Embed Size (px)
Citation preview

Informed Consent Form V.1.0; Clinical trials: NCT01595334
1
Informed consent form
Institution: Southern Cross Fertility Centre Title of the Study Influence of Luteinizing Hormone (LH) on Oocyte Maturity
(LH/M2-‐Oocyte) (ClinicalTrials.gov Identifier NCT01595334) Study director M R Bharucha, PhD (Sat Kaival Pvt. Ltd, Anand, Gujarat) Principal investiga-‐tors in different lo-‐cations
1. Nayana Patel, MD (Sat Kaival Hospital Pvt. Ltd, Anand, Guajarat) 2. Faram Irani, MD (Southern Cross Fertility Center, Mumbai, India) 3. Asha Baxi, MD, FRCOG (Disha Fertility & Surgical Hospital, Indore, In-‐dia)
Sponsor: Southern Cross Fertility Centre in collaboration with Disha Fertility and Surgical Centre, Indore, India
Locations: Sat Kaival Hospital Pvt. Ltd, Anand, Guajarat Southern Cross Fertility Center, Mumbai, India Disha Fertility & Surgical Hospital, Indore, India
Participant’s Printed Name: ______________________________________

Informed Consent Form V.1.0; Clinical trials: NCT01595334
2
1. Introduction We invite you to participate in a experimental study “Influence of Luteinizing Hormone (LH) on Oocyte Maturity (LH/M2-‐Oocyte)”. This study is done in Southern Cross Fertility Center and in two other hospitals (Sat Kaival Hospital Pvt. and Disha Fertility & Surgical Hospital). We hope that the results of this study will help women who cannot not have children to become mothers.
1.2 Take your time to decide to be in this study or not. (21 CRF part 50.25: A1.8 voluntary consent) Only you will decide to take part in the study or not. Nobody will push you. Take your time to make your decision. Talk with your family doctor and the people in our Center about this study. It is also a good idea to talk with your family and friends. It is very important to talk with you male partner. We will use his sperm cells to make a baby. He also need to come to our Center and talk to the Study Doctor before signing his consent. (If you do not have a male partner you may chose to use donor sperm.)
1.3 If you and you partner decide to participate, your need to: ICH E6: Subject’s responsibilities 1. Sign these “Informed consent” forms. “Informed” means that you fully understand what procedures you will do during the study, and what good or bad things may happen to you. “Consent” means that that you agree to take part in this study. 2. Follow the rules of the study. Your Study Doctor will tell you what and when you will do. You will need to call or come to The Center, take drugs, do shots and other procedures strictly at the time you Study Doctor will say. You cannot skip any procedures if you want to stay in the study. 3. Answer honestly on the questions the Study Doctor or other Study Team member will ask you. 4. Call the Center if: – you want to change the time of procedure (sometimes we cannot change the time); – something unusual or bad happened to your health during the study; – you need to use other drugs or to do procedures outside the study; – you want to stop being in the study. 5. Use drugs and study products that we will give only for yourself. 6. Not participate in other studies at this time.
Informed Consent Form V.1.0; Clinical trials: NCT01595334
3
1.4 You main rights will be: 1. To receive good medical care from the Study Doctor and the Study Team. 2. To receive all information about the study before, during, and after the study. 3. To ask questions to the Study Doctor and Study Team about this study. 4. To ask other doctors who is not in the study for second opinion (to know what do they think about your medical care in this study). 5. To be treated for the injuries that could be caused by the study. 6. To stop your participation in the study at any moment. Please read this papers carefully to understand you rights. You may want to talk with “re-‐search subjects protection advocate” (the lawyer who will better explain all your right). The address of one of such advocates is given in section “12. How to contact the Center and other organizations?”
1.5 Who pays for this study? The person or organisation who pays for the study of new drugs in people is named a “sponsor”. The sponsor of the study is Southern Cross Fertility Centre in collaboration with (which means “with the help of”) Disha Fertility and Surgical Centre.
Informed Consent Form V.1.0; Clinical trials: NCT01595334
4
1.6 Short glossary This consent form may contain words that you do not understand. Please ask the Study Doctor or the Study Team to explain any words or information that you do not clearly understand. To understand the consent better you may like to read this short glossary (Table 1). You may like to add some words to this glossary and ask the Study Team what do they mean.
Table 1. Short Glossary
Word What does it mean?
Conception, to con-‐ceive
A sperm cells gets inside an Egg.
Egg retrieval Taking eggs from a female body
Egg, egg cell, oocyte Tiny structure that is made by woman’s Ovary. When sperm cell gets inside an egg a baby may appear.
Embryo Very small baby (less than 8 weeks after Conception) Embryo transfer Placement of embryos into the Uterus
Fertilization Same as Conception
Male partner A man who will be the father of your baby.
Ovary The part of woman belly that makes Eggs. Study product Any of two drugs that we are testing in this study. Both were approved by FDA to
treat people. But to show that we are not sure which of them works better, we named them “study products”
(Your) Study doctor Dr. Faram Irani if you will participate in the study in Southern Cross Fertility Cen-‐ter. He will take care of you during the study.
Study subject You or other women on whom we will test Study Product.
Sperm cell Tiny structure that is made by man’s body. It moves in woman body and gets in-‐side an Egg to make a baby.
The Center Southern Cross Fertility Center, Mumbai, India. But if you would like to partici-‐pate in a study in one of another hospitals (Sat Kaival Hospital or Disha Fertility & Surgical Hospital) it will mean the hospital where your Study Doctor works.
Uterus The part of a woman belly where unborn baby lives.
We. The team, Study team
Study Doctor, Study nurses, clinical research coordinator, pharmacist and other people who will do the study in the Center.
