Embed Size (px)
Citation preview

Journal of Plastic, Reconstructive & Aesthetic Surgery (2009) 62, 1347e1354
Inferior gluteal artery perforator flap: a viablealternative for ischial pressure sores
Young Seok Kim, Dae Hyun Lew, Tai Suk Roh, Won Min Yoo, Won Jai Lee*,Kwan Chul Tark
Institute for Human Tissue Restoration, Department of Plastic & Reconstructive Surgery,Yonsei University, College of Medicine, Seoul, Republic of Korea
Received 19 July 2007; accepted 25 March 2008
KEYWORDSInferior gluteal arteryperforator;Perforator flap;Pressure sore;Ischium
* Corresponding author. Address: DeMedicine, 134 Shinchon-Dong, Seodae
E-mail address: [email protected] (
1748-6815/$-seefrontmatterª2009Britdoi:10.1016/j.bjps.2008.03.026
Summary The ischial area is by far the most common site for pressure sores in wheelchair-bound paraplegic patients, because most of the pressure of the body is exerted on this area inthe seated position. Even after a series of successful pressure sore treatments, the site is veryprone to relapse from the simplest everyday tasks. Therefore, it is crucial to preserve the mainpedicle during primary surgery. Several surgical procedures, such as myocutaneous flap andperforator flap, have been introduced for the treatment of pressure sores. During a 4-year timeperiod at our institute, we found favourable clinical results using the inferior gluteal arteryperforator (IGAP) procedure for ischial sore treatment.
A total of 23 patients (20 males and three females) received IGAP flap surgery in our hospitalfrom January 2003 to January 2007. Surgery was performed on the same site again in 10 (43%)patients who had originally relapsed after undergoing the conventional method of pressuresore surgery. The average age of patients was 47.4 years (range 26e71 years). Most of thepatients were paraplegic (16 cases, 70%) and others were either quadriplegic (four cases,17%) or ambulatory (three cases, 13%). Based on hospital records and clinical photographs,we attempted to assess the feasibility and practicability of the IGAP flap procedure throughcomparative analysis of several parameters including the size of the defective area, treatmentmodalities, relapses, complications, and postoperative treatments.
The average follow-up duration for 23 subjects was 25.4 months (range 5e42 months). Allflaps survived without major complications. Partial flap necrosis developed in one case but sec-ondary healing was achieved and the final outcome was not impaired. Most of the cases healedwell during the follow-up period. Postoperative complications such as wound dehiscence andfistula developed in some subjects, but all healed well with a secondary treatment. A total offive cases relapsed after surgery due to tissue deficit and these were treated with bursectomyand muscle transposition flap to fill the dead space.
partment of Plastic & Reconstructive Surgery, Yonsei Medical Center, Yonsei University College ofmun-Gu, Seoul, Republic of Korea. Tel.: þ82 2 2228 2219; fax: þ82 2 393 6947.W.J. Lee).
ish Association of Plastic, Reconstructive and Aesthetic Surgeons. Published by Elsevier Ltd. All rights reserved.

1348 Y.S. Kim et al.
We propose that the IGAP flap should be considered a viable alternative to other methods ofischial pressure sore surgery owing to its many advantages, which include the ability to pre-serve peripheral muscle tissue, the variability of flap designs, relatively good durability, andthe low donor site morbidity rate.ª 2009 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published byElsevier Ltd. All rights reserved.
A pressure sore is a chronic ulcer that appears in pressureareas, often over a bony prominence, and is due to a circu-latory defect from enhanced tissue pressure in high-contactareas. Pressure sores can occur at different locations ac-cording to the patient’s position and are prevalent amongparaplegic or quadriplegic patients and chronic and long-term hospitalised patients. The skin overlying the ischiumis the most common location for pressure sores, especiallyin paraplegic patients who are confined to wheelchairs.Even when surgical debridement and vascularised softtissue coverage is performed successfully, recurrence oftendevelops due to the continuous pressure on the ischial areaduring the patients’ daily activities.
