Embed Size (px)
Citation preview

Clinical Microbiology Newsletter 35:7,2013 © 2013 Elsevier 0196-4399/00 (see frontmatter) 53
Common Infections after LiverTransplantation
Orthotopic liver transplantation(OLT) has been performed since 1963(1). Over the last few decades, the 1-and 5-year survival rates have improvedtremendously, up to 92 and 86%,respectively (2).
Infections are still a leading compli-cation in OLT recipients and occur atrates of 54 to 67% of patients (3). Theinfections that are most common aredue to bacteria (22%) and viruses (6%)(4). Infections in this population dependon the time after transplant and areassociated with different risks. In theearly post-transplantation period (thefirst month), infections are due to 4major risk factors. They are the dura-tion of surgery, the number of bloodproducts transfused, the amount of
blood in the peritoneal cavity, and theneed for retransplantation. The mostcommon organisms causing infectionduring this period include nosocomialbacteria, such as methicillin-resistantStaphylococcus aureus, vancomycin-resistant enterococci (VRE), multi-drug-resistant Gram-negative bacteria,Clostridium difficile, and Candida spp.Additionally, problems can arise fromtechnical aspects of the transplant pro-cedure, such as bile leaks. Infectionsthat occur after the first month untilthe sixth month posttransplantation areusually due to opportunistic organisms,such as fungi, cytomegalovirus (CMV),or Pneumocystis. This is the time ofmaximal immunosuppression. After thesixth month posttransplantation, how-ever, the potential for opportunisticinfections continues, and the risk forcommunity-acquired bacterial infectionis important (5).
Bacterial InfectionsBacteria cause infections in almost
70% of liver transplant recipientsduring the early posttransplantationperiod and have an associated 13%
mortality. Bloodstream, wound, andintraabdominal infections account forthe majority of bacterial infectionsduring this period (6).
Gram-positive bacteria accountfor the majority of bacterial infections,which are mainly due to S. aureus,coagulase-negative staphylococci,Streptococcus spp., and Enterococcusspp. In particular, VRE play a large rolein infections in liver transplant recipi-ents. A recent report shows a prevalenceof colonization among liver recipientsbetween 3.4% and 55% (7). Anotherreport shows a VRE infection ratebetween 4% and 11% (8). VRE cancause urinary tract infections (UTIs)and wound infections, as well as blood-stream infections and endocarditis insome cases. The Gram-negative bacteriaalso cause significant morbidity and
Vol. 35, No. 7 www.cmnewsletter.com April 1, 2013
ClinicalMicrobiologyNewsletter
Stay Current ...Stay Informed.
Infections in Liver, Kidney, Pancreas, and Intestinal TransplantRecipientsHeather E. Clauss, M.D.,1 Rafik Samuel, M.D.,1 George J Alangaden, M.D.,4 Pranatharthi Chandrasekar, M.D.,4 Allan L. Truant,Ph.D.,2 Donald Jungkind, Ph.D.,3 and Byungse Suh,1 M.D., Ph.D., Section of Infectious Diseases, Temple University School ofMedicine,1 and Clinical Microbiology, Immunology, and Virology Laboratories, Department of Pathology and LaboratoryMedicine, Temple University Hospital and School of Medicine,2 Jefferson University Hospital and School of Medicine,3
Philadelphia, Pennsylvania, Division of Infectious Diseases, Transplantation Infectious Diseases Unit, Wayne State Schoolof Medicine,4 Detroit, Michigan
AbstractPatients who need abdominal organ transplantation are at high risk for community-acquired, nosocomial, and opportunistic
infections. In part, this is due to the invasive procedures they undergo, as well as the immunosuppression they require. Thisreview highlights the infections that these vulnerable patients may develop. The current epidemiology, diagnosis, and manage-ment of common infections in liver, kidney, pancreas, and intestinal transplant (IT) recipients are summarized here.
Corresponding Author: Allan L. Truant,Ph.D., Clinical Microbiology Laboratories,Department of Pathology and LaboratoryMedicine, Temple University School ofMedicine, 3401 N. Broad St., Philadelphia,PA 19140. Tel.: 215-707-3210. Fax: 215-707-3389. E-mail: [email protected]

54 0196-4399/00 (see frontmatter) © 2013 Elsevier Clinical Microbiology Newsletter 35:7,2013
include Enterobacteriaceae, such asEscherichia coli, Klebsiella spp., andEnterobacter spp., and others, includingPseudomonas aeruginosa and Acineto-bacter spp. There is worldwide variationin the amount of extended-spectrumbeta-lactamase (ESBL) production fromthese Gram-negative bacteria. In a sur-vey in 2001, 67% of the gastrointestinaltracts of liver transplant recipients in oneunit were found to be colonized withESBL-producing E. coli (9). P. aerugi-nosa was documented to be resistant47% of the time in infections in livertransplant recipients (10). These orga-nisms mostly cause intra-abdominalinfections. Clostridium difficile is afrequently encountered infectious bac-terium in solid-organ transplant (SOT)recipients. The incidence is estimatedto be 3 to 7% in liver recipients (11).Nocardia spp. cause infections inapproximately 0.1% of liver transplantrecipients (12, 13). Listeria monocyto-genes is another infectious bacteriumthat can occur rarely in SOT recipients.Mycobacterium tuberculosis also
causes infections in liver transplantrecipients. It has been reported to causeinfections in SOT recipients at a ratethat is 20- to 74-fold higher than in thegeneral population (14). These patientsusually have reactivation of latent tuber-culosis (TB) that causes fever and pos-sibly allograft dysfunction. A third ofthe patients have dissemination of theorganism. The transplant recipientsusually develop reactivation in the firstyear after the transplant (15). Treatmentwith isoniazid, ethambutol, and pyra-zinamide for 9 months is recommendedif no resistance is suspected (14). Theincidence of liver toxicity is about 50%in OLT recipients but 33 to 37% inother SOT recipients. Screening forlatent tuberculosis in liver transplantcandidates via a pretransplant PPDor interferon gamma release assay isimportant. Treatment of latent TB canbe attempted with isoniazid for a 9-month course or rifampin for a 4-monthcourse. At times, this treatment may bedeferred until after liver transplantationdue to the hepatotoxicity of theseagents.