Your Word
Your Word
Your Word
Informed Consent Form V.1.0; Clinical trials: NCT01595334
5
2. Why is this study being done? (21 CRF part 50.25: A1.1 Purpose) Many women like you try to become mothers, but they cannot make this. One of the best ways to help them is named “In vitro fertilization”. “In vitro” means “in glass”. So your egg will meet a sperm cell on a glass plate. To do this we need to take some eggs from your body. The more eggs we take, the better chance that one of them will become a child.
But your body makes only one egg each month. To make you body work harder, we will give you a special drug shot. It will “egg on” several eggs to grow at once. Than we will give you another drug. It will make growing eggs ripen. The more ripen the eggs are, the bet-‐ter their chances to become a healthy baby.
We used two different “ripening” drugs named Cetrorelix and Luprolide Acetate. We are not sure which of them makes the egg more “ripen”. So we make an experiment (a special test). We will divide all 300 women who will take part in the study into two groups. 150 women in the Group 1 will receive one drug and 150 women in Group 2 will re-‐ceive another drug. Then we will check which drug helped more women to become pregnant.
Note! The Study Doctor and Study Team who will treat you in the Center will take care about you health. But at the same time they are researchers. So they also will take care about the results of the study as well.
Randomization (ICH E6: probability of random assignment)
A computer may put you in Group 1 or Group 2 by chance (like a flip of a coin). This is named “randomization”. Neither you nor your Study Doctor can choose the group you will be in. You will have an equal chance of being placed in any of two groups.
“Unblinded” study
You and your doctor will know which of the two drugs (Cetrorelix or Luprolide Acetate) you will receive. As you could read the name of the drug with you own eyes this is named “unblinded”.
Informed Consent Form V.1.0; Clinical trials: NCT01595334
6
3. What will happen if I take part in this research study? (21 CRF part 50.25: A1.2 Procedures) If you decide to participate you will do many different procedures. Some of them may be unpleasant and risky. In this part we only describe the procedures. You could read about unpleasant thing in the chapter “5. What bad things may happen to me if I take part in the study?”
3.1 Before we begin • Give the Study Doctor some records from your other doctors: – results of your last physical exam from your PCP (or family doctor); – results of your last gynecological (female doctor) exam. You can bring this records at your first visit, send by mail or ask your doctors office to send your records to the Center. Do these exams 6 month or later before the date of your 1st visit to the Center. Blood test. We will take 10 ml (less than 1 tablespoon) of your blood to check if your body can make eggs. We will also check if you have some diseases (human immunodefi-‐ciency virus (HIV), hepatitis B and C viruses, and syphilis). Hysteroscopy. During this procedure the Study Doctor will look inside
your uterus with a tiny camera. He will do this to check if a baby can live in your body. This procedure lasts 15-‐20 minutes. We need to do this in one of the first 4 days after you monthly bleeding has started. Note! If the Study Doctor decides that your body cannot make eggs or bear a baby, you cannot be in the study. You also cannot take part if you have one of the diseases listed above, or if your heart is too weak to bear some procedures. Spermogram. Your male partner will need to give us some sperm. It takes 15-‐20
minutes. We will check how many sperm cells he makes, and if they are healthy.
3.2 “Calming” you body down. Oral contraceptives. You will take oral pills for 18 days starting from the 2nd day of your
cycle. You will take one pill every morning before or after you eat. If you forget to take a pill please call the Center. The pills will give your body a rest before we start the study. Blood test and ultrasound. After 18 days we will check if your body had enough rest. To do this we need to take 10 ml of blood again, and look inside you belly with “transvaginal” ultrasound. That means the spe-‐cial device will be inserted in the vagina for 10-‐15 minutes. The ultra-‐sound procedure is not painful.
Informed Consent Form V.1.0; Clinical trials: NCT01595334
7
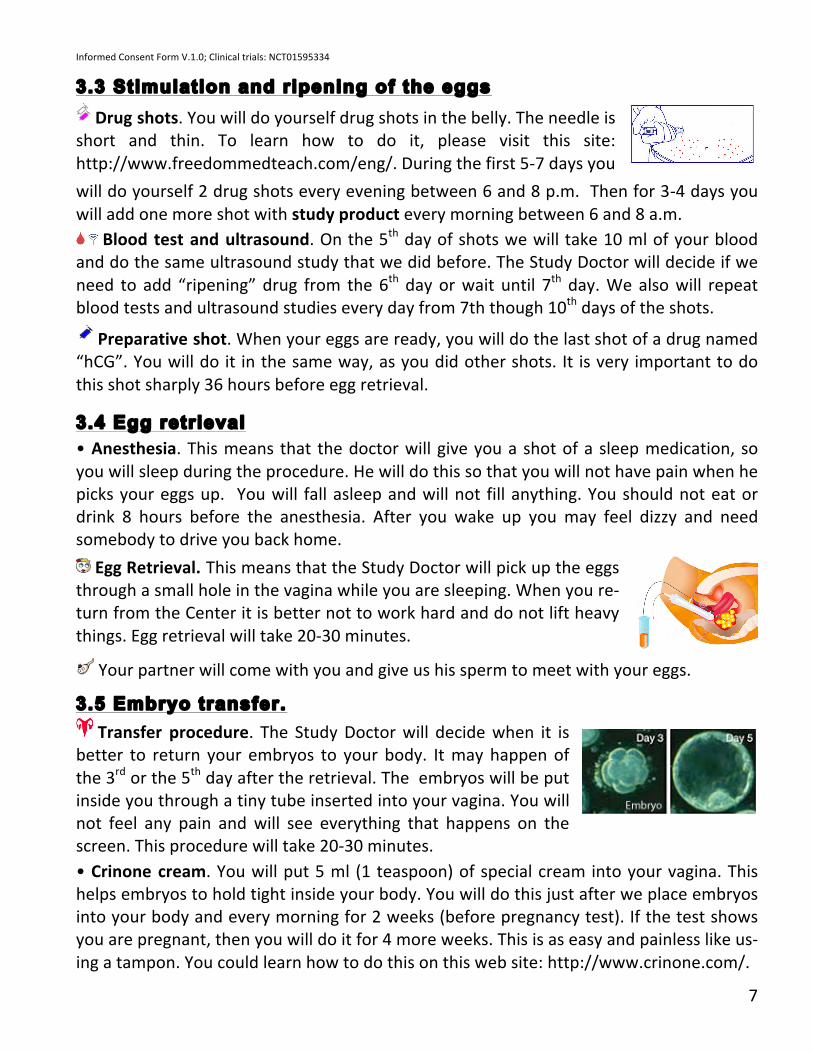
3.3 Stimulation and ripening of the eggs Drug shots. You will do yourself drug shots in the belly. The needle is
short and thin. To learn how to do it, please visit this site: http://www.freedommedteach.com/eng/. During the first 5-‐7 days you
will do yourself 2 drug shots every evening between 6 and 8 p.m. Then for 3-‐4 days you will add one more shot with study product every morning between 6 and 8 a.m. Blood test and ultrasound. On the 5th day of shots we will take 10 ml of your blood and do the same ultrasound study that we did before. The Study Doctor will decide if we need to add “ripening” drug from the 6th day or wait until 7th day. We also will repeat blood tests and ultrasound studies every day from 7th though 10th days of the shots.
