Embed Size (px)
Citation preview
Independent Health Facilities
Clinical Practice Parameters and Facility Standards
Magnetic Resonance Imaging & Computed Tomography
3rdth Edition – October 2015
The College of Physicians and Surgeons of Ontario
Vision Statement
Quality Professionals, Healthy System, Public Trust
Our Mandate
Build and maintain an effective system of self-governance.
The profession, through and with the College, has a duty to serve and protect the public interest by regulating the practice of the profession and governing in accordance with the Regulated Health Professions Act.
Our Vision Defined
Quality Professionals, Healthy System, Public Trust.
Our new vision is the framework by which we organize ourselves.
It guides our thinking and actions into the future. It defines not only who we are, but what we stand for, the role we see for ourselves, our critical relationships, in what system we work, and the outcomes we seek.
Each component of our vision is defined below:
Quality Professionals – as a profession and as professionals, we recognize and acknowledge our role and responsibility in attaining at a personal, professional, and at a system-level, the best possible patient outcomes.
We are committed to developing and maintaining professional competencies, taking a leadership position on critical issues that impact the performance of the system, and actively partner to provide tools, resources, measurement, to ensure the optimal performance at all levels of the system.
Healthy System – the trust and confidence of the public and our effectiveness as professionals is influenced by the system within which we operate. Therefore, we, as caring professionals, are actively involved in the design and function of an effective system including:
• accessibility • the interdependence of all involved • measurements and outcomes • continued sustainability
Public Trust – as individual doctors garner the trust of their patients, as a profession we must aim to have the trust of the public by:
• building positive relationships with individuals • acting in the interests of patients and communities • advocating for our patients and a quality system

Our Guiding Principles
Integrity, accountability, leadership and cooperation.
The public, through legislation, has empowered the profession to regulate itself through the College.
Central to the practice of medicine is the physician-patient relationship and the support of healthy communities. As the physician has responsibility to the patient, the profession has the responsibility to serve the public through the health-care system.
To fulfill our vision of quality professionals, healthy system, public trust we will work to enhance the health of the public guided by professional competence and the following principles:
Integrity – in what we do and how we go about fulfilling our core mandate: • Coherent alignment of goals, behaviours and outcomes;
• Steadfast adherence to a high ethical standard.
Accountability to the public and profession – we will achieve this through: • An attitude of service;
• Accepting responsibility;
• Transparency of process;
• Dedicated to improvement.
Leadership – leading by proactively regulating our profession, managing risk and serving the public.
Cooperation – seeking out and working with our partners – other health-care institutions, associations and medical schools, etc. – to ensure collaborative commitment, focus and shared resources for the common good of the profession and public.

Independent Health Facilities
Clinical Practice Parameters and Facility Standards
Magnetic Resonance Imaging & Computed Tomography
3rd Edition –October 2015

First Edition, January 2003: Members of the MRI & CT Task Force: Dr. George Lougheed, Chair Barrie Dr. Ian Cunningham London Dr. Richard Drost London Dr. Michael Fung Peterborough Dr. Pat Garces Timmins Dr. Barry Hobbs London Dr. Amit Mehta St. Catharines Dr. Mitesh Mehta Toronto Dr. Mark Prieditis Scarborough Dr. Lisa Thain London Ms Joy Craighead Toronto Mr. Mark Lepp Brampton Ms Marlene McCarthy Collingwood
Second Edition, May 2009 Members of the MRI & CT Task Force: Dr. Paul Voorheis, Chair Barrie Dr. Pat Garces Oakville Dr. Alex Hartman Toronto Ms Joan Hatcher Niagara Falls Dr. Erik Jurriaans Jersyville Ms Marlene McCarthy Collingwood Dr. Mark Prieditis Toronto Dr. Lalitha Shankar Toronto
Third Edition, October 2015 Members of the MRI & CT Task Force: Dr. Paul Voorheis, Chair Barrie Mr. Jeff Frimeth Toronto Dr. Anish Kirpalani Toronto Dr. Martin O’Malley Toronto Dr. Mark Prieditis Toronto Dr. Lalitha Shankar Toronto Ms Elizabeth Staten St. Catharines
Published and distributed by the College of Physicians and Surgeons of Ontario. For more information about the Independent Health Facilities program, contact:
Wade Hillier Director, Quality Management Division The College of Physicians and Surgeons of Ontario 80 College Street Toronto, Ontario M5G 2E2 Toll free (800) 268-7096 (416) 967-2600 ext. 636 Email: [email protected]

Table of Contents
Preface i
Purpose of Clinical Practice Parameters ...................................................................................... i
Role of the College of Physicians and Surgeons .......................................................................... i
Responsibilities of the College .................................................................................................... ii
Updating this Document ............................................................................................................. ii
Radiology Guiding Principles ...................................................................................................... iii
VOLUME 1 FACILITY STANDARDS ................................................................................... 1
Chapter 1 Staffing a Facility ...................................................................................... 1
Overview .................................................................................................................................... 1
Qualifications of Physicians MRI & CT ....................................................................................... 1
Qualifications for Radiologists who have not been in active practice in either MRI and/or CT 2
Continuing Professional Development ...................................................................................... 3
MRI/CT Director ......................................................................................................................... 3
Quality Advisor ........................................................................................................................... 4
Medical Physicist – CT and/or MRI ............................................................................................ 5
Radiation Protection Officer (RPO) for CT ................................................................................. 6
Medical Radiation Technologists (MR) ...................................................................................... 6
Medical Radiation Technologists CT .......................................................................................... 7
Injection Certification ................................................................................................................ 8
Chapter 2 Facilities, Equipment and Supplies ......................................................... 11
Overview .................................................................................................................................. 11
Facilities, Equipment and Supplies .......................................................................................... 11
Imaging Equipment for CT/MRI ............................................................................................... 11
Quality Control for CT .............................................................................................................. 12
Quality Control for MRI ............................................................................................................ 14
Safety Concerns and Resuscitation Equipment ....................................................................... 15
Administration of Medications in Imaging Department .......................................................... 16
Emergency Procedures ............................................................................................................ 18
Chapter 3 Developing Policies and Procedures ....................................................... 19
Overview .................................................................................................................................. 19
Developing Policies and Procedures ........................................................................................ 19
Infection Control ...................................................................................................................... 21
Respiratory Infections .............................................................................................................. 21
PHIPA ........................................................................................................................................ 21
Radiation Safety and Dose Reduction (ALARA Principles) ....................................................... 21
Chapter 4 Requesting and Reporting Mechanisms .................................................. 23
Overview .................................................................................................................................. 23
Requesting Procedures ............................................................................................................ 23
The Diagnostic Imaging Final Written Report .......................................................................... 24
Charges for Copying Patient Records (As Per MOHLTC Fact Sheet) ........................................ 29
Retrieval of Films from another IHF/Institution ...................................................................... 29
Chapter 5 Providing Quality Care ........................................................................... 31
Overview .................................................................................................................................. 31
Quality Management Program Goals ...................................................................................... 31
Providing Quality Care ............................................................................................................. 31
Components of a Quality Management Program.................................................................... 32
Monitoring the Program .......................................................................................................... 33
VOLUME 2 CLINICAL PRACTICE PARAMETERS................................................................ 35
CAR Practice Guidelines for Magnetic Resonance Imaging ..................................................... 37
CAR Standards for Computed Tomography ............................................................................. 37
CAR Guidelines for Test Appropriateness ................................................................................ 37
Ministry of Health and Long-Term Care, Wait Time Targets for MRI/CT Scans ...................... 37
VOLUME 3 TELERADIOLOGY (PACS) .............................................................................. 39
CPSO Telemedicine Policy ........................................................................................................ 40
CAR Standards for Teleradiology ............................................................................................. 40
OAR Teleradiology Practice Standard ...................................................................................... 40
APPENDICES FOR MRI/CT AND GENERAL GUIDANCE
Appendix I ACR Guidance Document on MR Safe Practices: 2013 ............................ 49
Appendix II MR Safety ............................................................................................. 80
Appendix V Sample Emergency Safety Policy .......................................................... 110
Appendix VI Requirement for MRI/CT Priority Protocol ............................................ 112
Appendix VII Prevention of IV Contrast Reaction Protocol ............................................ 113
Appendix VIII Independent Health Facilities Act - Ontario Regulation 57/92 ............... 115
Quality Advisor and Advisory Committee .............................................................................. 115
Standards ............................................................................................................................... 116
Records of Employees ............................................................................................................ 116
Patient Records ...................................................................................................................... 117
Books and Accounts ............................................................................................................... 118
Notices ................................................................................................................................... 119
Miscellaneous ........................................................................................................................ 119
Appendix IX Sample Patient Survey: Quality of Care ....................................... 121
Appendix X Sample Referring Physician Survey-Independent Health Facilities Program ............................................................................................. 123

Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition i
Preface The Independent Health Facilities Act (IHFA), proclaimed in April 1990, and amended in 1996 and 1998, gives the College of Physicians and Surgeons of Ontario the primary responsibility for carrying out quality assessments in Independent Health Facilities. These non-hospital facilities may provide some of the following insured services:
• in diagnostic facilities: radiology, ultrasound, magnetic resonance imaging, computed tomography, positron emission tomography (PET), nuclear medicine, pulmonary function, and sleep studies
• in treatment or surgical facilities: one or more of a variety of procedures in peripheral vascular disease, plastic surgery, obstetrics and gynaecology, dermatology, nephrology, ophthalmology, and their related anaesthetic services and perhaps other specialties.