For this reason, patients with ischial pressure sores mayrequire several flap surgeries during their lifetime, howeverthe number of surgeries is limited because there are notmany vascular pedicles in the gluteal region for the flapsurgery. To treat these patients, it is important to adopta surgical strategy in which the vascular pedicles andmuscles for future flaps are not injured during the initialflap procedure.1 There are various alternatives for theclosure of ischial pressure sores such as the gluteus maxi-mus musculocutaneous flap, inferior gluteal thigh flap,hamstring muscle flap, biceps femoris muscle flap, tensorfascia lata flap, and gracilis muscle flap.2
Since the introduction of the perforator flap by Krolland Rosenfield, Koshima further advanced the procedurefor the repair of the sacral pressure sore,3 and these flapshave been gaining in popularity for reconstructive surgeryover the past 15 years. Gluteal perforator flaps have beenused as pedicle or free flaps for coverage at various sites.In perforator flaps, muscles can be preserved by dissec-tion of pedicles parallel to the direction of the musclefibres, and island flaps with separated pedicles are usedfor the treatment of pressure sores on the sacral ortrochanteric area. Based on the superior gluteal arteryperforator flap, which is generally used for sacral sores,Higgins introduced the inferior gluteal artery perforator(IGAP) flap, and reported a single case of IGAP treatmentfor an ischial sore.4
Over a 4-year period, we achieved satisfying resultsusing the IGAP flap for treatment of ischial sores and in thispaper report a retrospective study on the effectiveness ofthe IGAP flap.
Materials and methods
We evaluated 23 patients (20 males, three females) whounderwent an IGAP flap operation for the treatment ofpressure sores in the ischial area at Yonsei University,Severance Hospital from January 2003 to January 2007.There were 10 patients (43%) who presented with
a recurrence of a pressure sore in the same area afterconventional surgery. Of the patients who underwent IGAPflap surgery, 10 were recurrence cases from previousconventional surgery, such as inferior gluteal maximusmyocutaneous flaps or bursectomy and primary closures.Four of these patients underwent previous operations in ourinstitute and six in other hospitals. The average age of thepatients was 47.4 years (range 26e71 years). Sixteenpatients (70%) were paraplegic, four (17%) were quadriple-gic, and three (13%) were ambulatory.
The causes of paralysis were spinal cord injury fromtrauma in 18 patients, vascular malformation of the spinalcord in one patient, spinal tuberculosis in one patient,complication of spinal surgery in one patient, complicationfrom aortic dissection in one patient, and long-termresidence in an intensive care unit in one patient. Allpatients maintained a prone position for 3 weeks after theoperation in an air-fluid bed to prevent pressure sores inother areas. After 3 weeks, the patients were trained toresume a seated position.
The area of the defect, treatment method, incidence ofrecurrence, complication, and proper management wereanalysed according to the patients’ medical records andclinical photographs.
Operative techniques of IGAP flap
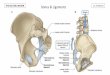
Preoperatively, all perforators of the inferior gluteal arterywere identified with Doppler. In the prone position,anatomical landmarks including the posterior iliac spine,greater trochanter, and ischial tuberosity were identifiedand the predicted course of the inferior gluteal artery wasmarked. Usually the inferior gluteal artery runs alonga linear line between the superior iliac spine, and ischialtuberosity and perforators are distributed along the line(Figure 1). The skin paddle is designed elliptically to in-clude the perforators and is positioned parallel to thetension line for primary closure of the donor site.
First, a wide excision was performed, which includeda bursectomy of the pressure sore area. Most cases neededostectomy of the ischial tuberosity. With regard to thedesign of the defect area, the flap was elevated above thefascia level and when several perforators were noticed,apparent size and Doppler was used to select one or twoadequate perforators for meticulous dissection above thegluteus maximus muscle. Although it is better to include asmany perforators as possible, the transposition of the flap isrestricted. Therefore, to increase the mobility of the flap,a single perforator is selected and the dissection isperformed to the perforator origin. The elevated flap isadvanced or transposed towards the defect area andsutured with a half-buried suture. The drain was maintained

Figure 1 Inferior gluteal artery (IGA) and its perforators. TheIGA was located along a line connecting the posterior superioriliac spine and the ischial tuberosity at the inferior border ofthe piriformis muscle. The perforators were located in the me-dial and lateral portion of the IGA (thick line: course of IGA;spots: perforators of IGA).
Inferior gluteal perforator flap for ischial sores 1349
for at least 7 days and the prone position was maintainedwithout pressure on the flap.
Results
Twenty-three patients were followed up for an average of25.4 months (range 5e42 months). The size of the flapvaried from 4� 2 cm to 10� 8.4 cm, and most of the flapssurvived without major complication. Primary closure ofthe donor site was achieved in all cases.