Preparative shot. When your eggs are ready, you will do the last shot of a drug named “hCG”. You will do it in the same way, as you did other shots. It is very important to do this shot sharply 36 hours before egg retrieval.
3.4 Egg retrieval • Anesthesia. This means that the doctor will give you a shot of a sleep medication, so you will sleep during the procedure. He will do this so that you will not have pain when he picks your eggs up. You will fall asleep and will not fill anything. You should not eat or drink 8 hours before the anesthesia. After you wake up you may feel dizzy and need somebody to drive you back home. Egg Retrieval. This means that the Study Doctor will pick up the eggs
through a small hole in the vagina while you are sleeping. When you re-‐turn from the Center it is better not to work hard and do not lift heavy things. Egg retrieval will take 20-‐30 minutes. Your partner will come with you and give us his sperm to meet with your eggs.
3.5 Embryo transfer. Transfer procedure. The Study Doctor will decide when it is
better to return your embryos to your body. It may happen of the 3rd or the 5th day after the retrieval. The embryos will be put inside you through a tiny tube inserted into your vagina. You will not feel any pain and will see everything that happens on the screen. This procedure will take 20-‐30 minutes. • Crinone cream. You will put 5 ml (1 teaspoon) of special cream into your vagina. This helps embryos to hold tight inside your body. You will do this just after we place embryos into your body and every morning for 2 weeks (before pregnancy test). If the test shows you are pregnant, then you will do it for 4 more weeks. This is as easy and painless like us-‐ing a tampon. You could learn how to do this on this web site: http://www.crinone.com/.

Informed Consent Form V.1.0; Clinical trials: NCT01595334
8
3.6 Pregnancy tests Blood test. 13 days after embryo(s) returned to your body, we will take 10 ml of your blood. We will tell you if you are pregnant or not 6-‐7 hour later. Ultrasound study. If the blood test showed that you are pregnant, 4 weeks later we will
do the last ultrasound study to see the baby.
3.7 Phone calls • You will need to call to the Center at least 2 times to tell that your monthly bleeding has started. Please also call us if something wrong has happened to your health.
Informed Consent Form V.1.0; Clinical trials: NCT01595334
9
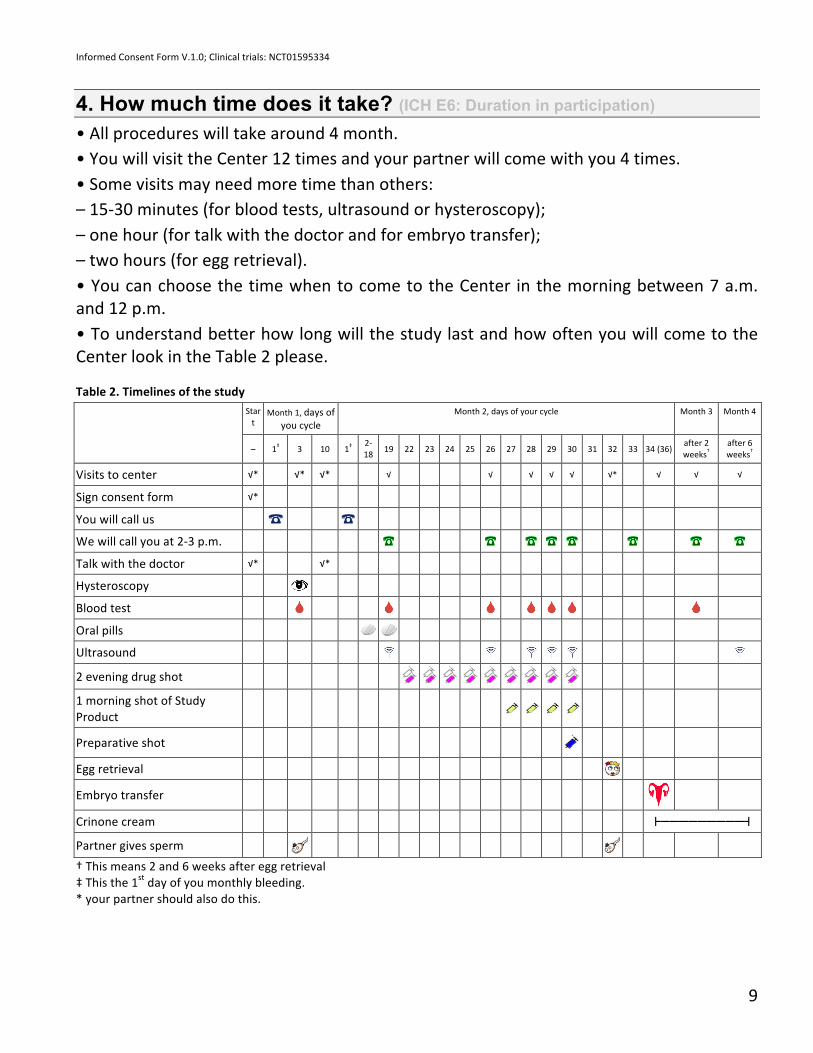
4. How much time does it take? (ICH E6: Duration in participation) • All procedures will take around 4 month. • You will visit the Center 12 times and your partner will come with you 4 times. • Some visits may need more time than others: – 15-‐30 minutes (for blood tests, ultrasound or hysteroscopy); – one hour (for talk with the doctor and for embryo transfer); – two hours (for egg retrieval). • You can choose the time when to come to the Center in the morning between 7 a.m. and 12 p.m. • To understand better how long will the study last and how often you will come to the Center look in the Table 2 please.