The College of Physicians and Surgeons of Ontario has a legislative mandate under the Act to perform quality assessment and inspection functions. This responsibility, and others set out by agreement with the Ministry of Health and Long-Term Care, contribute to the College achieving its goals as stated in the College’s Mission Statement. An important goal of the College is to promote activities which will improve the level of quality of care by the majority of physicians. The Independent Health Facilities program helps reach this goal by developing and implementing explicit clinical practice parameters and facility standards for the delivery of medical services in Ontario, assessing the quality of care provided to patients, and as a result, promotes continuous quality improvement.
Purpose of Clinical Practice Parameters The Independent Health Facilities clinical practice parameters and facility standards are designed to assist physicians in their clinical decision-making by providing a framework for assessing and treating clinical conditions commonly cared for by a variety of specialties. The primary purpose of this document is to assist physicians in developing their own quality management program and act as a guide for assessing the quality of patient care provided in the facilities.
Note: The parameters and standards are not intended to either replace a physician’s clinical judgment or to establish a protocol for all patients with a particular condition. It is understood that some patients will not fit the clinical conditions contemplated by certain parameters and that a particular parameter will rarely be the only appropriate approach to a patient’s condition.
In developing these clinical practice parameters, the objective is to create a range of appropriate options for given clinical situations, based on the available research data and the best professional consensus. The product, therefore, should not be thought of as being “cast in stone”, but rather subject to individual, clinically significant patient differences.
Role of the College of Physicians and Surgeons The College adopted the role of a facilitator for the development of clinical practice parameters and facility standards. Representatives of national specialty societies and sections of the Ontario Medical Association, and individuals with acknowledged skill, experience and expertise formed specialty-specific Task Forces.
All Clinical Practice Parameters and Facility Standards undergo an external review process.
ii The College of Physicians and Surgeons of Ontario
External Reviewers Include: Registrars of other regulatory colleges, department heads at relevant academic institutions, relevant national and provincial organizations, independent health facilities, IHF assessors and other stakeholders as determined by the relevant Task Force.
Task Force members ensure that: • clinical practice parameters must be based on the appropriate mix of current, scientifically-
reliable information from research literature, clinical experience and professional consensus. • any parameter-setting exercise must be done exclusively from the quality perspective. That
may well mean that some of the conclusions reached could add to medical care costs. • parameters have to be flexible enough to allow for a range of appropriate options and need to
take into account the variations in practice realities from urban to rural areas. • parameters need to be developed by consensus and consultation with the profession at large. • parameters should provide support and assistance to physicians without boxing them in with
“cookbook formulas.” • parameters will need to be regularly updated based on appropriate research studies. • parameters should reduce uncertainty for physicians and improve their clinical decision-
making. • information on practice parameters must be widely distributed to ensure that all physicians
benefit from this knowledge.
Responsibilities of the College Responsibilities of the College include:
• assessing the quality of care when requested by the Ministry. The College will maintain a roster of physicians, nurses, technologists and others to serve as inspectors and assessors as required.
• inspecting the illegal charging of facility fees by unlicensed facilities when requested by the Ministry.
• monitoring service results in facilities. The College’s information system will monitor individual and facility outcome performance. This is a unique feature of the legislation, which for the first time in North America, requires facility operators to establish and maintain a system to ensure the monitoring of the results of the service or services provided in a facility.
• providing education and assisting facilities so that they may continually improve the services they provide to patients. The College will work with and assist physicians in these facilities so that they can develop their own quality management programs based on the parameters and standards, monitor facility performance by conducting quality assessments, work with facilities to continually improve patient services, assist in resolving issues and conducting reassessments as necessary.
Updating this Document These parameters and standards are subject to periodic review, and amendments in the form of replacement pages may be issued from time to time. Such pages will be mailed automatically to all relevant independent health facilities. It is planned to issue new editions of the parameters and standards at intervals not greater than five years. The external review process will be repeated to validate the new parameters as they are developed.
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition iii
Radiology Guiding Principles Extracted from the first edition (February 1995) of Clinical Practice Parameters and Facility Standards for Diagnostic Imaging,
A diagnostic imaging practice is a consultative physician service rendered by qualified specialists who have completed an accredited residency program in diagnostic radiology which includes using all modalities in the imaging portrayal of human morphology and physiological principles in medical diagnosis.
The elements of radiologic consultation include:
• pre-examination evaluation by a referring physician. • a request for radiologic consultation. The requisition includes pertinent clinical findings, a
working diagnosis, and signature of referring physician or other qualified professional. • a safe patient environment in which the radiologist supervises a qualified staff whose efforts
are directed at producing a radiologic examination yielding maximum diagnostic information and consistent with the least possible exposure to radiation.
Diagnostic imaging is a patient care specialty and it is an important function of the radiologist to advise referring physicians about the best sequence of examinations for resolving a clinical problem expeditiously and with the least risk and cost.
It is not possible to establish a “minimum” or “optimum” standard of care. Guiding principles and attributes for appropriate care in diagnostic imaging can be summarized as follows:
• examinations and procedures are performed with the greatest benefit and least risk to the patient.
• examinations and procedures are interpreted with the highest degree of competence using all available information including comparison with previous examinations and procedures.
• examination/procedure findings and conclusions are communicated promptly and expeditiously to the referring physician.
• referring physicians are consulted in order to select and perform only the most useful examinations/procedures.
• flow of data including storage, retrieval, and general handling of images, diagnostic data, and reports are managed efficiently.
• patient services provided are considerate of the human side of care as well as the purely technical component of care.
• patient services are managed so that productivity is maintained and optimal use of available resources is assured.
These principles should constitute the basis for the evaluation of desirable and undesirable practice patterns.


Independent Health Facilities Clinical Practice Parameters and Facility Standards: Magnetic Resonance Imaging & Computed Tomography
VOLUME 1 FACILITY STANDARDS

Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd Edition 1
Chapter 1 Staffing a Facility
Overview Each licensee in consultation with the Quality Advisor (QA) ensures:
• Diagnostic imaging services are provided by qualified imaging physicians and technologists.
• There is a current written plan describing the organization of the facility and its services.
• There are sufficient numbers of qualified physicians, technologists, and clerical personnel available to meet the stated goals and objectives.
• That the duties and responsibilities of all diagnostic imaging service staff are specified in job descriptions. They are kept up to date and on site.
• Quality Advisors, Physicians, Technologists and Licensees review their legal obligations and may consider obtaining professional liability insurance as there is potential for liability issues in IHFs.
• Staff obtains education in Workplace Hazardous Materials Information System (WHMIS) which is documented and maintained on site for future review at the time of Ministry of Labour (MOL) inspections.
• A radiologist or designated physician with current Advanced Cardiac Life Support (ACLS) certification is personally and immediately available. Documentation regarding ACLS certification is maintained on site.
• At least one staff member with current Basic Cardiac Life Support (BCLS) certification is on site at all times during hours of scanner operation. Documentation regarding BCLS certification is maintained on site. It is expected that the training includes being certified in both theory and hands-on components. To identify training courses contact the Heart and Stroke Foundation of Ontario and/or St. John Ambulance.
Qualifications of Physicians MRI & CT Physicians performing or interpreting Magnetic Resonance Imaging (MRI) and Computed Tomography examinations are:
• Certified in Diagnostic Radiology with the Royal College of Physicians and Surgeons of Canada and have a certificate of registration to practice in Ontario.
OR
• Have a restricted certificate of Registration to practice independently. Documentation must be available to demonstrate full compliance with any terms, condition or limitations of their registration with the CPSO, including any supervision requirement or scope of practice definition.
And for MRI • Have demonstrated competence (6 months of MRI training, 1500 reported cases) in an
appropriate facility and under the full-time supervision of a radiologist fully trained in MRI as per the description of an MRI Director.
2 The College of Physicians and Surgeons of Ontario
Appropriate training centres for radiologists seeking to obtain the required MRI credentials are:
• An academic centre with a diagnostic radiology residency program OR • A hospital MRI facility in Canada under the supervision of the MRI Director.
Note: Where training occurs at a hospital MRI centre not associated with a University centre, the training should also include at least 160 hours of training through ACCME, RCPSC-recognized CME courses or equivalent (a full range of MRI clinical applications as well as MRI physics, instrumentation, QA and safety) within 2 years prior to start of practice.
A letter signed by the MRI Director attesting to the training outlining what specific anatomy they are trained to interpret for all MRI Radiologists, including the Director, will be required. This letter should be kept on file at the facility.
Note: For the following, “MRI Radiologist” means a radiologist satisfying the above criteria.
And for CT • Have demonstrated competence (6 months of CT training with 1500 reported cases) in an
appropriate facility and under the full-time supervision of a radiologist fully trained in CT as per the description of a CT Director.
Appropriate training centres for radiologists seeking to obtain the required CT credentials are:
• An academic centre with a diagnostic radiology residency program OR • A hospital CT facility in Canada under the supervision of the CT Director.
Note: Where training occurs at a hospital CT center not associated with a university center, the training should also include at least 160 hours of training through ACCME, RCPSC – recognized CME courses or equivalent (a full range of clinical applications of CT as well as CT physics, instrumentation, QA and radiation safety) within 2 years prior to start of practice.
A letter signed by the CT Director Attesting to the training outlining what specific anatomy they are trained to interpret for all CT Radiologists, including the CT Director, will be required. This letter should be kept on file at the facility.
Note: For the following, “CT Radiologist” means a radiologist satisfying the above criteria.
