Embed Size (px)
DESCRIPTION
kijhk
Citation preview

Bacterial Urinary Tract Infection
(UTI)
Riyani Wikaningrum
Bag. Mikrobiologi
FKUY





Terminology Used in UT
infections

Upper Urinary Tract Infection
• the urinary tract above the level of the bladder; that is, the ureters, kidneys, and peri-renal tissues.
• pyelonephritis.
• “Upper UTI” also encompasses – intrarenal abscess (“renal carbuncle”)
– perinephric abscess.
• Renal papillary necrosis refers to infarction of the papillae (sometimes with sloughing into the ureters) caused by pyelonephritis or analgesic abuse – diabetes mellitus
– sickle cell disease
– ureteral obstruction.

Acute bacterial pyelonephritis
• clinical syndrome
– Fever
– flank pain
– often with constitutional symptoms
• Laboratory findings:
– Leukocytosis
– leukocyte casts in the urine
– bacteriuria with or without signs of concomitant inflammation in the bladder

Lower Urinary Tract Infection
• Lower urinary tract infection refers to infection at or below the level of the bladder. In clinical practice, “lower UTI” is often used synonymously with “cystitis,” a syndrome characterized by dysuria, frequency, urgency, and variable suprapubic tenderness. Because one cannot say with certainty that infection involves mainly or exclusively the urinary bladder, some authorities suggest that “cystitis” should be abandoned. “Lower UTI” also encompasses prostatitis, urethritis, and infection of the periurethral glands.

Chronic bacterial pyelonephritis
• long-standing infection with active bacterial growth in the kidney, or the presence of residual lesions in the kidney caused by such infection in the past.
• Chronic interstitial nephritis – in which evidence for an etiologic role for
bacterial infection is lacking.
– Etiology : Drugs (not only prescription drugs but also non-prescription drugs as in analgesic nephropathy)

Introduction
• 20 – 30% females have recurrent urinary
tract infection (UTI)
• Men less common and primary occur
after 50 years old
• Acute infection

Common
cused
of UTI

Acquisition and Etiology
• Bacterial infection is usually acquired by the ascending route from the urethra to bladder
– Community acquired
– Hospital acquired catheterization
• Etiology
– E. coli and P. mirabilis
– Klebsiella, Enterobacter, Serratia sp, P aeruginosa hospital acquired
– Ureaplasma

– Gram-positive S. saprophyticus, S. epidermidis, and Enterococcus
– Hematogenous spread S. enterica Serotype Typhi, S. aureus and M. tuberculosis
• Viral cause of UTI rare but certain virus can be recovered from the urine in the absent of UTI, e.g. CMV, rubella, adenovirus, hantavirus
• Very few parasites cause UTI Candida; H. capsulatum; Trichomonas vaginalis; Schistostoma haematobium

Pathogenesis
• Predisposing factors:
– Disruption of urine flow
– Short female urethrae
– Sexual intercourse
– In male infants uncircumcised
– Pregnancy
– Prostatic hypertrophy
– Catheterization

Pathogenesis

Risk Factor in Female

Clinical Features
• Acute lower UTIs cause
– Dysuria burning pain on passing urine
– Urgency the urgent need to pass urine
– Frequency on micturition
• The urine is cloudy due to pyuria and
bacteriuria
• Pyuria in the absence of positive culture
chlamydial; mycobacterial infections
• Pyelonephritis causes a fever and lower
urinary tract symptoms

• Asymptomatic infections
– Pregnant women
– Young children
– Catheterization may proceed to bacteremia
– Elderly persons
– Diabetes

Laboratory Diagnosis
• Specimens:
– MSU
– Suprapubic aspiration of urine
– ‘bag urine’
– Urine in catheterized patients ………..
• Quantitative culture methods
– Infections bacterial count >= 105/ml urine
– Contaminated less than 103/ml urine

Sample Collection (supra pubic puncture)

Sample collection (in situ cathether)

Pyuria

Interpretation of Quantitative
Culture

• Interpretation of the significant bacterial cultures depends upon a variety factors:
– Collection of specimen
– Storage
– Antibiotic treatment
– Fluid intake
• Special urine samples:
– Three early morning urine samples on consecutive days for M. tuberculosis
– The last few milliliters of morning urine sample collected after exercise for detection of S. haematobium

Treatment
• Uncomplicated UTI oral antibacterial as
single dose or 3 days
• Complicated UTI (pyelonephritis)
systemic antibacterial agents

Prevention
• Reccurent infection in healthy women
Regularly emptying the bladder
• Avoid catheterization if possible or keep to
minimum duration

GUIDELINES FOR CATHETER
CARE
• avoid catheterization whenever possible
• keep duration of catheterization to a minimum
• use intermittent rather than continuous catheterization
when feasible
• insert catheters with good aseptic technique
• use a closed sterile drainage system
• maintain a gravity drain
• use topical antiseptics around the meatus in women
• wash hands before and after inserting catheters and
collecting specimens, and after emptying drainage bags.