Table 2. Timelines of the study Star
t Month 1, days of
you cycle Month 2, days of your cycle Month 3 Month 4
– 1‡ 3 10 1‡ 2-‐18 19 22 23 24 25 26 27 28 29 30 31 32 33 34 (36)
after 2 weeks†
after 6 weeks†
Visits to center √* √* √* √ √ √ √ √ √* √ √ √
Sign consent form √*
You will call us
We will call you at 2-‐3 p.m.
Talk with the doctor √* √*
Hysteroscopy
Blood test
Oral pills
Ultrasound
2 evening drug shot
1 morning shot of Study Product
Preparative shot
Egg retrieval
Embryo transfer
Crinone cream ┣━━━━━━━━━┫
Partner gives sperm
† This means 2 and 6 weeks after egg retrieval ‡ This the 1st day of you monthly bleeding. * your partner should also do this.
Informed Consent Form V.1.0; Clinical trials: NCT01595334
10
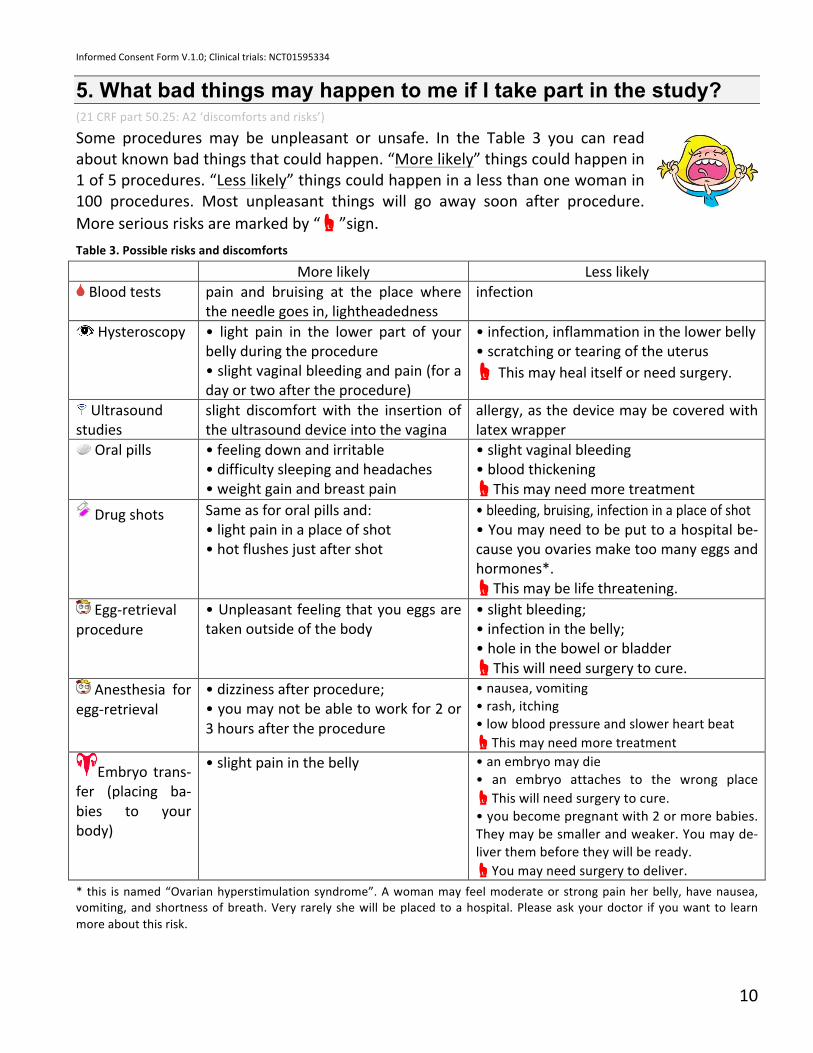
5. What bad things may happen to me if I take part in the study? (21 CRF part 50.25: A2 ‘discomforts and risks’)
Some procedures may be unpleasant or unsafe. In the Table 3 you can read about known bad things that could happen. “More likely” things could happen in 1 of 5 procedures. “Less likely” things could happen in a less than one woman in 100 procedures. Most unpleasant things will go away soon after procedure. More serious risks are marked by “☝”sign. Table 3. Possible risks and discomforts
More likely Less likely Blood tests pain and bruising at the place where
the needle goes in, lightheadedness infection
Hysteroscopy • light pain in the lower part of your belly during the procedure • slight vaginal bleeding and pain (for a day or two after the procedure)
• infection, inflammation in the lower belly • scratching or tearing of the uterus ☝ This may heal itself or need surgery.