Qualifications for Radiologists who have not been in active practice in either MRI and/or CT MRI and/or CT Radiologists who have not been in active practice of MRI and/or CT (i.e. performing less than 100 patient cases/year) or who have not actively provided MRI and/or CT services for two years or more but were fully trained in the past will require re-training at an appropriate MRI and/or CT facility as described earlier in this section. A minimum of one month of re-training at an appropriate MRI and/or CT facility will include reporting a minimum 300 patient cases, with an appropriate case mix, under the direct supervision of a qualified MRI and/or CT Director-level radiologist. A letter from the preceptor, attesting to competence, must be presented to the MRI and/or CT Director and kept on file by the licensed facility.
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 3
Under certain very specific situations, it may be appropriate for a highly specialized organ system based radiologist to interpret MRI (CT) studies limited to their sub-specialty despite not obtaining the minimum number of cases described above. Examples of this include Breast MRI or Abdominal/Body imaging. In this situation, training and limitations should be documented and approved by the MRI (CT) director and the MRI (CT) cases interpreted should be limited to the area of expertise.
Continuing Professional Development All physicians attend Continuing Professional Development (CPD) programs relevant to their practice, which comply with their Royal College requirements for maintenance of certification. Documentation of annual CPD in MRI/CT-related courses taken by every radiologist providing MRI/CT medical services must be submitted to the MRI Director no later than the end of each calendar year.
MRI/CT Director Each licensed facility has an MRI/CT Radiologist who is appointed as the MRI/CT Director (note: This position can be individual physicians or a dual role). The MRI/CT Director shall have demonstrated competence (one year of MRI/CT training) and would be qualified to provide additional on-site training to the other MRI/CT radiologists in the licensed facility.
Every MRI/CT Director shall:
• Be physically present at the IHF on a regular basis, on average at least 8 hours per week. The MRI/CT Director or a designated MRI/CT Radiologist should be available by phone for consultation at any time when services are provided and documented.
• Ensure that safe MRI/CT practice guidelines are established and maintained as current and appropriate for the facility.
• Consult with the facility staff after any serious MRI/CT safety incidents and, as a minimum, update the MRI/CT safety guidelines on a yearly basis.
• Approve and review all MRI protocols performed by the licensed facility at least annually, or as often as may be deemed necessary by the MRI Director. All requisitions will be assigned a specific protocol by an MRI radiologist associated with the facility prior to the study being performed. Changes to the assigned protocol can only be modified by the MRI Director or another designated MRI Radiologist.
• Approve and annually review all CT imaging protocols performed by the licensed facility including use of contrast, CT safety and radiation exposure as outlined in the Report of the Diagnostic Imaging Safety Committee for Computed Tomography (CT) – February 2007 by the Ministry of Health and Long-Term Care (see Appendix III). All requisitions will be assigned a specific protocol by a CT radiologist associated with the facility prior to the study being performed. Changes to the assigned protocol can only be modified by the CT Director or another designated CT Radiologist.
Note: MRI/CT Director can also be the Quality Advisor.
4 The College of Physicians and Surgeons of Ontario
Quality Advisor The Quality Advisor (QA) must be a physician licensed to practice in Ontario by the College of Physicians and Surgeons of Ontario and meet the qualifications as outlined above.
The Quality Advisor must submit the Notice of Appointment of Quality Advisor and Quality Advisor Acknowledgement forms to the Director, IHF. These forms are available at http://www.health.gov.on.ca/en/public/programs/ihf/forms.aspx
Role of the Quality Advisor The role of the Quality Advisor is an important one. Quality Advisors play a vital role in the overall operation of the IHF to ensure that the services provided to patients are being conducted appropriately and safely.
Each IHF licensee is responsible for operating the facility and providing services in accordance with the requirements of the IHFA. Pursuant to O. Reg. 57/92 under the Independent Health Facilities Act (see Appendix VII), “every licensee is required to appoint a Quality Advisor to advise the licensee with respect to the quality and standards of services provided in the IHF. The Quality Advisor must be a health professional who ordinarily provides insured services in or in connection with the facility and whose training enables him or her to advise the licensee with respect to the quality and standards of services provided in the facility.”
Note: The term “Health Professional” as referenced in the IHFA, refers to a physician.
Responsibilities of the Quality Advisor The Quality Advisor is responsible for advising the licensee with respect to the quality and standards of services provided. In order to fulfill this duty the Quality Advisor:
• Shall personally attend the facility at least twice each year, and may attend more frequently, where in the opinion of the Quality Advisor it is necessary based on the volume and types of services provided in the facility. The visits may be coordinated as part of the Quality Advisory Committee (QA Committee) meetings.
• Shall document all visits to the facility made in connection with the Quality Advisor’s role. • Shall ensure that a qualified physician be available for consultation during the facility’s hours of
operation. • Shall seek advice from other health professionals where in the opinion of the Quality Advisor it
is necessary to ensure that all aspects of the services provided in the facility are provided in accordance with generally accepted professional standards and provide such advice to the licensee.
• Shall chair the QA Committee. The QA Committee shall meet at least twice a year if the facility employs more than six full-time staff equivalents including the Quality Advisor; otherwise the QA Committee shall meet at least once a year. Regular agenda items should include: review of cases; policies and procedures; quality control matters on equipment; incidents; medical and technical issues.
• Shall ensure all QA Committee meetings are documented. • Obtain copies of assessment reports from the licensee/owner/operator. If deficiencies were
identified in the assessment, the Quality Advisor shall review same with the QA Committee and document such review. The Quality Advisor’s signature is required on any written plan submitted by the licensee to the College.
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 5
The Quality Advisor shall advise the licensee on the implementation of an ongoing Quality Management (QM) Program, which should include but not be limited to, the following:
• Ensuring ongoing and preventive equipment maintenance • Follow-up of interesting cases • Follow-up patient and/or medical and technical staff incidents • Continuing education for medical and technical staff • Ensuring certificates of registration, BCLS, etc. are current • Regular medical and technical staff performance appraisals • Patient and referring physician satisfaction surveys.
The Quality Advisor will advise the licensee, and document the provision of such advice, in connection with the following:
• Health professional staff hiring decisions, in order to ensure that potential candidates have the appropriate knowledge, skill and competency required to provide the types of services provided in the facility.
• Continuing education for all health professional staff members employed in the facility, as may be required by their respective regulatory Colleges or associations.
• Appropriate certification for all health professional staff members employed in the facility with the respective regulatory College or associations.
• Leadership, as may be required to address and resolve any care-related disputes that may arise between patients and health professional staff.
• Appropriate resources for health professional staff members employed in the facility. • Formal performance appraisals for all health professional staff. • Technology used in the facility, in order to ensure it meets the current standard(s) and is
maintained through a service program to deliver optimal performance. • Establishment and/or updating of medical policies and procedures for the facility, e.g.
consultation requests, performance protocols, infection control, and standardized reports, and other issues as may be appropriate.
• Equipment and other purchases as may be related to patient care. • Issues or concerns identified by any staff member, if related to conditions within the facility
that may affect the quality of any aspect of patient care. • Establishing and/or updating system(s) for monitoring the results of the service(s) provided in
the facility.
If the Quality Advisor has reasonable grounds to believe the licensee is not complying with the licensee’s obligation to ensure that services are being provided in accordance with the generally accepted standards and to ensure that the persons who provide services in the facility are qualified to provide those services, the Quality Advisor must inform the Director of Independent Health Facilities forthwith in accordance with the provisions and Regulations under the IHFA.
Medical Physicist – CT and/or MRI The medical physicist must have appropriate training in CT and/or MRI. A medical physicist has the responsibility for the initial acceptance testing of equipment and related systems/components and for implementing and overseeing routine quality control testing of the MRI and/or CT scanner. The medical physicist may repeat the acceptance test after any major hardware upgrades or major service incidents and failures (see Chapter 2, Quality Control).
6 The College of Physicians and Surgeons of Ontario
The medical physicist must either be:
• Board certified in Diagnostic Radiology by the Canadian College of Physicists in Medicine (for CT or MRI testing)
• Board certified in Magnetic Resonance Imaging by the Canadian College of Physicists in Medicine (for MRI testing only)
• Board certified in Diagnostic Medical Physics by the American Board of Radiology • Board certified in Magnetic Resonance Imaging by the American Board of Medical Physics, or • If the medical physicist does not have board certification, the following qualifications must be
met: o Graduate degree in medical physics, radiologic physics, physics, or other relevant
physical science or engineering discipline from an accredited institution o Formal coursework in the biological sciences with at least one course in
biology/radiation biology, one course in anatomy and physiology, and three years of documented clinical experience in a CT and/or MR environment
A copy of the physicist’s credentials should be kept on file at the facility.
Radiation Protection Officer (RPO) for CT According to the HARP Act, a Radiation Protection Officer (RPO) must be designated for the facility. This role may be assumed or designated by the Quality Advisor.
http://www.ontario.ca/laws/statute/90h02
The OAR has recently published a paper outlining the roles and responsibilities of the RPO. http://www.oar.info/pdf/OAR_RPO_DUTIES_2011.pdf
Medical Radiation Technologists (MR) In Ontario, Medical Radiation Technologists (MRTs) are self-regulated professionals. They must practice in accordance with the applicable provincial legislation, the Medical Radiation Technology Act (MRTA) and the College of Medical Radiation Technologists of Ontario (CMRTO) standards of practice.
Medical Radiation Technologists have a current and valid certificate of registration with the College of Medical Radiation Technologists of Ontario in the specialty of magnetic resonance imaging. Certification in MRI must be documented, and be of the designation MRT(MR).
All technologists must maintain and document current Basic Cardiac Life Support (BCLS) certification.
Continuing Medical Education Medical Radiation Technologists attend and document their attendance at relevant continuing medical education programs, as mandated by the CMRTO, or as identified by the MRI Director. This documentation must be provided to the MRI Director annually no later than at the end of the calendar year.
