Embed Size (px)
Citation preview
![Page 1: Influence of early prehospital thrombolysis on mortality and event-free survival (The Myocardial Infarction Triage and Intervention [MITI] Randomized Trial)](https://reader042.dokumen.tips/reader042/viewer/2022020605/5750749e1a28abdd2e956657/html5/page/1.jpg)
Influence of Early Prehospital Thrombolysis on Mortali
3 and Event-
Free Survival (The Myocar ial Infarction Triage and Intervention [ MlTl]
Randomized Trial) Marc A. Brouwer, MD, Jenny S. Martin, RN, Charles Maynard, PhD, Mark Wirkus, BS,
Paul E. Litwin, MS, Freek W.A. Verheugt, MD, and W. Douglas Weaver, MD, for the MIT1 Project Investigators
The Myocardial Infarction Triage and Intervention Trial of prehospital versus hospital administration of throm- bolytic therapy markedly reduced hospital treatment times, but the 2 groups had similar outcomes. However, patients treated <70 minutes from symptom onset had better short-term outcomes. The purpose of this study was to determine the long-term influence of very early thrombolytic treatment for acute myocardial infarction. A total of 360 patients were followed for vital status and cardiac-related hospital admissions over a period of 34 t 16 months. Patients enrolled in the trial had symptoms for 56 hours, ST-segment elevation on the prehospital electrocardiogram, and no risk factors for serious bleed- ing. They received aspirin and recombinant tissue plas- minogen activator either before or after hospital arrival. Primary end points in this study included long-term sur-
T hrombolytic therapy has been proven to reduce early mortality and to improve l-year survival
rates in patients with acute myocardial infarction.le7 The greatest mortality reduction is shown in patients who receive treatment within the first 1 to 2 hours after symptom onset. 3s,6,8 In several studies that have determined the components of treatment delay, pa- tient decision time and hospital treatment times each could account for 2 1 hour.8-” Prehospital initiation of thrombolytic therapy might therefore provide the opportunity to treat a large proportion of patients within the first 2 hours of symptom onset. Two trials of prehospital thrombolytic therapy demonstrated significant reductions in time to treatment, although
From University Hospital, Niimegen, The Netherlands; and the Uni- versitv of Washinaton Medical Center. Seattle. Washinaton. This study’was supportgd in Heart, Lung, and Bloo
art by Grant ROl HL38.54 from th<National
stricted grants from Genetech Inc., South San Francisco, Maraueite Electronics. Milwaukee. Wisconsin. and Pharmacia Del- tee, St. Paul, Minnesdta. Marc A. ‘Brouwer ardtefullv acknowledaes the financial support of The Dutch Heart Ass&iation,‘Den Haag, The Netherlands, Boehringer Ingelheim, Alkmaar, The Netherlands, MSD- Pharma, Haarlem, The Netherlands, The Free University of Amster- dam, Amsterdam, The Netherlands, and Hewlett-Packard, Amstel- veen, The Netherlands. Manuscriot received December 29. 199.5. revised manuscript received and accepted March 1 1, 1996.
Address for reprints: W. Douglas Weaver, MD, MIT1 Coordinat- ing Center, 19 10 Fair-view Avenue East, Suite 20.5, Seattle, Wash- ington 98 102.
0 1996 by Excerpta Medico, Inc 0002.9 149/96/s 15.00 All rights reserved. PII SOOO2-9149(96)00352-9
viva1 and survival free of death or readmission to the hospital for angina, myocardial infarction, congestive heart failure, or revascularization. Two-year survival was 89% for prehospital- and 91% for hospital-treated patients (p = 0.46). Event-free survival at 2 years was 56% and 64% for prehospital- and hospital-treated pa- tients, respectively (p = 0.42). In patients treated ~70 minutes from symptom onset, 2-year sunrival was 98%, and it was 88% for those treated later (p = 0.12). Two- year event-free survival was 65% for patients treated early and 59% for patients treated later (p = 0.80). In this trial, poorer long-term survival was associated with advanced age, history of congestive heart failure, and coronary artery bypass surgery performed before the index hospitalization, but not with time to treatment.