Ultrasound studies
slight discomfort with the insertion of the ultrasound device into the vagina
allergy, as the device may be covered with latex wrapper
Oral pills • feeling down and irritable • difficulty sleeping and headaches • weight gain and breast pain
• slight vaginal bleeding • blood thickening ☝This may need more treatment
Drug shots Same as for oral pills and: • light pain in a place of shot • hot flushes just after shot
• bleeding, bruising, infection in a place of shot • You may need to be put to a hospital be-‐cause you ovaries make too many eggs and hormones*. ☝This may be life threatening.
Egg-‐retrieval procedure
• Unpleasant feeling that you eggs are taken outside of the body
• slight bleeding; • infection in the belly; • hole in the bowel or bladder ☝This will need surgery to cure.
Anesthesia for egg-‐retrieval
• dizziness after procedure; • you may not be able to work for 2 or 3 hours after the procedure
• nausea, vomiting • rash, itching • low blood pressure and slower heart beat ☝This may need more treatment
Embryo trans-‐fer (placing ba-‐bies to your body)
• slight pain in the belly • an embryo may die • an embryo attaches to the wrong place ☝This will need surgery to cure. • you become pregnant with 2 or more babies. They may be smaller and weaker. You may de-‐liver them before they will be ready. ☝You may need surgery to deliver.
* this is named “Ovarian hyperstimulation syndrome”. A woman may feel moderate or strong pain her belly, have nausea, vomiting, and shortness of breath. Very rarely she will be placed to a hospital. Please ask your doctor if you want to learn more about this risk.
Informed Consent Form V.1.0; Clinical trials: NCT01595334
11
Note, that you should not have unprotected sex when you do the shots. This also may be uncomfortable.
Warning! If you get pregnant when you do shots, it may cause harm to your unborn baby. (21 CRF part 50.25: B1. unforeseeable risks)
Warning! The Study Products were approved by FDA, but they are new. So there also may be other risks or bad things that we cannot predict. The par-‐ticipation in this study may even harm your unborn baby.
5.1 Research injury If you think that drugs, study products or procedures injured you, please let your Study Doctor know right away. This is named “research injury”. Research injury is any injury to your body (not to your mind) DIRECTLY caused by procedures listed in the sec-‐tion “3. What will happen if I take part in this research study?”. For example, is you get injured when you travel to the Center it is not a “research injury”
Informed Consent Form V.1.0; Clinical trials: NCT01595334
12
6. Will somebody help me if one of those bad things happen? (21 CRF part 50.25: A6. compensation and/or medical treatment available if injury occurs)
We will not pay you if you will be injured We will do our best to keep all bad events away during the study. If “re-‐search injury” happen, Southern Cross Fertility Centre WILL NOT provide your any financial compensation. That mean that we will not pay you for the lost salary or your pain and suffering. We may pay you only for MED-‐ICAL CARE to treat a “research injury”.
We may pay for your treatment in some cases • Southern Cross Fertility Centre will pay for the treatment: 1. for any “Less likely” bad event listed in the Table 3 that need to be treated. The “More likely” bad events listed in the Table 3 will go away soon after procedures. They do not need any treatment; 2. for any other “research injury” during this study or 10 days after you stop to participate. • In those two cases, Southern Cross Fertility Centre will pay – all money if you do not have an insurance or are not covered by a government program; – or part of money that is not covered by your insurance or a government program. Please ask your insurance company about their rules. • Southern Cross Fertility Centre will pay for your treatment in Alpha, Beta or Gamma hospitals. If you will chose any other hospital, Southern Cross Fertility Centre will not pay for your treatment. • Southern Cross Fertility Centre WILL NOT compensate and pay for treatment: – for any bad event that WERE NOT caused by drugs or procedures during this study or that happen more than 10 days after you stop to participate;
– if your child was born unhealthy; – if you stopped the study suddenly before it was finished and did not tell your Study Doctor. (The rules how to stop the study safely are listed in the chapter “11. Stopping being in the study before it study ends”.) – if you did not follow doctors recommendation. (This means that you were not responsible for your duties listed in the chapter “1. Introduction”.)
The payment described in this section will be the only money Southern Cross Fertility Centre will pay you for any research injuries caused by this study. You are not giving up any of your legal rights by signing this form.

Informed Consent Form V.1.0; Clinical trials: NCT01595334
13
7. Benefits that I may get from the participation (21 CRF part 50.25: A3. benefits) All drugs, Study Products and procedures that are used in this study were approved by FDA. That means that they are reasonably safe and helpful.
Figure 1 shows how many women became pregnant after we treated them the same way we use in this study. The younger you are the more likely that you will become pregnant. Your success may also depend on the other things: – how old is your male partner? – do you have children? – some other things that you may want to talk about with your family doctor or Study Doctor.
Figure 1. Chances to become pregnant with the first IVF procedure done in our Center. We used either Cetrorelix or Luprolide Acetate. Now we want to know: which of them works better?
You may benefit from this study if you could not get pregnant because of: • problems with your heath: disease of your uterus, tubes, or ovaries; • problems with your male partner health: too little sperm cells, “lazy” or “weak” sperm cells; • when your body “kills” your partner’s sperm cells; • when you and your family doctor do not knows the reason. Note! Ask your family doctor if you will benefit from participation in this study. You participation may also help other women who cannot have a baby. We will understand which Study Product, Cetrorelix or Lu-‐prolide Acetate, works better and will use only this drug in future. (ICH E6: Will be informed of any new information in timely manner) Before the study ends, we may learn some good or bad things
about the Study Product we test. We will tell you about this right away. (21 CRF part 50.25: B5. new findings will be provided to the subject) After the end of the study we will send you a letter. In this letter we will tell you about any important results that we got from the study. You may also call us or come to the Center to learn about these results.