Charge Technologist Qualifications The designation of a Charge Technologist is mandatory. Their qualifications must include:
• Current and valid certificate of registration with the College of Medical Radiation Technologists
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 7
of Ontario (CMRTO) in the specialty of magnetic resonance imaging. • Should have 4 years full-time MRI experience. • Certificate in BCLS with recertification yearly.
Charge Technologist Responsibilities The Charge Technologist is current with changing technical trends in MRI by attending conferences, meetings, or other CME, and reading current relevant literature.
Documentation of CME is maintained.
Charge Technologists are responsible for the day-to-day operation of the MRI suite, including:
• Training of all technologists to include Quality Control, MRI safety, injections, policies and procedures
• Reporting to/advising the MRI Director/Quality Advisor • Advising the Quality Advisor that all technologists are current with all qualifications and CME
requirements • Ensuring that all support staff receive and implement MRI safety guidelines • Inputting site-specific protocols into the MRI unit • Writing and updating MRI policy and procedure manual on at least an annual basis • Ensuring implementation of policies and procedures • Maintaining records of equipment calibration, maintenance, and repair procedures • Maintaining copies of test observations and reports • Ensuring that safety policies and the equipment and facilities necessary for their
implementation are in place and in working order • Implementing infection control measures • Maintaining all necessary facility supplies • Performing and documenting Quality Control procedures • Responsible for supervising the technologists for injection certification. The MRI/Quality
Advisor certifies the technologist.
Medical Radiation Technologists CT In Ontario, Medical Radiation Technologists (MRTs) are self-regulated professionals. They must practice in accordance with the applicable provincial legislation, the Medical Radiation Technology Act (MRTA) and the College of Medical Radiation Technologists of Ontario (CMRTO) standards of practice.
Medical Radiation Technologists have a current and valid certificate of registration with the College of Medical Radiation Technologists of Ontario (CMRTO).
Technologists have completed cross sectional anatomy of the brain, neck and body similar to the CT Certification Course at Michener or equivalent.
All technologists must maintain and document current Basic Cardiac Life Support (BCLS) certification.
Continuing Medical Education CT Technologists attend and document their attendance at relevant continuing medical education programs, as mandated by the CMRTO, or as identified by the CT Director. This documentation must be provided to the CT Director annually no later than at the end of the calendar year.
8 The College of Physicians and Surgeons of Ontario
Charge Technologist Qualifications The designation of a Charge Technologist is mandatory. Their qualifications must include:
• Current and valid certificate of registration with the College of Medical Radiation Technologists of Ontario (CMRTO).
• Should have 4 years full-time CT experience • Certificate in BCLS with recertification yearly.
Charge Technologists have completed an injection course and are certified by a Radiologist as per facility policy. Their qualifications should also include 4 years of full-time CT experience consistent with the scope of practice at the facility.
Charge Technologist Responsibilities The Charge Technologist is current with changing technical trends in CT by attending conferences, meetings, or other CME, and reading current relevant literature.
Documentation of CME is maintained.
Charge Technologists are responsible for the day-to-day operation of the CT suite, including:
• Training of all technologists to include Quality Control, radiation safety, injections, policies and procedures
• Reporting to/advising the CT Director/Quality Advisor • Advising the Quality Advisor that all technologists are current with all qualifications and CME
requirements • Ensuring that all support staff receive and implement CT safety guidelines • Inputting site-specific protocols into the CT unit • Writing and updating CT policy and procedure manual on at least an annual basis • Ensuring implementation of policies and procedures • Maintaining records of equipment calibration, maintenance, and repair procedures • Maintaining copies of test observations and reports • Ensuring that safety policies and the equipment and facilities necessary for their
implementation are in place and in working order • Implementing infection control measures • Maintaining all necessary facility supplies • Performing and documenting Quality Control procedures • Responsible for supervising the technologists for injection certification. The CT Quality Advisor
certifies the technologist.
Injection Certification The Charge Technologist is responsible for supervising the technologist/regulated health care professional at the facility who performs injections. The Quality Advisor or the Director of CT/MRI certifies the technologist to be competent for the IHF.
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 9
For IV contrast injection at a CT/MRI facility, the licensee is responsible for the following:
• All technologists/regulated health care professionals are responsible for completion of the venipuncture/injection certification course from an accredited program, which include but are not limited to the following:
http://michener.ca/ce_course/venipuncture-techniques
https://www.humber.ca
http://www.cvaa.info/
• The technologist should provide the certificate to the IHF facility.
• The charge technologist is responsible for supervising the technologist following completion of IV injection training course.
• The CT/MR director or Quality advisor of the IHF facility will approve and document the competence of the technologist for IV injection.
• Observation of the technologist and recommendation where necessary by CT/MRI director.
• Review of all policies with the CT/MRI technologist regarding the contrast injection (patient consent, contraindication, contrast reaction, premedication, sterile techniques and needle disposal and facility standards)
• Annual refresher for contrast injections at the discretion of the QA and CT/MRI director.

10 The College of Physicians and Surgeons of Ontario
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 11
Chapter 2 Facilities, Equipment and Supplies
Overview The facility has adequate space, equipment and supplies for the safe and efficient performance of diagnostic imaging services.
Facilities, Equipment and Supplies Facilities have sufficient space to meet workload requirements and ensure the effective care and privacy of patients.
Appropriate safety precautions are maintained and documented against electrical, mechanical and radiation hazards as well as against fire and explosion, so that personnel and patients are not endangered.
The thermoluminescent dosimeter (TLD) monitoring service of the Personnel Dosimetry Services of Health Canada, Bureau of Radiation and Medical Devices, is used and documented to ensure the safety of personnel. Records are posted in the facility for staff information.
For CT, pregnancy warning signs are posted in the waiting area, change rooms and examination rooms.
Basic supplies for infection prevention and control is on site and used appropriately as per current provincial guidelines/policies. Resources are available through the Provincial Infectious Diseases Advisory Committee of Public Health Ontario at http://www.publichealthontario.ca/en/BrowseByTopic/InfectiousDiseases/PIDAC/Pages/Infection-Prevention-and-Control-for-Clinical-Office-Practice.aspx
If headphones are available to MRI patients, they must be disinfected after each use, otherwise disposable ear plugs should be offered.
An area must be provided for patients’ valuables/personal belongings to be secured/locked during procedures.
Facility monitoring equipment and procedures are appropriate to the documented patient mix and procedures.
Imaging Equipment for CT/MRI
Computed Tomography For patient imaging, the CT scanner meets or exceeds the following specifications:
• New when installed in the facility and manufactured within 6 months prior to installation and has at least a 64-row detector array
• Use of software and hardware to manage patient doses, in line with the ALARA principle, including, but not limited to automatic tube current modulation
• Power injector: the injector shall be pressure limited and have adjustable rate and volume
12 The College of Physicians and Surgeons of Ontario
• Must pass all quality control tests at the time of installation as outlined by organizations such as the American Association of Physicists in Medicine (AAPM), the American College of Radiology (ACR), or Health Canada Safety Code 35.
Note: The lifespan of CT equipment is no longer than 8-12 years, depending on utilization, and is normally expected to be 10 years based on expected mid-range utilization as defined in the CAR guidelines referenced below. Replacement equipment should be purchased as brand new equipment under the same conditions as new equipment
• Reference: Lifecycle Guidance for Medical Imaging Equipment in Canada 2013, Canadian Association of Radiologists (http://www.car.ca/en/standards-guidelines.aspx)
• Additional software upgrades are in accordance with the scope of practice being provided within the facility.
• A clear upgrade pathway, defined to keep the software and hardware technology current, will be implemented by the facility.
A vendor approved Original Equipment Manufacturer (OEM) service contract which includes hardware and software will exist for its lifespan.
Note: The Ministry of Health and Long-Term Care must give approval to install and operate a CT scanner under the Healing Arts Radiation Protection Act (HARP Act) R.S.O. 1990, c.H.2 clauses 23(2)(a) and (b). Under section 3 of the HARP Act, the written approval of the Director of X-ray Safety is required for CT equipment to be installed.
CT Layout When seated at the console, CT technologist should have a direct view of the patient. If this is not the case, then a closed television camera/monitor is installed to provide this view of the patient.
Requirements of the HARP Act and Regulations must be fulfilled.
Quality Control for CT All safety measures are in compliance with federal and provincial laws/regulations (HARP Act or equivalent). All equipment is properly maintained and calibrated during scheduled preventive maintenance sessions in accordance with manufacturer specifications. Written records of preventive maintenance, repairs, and unscheduled down time are maintained. The following Quality Control schedule is recommended:
Daily: The site is asked to perform the following tests which follow the ACR CT Accreditation program requirements
a) Water CT Number and Standard Deviation b) Artifact Evaluation
Monthly: The site is asked to perform the following tests which follow the ACR CT Accreditation program requirements
a) Visual Checklist b) Display Monitor QC
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 13
Annually: The site is asked to perform the following tests which follow the ACR CT Accreditation program requirements
a) Review of Clinical Protocols b) Scout Prescription and Alignment Light Accuracy c) Image Thickness d) Table Travel Accuracy e) Radiation Beam Width f) Low-Contrast Performance g) Spatial Resolution h) CT Number Accuracy i) Artifact Evaluation j) CT Number Uniformity k) Dosimetry l) Gray Level Performance of CT Acquisition Display Monitors A CT “protocol” refers to the settings and parameters that are used to acquire images for a specific examination (e.g. Abdominal/Pelvic CT) based on the clinical information provided. The CT protocols will determine image quality and dose. Each IHF must maintain a copy of CT protocols based on common clinical indications. Guidance on the development of CT scan protocols should be provided by the vendor, the CT Director and a medical physicist, as appropriate. Suggested CT scan protocols have been published by the AAPM (American Association of Physicists in Medicine).