Six cases of partial wound dehiscence caused by in-fection or excess tension during the position change werenoted within 1 month postoperatively. Debridement andprimary repair were performed in four cases, and two caseswere treated conservatively. There were no cases of totalflap necrosis, but there was one case of partial congestionand desquamation that progressed to partial flap necrosisat the lower margin of the flap, but which healedcompletely with conservative treatment.
The sore recurred in five patients, and all of these casesoccurred after 6 months postoperatively. The most fre-quent signs of recurrence were fistula and small bursa.After complete excision of the bursa, the dead space wasfilled with a muscle transposition flap; the biceps femoris,gracilis, gluteus maximus, or semitendinous muscles wereused in each case. Because the overlying skin and sub-cutaneous tissue is redundant, it is sufficient to use onlymuscle flap to fill the dead space. Of the patients whounderwent IGAP flap surgery, 10 were recurrence casesfrom a previous conventional operation. Of those 10 cases,four had a recurrence of the pressure sore during thefollow-up period, but the others healed completely withoutcomplications (Table 1).
Case 3
A 63-year-old male patient, with paraplegia below theninth thoracic vertebrae due to a fall, developed an ischialpressure sore on the left side, which was reconstructedwith two IGAP flaps. The preoperative skin defect was3� 2 cm with a bursa depth of 10 cm. On the seventh post-operative day, a 1 cm-sized wound dehiscence developedand was treated with conservative management. Satisfac-tory results were noted without any recurrence or compli-cation for 12 months postoperatively (Figure 2).
Case 16
A 43-year-old male patient, with paraplegia after a trau-matic accident, suffered from an ischial pressure sore onthe right side, which was reconstructed with a single IGAPflap. The patient had undergone a reconstructive operationfor a pressure sore in the same area 10 years previously.The preoperative skin defect was 4� 4 cm and the bursadepth was 5 cm. Satisfactory results were noted withoutany recurrence or complication for 39 months postopera-tively (Figure 3).
Case 10
A 35-year-old female patient who suffered paraplegia aftertraumatic removal of an A-V malformation of the spine hadreconstructive surgery with an IGAP flap. The preoperativedefect size was 5� 4 cm and the bursa depth was 12 cm.Recurrence with dead space was noticed 6 months postop-eratively, and was managed by repeated resection of thebursa and reconstruction with a biceps femoris muscletransposition flap (Figure 4).
Discussion
Reconstructions for pressure sores are considered difficultdue to the high recurrence and complication rate. Althoughconservative treatment is the primary choice, reconstruc-tive surgery, such as myocutaneous advancement, is some-times considered in cases where conservative treatmentfails. While various flap operations are feasible, recurrenceafter operation is still a severe problem.5,6
An ischial pressure sore is one of the most difficult areasto treat, because the ischial area is very mobile andvulnerable to pressure in the sitting position. Also, unlikein the sacral area or greater trochanter of the femur, in theischium, the position changes of flexion and extension ofthe lower extremities influence the tension and size of thepressure sore. To minimise the tension after a pressuresore operation, it is important to select a non-mobile flapfrom the pelvis area rather than one from the lowerextremities.2
