Embed Size (px)
Citation preview

PREVENTIVE MEDICINE 18, 847-855 (1989)
Influence of a Preventive Care Educational Intervention on Physician Knowledge, Attitudes, Beliefs, and Practice’
EUGENE C. RICH, M.D., *,' LEONARD SCHLOSSBERG, M.D.,* MICHAEL LUXENBERG, PH.D.,* ANDJANE KoRN,M.D.~
*Department of Medicine, St, Paul-Ramsey Medical Center, St. Paul, Minnesota, and fDepartment of Medicine, Minneapolis Veterans Administration Medical Center,
Minneapolis, Minnesota
We evaluated the effect of a three-part intervention on knowledge, attitudes, beliefs, and practices relevant to preventive care. A group of 13 second-year internal medicine residents (Group I) were exposed to a lecture, chart-based reminder, and biweekly feedback during a 3-month ambulatory care rotation. The remaining two groups of residents (Group II, n = 12; Group III, n = 11) were not exposed to the intervention. We performed a chart review to assess preventive care practice at a clinical site separate from the intervention and surveyed residents to assess preventive care knowledge, self-reported practice, professional attitudes, and health beliefs. Chart reviews revealed the intervention to be associated with improved performance of preventive care (0.52 vs 0.35 and 0.42, P = 0.01). In addition, the inter- vention was associated with improved scores for preventive care knowledge (90 vs 74 and 77, P = 0.001) and self-reported practice (85 vs 65 and 72, P = 0.007). Although attitudes toward prevention and health locus of control were not measurably influenced by the in- tervention, stepwise multiple linear regression analysis demonstrated these factors to be independently related to preventive practice. Our data support the notion that physician preventive practice is subject to a variety of influences involving not only knowledge, and practice environment, but also training, professional attitudes, and health beliefs. o isss Academic Press, Inc.
INTRODUCTION
A variety of preventive care maneuvers have been endorsed as valuable and applicable in the primary care setting (1, 2). Unfortunately, physician compliance with such screening recommendations has been highly variable and generally dismal (3-6). The reasons for poor physician practice in preventive care are com- plex, reflecting the multiple influences on the clinical decisions of individual prac- titioners. Factors previously suggested to influence preventive practice include specialty training (7, 8), knowledge (9), personal health beliefs (lo), attitudes regarding the role of physicians in prevention (1 l), personal experience (3), finan- cial incentives (12), and, of course, patient expectations (12). The extent of these various influences on actual practice remains unclear, however (13), as does their role in efforts to improve physician performance.
In order to improve preventive care by residents in our teaching clinics, we incorporated a three-part intervention into our ambulatory care rotation (14). In
i Supported in part by the Cost Effective Care Program, St. Paul-Ramsey Medical Center. ’ To whom reprint requests should be addressed at University of Kentucky Medical Plaza, Rose
Street, Lexington, KY 40536.
847 0091-7435/89 $3.00 Copyright 0 1989 by Academic Press, Inc. AU rights of reproduction in any form reserved.
848 RICH ET AL.
this study we evaluate the effect of this intervention on physicians’ knowledge, attitudes, and beliefs relevant to prevention, and we investigate the relationship of these factors to physician performance in a clinical site remote from the original intervention.
METHODS
Subjects
The subjects of our study were 36 second-year internal medicine residents who agreed to participate in our survey study. These represent 92% of the postgrad- uate years (PGY)-2’s enrolled in the University of Minnesota Internal Medicine Program for 1984. Beginning in July 1984 these residents practiced ambulatory care for one half-day each week in the General Medicine Clinic of the Minneapolis Veterans Administration Hospital (MVAH). In addition, 25 of these 36 PGY-2’s elected a 3-month ambulatory care block rotation at St. Paul-Ramsey Medical Center (SPRMC). The 13 PGY-2’s who completed the ambulatory block rotation by December 1984 constituted the intervention group of our study (Group I). The 12 PGY-2’s who also elected the rotation but were scheduled to begin it in 1985 constituted our control group (Group II) for evaluating the effect of our interven- tion.
The remaining 11 PGY-2’s either elected or were assigned to other inpatient or outpatient clinical activities for this 3-month period and did not participate in the ambulatory care rotation at SPRMC. Since performance and survey data were also collected on these 11 PGY-2’s, their results have been included for complete- ness in our presentation of comparisons; the 11 PGY-2’s not participating in the ambulatory care rotation have been designated as Group III.