Informed Consent Form V.1.0; Clinical trials: NCT01595334
14
8. What are the other ways to help me if I will not participate? (21 CRF part 50.25: A4. alternative procedures)
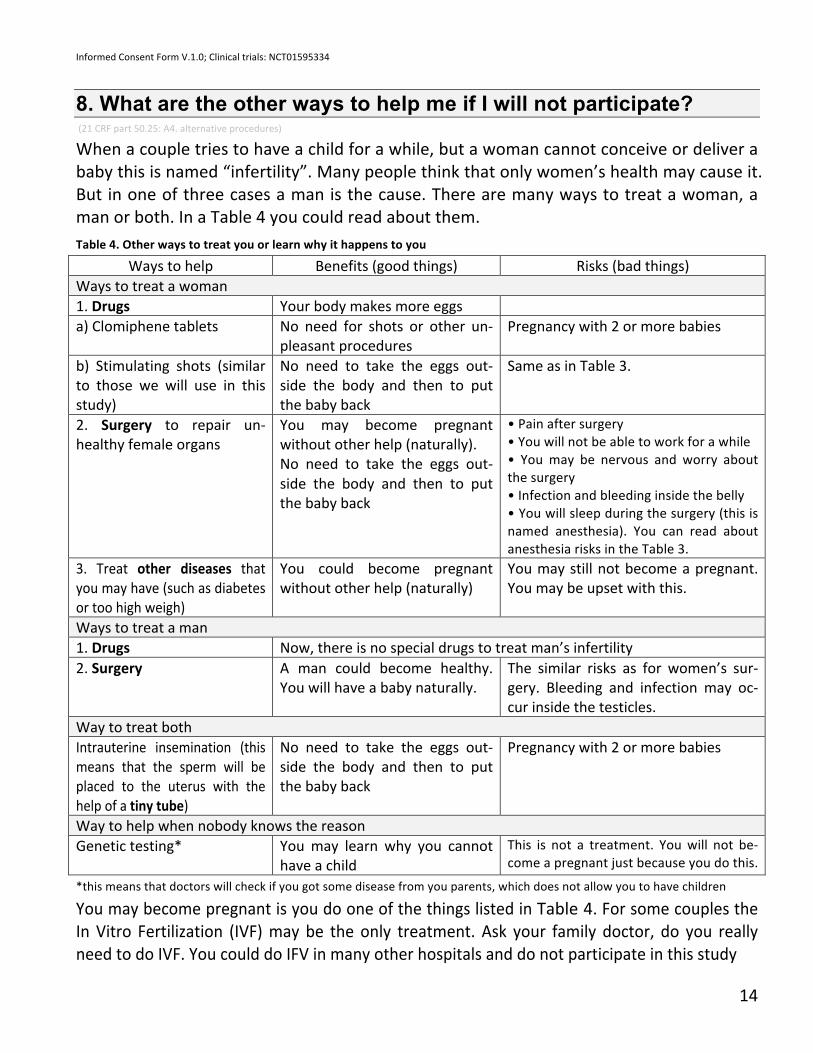
When a couple tries to have a child for a while, but a woman cannot conceive or deliver a baby this is named “infertility”. Many people think that only women’s health may cause it. But in one of three cases a man is the cause. There are many ways to treat a woman, a man or both. In a Table 4 you could read about them. Table 4. Other ways to treat you or learn why it happens to you
Ways to help Benefits (good things) Risks (bad things) Ways to treat a woman 1. Drugs Your body makes more eggs a) Clomiphene tablets No need for shots or other un-‐
pleasant procedures Pregnancy with 2 or more babies
b) Stimulating shots (similar to those we will use in this study)
No need to take the eggs out-‐side the body and then to put the baby back
Same as in Table 3.
2. Surgery to repair un-‐healthy female organs
You may become pregnant without other help (naturally). No need to take the eggs out-‐side the body and then to put the baby back
• Pain after surgery • You will not be able to work for a while • You may be nervous and worry about the surgery • Infection and bleeding inside the belly • You will sleep during the surgery (this is named anesthesia). You can read about anesthesia risks in the Table 3.
3. Treat other diseases that you may have (such as diabetes or too high weigh)
You could become pregnant without other help (naturally)
You may still not become a pregnant. You may be upset with this.
Ways to treat a man 1. Drugs Now, there is no special drugs to treat man’s infertility 2. Surgery A man could become healthy.
You will have a baby naturally. The similar risks as for women’s sur-‐gery. Bleeding and infection may oc-‐cur inside the testicles.
Way to treat both Intrauterine insemination (this means that the sperm will be placed to the uterus with the help of a tiny tube)
No need to take the eggs out-‐side the body and then to put the baby back
Pregnancy with 2 or more babies
Way to help when nobody knows the reason Genetic testing* You may learn why you cannot
have a child This is not a treatment. You will not be-‐come a pregnant just because you do this.
*this means that doctors will check if you got some disease from you parents, which does not allow you to have children
You may become pregnant is you do one of the things listed in Table 4. For some couples the In Vitro Fertilization (IVF) may be the only treatment. Ask your family doctor, do you really need to do IVF. You could do IFV in many other hospitals and do not participate in this study
Informed Consent Form V.1.0; Clinical trials: NCT01595334
15
9. How will you protect and use my personal information? (21 CRF part 50.25: A5. confidentiality)
We will protect your personal information as required by the law (HIPAA Privacy Rule). But during the study we will give your personal information to other responsible people. We need to do it to prove that we did everything right and that you are safe.
9.1 What does “personal identifiable infor-mation” mean? “Personal Identifiable information” (PII) means all data that may let others to find or rec-‐ognize you. For this study we will record PII about you and some other people: • your name, addresses (home and work), date of birth, phone numbers, electronic mail address, social security number, medical records number, full face photograph; • name, address, date of birth, phone number, full face photograph, and place of work of your male partner; • names, addresses, electronic mail address, and phone numbers of two your family members or close friends.