The most commonly used flaps for ischial sores are theinferior gluteal myocutaneous flap and the inferior glutealthigh fasciocutaneous flap. The inferior gluteal myocuta-neous flap originates from the pelvic area with sufficientsoft tissue and muscle and it has the merits of low donorsite morbidity and preservation of the pedicle of the

Table 1 Summary of cases
No. Sex Age Diagnosis Site Defectsize(cm)
Bursadepth(cm)
Flaptype
Flapsize(cm)
Status Past history Short-termCx
Tx (1) Long-termCx
Tx (2) Follow up(months)
1 M 50 Ischial sore(recurred)
Lt 4� 7 8 FC 5� 9 Quadriplegia Sore operationseveral times
Wounddehiscence
ConservativeTx
Recur after6 months
Gracilismuscletransposition
5
2 M 27 Ischial sore Lt 1� 1 5 FC 6� 5 Paraplegia None None None 103 M 63 Ischial sore Lt 3� 2 10 FC 10� 6 Paraplegia None Wound
dehiscenceConservativeTx
None 12
4 M 49 Ischial sore(recurred)
Lt 8� 1 4 FC 8� 10 Paraplegia Sore operationtwice
Wounddehiscence
Revision None 16
5 F 59 Ischial sore Lt 2� 1 5 FC 4� 3 Bed-ridden DM,HTN, ESRD,CAOD
None None 18
6 M 40 Ischial sore Lt 3� 3 4 FC 4� 2 Paraplegia None None None 217 M 58 Ischial sore Rt 7� 5 4 FC 8� 6 Quadriplegia None Wound
dehiscenceRevision None 21
8 M 71 Ischial sore Rt 2� 2 12 FC 6.5� 3.5 Paraplegia None None None 239 M 50 Ischial sore
(recurred)Lt 5� 6 4 FC 8� 6 Paraplegia HTN,Sore
operation onceNone Recur after
9 monthsBicepsfemorismuscletransposition
23
10 F 35 Ischial sore Rt 5� 4 12 MC 6� 5 Quadriplegia Spinal AVmalformation
None Recur after6 months
Bicepsfemorismuscletransposition
30
11 M 60 Ischial sore Lt 5� 2.5 6 MC 5.5� 3.5 Lower legweakness
HTN, DM None None 31
12 M 42 Ischial sore(recurred)
Lt 4� 5 5 MC 5� 6 Paraplegia DM, HTN,HBV (þ) Soreoperation3 times
Wounddehiscence
Revision None 34
13 F 61 Ischial sore(recurred)
Lt 1� 1 6 FC 6� 4 Paraplegia DM, Soreoperationonce
None None 37
14 M 38 Ischial sore Rt 3� 3 7 FC 10� 5 Paraplegia Sacral soreoperationtwice
None None 38
15 M 46 Ischial sore Rt 5� 2 1 FC 6� 4 Quadriplegia None None None 3916 M 43 Ischial sore
(recurred)Rt 4� 4 5 FC 7� 5 Paraplegia Sore operation
onceNone None 39
17 M 48 Ischial sore Lt 4� 4 5 MC 5� 4 Paraplegia Sacral soreoperation
Congestionand partialnecrosis at lower margin
ConservativeTx
None 42
1350Y.S.
Kim
et
al.

18M
35Is
chia
lso
re(r
ecu
rred)
Lt0.
5�
112
FC
4�
3Para
ple
gia
Marf
an
SD,
aort
icdis
sect
ion
None
Recu
raft
er
6m
onth
sG
lute
us
maxi
mus
musc
leadva
nce
ment
6
19M
26Is
chia
lso
reLt
0.5�
0.5
9FC
3�
3Para
ple
gia
None
None
None
720
M46
Isch
ial
sore
Lt7�
53
FC
7�
6Lo
wer
leg
weakn
ess
None
Wound
dehis
cence
Revi
sion
None
15
21M
45Is
chia
lso
re(r
ecu
rred)
Rt
2�
25
MC
5�
7Para
ple
gia
Sore
opera
tion
once
None
None
5
22M
59Is
chia
lso
re(r
ecu
rred)
Rt
2�
23
FC
4�
3Para
ple
gia
Sore
opera
tion
once
None
Recu
raft
er
8m
onth
sSe
mit
endin
ous
musc
letr
ansp
osi
tion
9
23M
65Is
chia
lso
re(r
ecu
rred)
Rt
2�
27
MC
8�
6Para
ple
gia
Sore
opera
tion
once
None
None
5
Cx,
com
plica
tion;
Tx,
treatm
ent;
FC,
fasc
iocu
taneous;
MC,
musc
ulo
cuta
neous;
DM
,dia
bete
sm
ellit
us;
HTN
,hyp
ert
ensi
on;
ESR
D,
end
stage
renal
dis
ease
;C
AO
D,
coro
nar
yart
ery
occ
lusi
vedis
ord
er;
AV,
atr
ial
valv
e;
HBV,
hepati
tis
Bvi
rus;
SD,
syndro
me.
Note
that
there
was
no
case
of
tota
lflap
necr
osi
s,but
there
was
one
case
of
part
ialco
nge
stio
nand
desq
uam
ati
on.
Ten
were
recu
rrence
case
sfr
om
apre
vious
conve
nti
onalopera
tion.
The
most
com
mon
short
-term
com
plica
tion
was
part
ial
wound
dehis
cence
,note
dw
ithin
1m
onth
post
opera
tive
ly.
The
sore
recu
rred
infive
pati
ents
,and
all
of
these
case
socc
urr
ed
aft
er
6m
onth
spost
opera
tive
ly.
Aft
er
com
ple
teexc
isio
nof
the
burs
a,
the
dead
space
was
filled
wit
ha
musc
letr
ansp
osi
tion
flap.