Reference: American Association of Physicists in Medicine; CT Protocols (http://www.aapm.org)
In the event of major hardware upgrades or service repairs being performed (e.g. tube replacement or detector module replacement), it is not required, but it is recommended to have the medical physicist repeat the acceptance tests. Magnetic Resonance Imaging The minimum strength of the primary magnet must be 1.5 Tesla. The MRI system should be equipped with the appropriate gradient hardware, radio frequency hardware (receiver channels), phased array coils, and software packages for the case mix. A power injector is required.
For patient imaging, the MRI system meets or exceeds the following specifications:
• New when installed in the facility and manufactured within 12 months prior to installation with current technology.
Note: The lifespan of MRI equipment is no longer than 8-12 years, depending on utilization, and is normally expected to be 10 years based on expected mid-range utilization as defined in the CAR guidelines referenced below. Replacement equipment should be purchased as brand new equipment under the same conditions as new equipment
• Reference: Lifecycle Guidance for Medical Imaging Equipment in Canada 2013, Canadian Association of Radiologists (http://www.car.ca/en/standards-guidelines.aspx
• A clear upgrade pathway, defined to keep the technology current, will be implemented by the facility.
14 The College of Physicians and Surgeons of Ontario
Note: A vendor approved OEM service contract which includes hardware and software will exist for its lifespan
In recognition of changing technology standards, machines need to be upgradeable to future state-of-the-art requirements.
• The MRI scanner must pass all quality assurance tests at the time of installation as outlined by organizations such as the American Association of Physicists in Medicine (AAPM) or the American College of Radiology (ACR).
Quality Control for MRI All equipment is properly maintained and calibrated during scheduled preventive maintenance sessions in accordance with manufacturer specifications. Written records of preventive maintenance, repairs, and unscheduled down time are maintained. A daily record of both the MRI magnet room and equipment room temperature, humidity, primary chilled water temperature, secondary water temperature, and the magnet helium level (where appropriate) are documented. While documentation by the technologist of the facility’s Quality Control program is required, the following Quality Control schedule is recommended:
Weekly: The site is asked to perform the following tests, which follow the ACR MRI Accreditation Program Requirements
a) Table positioning, setup and scanning, laser alignment b) Centre frequency c) Transmitter gain or attenuation d) Geometric accuracy e) High contrast spatial resolution f) Low contrast detectability g) Artifact evaluation h) Visual checklist i) Slice thickness accuracy j) Magnetic field uniformity k) Slice position accuracy
Annually: The medical physicist performs the complete system acceptance test with the ACR Test Phantom (or equivalent). The required tests are:
a) Table positioning, setup and scanning, laser alignment b) Centre frequency c) Transmitter gain or attenuation d) Geometric accuracy e) High contrast spatial resolution f) Low contrast detectability g) Artifact evaluation h) Visual checklist i) Percent signal ghosting (PSG) j) Image intensity uniformity (PIU) k) Magnetic field homogeneity l) Slice position accuracy m) Slice thickness accuracy n) RF coil checks
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 15
o) Soft copy (monitor) QC
In addition, the medical physicist must perform an assessment of the site’s own MR Safety Program.
After any service work/repairs the service engineer runs the calibrations/ service tests as appropriate for the specific hardware serviced.
Safety Concerns and Resuscitation Equipment The licensee shall reference the ACR Guidance Document on MR Safe Practices: 2013 (J Magnetic Resonance Imaging 2013, 37:501–530) for all MRI safety practice guidelines (see Appendix I).
Patient monitoring equipment and facilities for cardiopulmonary resuscitation including vital signs monitoring, support equipment and an emergency crash cart are immediately available. Radiologists, technologists, and staff members are able to assist with procedures, patient monitoring and support. A written policy is in place for dealing with emergency procedures such as cardiopulmonary arrest.
The facility has alternate materials available for patients with known or suspected latex allergies.
Contrast-enhanced studies require the presence of a physician who is trained and experienced in the recognition and management of adverse effects of these agents and other life threatening events. If this physician is not the CT/MRI Radiologist, then he/she must also have appropriate training and experience in CT/MRI safety. Technologists are trained in resuscitation (BCLS). IHFs must have an emergency protocol in place to deal with these types of emergencies.
Reference: ACR Manual on Contrast Media, Version 9 (http://www.acr.org/quality-safety/resources/contrast-manual) – see Appendix VI)
As pediatric patients receive contrast, specific paediatric doses/drugs and paediatric resuscitation equipment are clearly labeled and colour coded for age groups.
Facilities provide a means of moving patients in difficulty to an adjacent area, which is equipped to handle any adverse reactions up to and including respiratory and cardiac arrest.
MRI Layout The MRI facility layout must give the MRI technologist an unimpeded view of the magnet room entrance door when seated at the operating console. Access is restricted to all areas within the 5 gauss magnetic field line of the MRI magnet. The magnet room itself usually encompasses this area.
Ideally the MRI technologist has a direct view of the patient down the bore of the magnet when seated at the operating console. If this is not the case then a closed television camera/monitor is installed to provide this view of the patient to the MRI technologist.
16 The College of Physicians and Surgeons of Ontario
MRI Safety Zones All MRI facility layouts in Ontario must comply with and incorporate the four (4) recognized MRI Safety Zones as outlined in Appendix I.
The purpose of establishing MRI Safety Zones is to minimize potential risks to patients and staff within the MRI environment. There are four zones in total and each one is defined as follows:
a) Zone I: areas freely accessible to the general public; typically is outside the MRI environment and is the area where individuals can access the MRI environment.
b) Zone II: area where patients are greeted/screened and not allowed to move freely (only under MRI personnel supervision).
c) Zone III: access is strictly restricted and regions within it (e.g. Zone IV) are controlled/supervised by MR personnel.
d) Zone IV: the MRI scanner room (within Zone III) and the magnet’s associated magnetic fringe fields.
All zones must be labelled in the facility.
The MRI Director should designate individuals in the MRI environment as either MRI personnel or non-MR personnel. MR personnel are broken down into Level 1 and Level 2 personnel. Level 1 personnel are individuals who have passed minimal safety educational efforts to ensure their own safety within Zone III. Level 2 personnel are individuals who have received more extensive training in MR safety (e.g. issues in thermal burns). Non-MRI personnel constitute everyone else in the MRI environment.
Non-MRI personnel must be screened prior to entering Zone III.
It is recommended to use ferromagnetic detection systems as a supplement to screening of persons and devices approaching Zone IV.
Patients must remove all readily removable metallic personal belongings and devices as well as fill out a safety screening questionnaire.
If patients/non-MRI personnel have a history of potential ferromagnetic foreign object penetration, they must undergo further investigation (e.g. CT, radiograph).
All ferrous objects should be Zone III restricted (whenever practical). A handheld magnet can help to determine if there is significant ferromagnetism in objects. All objects/devices to be taken into Zone IV are either MR Safe or not MR Safe. MR Safe is defined as objects which present no attractive forces present and its composition is known to be non-magnetic. Non-MR safe objects present grossly detectable attractive forces. They may be taken into Zone III if they are deemed necessary and appropriate for patient care (under MR personnel supervision).
Administration of Medications in Imaging Department • It is reasonable to assume some medications may be given to maximize the information
obtained from CT and MR images (e.g. anxiolytics, beta blockers, nitroglycerin, antiperistaltic agents). In order to safely administer drugs in an IHF, there must be medical directives in place which include, but are not limited to: drug dosage, route of administration, and management of adverse events related to the various medications.
• Patients under the age of 18 requiring sedation are not to be examined in an IHF
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 17
Resuscitative and Monitoring Equipment Required for Both CT and MRI Appropriate emergency equipment and medications must be immediately available to treat adverse reactions associated with the administration of contrast media. It is recommended that for each site a plan of action and formulary be developed in consultation with local anaesthetists and internal medicine specialists responsible for their hospital arrest teams. Appropriate emergency equipment and medications, as noted below, must be immediately available to treat adverse reactions associated with the administration of contrast media. Protocols for the contact of Emergency Medical Services (EMS) and patient transfer to a hospital should be published, posted and regularly reviewed.
Emergency equipment and Formulary as per ACLS standards, includes but is not limited to:
• ECG monitor • Defibrillator • Oxygen source with mask and suction • Oxygen saturation monitor • Resuscitation drugs • Stethoscope • Sphygmomanometer • IV pole • Wheelchair • Stretcher • Laryngoscope and endotracheal tubes (sized for adults and children) • Oropharyngeal airways (sized for adults and children) • Ambu bag or equivalent (sized for adults and children)
The contents of the resuscitation tray are checked monthly for expiry dates on all drugs and sterile equipment. These activities are documented and kept with the resuscitation equipment. MRI Safe Equipment
The following MRI safe equipment is available:
• Stretcher (if scanner table is not detachable) • Wheelchair • IV poles • Laundry hamper • Step stool • All oxygen tanks must be MRI safe
If a parent is expected to accompany and stay inside the magnet room with their child, then a MR safe chair is provided for inside the magnet room.
All facility fire extinguishers that may be brought into the magnet room during a fire emergency are MR safe. The fire alarm must be audible inside the magnet room.
There should be a small, portable, strong (usually rare earth) magnet available to the MRI technologist to test whether objects are ferromagnetic. [For example, Lee Valley, product number 50K02.01]
A MR safe step ladder (usually aluminum) should be provided for changing light bulbs inside the MRI magnet room. This task should be performed by an individual trained in MR safety.