Viral InfectionsMany viral agents cause disease in
the OLT population. These organismscause significant morbidity and mor-
tality. None is more significant thanCMV (16). CMV is the most commonopportunistic viral infection after OLT.CMV is a betaherpesvirus. OLT recipi-ents can develop disease from CMV indifferent ways. First, it can be transmit-ted in the transplanted organ. Second,the virus can be transmitted via trans-fusion with blood that is CMV positive.Third, the OLT recipient can undergoreactivation of previously dormant CMV.Finally, there can be a new primaryinfection from a CMV-positive contact.CMV disease occurs in 20 to 30% ofOLT recipients.
The average time of infection in theabsence of CMV prophylaxis is about4 weeks after the transplantation, anddisease can occur about 2 weeks after-ward. The incidence of infection dependson the seropositivity of the donor andthe recipient. If both are negative, therate of disease is 10 to 22%. If the donoris positive and the recipient is negative,approximately 75% of the recipients willdevelop CMV disease. If the recipientis positive, whether or not the donor ispositive, this leads to an incidence ofdisease of 25 to 30% (17).
CMV has a predilection to invadethe allograft. CMV hepatitis is the mostcommon manifestation of CMV infec-tion in the OLT recipient, even thoughit is rarely seen in recipients of otherorgans. Patients present with fever andabnormal liver function test results thatcould be confused with graft rejection.To make the diagnosis, a liver biopsydemonstrating CMV inclusion bodies isnecessary. Treatment of CMV hepatitisincludes ganciclovir (GCV) or, for casesof GCV resistance, foscarnet. Othermanifestations of CMV infection includeinvolvement of the lungs or the gastro-intestinal tract. In patients receiving anOLT, antivirals are recommended toprevent acquisition or reactivation ofthe infection. This can be accomplishedin two ways. A universal prophylaxisregimen of GCV or valganciclovir(VGCV) for a defined period of timeafter transplantation and a preemptivetreatment strategy have been studied.Preemptive therapy involves seriallyassessing the patient for CMV infec-tion, typically with a CMV PCR orCMV antigenemia assay, and treatingthe patient only at a specified level ofCMV detection.
A meta-analysis performed to assess
the efficacy of preemptive and prophy-lactic strategies in reducing CMV dis-ease in 1,980 SOT recipients, including681 OLTs, showed that both strategiesreduce the incidence of CMV disease(18). Oral GCV at 1 g 3 times dailyshowed a reduction of CMV organdisease compared with controls whenused either by preemptive (72%) or byuniversal prophylactic (85%) strategies.
For treatment of CMV disease, intra-venous GCV as induction for 2 to 3weeks is recommended. The dose shouldbe 5 mg/kg of body weight twice daily,adjusted for renal function. Oral VGCVhas also been shown to be effective at900 mg twice daily as an inductioncourse. Maintenance therapy should behalf the dose of either GCV or VGCVfor the duration of the course.
Epstein-Barr virus (EBV) is a gamma-herpesvirus and has been associatedwith post-transplant lymphoprolifera-tive disease (PTLD). PTLD is a signi-ficant cause of morbidity in the OLTpopulation. The incidence of disease inthis group is about 2.2%. The findingsof PTLD range from localized lesionsto multisystem disease to lymphoma.The approach to treatment includesdecreasing the immunosuppressionand, depending on the severity of thedisease, chemotherapy, surgery, anti-viral agents, and even use of mono-clonal antibodies.
Herpes simplex virus 1 (HSV-1) andHSV-2 are alphaherpesviruses. They canlead to cutaneous lesions that includevesicles or ulcers. In OLT recipients,they can lead to disseminated or vis-ceral disease, which includes hepatitis(19). Most disease from HSV is dueto reactivation of previously acquiredvirus. Primary infection from the allo-graft is rare but has been described inliver transplant recipients (20). Hepa-titis can develop in the first month aftertransplantation with a median time of18 days after the transplantation. Thefrequency of disseminated HSV diseaseafter transplantation has been reducedby the use of antiviral prophylaxis.