We will keep this Personal Identifiable information in a secure areas. Pa-‐per documents will be stored in a safe at the ground floor of the Center building. Electronic records will be stored in protected computer files on Dr. Irani’s computer in his office. We will store this information for 2 years after we finish the study (or longer if the Sponsor will decide to do this).
Then we will destroy all paper information with a shredder. All electronic data will be erased by Dr. Irani. The security department of the Center will control this (To read more about the protection of your PII ask your Study Doctor for the “Privacy Notice” of South-‐
ern Cross Fertility Centre.) We will give you a “secret code” to hide your information. The list that matches your name with the code number will be kept in a protected file on Dr. Irani computer in his office. The samples of blood, your eggs and embryos will be labeled only with your secret code, but not with your name.
If we will publish or present any results of from this research study, no personally identifi-‐able information will be shared. We also will not share you personal information in the description of this study on http://www.ClinicalTrials.gov, as required by the law.
Informed Consent Form V.1.0; Clinical trials: NCT01595334
16
9.2 What other personal information will we gather? We will also gather and record some personal information about your health (“health in-‐formation”) such as: – results of all blood tests and procedures listed in the section “3. What will happen if I take part in this research study?; – records about your phone talks with the Study Team during the study; – records about your visits to the Center and talks during the visits; – records from your PCP and female doctor that you will share with us; – records about drugs and Study Product you will take during the study; – records about “research injuries” and other changes in your health during the study; – your signed informed consent form (the paper you reading now). This information is also protected by the law. All health records will be kept and protected in the same way as your personal identifiable information.
9.3 Who may read or use my personal information?
Your personal identifiable information and health information: – you may read it (you cannot copy this information or use it any other way before the study is finished); – Study Team of Southern Cross Fertility Centre may read and use (copying, calculations); – Study Team may give this information to governmental organisation such as:
1. FDA (The U.S. Food and Drug Administration); 2. Department of Health and Human Services (DHHS) agencies; 3. Governmental agencies to whom certain diseases must be reported. 4. Governmental agencies in other countries where we will use the Study Products. 5. The Southern Cross Fertility Centre Human Subjects Protection Office
– Study Team may also give this information to Institutional Ethics Review Board (IERB) of Jawaharlal Nehru University (you may read about IERB in the section “12. How to contact the Center and other organizations?”)
Your health information
You health information will be given to the sponsor of this study (you may read about the sponsor in the section “1.5 Who pays for this study?”). “Sponsor” includes any person or organization who works with/for sponsor in this study. All your personal identifiable in-‐formation will be removed from your health records. Sponsor will see only your “secret code” and health data.
Informed Consent Form V.1.0; Clinical trials: NCT01595334
17
9.4 Why do I need to give my permission? You will give you permission to use and give your personal information to the people and organizations listed above for three reasons: 1. to protect your safety and safety of the people in your community; 2. to finish the study and calculate its results; 3. to make the study legal and its results useful for other people.
9.5 What if I do not agree to give my personal information? • If you will not agree to give you personal information to the people and organizations listed in section 9.3, you cannot be in the study. • Your permission will continue until the Sponsor notifies the Study Team that the infor-‐mation is no longer needed or you will cancel your permission.
9.6 May I cancel my permission to use and give my personal in-formation? • Yes, you may do this. To cancel your permission you must write a paper letter to Dr. Ira-‐ni. This is named “cancellation letter”. For Dr. Irani’s mailing address see the section “12. How to contact the Center and other organizations?”) Note! We cannot take back any personal information that has been already given to oth-‐ers before we received your “cancellation letter”. • You may decide to pull out (cancel) your permission any time DURING the study. This will mean that you will stop participation in the study. Your information gathered before we receive your “cancellation letter” still will be used and given to others. • You may decide to pull out your permission any time AFTER the study. This will mean that you will pay for all drugs (expect Study Product) and procedures done during the study. After we receive your “cancellation letter” and payment, we will destroy you per-‐sonal information and will not use it or give it to others. (Except the records of the medi-‐cal care that was given to you, as it is required by law.)
9.7 Can you promise that my information will be fully protected? We cannot promise this. We will do our best to protect your personal information, but we need to share it with others. There is the risk that that other people may become aware of your personal information without your permission.
Informed Consent Form V.1.0; Clinical trials: NCT01595334
18
10. Do I need to pay for participation or you will pay me? (ICH E6: Prorated payment and expenses, 21 CFR 50.25 B3. additional cost to the subject)
• You and your male partner do not need to pay for participation in this study. The South-‐ern Cross Fertility Centre will pay for all drugs and procedures. • We will give $50 for each study visit listed in Table 2. We will give you money after you will finish the visit and do all necessary procedures. This means that for all 12 visits you will be paid $600. This money will be paid you for your time and transportation to the Center. • If you will stop participation in the study we will pay you only for the visits you did ($50 for each visit). • We will not pay any money for your male partner.
Informed Consent Form V.1.0; Clinical trials: NCT01595334
19
11. Stopping being in the study before it study ends (ICH E6: Reasons for termination of participation, 21 CFR 50.25 B2. termination of subject’s participation by the investigator without regard to the subject's consent)
If you will decide to take part in this study and even will do some procedures, you can stop doing this. Why it could happen and what to do next?
11.1 You may decide to stop the study because: • you do not like it. It is too uncomfortable for you or your partner; • bad things happened in your family or at your work; • you decided to use another way of treatment; • the Study Doctor told you that they learn that the study was more risky that they though before; • you decided to pull out your permission to give your personal in-‐formation to the people and organizations listed in the section “9.3 Who may read or use my personal information?” You do not have to tell anybody WHY did you decide to stop. It is only you who will decide to stay in the study or not. (You doctor also may want you to leave in some cases). But it will be better that you ask your Study Doctor WHAT TO DO next.
Warning! It may be unsafe if you stop the study suddenly and do not tell anybody that your are leaving!