Intervention
The preventive care intervention consisted of three components incorporated into the ambulatory blcok rotation at SPRMC. The first component was a 1-hr lecture on the periodic health examination which provided the rationale for our preventive care recommendations. The second component was a biweekly chart review conference, where SPRMC faculty gave residents feedback regarding their outpatient care (including provision of preventive care services) based on review of charts randomly selected from among the residents’ clinic patients seen in the previous week. The third component was a health maintenance checklist available as part of the medical record for all patients seen in the clinic at SPRMC. This checklist had been previously adapted by the clinic faculty from various published guidelines. All components of the intervention were established and in place before July 1984.
EVALUATION OF PREVENTIVE PRACTICE
The practice of the PGY-2’s was evaluated at the MVAH Clinic, a separate clinical site with no preventive care interventions at the time of study. Two of the authors reviewed the medical records of 393 patients seen by the PGY-2’s at the MVAH Clinic during the month of December 1984. Preventive practice was, therefore, evaluated for MVAH patients seen from 2 to 5 months after the Group
INFLUENCE OF PREVENTIVE CARE EDUCATION 849
I residents first experienced the intervention at SPRMC. The record reviewers were unaware of the group assignment of the PGY-2’s. Each patient record was reviewed for performance of rectal examination, stool hemoccult tests, breast examination, mammography, and influenza vaccination. These maneuvers were scored as performed if ordered within the preceding 12 months (inclusive of the index visit). In addition, pneumococcal vaccination was evaluated using nurse or physician documentation of any prior immunization. Although efforts in patient education are also important aspects of preventive care, we could not reliably assess these from the outpatient record. Thus, our evaluation of preventive prac- tice measures only two of the three types of maneuvers (screening, patient edu- cation, immunization) available to physicians.
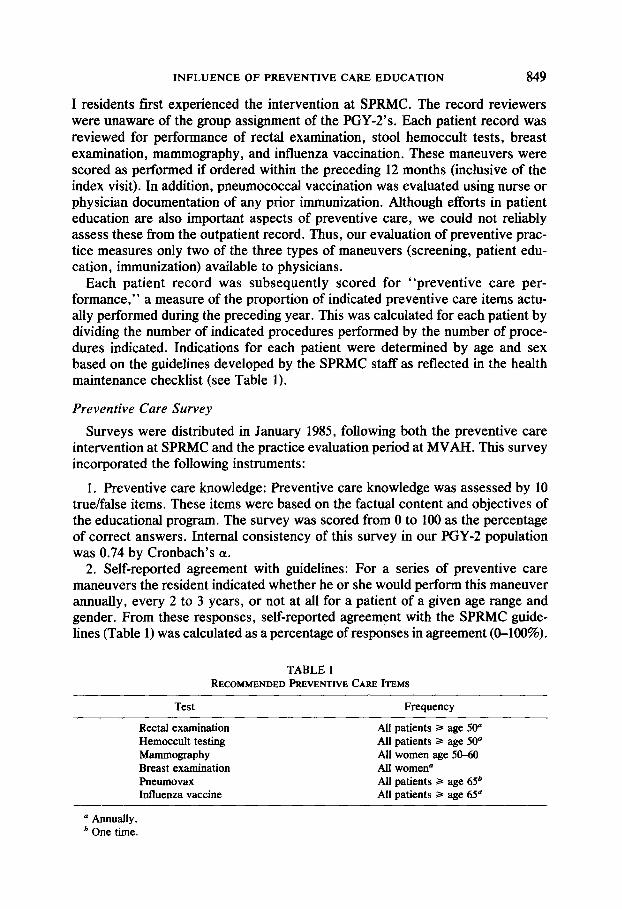
Each patient record was subsequently scored for “preventive care per- formance,” a measure of the proportion of indicated preventive care items actu- ally performed during the preceding year. This was calculated for each patient by dividing the number of indicated procedures performed by the number of proce- dures indicated. Indications for each patient were determined by age and sex based on the guidelines developed by the SPRMC staff as reflected in the health maintenance checklist (see Table 1).