18 The College of Physicians and Surgeons of Ontario
Emergency Procedures All resuscitations are performed outside the scanner room.
For MRI the biggest danger is the introduction of ferromagnetic objects into the magnet room by the responding staff and the resulting projectile motion of the ferromagnetic objects toward the centre of the magnet causing injury/death to anyone intersecting the projectile trajectory.
Although it is possible to set up a complete emergency response trolley and equipment which is MR safe, it is almost impossible to ensure that all staff who may respond to the emergency will not carry any ferromagnetic objects into the magnet room.
Ambulance, fire or police crews who respond to an emergency call will be carrying ferromagnetic objects. For these reasons, it is imperative that the first response to a patient code inside the magnet is for the MRI technologist(s) to remove the patient from the magnet room.
CT/MRI Facilities provide a means of moving patients in difficulty outside the magnet room to an area equipped to handle any adverse reactions up to and including respiratory and cardiac arrest.
Any interventions and resuscitative procedures MUST take place outside the magnet room. No additional personnel or equipment will enter the magnet room.
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 19
Chapter 3 Developing Policies and Procedures
Overview Current written policies and procedures are required to provide staff with clear direction on the scope and limitations of their functions and responsibilities to patient care.
Developing Policies and Procedures The procedure manual is available for consultation by all facility staff. The manual is reviewed annually, revised as necessary, and dated to indicate the time of the last review or revision.
There is documentation to indicate who makes the policies, sets the standards, and who supervises physicians, technologists, and other staff.
Procedures in the manual include, but are not limited to, the following: Facility
• Scope and limitations of diagnostic imaging services provided by the facility. • Patient-booking systems. • Documentation of and method for receiving written referrals for consultation.
Facility Staff
• Delegated acts and medical directives. Refer to CPSO policy on Delegation of Controlled Act: http://www.cpso.on.ca/Policies-Publications/Policy/Delegation-of-Controlled-Acts.
• Safety training for medical and non-medical staff. • Certification for administration of contrast injections.
Records and Communication/Reporting & Privacy Principles • Methods for preliminary interpretations and/or telephone calls of reports, and for the
subsequent written interpretation of images by qualified diagnostic imaging physicians. • Maintenance of requisitions, imaging media and interpretation reports (See Appendix VII,
Independent Health Facilities Act-Ontario Regulation 57/92 -Amended to O.Reg. 14/95). • Confidentiality. • Patient consent, written or verbal, based on the scope of practice in the facility and in
accordance with the Health Care Consent Act.
Diagnostic Services • Instructions regarding routine preparation of patients. • Imaging protocols detailing the sequences involved in examining a target organ for both adult
and pediatric patients. For CT these include but are not limited to: o Oral contrast –volume and type o IV contrast –volume and rate and type of administration o Scanning region and length
20 The College of Physicians and Surgeons of Ontario
o Patient Position o Detector Configuration o Reconstructed Slice thickness o Reconstruction Algorithm o Scan type o Rotation time o mAs and kVp o Pitch o Displayed CTDIvol o Pediatric/small adult protocols preprogrammed in scanner with reduced specific organ
patient dose. o Contraindications for performing tests.
• Screening just prior to patient entering the magnet room. • Adult sedation. • Family member/ support person in the room. • Performance of additional views and examinations- any additional views or examinations are
identified in the imaging report with reasons. • Use of protective devices. • Pre-medication for known contrast allergy. • Assessment of renal function where appropriate prior to contrast injection.
Equipment Maintenance • Maintenance work inside the magnet room. • Routine maintenance and calibration of equipment.
Emergency Procedures and Safety Policies
• Ensuring patients who have taken oral or sublingual anxiolytics/antihistamines are provided discharge instructions and are accompanied by a person prior to departing the facility.
• Techniques for managing patients with claustrophobia, anxiety and emotional distress. • Managing patients with possible or definite ferrous/metallic foreign bodies (particularly
intracranial and intraocular locations). • Response to fire alarm and fire within the magnet room.
o When personnel are present in the facility o When personnel are not present in the facility. o Inadvertent magnet quenches.
• Pregnancy of patients or facility staff. • Infection control. • Specific first aid measures to be followed and documented in the event of an adverse health
effect, including a description of the arrangements for transferring patients to an acute care facility when required.
• Emergency resuscitation for MR only to occur outside the magnet room.
Quality Management Program Refer to Chapter #5
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 21
Infection Control Routine practices to prevent infection are in keeping with provincial guidelines. Resources are available through the Provincial Infectious Diseases Advisory Committee of Public Health Ontario at http://www.publichealthontario.ca/en/BrowseByTopic/InfectiousDiseases/PIDAC/Pages/Infection-Prevention-and-Control-for-Clinical-Office-Practice.aspx
At Risk Patients The facility must identify patients who have any possibility of transmission of infection at the front desk. Hand Hygiene It is recommended to post the Ministry of Health “Hand-washing Techniques” document for IHF staff and patients in designated areas.
Personal Protective Equipment Gloves, masks, gowns and eye- protection equipment must be used where and when necessary to protect both patient and personnel. Needle Safety Under the Occupational Health and Safety Act, the Needle Safety section states, “when a worker is to do work requiring use of a hollow-bore needle, the employer shall provide the worker with a safety-engineered needle that is appropriate for the work. O.Reg. 474/07, s.3(1)”. Therefore IHFs shall provide appropriate access to safety-engineered needles as required.
Respiratory Infections Each facility should implement a written protocol to manage all patients with potentially infectious respiratory conditions.
PHIPA The independent health facility is expected to implement the various privacy procedures and policies to maintain patient information confidentiality within the organization. The organization must respect all laws that apply to it, including laws relating to privacy, confidentiality, security of records and access to records, including the Personal Health Information Protection Act, 2004.
Information and Privacy Commissioner/Ontario, Suite 1400, 2 Bloor Street East, Toronto, ON M4W 1A8 https://www.ipc.on.ca
Radiation Safety and Dose Reduction (ALARA Principles) The ALARA principle (As Low As Reasonably Achievable) must be considered for all examinations using ionizing radiation to minimize radiation exposure to the patient and staff.
22 The College of Physicians and Surgeons of Ontario
Pre-programmed protocols should be available for infant, child and youth (small, medium and large by weight for each) and also organ specific.
Low dose CT protocols should be designed to minimize the dose based on the clinical indication (e.g. low dose CT protocol for renal colic), without sacrificing the image quality necessary to make a diagnosis.
Note: Refer to the Report of the Diagnostic Imaging Safety Committee for Computed Tomography (CT) –February 2007 by the Ministry of Health and Long-Term Care (see Appendix III).
Policies and procedures should be developed under the direction of the radiation protection officer (RPO) to ensure compliance with the HARP Act and other applicable legislation.

Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 23
Chapter 4 Requesting and Reporting Mechanisms
Overview
The content of this overview has been extracted from the CAR Standard for Communication of Diagnostic Imaging Findings (2010) (www.car.ca)
Communication is a critical component of the art and science of medicine and is especially important in Diagnostic Imaging. It is incumbent upon radiologists and the facilities in which they work to ensure that the results of diagnostic studies are communicated promptly and accurately in order to optimize patient care.
The final product of any consultation is the submission of a report on the results of the consultation. In addition, the radiologist and the ordering physician have many opportunities to communicate directly with each other during the course of a patient’s case management. Such communication should be encouraged because it leads to more effective and appropriate utilization of Diagnostic Imaging services and it can enhance the diagnostic yield of the study in question. From a utilization standpoint, discussions with the referring team will help to focus attention on such concerns as radiation exposure, appropriate imaging studies, clinical efficacy and cost-effective examinations. The provision of a well- defined clinical question and the overall clinical context can improve interpretation of complete cases and may enable the radiologist to streamline the diagnostic impression into a few likely and relevant differential considerations rather than providing a textbook list of possible differential diagnoses that may be of less utility and of less impact.
These principles apply to all radiology consultations irrespective of the technology used including teleradiology, Picture Archiving & Communication Systems (PACS) or an equivalent electronic work station with an archival system refer to Volume # Teleradiology (PACS).
In order to afford optimal care to the patient and enhance the cost-effectiveness of each diagnostic examination, radiological consultations should be provided and images interpreted within a known clinical setting. No screening radiological examination should be performed unless evidence-based or part of an organized population-based screening program.
The Canadian Association of Radiologists (CAR) supports radiologists who insist on clinical data with each consultation request and the IHF Task Force supports this same principle.
All communication should be performed in a manner that respects patient confidentiality. Medical images and reports constitute confidential patient information and must be treated accordingly. It is incumbent upon IHF staff and all imaging personnel including radiologists to ensure patient privacy. This includes institution of appropriate privacy procedures, and appropriate policies and procedures for release of images or reports from medical images to third parties.
Requesting Procedures Written requisitions and forms to screen the patient for CT/MRI compatibility must be completed by the referring physician. All CT/MRI requests must be approved and prioritized by a radiologist prior to booking the test.
24 The College of Physicians and Surgeons of Ontario
The technologist rescreens just prior to the patient entering the magnet room. (for sample screening forms, see Appendix II)
Overview An appropriate request for all radiological consultations is the responsibility of the referring physician and specifies:
• The basic demographic information of the patient such as name, health number, date of birth, and sex.
• The name of the ordering physician/healthcare provider and the names of any other physicians who are to receive copies of the report.
Note: If patient information is entered electronically, clinic staff must ensure that the patient demographic information including the requesting physician noted on the requisition is current and correct. Any changes to update the information must be made prior to the performance of the study.
• The type of procedure requested for the patient including any special instructions where applicable.
• Pertinent clinical information including indications, pertinent history, and provisional diagnosis.