(Am J Cardiol 1996;78:497-502)
mortality in the prehospital and hospital groups was not significantly different.12,13 In the Myocardial In- farction Triage and Intervention (MITI) prehospital trial, time to treatment was reduced by 33 minutes in the prehospital group. In addition, patients treated <70 minutes from symptom onset had lower mor- tality, smaller infarct size, and improved left ventric- ular function.13 Over the years, several studies re- porting the long-term influence of thrombolytic therapy have been published.14-l6 The purpose of the current study was to determine whether the benefits of very early treatment were sustained in the years after discharge from the hospital.
METHODS Patient population: All patients who called 9 11 and
had chest pain were evaluated by the 15 paramedic units in the Seattle metropolitan area. Using a checklist with inclusion and exclusion criteria, par- amedics gathered information on the patients’ clini- cal presentations. This information enabled hospital- based physicians to determine whether the patients were candidates for thrombolytic therapy. Patients were excluded from participating in the trial for the following reasons: ( 1) chest pain >6 hours from symptom onset, (2) age >75 years, or (3) the pres- ence of complicating illnesses that were considered to be contraindications for prehospital thrombolytic therapy. Detailed information on the study protocol
497
![Page 2: Influence of early prehospital thrombolysis on mortality and event-free survival (The Myocardial Infarction Triage and Intervention [MITI] Randomized Trial)](https://reader042.dokumen.tips/reader042/viewer/2022020605/5750749e1a28abdd2e956657/html5/page/2.jpg)
B Pa.46 by log rank
$ 3 .7 &
.6- Prehospital
Hospital
.5 i ~---~- -.-~ .-- ._ --I- __~-- 1
0 1 2 3 4 5
Years
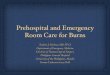
FIGURE 1. Cumulative survival curves for the prehospital and hospital groups. No statistically significant difference was observed (p = 0.46).
1.0.
P=O.42 by log rank
---- Prehospital
.4 - Hospital
FIGURE 2. Event-free survival analysis of 360 randomized patients allocated to prehospi- tal- or hospital-initiated throm- bolytic therapy. There was no statistically significant differ- ence between the groups (p = 0.42).
and criteria for patient selection have been pub- lished.11,13
Briefly, a 1Zlead prehospital electrocardiogram was obtained in the subset of patients who satisfied the criteria for enrollment. The final decision to ran- domize the patient was made by a physician in the emergency department of 1 of 6 paramedic base hos- pitals. Paramedics used a standard verbal consent to enroll patients into the study. After enrollment, pa- tients were randomized to receive aspirin and recom- binant tissue plasminogen activator either before or
after hospital arrival. Intravenous sodium heparin was administered to both patient groups at the time of hospital arrival. After hospital discharge, 289 pa- tients underwent radionuclide measurements of in- farct size and left ventricular ejection fraction.
follow-up: To determine survival status and the need for readmission to the hospital for cardiac rea- sons, mail questionnaires were sent to patients an- nually. Patients were queried concerning hospital ad- missions for the following reasons: ( 1) angiography, (2) coronary angioplasty, (3 ) coronary artery bypass
498 THE AMERICAN JOURNAL OF CARDIOLOGY@ VOL. 78 SEPTEMBER 1, 1996
![Page 3: Influence of early prehospital thrombolysis on mortality and event-free survival (The Myocardial Infarction Triage and Intervention [MITI] Randomized Trial)](https://reader042.dokumen.tips/reader042/viewer/2022020605/5750749e1a28abdd2e956657/html5/page/3.jpg)
TABLE I Observed Cardiac-Related Events for Both Randomized Groups and the Subgroups
Number of Events/l 00 Number of Events Patients/Year
Prehospital Hospital Prehospital Hospital Event (n = 175) (n = 185) (n = 175) (n = 185) pValue
Angiography 54 70 1 1.5 13.8 0.37 Angioplasty 34 43 7.0 8.5 0.45 Bypass surgery 20 20 4.1 4.0 0.90 Congestive heart failure 12 13 2.6 2.5 0.94 Myocardial infarction 22 21 4.3 4.3 0.98 Recurrent ischemia 24 40 4.9 7.9 0.11
Total 166 207 34.2 41.0 0.28
surgery, (4) congestive heart failure, (5) chest pain, or (6) subsequent myocardial infarction. In addition to the mail questionnaires, hospital admission logs were screened for cardiac-related admissions. Infor- mation about procedures and admission and dis- charge diagnoses was also recorded. Telephone con- tact with patients or surviving relatives often enabled us to complete missing information. Finally, the Na- tional Death Index was used to ascertain vital status for patients who were lost to follow-up.