Preventive Care Survey
Surveys were distributed in January 1985, following both the preventive care intervention at SPRMC and the practice evaluation period at MVAH. This survey incorporated the following instruments:
1. Preventive care knowledge: Preventive care knowledge was assessed by 10 true/false items. These items were based on the factual content and objectives of the educational program. The survey was scored from 0 to 100 as the percentage of correct answers. Internal consistency of this survey in our PGY-2 population was 0.74 by Cronbach’s (Y.
2. Self-reported agreement with guidelines: For a series of preventive care maneuvers the resident indicated whether he or she would perform this maneuver annually, every 2 to 3 years, or not at alI for a patient of a given age range and gender. From these responses, self-reported agreement with the SPRMC guide- lines (Table 1) was calculated as a percentage of responses in agreement (O-100%).
TABLE 1 RECOMMENDED PREVENTIVE CARE ITEMS
Test Frequency
Rectal examination Hemoccult testing Mammography Breast examination Pneumovax Influenza vaccine
All patients 2 age 50” All patients 3 age 50” All women age 50-60 All women” All patients > age 65’ All patients z age 65”
D Annually. b One time.
850 RICH ET AL.
3. Professional attitudes toward preventive care: To measure professional at- titudes regarding prevention we administered the Attitudes Towards Social Issues in Medicine Survey (15). A subscale of this survey measures the perceived im- portance of preventive medicine in physician practice and is scored from 9 (low importance) to 45 (high importance). Previous use of this scale with medical students has revealed an internal consistency by Cronbach’s (Y of 0.684 (15).
4. Personal health beliefs: To measure our residents personal health beliefs we administered the Health Locus of Control Survey. This survey has three sub- scales (“internal,” “chance,” and “others”) assessing the individual’s perception of personal control over health (16). For our study we used only the internal subscale, which has shown the best reliability in previous studies (Cronbach’s a 0.72) (17). This subscale is scored from 6 (low internal locus of control) to 36 (high internal locus of control).
Statistical Analysis
Statistical analyses were performed using the Statistical Package for the Social Sciences. Preventive care performance scores of residents in the three groups (Group I, Group II, and Group III) were compared by analysis of variance. Sim- ilarly, responses on the preventive care survey were compared by analysis of variance.
Stepwise multiple linear regression was performed to analyze for independent relationships between resident responses on the preventive care survey and res- ident’s preventive care performance. This analysis controlled for resident’s ex- perience with the educational intervention.
RESULTS
Analysis of variance revealed the intervention to be associated with signifi- cantly greater preventive care performance (overall P = 0.01 by ANOVA). An average of 49% of indicated procedures were performed on patients cared for by the intervention group (Group I), compared to 34% in Group II and 41% in Group III. On paired comparisons, Group I was different from Groups II and III (P < 0.05), while Groups II and III were not different (P > 0.05).
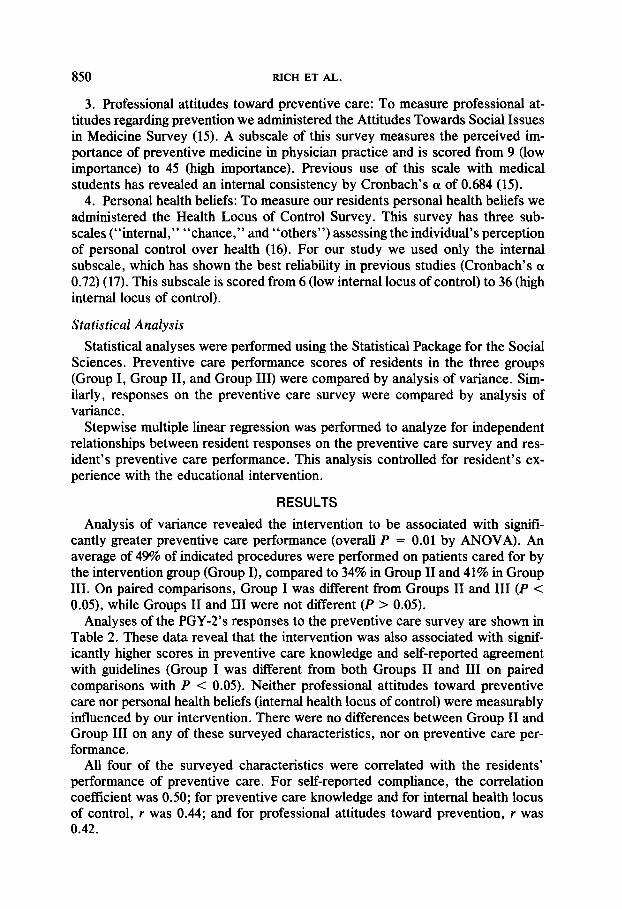
Analyses of the PGY-2’s responses to the preventive care survey are shown in Table 2. These data reveal that the intervention was also associated with signif- icantly higher scores in preventive care knowledge and self-reported agreement with guidelines (Group I was different from both Groups II and III on paired comparisons with P < 0.05). Neither professional attitudes toward preventive care nor personal health beliefs (internal health locus of control) were measurably intluenced by our intervention. There were no differences between Group II and Group III on any of these surveyed characteristics, nor on preventive care per- formance.