Chronic hepatitis B virus (HBV)and hepatitis C virus (HCV) infectionsrepresent important causes of liver fail-ure leading to liver transplantation. HBVcan recur in 75 to 80% of OLT recipientsand can significantly damage the graftand decrease survival after transplanta-tion (21). There are multiple predictors

of recurrence after transplantation. Themost important predictor is the HBVload. If the HBV load is greater than1 million copies, the relapse rate is upto 85%. On the other hand, if the OLTrecipient is HBV antigen negative,the risk of relapse is much lower. Itis also lower in those with fulminanthepatitis B.
As a result, the HBV load should belowered before transplantation. Recur-rent hepatitis B after OLT leads to anaggressive infection causing fibrosingcholestatic hepatitis. Antiviral therapyfor HBV, such as lamivudine, adefovirdipivoxil, or possibly entecavir, com-bined with hepatitis B immune globulin(HBIG) significantly improves the out-comes for OLT recipients with HBVinfection. A combination of HBIG andlamivudine can drop the rate of recur-rence to below 10% (22).
Ninety percent of OLT recipientswho have hepatitis C develop chronichepatitis by 5 years after transplantation(23). HCV replication in the allograft isevident within hours to days after livertransplantation, and the infection takeson an accelerated course. As with hepa-titis B, bringing the HCV load down toless than a million can improve graft andpatient survival. Currently, the standard-of-care regimen for HCV infections isa combination of pegylated interferonpreparations and ribavirin. The rate ofsustained virologic response in patientson this regimen varies substantiallywith pretreatment host characteristics,including viral load, age, body weight,and, most importantly, the genotype ofthe virus. The newly approved proteaseinhibitors that treat hepatitis C have notyet been studied for HCV recurrenceafter liver transplantation.
All donors and recipients should bescreened for HIV, since it can be trans-mitted with the transplanted organ. Therehave been recent data to indicate thatHIV-infected patients can do well afterOLT as a result of highly active anti-retroviral therapy (HAART).
The survival rates for 12, 24, and 36months after OLT procedures amongHIV-positive and -negative recipientswere comparable (24). Carefully selectedpatients should have a CD4 count greaterthan 100 for 3 months, an undetectableviral load, and no history of opportunis-tic infections and be on a stable HAARTregimen.
Fungal InfectionsCandida species are the most com-
mon cause of invasive fungal infectionafter liver transplantation. In many organtransplant recipients, invasive candidiasisoccurs within the first 3 months follow-ing transplantation, but in liver trans-plantation, this risk period is extendedbeyond 3 months (25). Candida albicansis typically the dominant pathogen. Thereare both medical and surgical risk fac-tors for invasive candidiasis. In livertransplantation, a choledochojejunos-tomy is associated with a higher riskof candidiasis than a choledocho-chole-docho anastomosis (26). Antifungalprophylaxis against Candida should begiven to all liver transplant recipientsat high risk for development of invasivecandidiasis. High risk has been definedas those patients with ≥ 2.0 of the fol-lowing risk factors: prolonged or repeatoperation, retransplantation, renal failure,high transfusion requirement, choledo-cojejunostomy, and Candida coloniza-tion in the perioperative period (25).Cryptococcus neoformans is a
ubiquitous yeast. Cryptococcosis istypically a late-occurring infection. Themedian time to onset usually ranges from16 to 21 months post-transplantation.The time to onset is earlier for livertransplant recipients and is <12 months,perhaps due to a higher intensity ofimmunosuppression in these patients(27). The organism enters the bodythrough the respiratory tract. The orga-nism can lead to a pneumonitis but hasa tropism for the central nervous system,resulting in meningitis. The mortalityrate for cryptococcal meningitis is 71%in transplant recipients. Treatment witha lipid formulation of amphotericin incombination with flucytosine is recom-mended. Alternatives include flucona-zole, itraconazole, or voriconazole (28).Aspergillus spp. can cause signifi-
cant disease in a transplant recipient.It is the second most common invasivefungal infection in this population. Thetime of infection is usually in the first6 months after transplantation, but therisk can persist. Invasive aspergillosis inOLT recipients presents with localizedpneumonitis with an accompanyingmental status change. Major risk factorsfor invasive aspergillosis include allo-graft dysfunction and HCV or CMVinfection (29). The mortality rate ofAspergillus infection approaches 100%
in the OLT population. In a study look-ing at mold infections, non-Aspergillusgenera accounted for 30% of the mycelialfungal infections (30). The most com-mon non-Aspergillus organisms foundincluded Scedosporium apiospermum,Fusarium spp., and Zygomycetes. Theseinfections were more often associatedwith dissemination, with mortalityapproaching 100%, as well.Pneumocystis jirovecii causes an
atypical subacute pneumonitis in organtransplant recipients. Among liver andkidney transplant (KT) recipients, theincidence appeared to be lower thanamong heart and lung recipients, fromclose to 2% to 10 to 15% (31). Thisincidence has significantly decreasedwith the use of prophylaxis and thedecrease in steroid dosing in immuno-suppressive regimens. One study demon-strated that a corticosteroid dose of 16mg prednisone for 8 weeks is associatedwith a significant risk of Pneumocystiscarinii pneumonia PCP in patients with-out HIV infection. Symptoms includenonproductive cough, shortness of breath,and fevers; however, they are not speci-fic. A chest radiograph demonstratesbilateral interstitial infiltrates. The mor-tality rate is high and can reach 60%(32). Induced sputum or bronchoscopywith bronchoalveolar lavage should beperformed to make the diagnosis. Thespecimen should be sent for specialstaining, such as Gomori methenaminesilver, to identify the cysts.