Statistical methods: The primary end points of this study were survival and event-free survival, defined as survival free of death, myocardial infarction, or hospitalization for angina, congestive heart failure, or revascularization. Survival analyses included deaths from all causes. Survival curves for all groups were obtained according to the method of Kaplan and Meier.17 The log rank test was used to determine whether survival and event-free survival were dif- ferent according to randomization group and time to
FIGURE 3. Cum&Hive survival curves for patients treated very early (<70 minutes) versus those treated later (70 minutes to 3 hours). The observed dif- ference was not stutisticaliy significant (p = 0.12).
treatment, dichotomized by a 70- minute cutpoint. Stepwise Cox re- gression analysis was used to iden- tify factors related to long-term survival; variables were included in the model if the p value for inclu- sion was <0.05. To compare the numbers of cardiac-related hospital admissions, we calculated the aver- age number of events per patient per follow-up year. Baseline character- istics and clinical outcomes were compared by the chi-square test for discrete variables and the t test for continuous variables.
RESULTS Of all 360 patients, 175 were randomized to re-
ceive prehospital-initiated thrombolytic therapy, and the other 185 were allocated to thrombolytic treat- ment after hospital arrival. Baseline characteristics of these patients have been described.13 Cardiac his- tories and hemodynamic findings did not differ sig- nificantly between the groups, and baseline electro- cardiographic findings were also similar: Anterior infarction occurred in 39% (p = 0.99) and inferior infarction in 58% (p = 0.99) of both groups. Patients in the hospital group were slightly older than their counterparts (59 + 10 years in the prehospital group vs 57 +- 10 years in the hospital group; p = 0.04). Time from symptom onset to treatment differed sig- nificantly; the median time to treatment for the pre- hospital group was 77 minutes (56 and 101; 25th and 75th percentiles), and it was 110 minutes (85
““d .9 i -L-%- x-- 7----L
%-
L
L-----------------
P=O.12 by log rank
> = 70 minutes
< 70 minutes
Years
CORONARY ARTERY DISEASE/lONGTERM OUTCOME IN MIT1 499
![Page 4: Influence of early prehospital thrombolysis on mortality and event-free survival (The Myocardial Infarction Triage and Intervention [MITI] Randomized Trial)](https://reader042.dokumen.tips/reader042/viewer/2022020605/5750749e1a28abdd2e956657/html5/page/4.jpg)
.8- .8-
a a
i .I i .I z z 8 8 b b 4 4
.6- I .6- I
P=O.80 by log rank P=O.80 by log rank
---- ---- L--. L--. >= 70 minutes >= 70 minutes
< 70 < 70 minutes minutes
2 2 3 3 4 4 5 5
Years Years
FIGURE 4. Event-free rurvival analysis for patient5 healed very early (< 70 minutes) ver- sus Ihose lreabcl later (70 minute5 to 3 hours). The curve5 were similar (p = 0.80).
and 140; 25th and 75th percentiles) for the hospital group (p <O.OOOl).
Overall, 336 patients received thrombolytic ther- apy in either the prehospital or the hospital setting; 24 did not receive thrombolytic treatment for varying reasons.13 In nearly 25% (82 of 336) of the patients receiving thrombolytic therapy, time from symptom onset to treatment was <70 minutes. Most were treated later ; 254 patients received thrombolytic therapy between 70 minutes and 3 hours of symptom onset.