All four of the surveyed characteristics were correlated with the residents’ performance of preventive care. For self-reported compliance, the correlation coefficient was 0.50; for preventive care knowledge and for internal health locus of control, r was 0.44; and for professional attitudes toward prevention, I was 0.42.
INFLUENCE OF PREVENTIVE CARE EDUCATION 851
TABLE 2 INTERVENTIONANDPREVENTIVECARESURVEY
Group I Group II Group III F P
Preventive care knowledge” 90 74 77 8.28 0.001 Self-reported agreeme& 85 65 72 9.24 0.007 Professional attitudesc 35 33 34 1.20 0.31 Health beliefsd 24 23 22 0.56 0.58
a Preventive care knowledge scored from 0 (no correct responses) to 108 (all correct responses). b Self-reported practice scored from 0 (no responses in agreement with guidelines) to 100 (all re-
sponses in agreement with guidelines). c Professional attitudes toward prevention scored from 5 (minimal importance indicated for preven-
tive care) to 45 (maximal importance indicated for preventive care). d Internal health locus of control scored from 6 (minimal internal health locus of control) to 36
(maximal internal health locus of control).
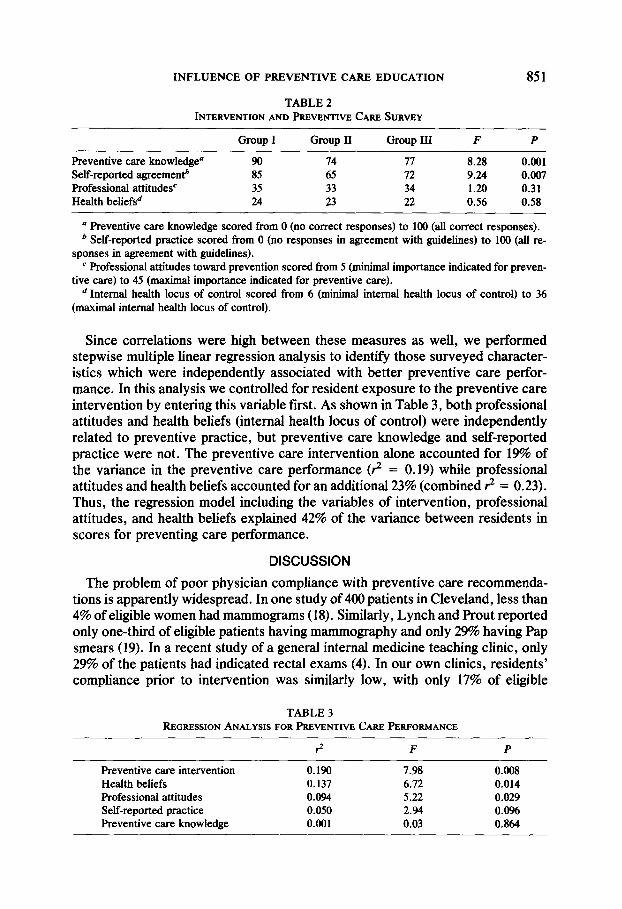
Since correlations were high between these measures as well, we performed stepwise multiple linear regression analysis to identify those surveyed character- istics which were independently associated with better preventive care perfor- mance. In this analysis we controlled for resident exposure to the preventive care intervention by entering this variable first. As shown in Table 3, both professional attitudes and health beliefs (internal health locus of control) were independently related to preventive practice, but preventive care knowledge and self-reported practice were not. The preventive care intervention alone accounted for 19% of the variance in the preventive care performance (3 = 0.19) while professional attitudes and health beliefs accounted for an additional 23% (combined ? = 0.23). Thus, the regression model including the variables of intervention, professional attitudes, and health beliefs explained 42% of the variance between residents in scores for preventing care performance.