Parasitic InfectionsProtozoan infections are uncommon
in OLT recipients in developed countries.Potential donors or recipients from areasof endemicity or travelers to areas ofendemicity should be screened for pos-sible infection. Malaria in OLT patientsgenerally carries a mortality rate of 40%compared to approximately 6% in KTrecipients (33).Toxoplasma gondii is a parasite that
is ubiquitous in nature that causes ence-phalitis and meningoencephalitis, myo-carditis, pneumonitis, and disseminatedlymphadenopathy in transplant recipi-ents. Toxoplasma infections can betransmitted from a donor to a negativerecipient or, more commonly, can occurfrom reactivation of an endogenousToxoplasma infection. Treatment oftoxoplasmosis includes pyrimethamineand sulfadiazine. Other agents that have
Clinical Microbiology Newsletter 35:7,2013 © 2013 Elsevier 0196-4399/00 (see frontmatter) 55

56 0196-4399/00 (see frontmatter) © 2013 Elsevier Clinical Microbiology Newsletter 35:7,2013
been used include clindamycin, trimetho-prim-sulfamethoxazole (TMP/SMX),atovaquone, azithromycin, and dapsone.
In the southeastern United States andthe Caribbean, Strongyloides stercoraliscan be an important pathogen. Often,donors and recipients are screened usingserial stool direct examinations for ovaand parasites, as well as a Strongyloidesenzyme-linked immunosorbent assay.Routine screening is recommended onlyfor patients living in this area or with anextensive travel history there.
Risk and Temporal Sequenceof Infection After Kidney,Pancreas, and IntestinalBowel Transplantation
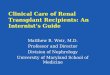
The risk for infections caused byspecific pathogens follows a predictabletemporal pattern dictated by the intensityof immunosuppression (34,35) (Fig. 1).In the first month, infections generallyresult from complications of surgery,and bacterial infections predominate.Opportunistic infections caused by vir-uses and fungi occur during the secondperiod (2 to 6 months) as a consequenceof impaired cell-mediated immunitycaused by anti-rejection therapy. Strate-gies for prevention of infections withspecific pathogens, e.g. CMV and P.jirovecii, have been developed basedupon this sequence of infections. How-ever, the pattern of infection may bealtered by the intensification of immuno-suppressive therapy, the use of neweranti-rejection therapies, and the imple-mentation of antimicrobial prophylaxis.After the 6-month period, primarily dueto the decrease in immunosuppressivetherapy, infections decline, and therelative risks are similar to the non-transplant population.
Common Infections AfterKidney Transplantation
KTs account for the majority of SOTs.The 5-year survival of KT recipients is81% to 90 %, with graft survival ratesof 67% in deceased-donor and 80% inliving-donor transplantations. The goodoutcomes after KT, in large measure, areattributable to the low (<5%) infection-related morbidity and mortality.
The most common infections in KTrecipients at our Detroit facility are UTIs(47%), opportunistic viral infections(17%), pneumonia (8%), surgical woundinfections (SWIs) (7%), and bacteremia
(6%). During the first month, bacterialinfections predominate, with viralinfections occurring later. Commonopportunistic pathogens are listed inTable 1.
Urinary Tract InfectionUTIs occur in 5% to 10% of KT
recipients and are the commonestinfections in the first 6 months aftertransplantation. Enterobacteriaceaeaccount for the majority of UTIs, withE. coli being the most common patho-gen. Enterococcus spp. have been iden-tified as important uropathogens in theearly KT period (36). Antimicrobialprophylaxis against UTIs is often usedafter KT; TMP/SMX is the most com-monly used agent. TMP/SMX prophy-laxis has also significantly decreasedopportunistic infections caused by P.jirovecii, L. monocytogenes, Nocardiaasteroides, and T. gondii (37). Empirictherapy for UTI should include cover-age for Enterobacteriaceae (38). Spe-cific therapy should be modified basedupon the results of cultures. Break-through UTI while on prophylaxis orrecurrent and relapsing UTIs necessitatefurther workup to exclude anatomical orfunctional defects of the urinary tract.
Surgical Wound InfectionThe incidence of SWIs in KT recipi-
ents is low (<5%). S. aureus is the mostcommon pathogen isolated from woundinfections, but infections due to Gram-negative enteric bacteria, Staphylo-
coccus epidermidis, Candida spp.,and Mycoplasma hominis may occur.