Inferior gluteal perforator flap for ischial sores 1351
inferior gluteal thigh fasciocutaneous flap for a secondoperation.2,7 The inferior gluteal thigh fasciocutaneousflap cannot provide sufficient volume and the mobilecharacteristics of the lower extremities result in in-creased tension in this flap. Therefore it is considereda less favourable choice. When the above two flapsare not indicated, myocutaneous flaps, such as the ham-string muscle, gracilis muscle, biceps femoris muscle,and tensor fascia lata flaps are considered.
Over the past 10 years, due to developments in theuse of the perforator flap and increased clinical use ofthe perforator flap, there are more options for availableflaps. Usually the pedicles of the perforator arise fromthe muscle, and dissection of the pedicle allows exclu-sion of the muscle and availability of the flap includingskin and subcutaneous tissue. The perforator flap allowsreconstruction of various areas with minimal donor sitemobility by utilising local or free flaps.
The concept of a perforator flap was introduced byKoshima et al.,3 and successful results have been re-ported for the use of a fasciocutaneous flap with theparasacral perforator of the superior gluteal artery inseven patients. There were also additional reports of sa-cral-coccyx reconstruction with a gluteus maximus mus-cle perforator pedicled flap.8e10 However, due to theinsufficient length of the pedicle, application of a supe-rior gluteal artery perforator flap, which is used for thesacral area, is inadequate for coverage of the ischialarea. Since the report of ischial area pressure sore re-construction by IGAP flap in 2002 by Higgins et al.,4 webegan to use the IGAP flap for ischial area pressuresores. The IGAP flap involves a dissection of the perfora-tor penetrating the gluteus maximus muscle underneaththe piriformis muscle. By separating the dissected ped-icle for an island flap, the defect site can be replacedwithout any tension on the flap. According to studieson cadaver dissection, of the 13 to 20 perforators dis-persed in the gluteus maximus muscle area, 31.5% ofthe perforators are located in the inferior glutealarea,11 and the length and diameter of the pedicle is re-ported to be 3e9.1 cm and 0.7e1.7 mm, respec-tively.3,11 In studies based on Korean populations, thenumber of perforators from the gluteus maximus muscleis reported to be 12.2 and 60% of the perforators origi-nate from the inferior gluteal artery.12
The following precautions should be taken withdissection of the IGAP during elevation. First, vasocon-strictors such as epinephrine, must not be used duringthe bursectomy. Second, with respect to the perforatorslocated preoperatively, available perforators should betraced again with Doppler after bursectomy. Also, theperforator pedicle must not be completely isolated andthe flap must be large enough for coverage.
Use of the perforator flap conserves the adjacentmuscle for subsequent selection of flaps in cases ofrecurrence. This can be important for ischial soresbecause of the higher recurrence rate in the ischium.Also, a perforator flap allows various design choices forthe advancement flap and transposition flap. Tension-free primary closure of the donor site is possible due tosufficient subcutaneous tissue around the donor site andseparation of the suture line of the donor site from the

Figure 2 Case 3 (Above, left) Preoperative view of a 63-year-old male paraplegic patient with left ischial pressure sore. (Above,right) Postoperative view 21 months after reconstruction using IGAP flap. (Below, left) Preoperative design of the flap including twoperforators. (Below, right) Intraoperative view.
1352 Y.S. Kim et al.
pressured area. In 10 cases, perforator flaps were used forrecurrence cases after previous conventional operations,and when the perforator pedicle was preserved in theprimary operation, a secondary operation with the inferiorgluteal perforator flap could be performed. Recurrence wasonly reported in five of our cases during the follow-up
Figure 3 Case 16 (Left) Preoperative view of a 43-year-old male poperative view 7 days after reconstruction using IGAP flap. (Below, lor recurrence.
period, demonstrating that the perforator flap is relativelydurable for reconstruction of ischial sores.
Of course, there are limitations to the application of anIGAP flap. The insufficient supply of subcutaneous tissueresults in dead space and reoperation may be necessary.Paraplegic patients, or those who have lived in long-term
araplegic patient with right ischial pressure sore. (Centre) Post-eft) Forty-eight months postoperatively, showing no breakdown

Figure 4 Case 10 (Above, left) Preoperative view of a 35-year-old female quadriplegic patient with a right ischial pressure sore.(Above, right) Postoperative view immediately after reconstruction using an IGAP flap. (Below, left) Six months after the operation,the pressure sore recurred at the same site. (Below, right) After a complete bursectomy, the dead space was filled with a bicepsfemoris muscle transposition flap.