DISCUSSION
The problem of poor physician compliance with preventive care recommenda- tions is apparently widespread. In one study of 400 patients in Cleveland, less than 4% of eligible women had mammograms (18). Similarly, Lynch and Prout reported only one-third of eligible patients having mammography and only 2% having Pap smears (19). In a recent study of a general internal medicine teaching clinic, only 29% of the patients had indicated rectal exams (4). In our own clinics, residents’ compliance prior to intervention was similarly low, with only 17% of eligible
TABLE 3 REGRESSION ANALYSIS FORPREVENTIVE CAREPERFORMANCE
Preventive care intervention 0.190 7.98 0.008 Health beliefs 0.137 6.72 0.014 Professional attitudes 0.094 5.22 0.029 Self-reported practice 0.050 2.94 0.096 Preventive care knowledge 0.001 0.03 0.864
852 RICH ET AL.
patients receiving mammography and 18% receiving fecal occult blood tests (14). This poor performance persists despite consensus among authorities of the ben- efits of these maneuvers (1, 2) and, at least for mammography, despite strong scientific evidence favoring the practice (20).
Various interventions have been tried, each designed to address one of the various possible reasons for this dismal physician performance. One important problem may be physician’s failure to think of the maneuver during the visit. In a study of simulated periodic health examination visits, few residents remembered to recommend pneumococcal vaccination despite their belief that such vaccina- tion would be beneficial (21). Physicians in another study indicated “forgetting” to be an important cause of their failure to perform fecal occult blood testing (4). One solution to this problem is reminding the physician in a timely way. Passive, chart-based checklists (22), nurse initiated reminders (23), and computer initiated reminders (24) have all proven successful in improving the rates of physician performance in the indicated preventive services. Accordingly, our intervention included a reminder scheme (the Health Maintenance Checklist), which could have accounted for our previously reported improvements at SPRMC (14). These reminders could not, however, directly influence performance at the MVAH Clinic, since no checklists or other reminders were available to our residents when practicing there. Thus, our intervention improved physician performance at the MVAH through some mechanism other than simply prompting the physician at the time of the clinic visit.
Another problem is physician ignorance of their own poor performance. Pre- vious studies have demonstrated that physicians considerably overestimate their performance of preventive services (3, 6). Feedback interventions attempt to address this type of problem and have met with success in a variety of clinical settings (5, 25, 26). Our intervention incorporated chart review conferences, a feedback strategy which has been successfully applied to change laboratory uti- lization (25). As with our chart reminders, however, this feedback did not involve the patients or personnel of the MVAH Clinic. Thus although this intervention could have directly influenced patient care at SPRMC, it could have had no direct benefit for patients at MVAH.
Certainly lack of knowledge can be an important reason for poor preventive practice. A physician is unlikely to provide a service if he or she has never learned of its benefits. Previous research has found lack of knowledge to be related to self-reported cancer screening (9) and to influenza vaccination practice (27). Other studies, however, have found little relationship between knowledge and preven- tive practice (28). Furthermore, knowledge-directed interventions have given gen- erally unimpressive results, with neither written materials (29) nor educational seminars (30) influencing practice. Our intervention included a didactic compo- nent in addition to the chart reminders and feedback. Indeed, the preventive care survey which followed our intervention indicated improved knowledge on two scales, preventive care knowledge and self-reported agreement with guidelines. In our regression analysis, however, responses on these scales were not associated with resident performance independent of resident exposure to the intervention.
INFLUENCE OF PREVENTIVE CARE EDUCATION 853
Thus, the relationship between physician knowledge and preventive care practice remains unclear.
Professional education may impart much more than knowledge. Various atti- tudes and beliefs are acquired by trainees, some held in common by all physicians and some differing among physician groups (31). We evaluated the intluence of our intervention on two such factors, professional attitudes toward prevention and personal health beliefs (internal health locus of control). Interestingly, al- though our educational program had no measurable effect on responses to either of these surveys, the responses were strongly and independently related to prac- tice.