Lower Respiratory Tract InfectionPneumonia occurs in <5% of KT
recipients and bacterial pathogensaccount for the majority of infections,with Streptococcus spp., Haemophilusinfluenzae, and S. aureus being thecommonest. P. jirovecii and CMV maycause infection in patients not receivingappropriate prophylaxis.M. tuberculo-sis is an important respiratory pathogenin countries where it is endemic.
Specific Opportunistic Pathogensof importance in KT recipients
The improper functioning of cell-mediated immunity, which may resultfrom anti- rejection therapy, can set thestage for infections caused by opportu-nistic intracellular pathogens. Most ofthese infections are a consequence ofreactivation of latent infection duringimmunosuppression.
PolyomavirusPolyomavirus-associated nephropa-
thy (PVAN) is as an important causeof kidney allograft dysfunction and iscaused by reactivation of polyoma virushominis type 1 (39), also known as BKvirus (BKV). PVAN occurs in 1 to 10%of KT recipients and is characterized byallograft dysfunction, viremia, and mor-phological and immunohistochemicalevidence of polyomavirus (PV)infection.
Figure 1. Risk of common infections in kidney transplant recipients
Phase I Phase II Phase Ill0-30 days 30-180 days >180 days
Urinary tract infection Polyomavirus nephropathy
Surgical site infections Cytomegalovirusinfection
(in absence ofprophylaxis)
Pneumocystisjirovecci infection
(in absence ofprophylaxis)
Cytomegalovirusinfection
(late onset as a resultof prophylaxis)

Clinical Microbiology Newsletter 35:7,2013 © 2013 Elsevier 0196-4399/00 (see frontmatter) 57
Screening assays for BKV areincreasingly utilized for the diagnosisand management of PVAN. They includeurine cytology for the detection of PV-infected “decoy cells” and moleculartests for the detection and quantificationof BK DNA in plasma or urine. Defini-tive diagnosis of PVAN requires demon-stration of PV infection in the renal grafttissue. There are no specific antiviralagents to treat PV infection; the primarytherapeutic approach is to reduce theintensity of immunosuppression.
CMVSymptomatic CMV infection occurs
in 20 to 60% of transplant recipients.CMV infection can result from (i) pri-mary infection caused by transmissionof CMV from a CMV-seropositivedonor (D+) kidney to a CMV-seronega-tive (R-) recipient (this is the group athighest risk) and (ii) reactivation ofCMV in a seropositive recipient. CMVinfection and disease can present asasymptomatic infection, mononucleo-sis-like syndrome, or life-threateningsystemic disease. The presence of dis-ease is confirmed by demonstration ofCMV in the tissue. The CMV antigene-mia test is a semi-quantifiable assaythat detects the pp65 protein of CMVwithin polymorphonuclear leukocytesin blood and is used with decreasingfrequency as a screening assay. Moresensitive and rapid qualitative and quan-titative nucleic acid amplification teststhat detect CMV DNA are increasinglyused for diagnosis, as well as for mon-itoring the response to therapy. Thetherapy for CMV disease requiresdecreasing immunosuppression, alongwith antiviral therapy (40). IntravenousGCV is the drug of choice, although oralVGCV, a pro-drug of GCV, has beenused. CMV disease can be prevented bymatching CMV-negative donors withseronegative recipients and prophylaxiswith antiviral agents. CMV prophylaxisis recommended especially for highriskpatients (0+/R-) for the first 3 months. InSOT recipients receiving antiviral pro-phylaxis, late-onset CMV disease afterdiscontinuing prophylaxis has occurred(41). The use of GCV has also resultedin the emergence of GCV-resistantstrains of CMV. Most GCV-resistantisolates are associated with a mutation,UL97, in the CMV phosphotransferasegene or a UL54 mutation in the DNApolymerase gene. Rapid genotypic PCR
assays can identify these specificmutations.
EBV-associated PTLDPTLD is a term used to describe
lymphoproliferative diseases that occurin <2% of KT recipients. The incidenceof PTLD is highest during the first yearwithin the period of intense immuno-suppression. It results from abnormalproliferation of recipient B cells that areEBV infected and can cause disease thatranges from benign lymphoid hyperpla-sia to malignant lymphoma (42). Mostcases occur as a result of acquisition ofEBV from the donor, resulting in primaryinfection, often in pediatric recipients.The diagnosis of PTLD is confirmed byin-situ hybridization tests that detect
EBV within the affected cells. Quanti-tative-PCR screening tests are used todetect EBV in the blood. High EBVloads trigger pre-emptive reduction ofimmunosuppression to prevent thedevelopment of PTLD.
West Nile Virus InfectionThere have been reports of West Nile
virus (WNV) transmission to differentorgan recipients from the same infecteddonor. The diagnosis is confirmed bydetection of WNV lgM antibodies inthe cerebrospinal fluid or by the use ofnucleic acid amplification tests.
Fungal infectionsDespite their low incidence, fungal
infections in KT recipients are associatedwith the highest mortality. Candida is
Table 1. Opportunistic pathogens in kidney transplantation
Pathogen Comments
Bacteria
Legionella spp.
Listeria monocytogenes
Mycoplasma hominis
Mycobacterium tuberculosis
Non-TBMycobacterium spp.
Nocardia spp.