The baseline characteristics of patients treated early (<70 minutes) and of those treated later were similar. Patients in the early group were slightly younger, although this difference was not statisti- cally significant (56 + 10 years in the early-treated patients vs 58 + 10 years in the later-treated patients; p = 0.05 1) . Time to treatment showed a distinct dif- ference: The median time to treatment was 55 minutes (49 and 63; 25th and 75th percentiles) for the early-treated patients compared with 104.5 minutes (85 and 141; 25th and 75th percentiles) for those who were treated later.
In the first year of follow-up, 31 patients died; information on cardiac-related events was available for 97% of patients. With the National Death Index and returned follow-up letters, it was possible to as- certain vital status for all patients. Figure 1 shows cumulative survival curves for the prehospital and hospital groups. There was no significant difference in long-term survival between the groups; 2-year sur- vival was 89% for prehospital-treated patients and 91% for those treated in the hospital setting (p = 0.46). Event-free survival also did not differ accord-
ing to randomization group (Figure 2). Two years after enrollment, event-free survival was 56% and 64% in the prehospital and hospital groups, respec- tively (p = 0.42).
To determine whether patients differed in the number of cardiac-related events, we calculated event rates for both groups (Table I). The prehos- pita1 group showed a slightly lower number of car- diac-related admissions (p = 0.28). Overall, there was a difference of 68 cardiac-related events per 1,000 patients per year (Table I). Hospital read- mission rates at 1 and 2 years of follow-up were also determined. For the prehospital group, 31% and 36% of patients were rehospitalized at 1 and 2 years, respectively. In the hospital group, 25% of patients were readmitted at 1 year and 3 1% at 2 years (p = 0.65).
During the first year of follow-up, 28 of 336 pa- tients who received thrombolytic therapy died. In- formation on cardiac-related events was available for 96% of surviving patients. Figure 3 shows the long- term survival for the group that was treated very early versus the group that received thrombolytic agents 270 minutes from symptom onset. Unad- justed survival in the early-treatment group appeared to be improved, but the difference was not statisti- cally significant, because the survival curves crossed after 3 years. Two-year survival was 98% for the early-treated patients and 88% for those who re- ceived thrombolytics later (p = 0.12).
Figure 4 shows that there was no significant dif- ference in event-free survival between the very early and the later-treated group. Event-free survival at 2 years was 65% for the early group and 59% for the
500 THE AMERICAN JOURNAL OF CARDIOLOGY” VOL. 78 SEPTEMBER 1, 1996
![Page 5: Influence of early prehospital thrombolysis on mortality and event-free survival (The Myocardial Infarction Triage and Intervention [MITI] Randomized Trial)](https://reader042.dokumen.tips/reader042/viewer/2022020605/5750749e1a28abdd2e956657/html5/page/5.jpg)
TABLE II Observed Cardiac-Related Events far Patients Treated Very Early and Those Treated later
to treatment of only 33 minutes, in- stead of the expected time of 21 hour.13 This. combined with the
Event <70 min 270 min t70 min 270 min (n = 82) (n = 254) (n = 82) (n = 254)
Angiography 27 89 11.0 13.1 Angioplasty 22 46 9.0 6.8 Bypass surgery 9 29 3.7 4.3 Congestive heart failure 4 19 1.6 2.8 Myocardial infarction 8 35 3.3 5.1 Recurrent ischemio 11 49 4.5 7.2
Total 81 267 33.0 39.2
Number of Events Number of Events/l 00
Patients/Year
p Value
0.45 0.35 0.69 0.38 0.18 0.18 0.35
later group (p = 0.80). Event rates were similar in the 2 groups (Table II). Readmission rates at 1 and 2 years of follow-up were 30% and 33%, respec- tively, for the early-treated patients and 27% and 33% for those treated later. These differences were not statistically significant (p = 0.74).
To identify factors that were related to long-term survival, we performed stepwise Cox multivariate regression analysis in 329 patients with complete in- formation. Advanced age, a history of heart failure, and bypass surgery performed before the index hos- pitalization were associated with decreased survival. After adjustment for these variables, treatment <70 minutes from symptom onset was not associated with survival (p = 0.30). In addition, time to treat- ment measured as a continuous variable was not pre- dictive of long-term survival (p = 0.84).