The association between personal health beliefs and preventive practice is par- ticularly interesting. A number of studies have demonstrated that patient health locus of control may be related to individual preventive behaviors (32-34). Re- cently, Wells and colleagues have suggested that a physician’s personal health beliefs and personal practices may relate to performance of preventive care (8, 10). Physician health beliefs may influence preventive practice at several levels. First, a physician who has a strong belief in personal control over health may more readily accept the evidence of benefit for a screening test. Second, a phy- sician with strong personal health beliefs might more readily remember to perform the screening test. Third, the physician with strong personal health beliefs may be more successful in persuading patients to undergo screening. Our data suggest that at least the first explanation is incomplete, since our physicians’ health locus of control was associated with performance independent of agreement with rec- ommended guidelines.
Several limitations to our study should be noted when interpreting these results. First, the subjects of our intervention (Group I) and the comparison group of residents who had elected but not yet received the intervention (Group II) were determined by a rotation scheduling process which was not necessarily random. Our available data reveal no relevant selection bias in the scheduling of residents to the ambulatory care rotation, however, with performance, knowledge, atti- tudes, and beliefs of the Group II residents (scheduled for the intervention) being similar to the characteristics of the Group III residents (not scheduled for the intervention).
Second, the ambulatory care rotation itself might constitute part of the inter- vention, influencing both knowledge and practice. A previous preventive care study found that our three-part preventive care intervention significantly affected practice during the ambulatory care rotation (14). Knowledge was not assessed in that study, however, so that we cannot exclude the possibility that knowledge and agreement with guidelines were influenced by the ambulatory care rotation, in- dependent of our specific preventive care intervention.
Third, our survey instruments have limited reliability, and no previous deter- mination of validity. Furthermore, the number of subjects in our regression anal- ysis was limited relative to the number of independent variables tested. Thus our findings with these instruments must be considered preliminary.
Finally, it should be noted that each patient was subject to the care of at least
854 RICH ET AL.
two residents during the course of 1984 (the PGY-2’s we observed provided care only from July through December). These PGY-2’s were randomly assigned to panels of clinic patients; thus the care (or non-care) provided by previous resi- dents constitutes no source of bias, although it does result in potential variation in preventive care practice not attributable to the knowledge, attitudes, beliefs, or training of the physicians observed in our study. Interestingly, despite these lim- itations, over 40% of the variation in preventive practice was explained by our regression model.
CONCLUSION
In summary, we demonstrate that a preventive care intervention consisting of education, chart reminders, and feedback incorporated into an ambulatory care rotation was associated with differences in physicians’ preventive care knowl- edge, self-reported practice, and actual practice assessed at a separate primary- care clinic. While the intervention had no measurable effect on professional atti- tudes or health beliefs, these characteristics were strong additional correlates of improved preventive care practice. Our data confirm that the influences on phy- sician performance of preventive care are complex, involving not only personal knowledge and practice site, but educational experiences, professional attitudes, and personal beliefs. Further understanding of these influences may prove useful in devising efficient strategies to improve preventive care by physicians.
REFERENCES 1. Canadian Task Force on the Periodic Health Examination. The periodic health examination. Can
Med Assoc J 1979; 1193-1254. 2. American Cancer Society. ACS report on the cancer related check-up. Cancer 1980; 30~194-240. 3. Woo B, Woo B, Cook FC, Weisberg M, Goldman L. Screening procedures in the asymptomatic
adult; comparison of physicians recommendations, patients desires, published guidelines and actual practice. JAMA 1985; 254~1480-1484.
4. McPhee SJ, Richard RJ, Solkowitz SN. Performance of cancer screening in a university general medicine clinic. J Gen Znt Med 1986; 1:275-281.
5. Tiemey WM, Hui SI, McDonald CJ. Delayed feedback of physician performance vs. immediate reminders to perform preventive care: Effects on physician compliance. Med Care 1986; 243659-666.
6. Romm FJ, Fletcher SW, Hulka BS. The periodic health examination: Comparison of recommen- dations and internists’ performance. South Med J 1981; 74265-271.