Escherichia coli

Escherichia coli
• Flora normal pada usus manusia & hewan
• Manifestasi klinis:
– Infeksi saluran kemih: penyebab 80% kasus; kuman hemolisin (+), tahan serum, faktor virulensi pili P
– Septisemia: asal infeksi adalah infeksi saluran kemih atau penjalaran kuman dari usus
– Meningitis pada neonatus: E. coli K1
– Gastroenteritis (Diare) karena E. coli

• Pathogenesis factors of bacteria:
– Somatic serotype O1, O2, O4, O6, O7,
O75
– Capsular serotype K1, K2, K3, K5, K12,
K13
– Pili P Uropathogenic E. coli (UPEC)
• The healthy urinary tract is resistant to
bacterial colonization, due to:
– pH, chemical content and flushing mechanism
of urine


UPEC (Uropathogenic E. coli)
BACK

Proteus, Providencia, Morganella
• Spesies penting: P. vulgaris, P. mirabilis
• Pertumbuhan: menjalar, H2S (+), urease
(+)
• Manifestasi klinis: infeksi sal. kemih,
bakteremia, pneumonia, infeksi
nosokomial (P.vulgaris; Morganella)
• Terapi: ampisilin, trimetoprim. Perlu tes
sensitivitas kuman

Proteus
BACK

Klebsiella
• Morfologi Kuman: batang, Gram (-), gerak (-), mempunyai kapsul tebal
• Faktor virulensi:
– Kapsul menghambat fagositosis
– Ag.O menghambat lisis oleh komplemen
• Manifestasi Klinis:
– infeksi saluran kemih, bronkhopneumoni, infeksi nosokomial

Enterobacter
• Serupa dengan Klebsiella, hanya gerak (+)
• Spesies penting: E. aerogenes & E.
cloacae
• Penyebab infeksi nosokomial, dan infeksi
saluran kemih
• Umumnya resisten terhadap penisilin
• Terapi: gol. aminoglikosida
BACK

Family: Mycoplasmataceae
• Genus: Mycoplasma
– Species: M. pneumoniae
– Species: M. hominis
– Species: M. genitalium
• Genus: Ureaplasma
– Species: U. urealyticum

Organism Disease
M. pneumoniae Upper respiratory tract disease,
tracheobronchitis, atypical
pneumonia, (chronic asthma??)
M. hominis Pyleonephritis, pelvic
inflammatory disease,
postpartum fever
M. genitalium Nongonococcal urethritis
U. urealyticum Nongonococcal urethritis,
(pneumonia and chronic lung
disease in premature infants??)
Diseases Caused by Mycoplasma

Morphology and Physiology
• Smallest free-living bacteria (0.2 - 0.8 m)
• Small genome size
– Require complex media for growth
• Facultative anaerobes
– Except M. pneumoniae - strict aerobe
• Lack a cell wall
• Grow slowly by binary fission
• “Fried egg” colonies – M. pneumoniae colonies have a granular
appearance

“Fried Egg” Colonies of
Mycoplasmas

Morphology and Physiology
• Ureaplasma - T strains
• Require sterols for growth

Differentiation of Species
• M. pneumoniae - glucose
• M. hominis - arginine
• U. urealyticum - urea
• M. genitalium - difficult to culture

M. hominis, M. genitalium and
U. urealyticum
• Clinical syndromes
– M. hominis - pyleonephritis, pelvic inflammatory
disease and postpartum fever
– M. genitalium - nongonococcal urethritis
– U. urealyticum - nongonococcal urethritis
• Epidemiology
– Colonization at birth - usually cleared
– Colonization with M. hominis - 15%
– Colonization with U. urealyticum - 45% -75%
– Colonization with M. genitalium - ??

M. hominis, M. genitalium and
U. urealyticum
• Laboratory diagnosis
– Culture (except M. genitalium)
• Treatment and prevention
– Treatment
• Tetracycline or erythromycin
– Prevention
• Abstinence or barrier protection
• No vaccine
BACK

INFEKSI pada PROSTAT

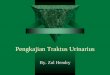
Sampling Technique

Three-glass Procedure

Meares and Stamey localization technique

1. Approximately 30 minutes before taking the specimen,
the patient should drink 400 ml of liquid (two glasses).
The test starts when the patient wants to void
2. The lids of four sterile specimen containers, which are
marked VB1, VB2, EPS and VB3, should be removed.
Place the uncovered specimen containers on a flat
surface and maintain sterility
3. Hands are washed
4. Expose the penis and retract the foreskin so that the
glans is exposed. The foreskin should be retracted
throughout
5. Cleanse the glans with a soap solution, remove the
soap with sterile gauze or cotton and dry the glans
6. Urinate 10–15 ml into the first container marked VB1

7. Urinate 100–200 ml into the toilet bowl or vessel and
without interrupting the urine stream, urinate 10–15 ml
into the second container marked VB2
8. The patient bends forward and holds the sterile
specimen container (EPS) to catch the prostate
secretion
9. The physician massages the prostate until several
drops of prostate secretion (EPS) are obtained
10. If no EPS can be collected during massage, a drop may
be present at the orifice of the urethra and this drop
should be taken with a 10 ml calibrated loop and
cultured
11. Immediately after prostatic massage, the patient
urinates 10–15 ml of urine into the container marked
VB3.

Prostatitis: • Akut - Disebabkan oleh:
– E. coli
– P. aeruginosa
– Serratia sp.
– Klebsiella sp.
– Proteus sp.
– Enterococci
– Staphylococcus
• Kronik
– dibagi menjadi 3 sindrom:
• Chronic bacterial prostatitis
• Chronic abacterial prostatitis/CPPS-inflammatory
• Chronic abacterial prostatitis/CPPS-non-inflammatory
– Disebabkan S. aureus, S. faecalis, Enterococcus, difteroid


Prostatitis
• Pemeriksaan laboratorium:
– MSU
– EPS (expressed prostatic secretion – digital rectal
massage):
• Lepas antibiotik selama 1 bulan
• Tidak mengalami ejakulasi selama 2 hari

Epididymo-orchitis
• Penyebab: – Mumps virus
– Coxsackievirus
– N. gonorrhoeae
– C. trachomatis
– E. coli
– Koliform lainnya