DISCUSSION Time to treatment is an important predictor of
hospital mortality.3,8.13 The earlier thrombolytic treat- ment is initiated, the more myocardium is saved and the better the clinical outcome. According to this hy- pothesis, outcome would be best in patients treated very early. We conducted this follow-up study to assess the long-term influence of very early initiation of thrombolytic therapy.
There was a trend toward improved long-term survival after very early thrombolysis. This benefit resulted primarily from a much more favorable in- hospital mortality rate for patients treated very early. Moreover, readmission rates and event-free survival were not influenced by a substantial reduction in time to treatment. Therefore, despite the major im- pact of early treatment on short-term mortality, the influence on long-term clinical outcome was less im- pressive. The benefits of very early treatment are im- mediate; with the passage of time, other factors, in- cluding age and gender, as well as the use of aspirin, p blockers, risk factor reduction, or revascularization procedures, become preeminent for all patients.
Survival curves for the prehospital- and hospital- treated patients were similar. These findings may have been influenced by the unanticipated reduction of 40 minutes in hospital treatment times in this study. l3 Consequently, prehospital initiation of thrombolytic therapy resulted in a reduction in time
conservative’ selection criteria and the relatively low patient numbers, might have prevented the difference between treatment groups that was expected.
In the analysis of early treatment, the earlier reported 30-day survival benefit for patients treated <70 minutes from symptom onset re- sulted in markedly improved sur- vival in this group. This gain was caused primarily by a lower number
of in-hospital deaths for the early-treated patients. Considering the entire follow-up period, the ob- served difference between curves was not statisti- cally significant (p = 0.12). In addition, results from Cox regression analysis indicated that early treat- ment was not associated with long-term survival. These findings do not suggest that very early treat- ment exerts an additional salutary effect that was re- alized in the first month after treatment.
Event-free survival was not influenced by a re- duction in time to treatment. Readmission rates and event rates also did not differ significantly. The slightly higher event-free percentages in the very early-treated group were caused by the fewer deaths in this group and not by a difference in hospital ad- missions for cardiac events. These findings do not support the hypothesis that early treatment would re- sult in improved overall cardiac status and thus fewer subsequent admissions. A Dutch study has suggested that freedom from reocclusion does result in im- proved long-term event-free survival.‘8
Follow-up in the MIT1 prehospital thrombolysis trial demonstrated that short- and long-term clinical outcomes were similar for prehospital- and hospital- treated patients. Thirty-day survival was improved with very early thrombolytic therapy, but very early treatment did not decrease either subsequent survival or the number of cardiac events after hospital dis- charge.
1. Kennedy JW, Ritchie JL, Davis KB, Fritz JK. Western Washington random- ized trial of intracoronary streptokinase in acute myocardial infarction. N Engl JMed 1983;309:1477-1482. 2. Thrombolysis in Myocardial Infarction (TIMI) the TIMI Study Group. Spe- cial report: the Thrombolysis in Myocardial Infarction (TIMI) trial. N Engl J Med 1985;312:932-936, 3. Gmppo Italian0 per lo Studio della Streptcchinase nell’ Infarto Miocardico (GISSI). Effectiveness of intravenous tbrombolytic treatment in acute myocar- dial infarction. Lancet 1986;1:397-402. 4. Gmppo Italian0 per lo Studio della Streptochinase nell’ Infarto Miocardico (GISSI). Long-term effects of intravenous thrombolysis in acute myocardial infarction: final report of the GISSI study. Lancet 1987;2:871-874. 5. AIMS Trial Study Group. Effect of intravenous APSAC on mortality after acute myocardial infarction: preliminary report of a placebo-controlled clinical trial. Lancet 1988;1:545-549. 6. Wilcox RG, van-der-Lippe G, Olsson CG, Jensen G, Skene AM, Hampton JR. Trial of tissue plasminogen activator for mortality reduction in acute myo- cardial infarction: Anglo-Scandinavian Study of Early Thrombolysis (ASSET). Lancet 1988;2:525-530. 7. Thmmbolysis in Myocardial Infarction (TIMI)-2. Comparison of invasive and conservative strategies after treatment with intravenous tissue plasminogen activator in acute myocardial infarction. N Engl J Med 1989;320:618-627.
