4 10.2
118 / MATHUR ET AL.
� BLACKWELL MUNKSGAARD, 2003

16. Baxter RC, Martin JL, Beniac VA: High molecularweight insulin-like growth factor binding protein com-plex. J Biol Chem 1989; 264:11843–11848.
17. Rachlar M: Insulin-like growth factor-binding proteins.Vitam Horm 1993; 47:1–114.
18. Steller MA, Delgado CH, Zou Z: Insulin-like growthfactor II mediates epidermal growth factor-inducedmitogenesis in cervical cancer cells. Proc Natl Acad SciUSA 1995; 92:11970–11974.
19. Steller MA, Delgado CH, Bartels CJ, Woodworth CD,Zou Z: Overexpression of the insulin-like growth factor-1 receptor and autocrine stimulation in human cervicalcancer cells. Cancer Res 1996; 56(8):1761–1765.
20. Douc-Rasy S, Barrois M, Fogel S, Ahomadegbe JC,Stehelin D, Coll J, Riou G: High incidence of loss ofheterozygosity and abnormal imprinting of H19 andIGF2 genes in invasive cervical carcinomas. Uncouplingof H19 and IGF2 expression and biallelic hypomethy-lation of H19. Oncogene 1996; 12(2):423–430.
21. Naik P, Christofori G, Hanahan D: Insulin-like growthfactor II is focally upregulated and functionally involvedas a second signal of oncogene-induced tumorigenesis. InCold Spring Harbor Symposia on Quantitative Biology,vol. LIX. New York, Cold Spring Harbor LaboratoryPress, 1994, pp 459–470.
22. Yaginuma Y, Nishiwaki K, Kitamura S, Hayashi H,Sengoku K, Ishikawa M: Relaxation of insulin-likegrowth factor-II gene imprinting in human gynecologictumors. Oncology 1997; 54(6):502–507.
23. Ayabe T, Tsutsumi O, Sakai H, Yoshikawa H, Yano T,Kurimoto F, Taketani Y: Increased circulating levels ofinsulin-like growth factor-I and decreased circulatinglevels of insulin-like growth factor binding protein-1 inpostmenopausal women with endometrial cancer. End-ocr J 1997; 44(3):419–424.
24. Mathur RS, Mathur SP, Young RC: Up regulation ofepidermal growth factor receptors (EGF-R) by nicotinein cervical cancer cell lines: this effect is mediated byEGF. Am J Reprod Immunol 2000; 44:114–120.
25. Mathur SP, Mathur RS, Rust PF, Young RC: Humanpapilloma virus (HPV)-E6/E7 and epidermal growthfactor receptor (EGF-R) protein levels in cervical cancerand cervical intraepithelial neoplasia (CIN). Am JReprod Immunol 2001; 46:280–287.
26. Van Dessell HJHM, Chandrasekher Y, Yap OWS, LeePDK, Hintz RL, Faessen GHJ, Braat DDM, Bart C,
Fauser JM, Guidice LC: Serum and follicular fluidlevels of insulin-like growth factor I (IGF-I), IGF-II andIGF-binding protein-1 and -3 during the normalmenstrual cycle. J Clin Endocrinol Metab 1996; 81:1224–1231.
27. Mathur SP, Mathur RS, Young RC: Cervical epidermalgrowth factor receptor (EGF-R) and insulin-like growthfactor II (IGF-II) levels in women with cervical cancerand cervical intraepithelial neoplasia (CIN). Am JReprod Immunol 2000; 44:222–230.
28. Parker SL, Tong T, Bolden S, Li MD, Kanej K: Cancerstatistics 1997. CA Cancer J Clin 1997; 47:1–27.
29. Blomfield PI, Lancashire RJ, Woodman CBJ: Canwomen at risk of cervical abnormality be identified? Br JObstet Gynaecol 1998; 105:486–492.
30. Genest DR, Dean B, Lee KR, Sheets E, Crum CP, CibasES: Qualifying the cytologic diagnosis of ‘Atypical squ-amous cells of undetermined significance’ affects thepredictive value of a squamous intraepithelial lesion onsubsequent biopsy. Arch Pathol Lab Med 1998; 122:338–341.
31. Kim PY, Monk BJ, Chabra S, Burger RA, Vasilev SA,Manetta A, DiSaia PJ, Berman ML: Cervical cancerwith paraaortic metastases: significance of residualparaaortic disease after surgical staging. Gynaecol Oncol1998; 69:243–247.
32. Arai T, Busby W Jr., Clemmons DR: Binding of insulin-like growth factor (IGF) I or II to IGF-binding protein-2enables it to bind to heparin and extracellular matrix.Endocrinology 1996; 137(11):4571–4575.
33. Collett-Solberg PF, Cohen P: Genetics, chemistry, andfunction of the IGF/IGFBP system. Endocrine 2000;12(2):121–136.
34. Han VK, Carter AM: Spatial and temporal patterns ofexpression of messenger RNA for insulin-like growthfactors and their binding proteins in the placenta ofman and laboratory animals. Placenta 2000; 21(4):289–305.
35. Bond JJ, Meka S, Baxter RC: Binding characteristics ofpro-insulin-like growth factor-II from cancer patients:binary and ternary complex formation with IGF bindingproteins-1 to -6. J Endocrinol 2000; 165(2):253–260.
36. Upton Z, Webb H, Hale K, Yandell CA, McMurtry JP,Francis GL, Ballard FJ: Identification of vitronectin asa novel insulin-like growth factor-II binding protein.Endocrinology 1999; 140(6):2928–2931.
IGF-II IN GYNECOLOGICAL CANCERS / 119
AMERICAN JOURNAL OF REPRODUCTIVE IMMUNOLOGY VOL. 49, 2003












![Epidemiology of Ovarian Cancer: Risk Factors and PreventionOvarian Cancer (OC) is a global health crisis and one of the deadly gynecological cancers among women worldwide [1]. Despite](https://img.dokumen.tips/doc/110x75/5e96ed02b573f005ce5939f4/epidemiology-of-ovarian-cancer-risk-factors-and-prevention-ovarian-cancer-oc.jpg)