Note: This is the responsibility of the ordering physician/healthcare provider. If a patient arrives with a requisition containing incomplete information, the diagnostic imaging physician or designated staff member should attempt to contact the ordering physician/healthcare provider or interview the patient to obtain the necessary information prior to conducting the procedure.
• Whether a “stat report” is required.
It is recommended that patients be provided written information about computed tomography/magnetic resonance imaging procedures prior to an appointment. Technologist Identification Technologists must be identified at the time of the examination in order for the interpreting physician to identify the technologist performing the examination.
The Diagnostic Imaging Final Written Report The final report is considered to be the definitive means of communicating to the ordering physician or other healthcare professionals the results of an imaging examination or procedure. Additional methods of communication of results are necessary in certain situations.
The final report should be transmitted to the ordering physician or healthcare professional who is responsible for the clinical follow-up. The ordering physician or other healthcare professional also shares in the responsibility of obtaining the results of imaging studies he or she has ordered.
The timelines of reporting any imaging examination varies with the nature and urgency of the clinical problem. The written final report should be made available to the ordering physician/healthcare provider within 24 hours if possible.
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 25
The final report should be proofread carefully to avoid typographical errors, accidentally deleted words, and confusing or conflicting statements, and should be authenticated by the reporting radiologist, whenever possible.
Note: Given the complexity of CT and MRI studies in general, compared to other modalities, it is strongly recommended that the final report should be proofread and verified by the reporting radiologist
Electronic and rubber-stamp signature devices, instead of a written signature, are acceptable if access to them is secure. In any case, the name of the dictating radiologist must appear as such on the report.
A copy of the diagnostic image is retained as the permanent record for the appropriate length of time as prescribed by regulations.
If there was a significant discrepancy between the preliminary report and the final report, this should be documented and the referring physician notified of the change in cases where they change may alter immediate patient management.
Voice recognition systems are widely employed to facilitate timely reporting. These systems are not foolproof and methods should be in place to allow detection and correction of program generated errors.
Final reports may be transmitted by paper, fax, and email, provided appropriate security measures are in place. Facilities should seriously consider instituting “read receipt” mechanisms to identify any report that has not been picked up by the ordering physician/healthcare provider.
A copy of the final report should be archived by the imaging facility as part of the patient’s medical record (paper or electronic) and be retrievable for future reference. It is of sufficient quality to record permanent findings, to be used for comparison with subsequent examinations, and enable third party radiologists to confirm the diagnosis.
The IHF must have the ability to retrieve and/or produce a copy of the image(s) stored within one working day of the request as required.
The imaging media and reports are filed using an accepted coding system which allows films and reports to be retrieved by patient identification information.
Unusual and interesting examinations are maintained for educational purposes in accordance with the IHF Regulations.
Previous stored diagnostic images are available for the interpreting physician. Report Attributes Reports of the interpretation of imaging procedures include the following:
• Name of the patient and another identifier such as birth date, pertinent identification number or office identification number.
• The facility or location where the study was conducted. • Name of the ordering physician. • Name of most responsible physician for patients cared for by multiple clinical services.
26 The College of Physicians and Surgeons of Ontario
Rationale: To provide more accurate routing of the report to one or more locations specified by the ordering physician. Each facility has a policy to ensure proper distribution of the written report to the most responsible physician and/or other physicians/healthcare professionals.
• Name or type of examination. • Dates of examination.
Whenever possible, the month should be spelled rather than risking the ambiguity of American and international formats (e.g. 03 July 2010 rather than 03/07/10 or 07/03/10.
• Dates of dictation.
Rationale: Quality Control
Body of the Report The effective transmission of imaging information from the radiologists to the ordering physician/healthcare provider constitutes the main purpose of the report.
The report should be clear and concise. Normal or unequivocally positive reports can be short and precise. Whenever indicated the report includes:
Procedures and Materials A description of the examinations and/or procedures performed and any contrast media (including agent, concentration, volume and route of administration, where applicable), medications, catheters, or devices if not reported elsewhere. Any known significant patient reaction or complication should be recorded.
Rationale: To ensure accurate communication and availability of the information for future reference.
Findings Use precise anatomical, radiological and pathological terminology to describe the findings accurately. Abbreviations should be avoided to avoid ambiguity and risk of miscommunication, unless initially spelled out. Limitations Where appropriate, identify factors that can limit the sensitivity and specificity of the examination. Such factors might include technical factors, patient anatomy (e.g. dense breast pattern,) and limitations of the technique (e.g. the low sensitivity of a chest x-ray for pulmonary embolism). Clinical Issues The clinical history, indication or clinical question may be inserted at the beginning of the report. While not mandatory this practice is encouraged.
Note: It is strongly recommended that clinical history, indication or clinical question be included in the final report under a separate heading.
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 27
The report should address or answer any pertinent clinical issues raised in the request for the imaging examination. If there are factors that prevent answering the clinical question, these should be stated.
For example, to rule out pneumothorax, state “there is no evidence of pneumothorax” or to rule out fracture, state “there is no evidence of fracture”. It is not appropriate to use universal disclaimers such as “the mammography examination does not exclude the possibility of cancer” as it is expected that the ordering physician understands that even a well performed diagnostic exam does not necessarily have a 100% sensitivity. Descriptive reporting that offers no opinion, or guidance for resolution of the clinical question should be avoided.
Comparative Data Comparisons with previous examinations and reports, when possible, are part of an imaging consultation and report, and should be included in the body of the report and/or conclusion section when appropriate.
Note: It is strongly recommended that comparative data be included in the final report under a separate heading.
Assessment and Recommendations The report should conclude with an interpretive commentary on the data described. The proper terminology for ending the report may include the following terms: conclusion, impression, interpretation, opinion, diagnosis or reading.
Each examination should contain such an interpretive commentary. Exceptions can be made when the study is being compared with other recent studies and no changes have occurred during the interval or the body of the report is very brief and a separate conclusion would be a redundant repetition of the body of the report.
• Give a precise diagnosis whenever possible. • Give a differential diagnosis when appropriate. • Recommend follow-up and/or additional diagnostic imaging studies to clarify to confirm the
conclusion, only when appropriate. • Any significant patient reaction should be reported.
Standardized computer-generated template reports (or other structured report formats) that satisfy the above criteria are considered acceptable.
Note: It is strongly recommended that conclusion, impression, interpretation, or opinion be included in the final report under a separate heading.
28 The College of Physicians and Surgeons of Ontario
Preliminary Report A preliminary report may precede the final report in certain circumstances and contains limited information relevant to immediate patient management. It may be time sensitive and should not be expected to contain all the imaging findings. It should be generated when a timely communication is necessary in unexpected elective cases where clinical urgency mandates immediate communication of the results. It is acknowledged that not all serious findings require a preliminary report if they are already known or could have been reasonably expected by the referring physician (e.g. bowel cancer on a barium enema) as long as the final report is generated within 24-48 hours.
A preliminary report may not have the benefit of prior imaging studies and/or reports and may be based upon incomplete information due to evolving clinical circumstances which may compromise its accuracy. Preliminary reports may be communicated verbally, in writing or electronically and this communication should be documented. Preliminary communications should be reproduced into a permanent format as soon as practical and appropriately labeled as a preliminary report, distinct from the final report.
Note: Technologists are not permitted to provide preliminary findings of any examination either directly to the patient and/or the ordering physician without first consulting the radiologist. The radiologist must then decide, based on the preliminary findings who will convey the information to the ordering physician.
Verbal or Other Direct Communication Radiologists should attempt to co-ordinate their efforts with those of the ordering physician in order to best serve the patient’s well-being. In some circumstances, such co-ordination may require direct communication of unusual, unexpected or urgent findings to the ordering physician in advance of the formal written report. These include:
• The detection of conditions carrying the risk of acute morbidity and/or mortality which may require immediate case management decisions.
• The detection of disease sufficiently serious that it may require prompt notification of the patient, clinical evaluation or initiation of treatment.
• Detection of life or limb threatening abnormalities which might not have been anticipated by the referring physician.
• Any clinically significant discrepancy between an emergency or preliminary report and the final written report should be promptly reconciled by direct communication to the ordering physician or his/her representative.
In these circumstances, the radiologist or his/her representative, should attempt to communicate directly (in person or by telephone) with the ordering physician or his/her representative. Alternative methods including fax, text messaging or email could be used for these purposes if there is a way of verifying receipt of the reports. The timeliness of direct communication should be based upon the immediacy of the clinical situation.
Documentation of the actual or attempted direct communication may be a desirable facility policy.
• It is incumbent upon ordering physicians/healthcare professionals to make available a way of communicating results to an alternative provider in circumstances such as holiday, sickness or restricted office hours.
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 29
Charges for Copying Patient Records (As Per MOHLTC Fact Sheet) http://www.health.gov.on.ca/en/public/programs/ihf/fact_sheets.aspx
If an individual requires a copy of all or any part of his/her patient record, which may include imaging media, for the provision of ongoing care by another health care provider, the IHF must provide a copy of the record(s) at no cost/charge to the patient or health care provider.
When the patient attends an IHF to obtain a copy of their images and reports for their ongoing care/treatment the acceptable turnaround time for requests that are received by the IHF for the images and reports to be made available for courier or pick-up is within 3 working days of receiving the request.
Retrieval of Films from another IHF/Institution When previous images and reports are required from another IHF in order to make a comparison, the acceptable turnaround time for requests that are received by the IHF would be for the images and reports to be made available for courier or pickup within 3 working days of receiving the request. Based on the above turnaround time couriered images and reports must be received by the requesting party within a maximum of 5 working days of the IHF receiving the original request.