CORONARY ARTERY DISEASE/LONG-TERM OUTCOME IN MIT1 501
![Page 6: Influence of early prehospital thrombolysis on mortality and event-free survival (The Myocardial Infarction Triage and Intervention [MITI] Randomized Trial)](https://reader042.dokumen.tips/reader042/viewer/2022020605/5750749e1a28abdd2e956657/html5/page/6.jpg)
8. ISIS-2 (Second International Study of Infarct Survival Collaborative Group). Randomized trial of intravenous streptokinase, oral aspirin, both or neither among 17,187 cases of suspected acute myocardial infarction: ISIS-2. Lancet 1988:2:349-360. 9. Sbarkev SW. Brunette DD. Ruiz E. Hession WT. Wvsham DG. Goldberg IF, Hodges M. An analysis of the time delays preceding thrombolysis for acute myocardial infarction. JAMA 1989;262:3171-3174. lb. Kereiakes DJ, Weaver WD, Anderson JL, Feldman T, Gibler B, Aufderheide T, Williams DO, Martin LH, Anderson LC, Martin JS, McKendall G, Sherrid M, Greenberg H, Teichman SL. Time delays in the diagnosis of acute myocar- dial infarction: a tale of eight cities. Report from the pre-hospital study group and the Cincinnati Heart Project. Am Heart .I 1990;120:773-780. 11. Weaver WD. Eisenbere MS. Martin JS. Litwin PE. Shaeffer SM. Ho MT. Kudenchuk PJ, Hallstrom AP, Cerquiera MD, Copass MK, Kennedy JW, Cobb LA, Ritchie MD. Myocardial Infarction, Triage and Intervention Project-Phase 1: patient characteristics and feasibility of prehospital initiation of thrombolytic therapy. JAm Coil Car&l 1990;15:925-931. 12. European Myocardial Infarction Project (EMIP) Group. Prehospital throm- bolytic therapy in patients with suspected acute myocardial infarction. N Engl J Med 1993;329:383-390.
13. Weaver WD. Ceraueira M. Hallstrom AP. Litwin PE. Martin JS. Kudenchuk PJ, Eisenberg M. The Myoc’ardial Infarction Triage and Intervention’Trial. Prehospital-initiated vs. hospital-initiated thrombolytic therapy. JAMA 1993; 270:1211-1216. 14. Mathev D. Schafer J. Sheehan F. Krebber HJ. Justen M. Rodewald G. Dodge HT:Bleifeld W. Improved survival up to four years after early coronary thrombolysis. Am J Cardiol 1988;61:524-529. 15. Simoons ML, Vos J, Tijssen JG, Vermeer F, Verheugt FW, Krauss XH, Cats VM. Lone-term benefit of earlv thrombolvtic therauv in uatients with acute myocardial infarction: 5 year follow-up of a-trial conducted by the Interum- versity Cardiology Institute of the Netherlands. J Am Coil Cardiol 1989; 14:1609-1615. 16. Cerqueira MD, Maynard C, Ritchie JL, Davis KB, Kennedy JW. Long-term survival in 618 oatients from the Western Washineton Strentokinase in Mvo- cardial Infarction Trials. JAm Co11 Cardiol 1992;%:1452-i459. . 17. Kaplan EL, Meier P. Nonparametric estimation from incomplete observa- tions. .i Am Stat Assoc 1958;53:457-481. 18. Brouwer MA, Bohncke JR, Veen G, Meijer A, van Eenige MJ, Verheugt FWA. Adverse long term effects of reocclusion after coronary thrombolysis. J Am Ccl!- Cardiol 1995;26:1440-1444.
502 THE AMERICAN JOURNAL OF CARDIOLOGY” VOL. 78 SEPTEMBER 1, 1996