Salmonella spp.
Viruses
Adenovirus
Cytomegalovirus
Epstein-Barr virus
Hepatitis A, B, C, G virus
Herpes simplex virus
Human herpesviruses 6, 7, 8
Influenza virus
Parainfluenza virus
Respiratory syncytial virus
Parvovirus B19
Polyomavirus BK, JC
Varicella zoster virus
Fungi
Aspergillus spp. Use of TMP/SMX prophylaxis has significantly
Blastomyces dermatitidis decreased infections with P. jirovecii.
Coccidioides immitis
Cryptococcus neoformans
Histoplasma capsulatum
Pneumocystis jirovecii
Zygomycetes
Protozoa
Toxoplasma gondii Use of TMP/SMX prophylaxis for P. jirovecii hasalso redcued infections caused by Toxoplasma spp.
CMV infection and disease have significantlydecreased with the use of prophylaxis againstCMV. The same strategy has reduced infectionscaused by HSV and varicella zoster virus. However,late-onset CMV infection after discontinuation ofviral prophylaxis is a concern. Immunization againsthepatitis A and B viruses has reduced suchinfections. Influenza immunization duringfall/winter is recommended.
Use of TMP/SMX prophylaxis for Pneumocystisjirovecii has also reduced infections caused byNocardia spp.

58 0196-4399/00 (see frontmatter) © 2013 Elsevier Clinical Microbiology Newsletter 35:7,2013
the most common fungal pathogen,although mortality is greater with zygo-mycosis, aspergillosis, and cryptococco-sis. The incidence of Candida infectionin SOT has decreased, probably due tothe frequent use of fluconazole prophy-laxis, but there has been an increase ininfections due to non-albicans Candidaspp., notably Candida krusei and Can-dida glabrata, which are often lesssusceptible to fluconazole. P. jiroveciipneumonia is rare with the routine useof TMP/SMX prophylaxis.
Common Infections AfterKidney-Pancreas Transplantion
Simultaneous kidney-pancreastransplantation (SKPT) is increasinglyused in the management of patientswith type 1 diabetes mellitus with end-stage renal disease. The 1-year patient,kidney, and pancreas survival rates are95 to 98%, 92 to 94%, and 78 to 84%,respectively (43). In pancreatic trans-plantation, drainage from the pancreasis diverted into the duodenum (entericdrainage [ED]) or into the urinary blad-der (bladder drainage [BD]) (44). Therisk factors for early infection are relatedto the complexity of the surgical tech-niques and structural and metabolicchanges that occur in the urinary blad-der due to pancreatic secretions. Con-sequently, the early infection-relatedmorbidity is greater among SKPT reci-pients than among KT recipients. Uro-logical problems, including UTIs, arecommon in SKPT recipients with BDcompared to those with ED. In contrast,SKPT recipients with ED have a higherrate of intra-abdominal infections. Intra-abdominal cultures often demonstrate apolymicrobial bacterial flora, includingaerobic Gram-positive and Gram-nega-tive bacteria, anaerobes, and Candidaspp. (45). The clinical approach to sel-ected opportunistic infections, such asCMV and P. jirovecii infections, isgenerally similar to that used for KTrecipients.
Common Infections AfterIntestinal Transplantation
IT is performed as a life-saving pro-cedure for patients with chronic intesti-nal failure who cannot be maintained ontotal parenteral nutrition (46,47). Intest-inal failure may occur as a consequenceof an intestinal calamity (e.g., short-bowel syndrome following volvulus ornecrotizing enterocolitis) or on the basis
of congenital (e.g., intestinal atresia) ormechanical (e.g., pseudo-obstructionsyndrome) problems. Recipients of JTare in the younger age group (48); mostare less than 18 years old. Comparedto other SOTs, relatively few ITs areperformed each year, most in the U.S.Surgical innovations, novel immuno-suppressive regimens, and improvedpost-operative management have ledto 5-year survival rates of more than70% in some institutions. IT may beperformed as an isolated procedure,concomitant with liver allograft, or asa multivisceral (including stomach,duodenum, pancreas, liver, and smallintestine) procedure.
Given the high immunogenicity(high lymphoid tissue content) of thegut, appropriate immunological controlis critical in IT. Excess immunosuppres-sion predisposes to infection, which isthe major cause of death in IT; con-versely suboptimal immunosuppressionleads to acute allograft rejection andpossible graft loss. The consequence ofrejection is a disrupted mucosal barrierthat leads to transgression of microor-ganisms from the intestinal lumen intothe peritoneal cavity, resulting in sepsisand frequently death.
Bacteremia from the gastrointestinalsource is the most frequent infectiouscomplication following IT; it occurs soonafter the procedure or during rejection.As with most gastrointestinal surgeries,intra-abdominal infections, SWIs, anddevice-related bacteremia are common.Pathogens include enteric Gram-nega-tive bacilli, Candida, staphylococci,and streptococci, including enterococci.Aggressive prophylaxis and empirictherapy with broad-spectrum anti-microbials are routine.