7. Withers JN, Wienke JW. Hemoccult screening for colon cancer by Hawaii’s physicians. Hawaii
Med J 1981; 40~75-77. 8. Wells KB, Lewis CE, Leake B, Ware JE. Do physicians practice what they preach. JAMA 1984;
252~2846-2848. 9. Battista RN, Williams JI, MacFarlane LA. Determinants of primary medical practice in adult
cancer prevention. Med Care 1986; 24216224. 10. Lewis LE, Wells KB, Ware J. A model for predicting the counselling practices of physicians. J
Gen Znt Med 1986; 1:14-19. 11. Kottke TE, Blackbum H, Brekke ML, Solberg LI. The systematic practice of preventive cardi-
ology. Am J Cardiol 1987; 59690-694. 12. Carter WB, Belcher DW, Inui TS. Implementing preventive care in practice. II. Problems for
managers, clinicians and patients. Med Cure Rev 1981; 38195-216. 13. Battista RN. Adult cancer prevention in primary care. Am J Public Health 1983; 73:103&1039.
INFLUENCE OF PREVENTIVE CARE EDUCATION 855
14. Kom JE, S&lo&erg LA, Rich EC. Improved preventive care following an intervention during an ambulatory care rotation. J Gen Znt &fed 1988; 3:1X-160.
15. Parlow J, Rothman AJ. ATSIM. A scale to measure attitudes toward psychological factors in health care. J Med Educ 1974; 49385-387.
16. Wallston KA, Wallston BS, Devellis R. Development of the multidimensional health locus of control (MHLC) scales. Health Educ Monogr 1978: 6:160-170.
17. Meyer R, Donham GW, Ludenia K. The psychometric properties of the Helath Locus of Control scale with the medical and surgical patients. J Clin Psychol 1982; 38:783-787.
18. Cargill VA, McCormick M, Fenton B. Housestaff Knowledge and Attitudes as Predictors of Screening Behavior. Presentation, Midwest Society for Research and Education in Primary Care Internal Medicine, Chicago, IL, November 1984.
19. Lynch GR, Prout MN. Screening for cancer by residents in an internal medicine program. J Med
Educ 1986; 61:387-393. 20. Shapiro S. Evidence on screening for breast cancer from a randomized trial. Cancer 1977;
392772-2782. 21. Young MJ, Yates JF, Curley SP. Physicians active versus default health maintenance decisions.
Med De& Making 1986; 6264. 22. Frame PS. Periodic health screening in a rural private practice. J Fam Pratt 1979; 957-64. 23. Davidson RA, Fletcher SW, Retchin S, Duh S. A nurse initiated reminder system for the periodic
health examination. Arch Znt Med 1984; 144:2167-2170. 24. McDonald CJ, Hui SL, Smith DM, Tiemey WM, Cohen SJ, Weinberger M, McCabe GP. Re-
minders to physicians from an introspective computer medical record. Ann Znt Med 1984; 100:13&138.
25. Martin AR, Wolf MA, Thibodeau LA, Dzau Y, Braunwald E. A trial of two strategies to modify test ordering behavior of medical residents. N Engl J Med 1980; 303:1330-1336.
26. Eisenberg JM. Physician utilization. The state of research about physicians’ practice patterns. Med Care 1985; 23:401-483.
27. O’Mally MS, Retchin SM, Jeffries B, et al. Factors inthrencing physician performance of preven- tive procedures (abstract). Clin Res 1985; 33:729.
28. Greenland P, Mushlin AL, Griner PF. Discrepancies between knowledge and use of diagnostic studies in asymptomatic patients. J Med Educ 1979; 54863-869.
29. Cohen DI, Littenburg B, Wetzel C, Neuhauser DB. Improving physician compliance with pre- ventive medicine guidelines. Med Care 1982; 20:1040-1045.
30. Cohen SJ, Weinberger M, Hui S, Tiemey WM, McDonald CJ. The impact of reading on physi- cians’ non-adherence to recommended standards of medical care. Sot Sci Med 1985; 21909 914.
31. Eisenberg JM. Sociological inthtences on decision-making by clinicians. Ann Znt Med 1979; 90:957-964.
32. Balch P, Ross DW. Predicting success in weight reduction as a function of locus of control: A unidimensional multidimensional approach. .Z Consult Clin Psycho1 1975; 43:119.
33. James W, Woodruff A, Warren W. Effect of internal and external control upon changes in smoking behavior. J Consult Clin Psycho1 1965; 29184-186.
34. Seeman M, Seeman J. Health behavior and personal autonomy: A longitudinal study of the sense of control in illness. J Health Sot Behav 1983: X144-160.





