Inferior gluteal perforator flap for ischial sores 1353
intensive care units, have insufficient subcutaneous tissuedue to cachexia. In one of our cases, wound dehiscencefrom dead space was managed by muscle flap transposition.Also, due to the characteristics of the ischial area, wounddehiscence may develop by exerting pressure after re-suming a seated position. The dehiscence can be treated bysecondary closure or conservative management. However,in cases of bursa or dead space, reoperation with a muscleflap or myocutaneous flap may be necessary.
Inexperienced surgeons may encounter difficulties indissection of the pedicle and when the transpositionvolume of the flap is large and the pedicle length is short,great tension in the flap and pedicle may develop. Inaddition, if the pedicle is completely separated, congestionmay develop due to the kinking phenomenon of the vessels.However, congestion can usually be resolved by conserva-tive management. When recurrence occurs in a short periodpostoperatively or fistulas appear, insufficient resection ofthe bursa or an insufficient volume of soft tissue may havebeen supplied, and this requires reconstruction by a muscleflap or myocutaneous flap.
Despite its shortcomings, the many advantages listedabove make the IGAP flap a useful alternative technique forischial pressure sore reconstruction. However, when the
defect area of the ischial sore is large and the bursa is deep,a perforator flap along with muscle flaps such as a gluteusmaximus muscle advancement flap or biceps femoris muscleor gracilis muscle transposition flap can be considered to fillthe large dead space for successful results.
In conclusion, for the past 4 years we have used an IGAPflap for the reconstruction of ischial sores at our institute.Based on its characteristics, such as preservation ofadjacent muscles, variability of flap designs, durability,and minimal donor site morbidity, the IGAP flap should beconsidered a viable alternative to other methods of ischialsore reconstruction surgery.
Disclosure
None of the authors has a financial interest in any of theproducts, devices, or drugs mentioned in this article.
References
1. Foster RD. Pressure sores. In: Mathes SJ, editor. Plasticsurgery. 2nd ed., Vol 6. Philadelphia: Saunders/Elsevier;2006. p. 1321.

1354 Y.S. Kim et al.
2. Foster RD, Anthony JP, Mathes SJ, et al. Ischial pressure sorecoverage: a rationale for flap selection. Br J Plast Surg 1997;50:374e9.
3. Koshima I, Moriguchi T, Soeda S, et al. The gluteal perforator-based flap for repair of sacral pressure sores. Plast ReconstrSurg 1993;91:678e83.
4. Higgins JP, Orlando GS, Blondeel PN. Ischial pressure sore re-construction using an inferior gluteal artery perforator (IGAP)flap. Br J Plast Surg 2002;55:83e5.
5. Goodman CM, Cohen V, Armenta A, et al. Evaluation of re-sults and treatment variables for pressure ulcers in 48 vet-eran spinal cord-injured patients. Ann Plast Surg 1999;42:665e72.
6. Kierney PC, Engrav LH, Isik FF, et al. Results of 268 pressuresores in 158 patients managed jointly by plastic surgeryand rehabilitation medicine. Plast Reconstr Surg 1998;102:765e72.
7. Stevenson TR, Polloc RA, Rohrich RJ, et al. The gluteus maxi-mus musculocutaneous island flap: refinements in design andapplication. Plast Reconstr Surg 1987;79:761e8.
8. Ao M, Mae O, Namba Y, et al. Perforator-based flap for coverageof lumbosacral defects. Plast Reconstr Surg 1998;101:987e91.
9. Roche NA, Van Landuyt K, Blondeel PN, et al. The use ofpedicled perforator flaps for reconstruction of lumbosacraldefects. Ann Plast Surg 2000;45:7e14.
10. Cosxkunfirat OK, }Oxgentasx HE. Gluteal perforator flaps for cov-erage of pressure sores at various locations. Plast ReconstrSurg 2004;113:2012e7.
11. Kankaya Y, Ulusoy G, Oruc M, et al. Perforating arteries of thegluteal region: anatomic study. Ann Plast Surg 2006;56:409e12.
12. Song WC, Bae SM, Lee BY, et al. An anatomical study of the su-perior and inferior gluteal arteries supplying gluteus maximusfor musculocutaneous flaps. Korean J Phys Anthropol 2002;15:149e58.