Viruses account for up to 60% ofgraft losses. The Herpesvirus family(CMV, HSV, EBV, and human herpes-virus 6) plus adenovirus are the usualpathogens. By far, CMV and EBV areof the greatest concern. During IT, thereis a transfer of a large quantity of lym-photropic CMV in a lymph-rich organinto a profoundly immunocompromisedhost, thereby increasing the potentialfor infection/disease. In D+/R- serodis-cordant transplants, CMV disease tendsto be most severe. Routine surveillancewith CMV PCR and pre-emptive ther-apy with GCV have led to effectiveprevention of CMV infection. EBV
disease, PTLD, EBV enteritis, andhepatitis are mostly seen in seropositivechildren and occur most frequently inmultivisceral transplant recipients. Peri-odic serum EBV DNA measurementsby PCR have become routine in mostcenters; an increasing viral load dic-tates a reduction in immunosuppres-sion. Rituximab, a monoclonal antibodydirected at CD20, may be beneficial inpatients with high EBV PCR and/orPTLD. Antiviral drugs (acyclovir andGCV) and hyperimmune globulin arenot useful.
IT recipients are at high risk forinfection because the transplanted organis rich in lymphoid tissue harboringviruses and the transplanted organ con-tains a large burden of bacteria. Recentadvances include aggressive use ofpotent antimicrobials for perioperativeprophylaxis, novel and effective immuno-suppressive regimens, improved surgicaltechniques, and, above all, availabilityof diagnostic tests for early detection ofviruses to facilitate prompt intervention.
References
1. Starzl, T.E. et al. 1963. Homotrans-plantation of the liver in humans.Surg. Genecol. Obstet. 117:659-676.
2. Alangaden, G.P. et al. 2008. Cumitech45. Infections in solid organ transplantrecipients. Coordinating ed., A.L.Truant. ASM Press, Washington, DC.
3. Kusne, S. et al. 1988. Infections afterliver transplantation: an analysis of 101consecutive cases. Medicine 67:132-143.
4. Chang, F.Y. et al. 1998. Fever in livertransplant recipients: changing spectrumof etiologic agents. Clin. Infect. Dis.26:59-65.
5. Fishman, J. 2007. Infection in solidorgan transplant recipients. N. Engl. J.Med. 357:2601-2614.
6. George, D.L. et al. 1991. Bacterialinfection as a complication of livertransplantation: epidemiology and riskfactors. Rev. Infect. Dis. 13:387-396.
7. Bakir, M. et al. 2001. Epidemiology andclinical consequences of vancomycin-resistant enterococci in liver transplantpatients. Transplantation 72:1032-1037.
8. McNeil, S.A. et al. 2006. Vancomycin-resistant enterococcal colonization andinfection in liver transplant candidatesand recipients: a prospective surveillancestudy. Clin. Infect. Dis. 42:195-203.
9. Paterson, D.L. et al. 2001. Control of anoutbreak of infection due to extended-spectrum beta-lactamase-producingEscherichia coli in a liver transplanta-

tion unit. Clin. Infect. Dis. 33:126-128.
10. Singh, N. et al. 200I. Evolving trends inmultiple antibiotic-resistant bacteria inliver transplant recipients: a longitudinalstudy of antimicrobial susceptibilitypatterns. Liver Transplant. 7:22-26.
11. Riddle D.J. and E.R. Dubberke. 2008.Clostridium difficile infection in solidorgan transplant recipients. Curr. Opin.Organ Transplant. 13:592-600.
12. Peleg, A.Y. et al. 2007. Risk factors,clinical characteristics, and outcome ofNocardia infection in organ transplantrecipients: a matched case-control study.Clin. Infect. Dis. 44:1307-1314.
13. Forbes, G.M. et al. 1990. Nocardiosis inliver transplantation: variation in presen-tation, diagnosis and therapy. J. Infect.20:11-19.
14. Munoz, P., C. Rodriguez, and E. Bouza.2005. Mycobacterium tuberculosis inrecipients of solid organ transplants.Clin. Infect. Dis. 40:581-587.
15. Singh, N. and D. I. Paterson. 1998.Mycobacterium tuberculosis infection insolid-organ transplant recipients: impactand implication for management. Clin.Infect. Dis. 27:1266-1277.
16. Kanj, S.S. et al. 1996. Cytomegalovirusinfection following liver transplantation:review of the literature. Clin. Infect.Dis. 22:537-549.
17. Wiesner, R.H. et al. 2003. Recentadvances in liver transplantation. MayoClinic Proc. 78:197-210.
18. Kalil, A.C. et al. 2005. Meta-analysis:the efficacy of strategies to preventorgan disease by cytomegalovirus insolid organ transplant recipients. Ann.Intern. Med. 143:871- 880.
19. Kusne, S. et al. 1991. Herpes simplexvirus hepatitis after solid organ trans-plantation in adults. J. Infect. Dis.163:1001-1007.
20. Singh, N. et al. 1988. Infections withcytomegalovirus and other herpes vir-uses in 121 liver transplant recipients:transmission by donated organ and theeffect of OKT3 antibodies. J. Infect.Dis. 158:124-131.
21. Samuel, D. et al. 1993. Liver transplan-tation in European patients with thehepatitis B surface antigen. N. Engl. J.Med. 329:1842-1847.