12.1 Your Study Doctor may decide that you have to leave the study. The doctor may do this EVEN IF YOU STILL WANT TO BE IN THE STUDY, because it may be no longer useful and/or safe for you to continue. Here are the reasons (one reason is enough to stop your participation):
When it is not useful for you:
• After the first blood test or hysteroscopy (study of the uterus) the Study Doctor learned that you body could not make eggs or bear a baby. • You partner do not make sperm cells at all
(Note! You may chose to use donor sperm and stay in the study); • Your body did not respond to the drugs and research products the Study Doctor used in the study.
When it is not safe for you: • The doctor learned that your health got worse during the study. • The doctor learned that the study drugs were not safe. Note! The doctor WILL NOT stop your medical care even if the sponsor decided that the research product did not work as good as (s)he wanted. Sponsor may even stop the study.
Informed Consent Form V.1.0; Clinical trials: NCT01595334
20
But if the Study Doctor is still sure that it will be useful and safe for YOU, you will receive all procedures listed in Table 2 for free.
When it is both useless and not safe for you: This may happen if you did not follow the doctors recommendation. For example: • you forgot to take oral pills or to do shots more then 2 times in a row or more than the 3 times during the whole study; • you forgot to do the last “Preparative shot” or did it 12 or more hours later or sooner and did not call to the Center; • you did not come to the center for blood tests and ultrasound more then 2 times in a row or more than the 3 times during the whole treatment; • you did not appear to the center for egg retrieval or embryo transfer;
☎ We could change the time for egg retrieval for a while only BEFORE you did the “Preparative shot”. Please call us if you want to do so. We cannot change the time for embryo transfer (putting baby to your body) because the baby may die.
• you had unprotected sex and got pregnant when you did shots. Warning! It may cause harm to your unborn baby
• your partner did not appear for spermogram and/or did not give his sperm for fertiliza-‐tion.
What will happen to me if I stop to participate by any reason? 21 CFR 50.25 B4 ‘consequences of a subject’s withdrawal from the study’ Warning! It may be unsafe to stop the study suddenly and cause harm to your body or
your unborn babies. Safe steps to stop participation:
1. Tell your doctor that you do not want to participate any longer. 2. The Study Doctor will explain you what is happening with your body right now. The most unsafe things may happen when you just started to do the shots or when you did most of shots. The Study Doctor may tell you not to work hard, do not to lift heavy things, or even to stay in a hospital for a while. 3. The Study Doctor will call your family doctor or women doctor. They will call you and tell what to do next. You may still be treated in the Center if you stopped your participation in the study, but you have to pay for the treatment.

Informed Consent Form V.1.0; Clinical trials: NCT01595334
21
12. How to contact the Center and other organizations? (21 CRF part 50.25: A7. name address, phone numbers of contact persons)
You may want to contact Southern Cross Fertility Centre if: – you decide to participate in the study; – you have questions about the study or your participation; – you decide to stop your participation in the study.
• Contact: Dr. Faram Irani, MD. Southern Cross Nursing Home, Ground Floor, United Western Apart-‐ments, Prabhadevi (Land Mark: Near Kismat Cinema) Bombay-‐400025. Maharashtra, India ☎ Tel: 91-‐9892211941 ✍E-‐mail: [email protected]
Note! Doctor Irani works for the same organization that pays for the study (the Sponsor). • If you already in the study and some emergency happened with your body (such as “re-‐search injury”), please call the “study hotline” anytime ☎ +91-‐22-‐24374133,
☎ +91-‐22-‐24377994 If you cannot reach the Center or wish to talk to someone else about the study or think that you was injured during the study please contact a research participant protection advocate, such as: Keryl Jones, RN
CTSI Research Participant Advocate & IRB Navigator in the Medical College of Wisconsin, Subjects Protection Office ☎ Tel. (414) 805-‐7321
You also may contact the institutional ethics review board (IERB). IERB is a group of peo-‐ple who checks this research study to protect your rights:
Prof. Amita Singh Institutional Ethics Review Board, Room numbers 102 & 103 Old CRS Building, Aruna Asaf Ali Marg Jawaharlal Nehru University New Delhi-‐ 110067 ☎ Tel: +91-‐11-‐26704697 ✍ Email: [email protected]
The study will also be monitored by Sponsor
Informed Consent Form V.1.0; Clinical trials: NCT01595334
22
Ask you questions Please ask the Study Doctor any questions about the study and your rights. You may like to write the questions before you will come to the Center: __________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
References 1. Johns Hopkins Medicine Health Library http://www.hopkinsmedicine.org/healthlibrary 2. In vitro fertilization (IVF) Risks -‐ Mayo Clinic http://www.mayoclinic.org/tests-‐procedures/in-‐vitro-‐fertilization/basics/risks/prc-‐20018905 3. http://www.hunterivf.com.au/ivf-‐success-‐rates 4. Center for Infertility and Reproductive surgery at Brigham and Women's Hospital http://infertility.brighamandwomens.org 5. CFR (Code of Federal Regulations) Title 21 Part 50. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=50.25 6. ICH E6
Informed Consent Form V.1.0; Clinical trials: NCT01595334
23
CONSENT I have read the information in this consent form (or somebody read it to me). The Study Team answered all my questions about the study. I freely consent (agree) to participate in this research study. I permit the release of my medical records for research or regulatory purposes to the sponsor, the FDA, DHHS agencies, governmental agencies in other countries, and Institutional Ethics Review Board of Jawaharlal Nehru University. By signing this consent form I have not waived any of the legal rights which I otherwise would have as a subject in a research study. ________________________________________ Subject Name ________________________________________ __________________ Signature of Subject Date ________________________________________ __________________ Signature of Person Conducting Informed Date Consent Discussion

