22. Marzano, A. et al. 2001. Prevention ofhepatitis B virus recurrence after livertransplantation in cirrhotic patientstreated with lamivudine and passive
immunoprophylaxis. J. Hepatol. 34:903-910.
23. Fukumoto, T. et al. 1996. Viraldynamics of hepatitis C early afterorthotopic liver transplantations:evidence of rapid turnover of serumvirions. Hepatology 24:1351-1354.
24. Ragni, M.V. et al. 2003. Survival ofhuman immunodeficiency virus-infectedliver transplant recipients. J. Infect. Dis.188:1412-1420.
25. Pappas, P.G. et al. 2010. Invasive fungalinfections among organ transplant recipi-ents in the United States: results of theTransplant-Associated Infection Survei-llance Network (TRANSNET). Clin.Infect. Dis. 50:1101-1111.
26. Collins, L.A. et al. 1994. Risk factorsfor invasive fungal infections complicat-ing orthotopic liver transplantation. J.Infect. Dis. 170:644-652.
27. Singh, N. et al. 2007. Cryptococcusneoformans in organ transplant recipi-ents: impact of calcineurin inhibitoragents on mortality. J. Infect. Dis.195:756-764.
28. Singh, N. et al. 1997. Clinical spectrumof invasive cryptococcosis in liver trans-plant recipients receiving tacrolimus.Clin. Transplant. 11:66-70.
29. Singh, N. et al. 2003. Trends in riskprofiles for and mortality associatedwith invasive aspergillosis among livertransplant recipients. Clin. Infect. Dis.36:46-52.
30. Husain, S. et al. 2003. Opportunisticmycelial fungal infections in organtransplant recipients: emerging impor-tance of non-Aspergillus mycelial fungi.Clin. Infect. Dis. 37:221-229.
31. Rodriguez M. and J.A. Fishman. 2004.Prevention of infection due to Pneumo-cystis spp. in human immunodeficiencyvirus-negative immunocompromisedpatients. Clin. Microbiol. 17:770-782.
32. Thomas, C.F. and A.H. Limper. 2004.Pneumocystis pneumonia. N. Engl. J.Med. 350:2487-2498.
33. Chiche, L. et al. 2003. Post transplantmalaria: first case of transmission ofPlasmodium .falciparum from a whitemultiorgan donor to four recipients.Transplantation 75:166-167.
34. Marty, F.M. and R.H. Rubin. 2006. Theprevention of infection post-transplant:the role of prophylaxis, preemptive andempiric therapy. Transpl. Int. 19:2-11.
35. Schaffner, A. 2001. Pretransplant
evaluation for infections in donors andrecipients of solid organs. Clin. Infect.Dis. 33(Suppl.1):S9-S14.
36. Alangaden, G.J. et al. 2006. Infectiouscomplications after kidney transplanta-tion: current epidemiology and associ-ated risk factors. Clin. Transplant.20:401-409.
37. Avery, R.K. and P. Ljungman. 2001.Prophylactic measures in the solid-organ recipient before transplantation.Clin. Infect. Dis. 33(Suppl.1):S15-S21.
38. Patel, R., 2001. Infections in recipientsof kidney transplants. Infect. Dis. Clin.N. Am. 15:901-953.
39. Hirsch, H.H. et al. 2005. Polyomavirus-associated nephropathy in renal trans-plantation: interdisciplinary analysesand recommendations. Transplantation79:1277-1286.
40. Razonable, R.R. and V.C. Emery. 2004.Management of CMV infection anddisease in transplant patients, 11thAnnu. Meet. IHMF, Herpes Journal11:77-86.
41. Singh, N. 2003. The impact of currenttransplantation practices on the chang-ing epidemiology of infections in trans-plant recipients. Lancet Infect. Dis.3:156-161.
42. Taylor, A.L., R. Marcus, and J.A.Bradley. 2005. Post-transplant lympho-proliferative disorders (PTLD) aftersolid organ transplantation. Crit. Rev.Oncol. Hematol. 56:155-167.
43. Larsen, J.L. 2004. Pancreas transplan-tation: indications and consequences.Endocrinology 25:919-946.
44. Becker, B.N. et al. 2002. Simultaneouspancreas kidney and pancreas transplan-tation. J. Am. Soc. Nephrol. 12:2517-2527.
45. Berger, N. et al. 2006. Infectious com-plications following 72 consecutiveenteric-drained pancreas transplants.Transpl. Int. 19:549-557.
46. Abu-Elmagd, K.M. 2006. Intestinaltransplantation for short bowel syn-drome and gastrointestinal failure:current consensus, rewarding outcomes,and practical guidelines. Gastroenterol-ogy 130(Suppl.1):S132-S137.
47. Grant, D. et al. 2005. Intestine trans-plant registry. Ann. Surg. 241:607-613.
48. Kato, T. et al. 2006. Intestinal and mult-visceral transplantation in children.Ann. Surg. 243:756-766.
Clinical Microbiology Newsletter 35:7,2013 © 2013 Elsevier 0196-4399/00 (see frontmatter) 59