30 The College of Physicians and Surgeons of Ontario
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 31
Chapter 5 Providing Quality Care
Overview A Quality Advisory Committee is established as per the IHF Act (See Appendix VIII). The QA Committee shall consist of health professionals who provide health services in or in connection with the independent health facility and must be chaired by the Quality Advisor. Regular meetings are held and minutes maintained (IHF Act Regulation 57/92).
The requirements for and responsibilities of the Quality Advisor (QA) are detailed in Chapter 1, Staffing a Facility.
The QA Committee shall meet at least twice a year if the facility employs more than six full time staff equivalents including the Quality Advisor, otherwise the QA Committee shall meet at least once a year. Regular agenda items may include but not be limited to: review of cases; policies and procedures; QC matters on equipment, incidents, staffing issues.
All QA Committee meetings shall be documented.
Records are to be kept of the:
o Minutes of the quality advisory committee. o Minutes of general staff meetings.
The Committee is to supervise creation and maintenance of a quality management program adequate to reach the goals detailed below.
The goals, procedures and protocols for the quality management program of the facility are written and included in the policy and procedure manual.
Quality Management Program Goals The goals of the program include but are not limited to ensuring that:
• The services planned and provided are consistent with the patient’s needs and assure diagnostic reliability and patient safety.
• Services conducted in the facility are safe. • Services conducted are appropriate to the problem(s) being investigated. • The performance of diagnostic radiological examinations comply with current Canadian
Association Radiologists (CAR) Guidelines accepted by the College of Physician and Surgeons of Ontario and in the absence of current standards and guidelines generally accepted medical standards of practice.
Providing Quality Care The performance of CT/ MRI examinations complies with standards accepted by the College of Physicians and Surgeons of Ontario as described in the Clinical Practice Parameters section.
A designated CT/MRI Radiologist is available for consultation with the technologist on a case-by-case basis. For cases requiring monitoring, ideally, the CT/MRI Radiologist is on-site and available to participate in the examination when required.
32 The College of Physicians and Surgeons of Ontario
Although optimally a designated CT/ MRI Radiologist is present for all cases, this is not always possible. For cases that do not require monitoring a designated CT/MRI Radiologist should always be available by phone to consult with the technologist and referring physician.
Whenever contrast is administered, a designated physician must be personally and immediately available. There must be adequate equipment/medications available to treat an adverse reaction.
A CT/MRI-trained radiologist should visit the facility on a regular basis to review imaging procedures and provide technologist supervision. Ideally there should be a CT/MRI radiologist present at the facility on a daily basis. Even in remote sites, a CT/MRI-trained radiologist should be on site at least one day per week. A daily log of visits to the facility by the radiologist should be maintained.
Diagnostic imaging procedures are carried out in a manner in which patient privacy is respected.
Components of a Quality Management Program The facility establishes and maintains a system to monitor the results of the services provided.
The facility establishes a quality management program appropriate for its size, volume and types of services provided. It is recognized that quality management programs will vary depending on the facility size, scope of practice, and geographical considerations. Quality Management Program activities are documented and maintained on-site.
To ensure that the goals of the Quality Management Program are met the Committee’s tasks include but are not limited to:
• Review quality management goals and objectives annually. • Supervise and document a systematic ongoing review of the facility policy and procedures
manual. • Review safety data on any equipment new to the facility since the last meeting, and ensure that
all equipment in the facility meets safety standards. • Review any incident or accident report since the last meeting and document any such actions to
prevent similar incidents or accidents. Provide a report of all such proceedings to the facility’s Quality Advisor.
• Recommendations from other assessing bodies such as the Ministry of Health X-ray Inspection Services and HARP.
• Supervise and document a program of annual performance reviews for all staff who have patient contact, including documentation of action taken to correct any significant deficiencies in performance.
• Ensure registration certificates, BCLS certificates, etc. are current. • Review the CPD activities of the technical and medical staff. • Promote the discussion of interesting/challenging cases seen at the facility and disseminate any
teaching points to the staff for educational purposes. • Review results of regular surveys of patient, referring physician and staff satisfaction,
documenting actions to address any suggestions, problems, or issues raised. • Compliance with quality assurance protocols as appropriate. • Assessing the accuracy of interpretations and the appropriateness of procedures process. • The IHF will have established a physician peer review program and provide a description of the
process of how this is done. http://www.car.ca/uploads/standards%20guidelines/20120831_EN_Peer-Review.pdf

Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 33
• Staff participation in planning strategies to overcome any deficiencies and to continually improve the services provided to patients.
Monitoring the Program To monitor the program the QA committee shall be comprised of a minimum of 2 health professionals who provide health services in or in connection with the IHF, including at least one physician and at least one technologist.
Recommendations from the QA Committee shall be circulated to all staff as minutes of the meeting once they are finalized. These recommendations shall be reviewed at a general staff meeting including all healthcare professionals who provide services in or in connection with the IHF. Quorum for such meetings shall be 2 or 50% of the staff whichever is greater. Staff members who cannot attend are to review and sign off on the minutes of that meeting.

34 The College of Physicians and Surgeons of Ontario
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd Edition 35
Independent Health Facilities Clinical Practice Parameters and Facility Standards: Magnetic Resonance Imaging & Computed Tomography VOLUME 2 CLINICAL PRACTICE PARAMETERS
36 The College of Physicians and Surgeons of Ontario
Position Statement from the IHF Diagnostic Imaging Task Force
It is the position of the IHF Diagnostic Imaging Task Force that the revised (2015) Clinical Practice Parameters and Facility Standards will contain a list of CAR/ACR standards that are applicable to the services provided in Independent Health Facilities.
To ensure that Radiologists and Facilities are in compliance with current CAR/ACR Standards, the radiologist and facility staff are responsible for, at least annually, reviewing the Canadian Association of Radiologists website www.car.ca to ensure that they have obtained and are in compliance with the most current standards of practice for the profession.
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 37
CAR Practice Guidelines for Magnetic Resonance Imaging CAR Practice Guidelines for Magnetic Resonance Imaging http://www.car.ca/uploads/standards%20guidelines/20110428_en_standard_magnetic_resonance.pdf
CAR Practice Guidelines for Breast Imaging & Intervention http://www.car.ca/uploads/standards%20guidelines/20131024_en_breast_imaging_practice_guidelines.pdf
CAR Standards for Computed Tomography CAR Practice Guidelines for Cardiac Computed Tomography http://www.car.ca/uploads/standards%20guidelines/GSCCT_Guidelines_Standards_Cardiac_CT_EN.pdf
CAR Practice Guidelines for Consensus Training Standards for Cardiac CT http://www.car.ca/uploads/standards%20guidelines/standard_car_ccs_train_cardiacct_en.pdf
CAR Practice Guidelines for CT Colonoscopy http://www.car.ca/uploads/standards%20guidelines/201001_CAR_CTC_Standards_EN.pdf
CAR Practice Guidelines for Prevention of Contrast Induced Nephropathy http://www.car.ca/uploads/standards%20guidelines/20110617_en_prevention_cin.pdf
CAR Guidelines for Test Appropriateness http://www.car.ca/en/standards-guidelines/guidelines.aspx
Ministry of Health and Long-Term Care, Wait Time Targets for MRI/CT Scans http://www.health.gov.on.ca/en/pro/programs/waittimes/surgery/target.aspx

38 The College of Physicians and Surgeons of Ontario
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd Edition 39
Independent Health Facilities Clinical Practice Parameters and Facility Standards: Magnetic Resonance Imaging & Computed Tomography VOLUME 3 TELERADIOLOGY (PACS)
40 The College of Physicians and Surgeons of Ontario
CPSO Telemedicine Policy http://www.cpso.on.ca/CPSO/media/documents/Policies/Policy-Items/Telemedicine.pdf?ext=.pdf
CAR Standards for Teleradiology http://www.car.ca/uploads/standards%20guidelines/Standard_Teleradiology_EN.pdf
OAR Teleradiology Practice Standard
May 2015 OAR TELERADIOLOGY PRACTICE STANDARD Amended May 2013 Originally Approved June 2007 Definition Teleradiology in Ontario is the electronic transmission of radiographic images from one geographical location to another for the purposes of interpretation and consultation by diagnostic imaging physicians accredited by the Royal College of Physicians and Surgeons of Canada (or recognized equivalent) and licensed by the College of Physicians and Surgeons of Ontario. These guidelines and standards have been developed to protect patients and ensure their data is kept confidential. Teleradiology services are to facilitate patient care and are not intended to be a cost-cutting measure, which may jeopardize patient safety and the standards of health care. Preface The transmission of images between centres has been going on for a number of years and has proved to be valuable for centres seeking expert opinions on emergency and problem cases. The most common such connections have been with radiologists who work at a site and are now able to offer image interpretations online from other sites within an institution, from their offices, home or elsewhere. More recently radiological images have been transmitted to main centres from smaller community hospitals in areas of low population density where small radiology departments have proven unsustainable. The vastly improved capacity of the internet and the speed of transmission have permitted a much wider use of teleradiology. Teleradiology has advantages but it must be done properly to ensure that a high quality of care is provided to patients and to maintain the radiologist interaction with their clinical colleagues. It is also important that those radiologists providing the service are properly trained, are registered with the appropriate authorities, and undergo continuing update through Continuing Medical Education (CME).
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 41
The services provided must be open to audit and the ability to discuss cases with those reporting the studies must be available. This standard has been developed to provide guidance to radiologists, managers of health care facilities, patient’s representatives and governments on appropriate standards for teleradiology services. Teleradiology has undergone a number of health-technology assessments in different countries with regard to the context of its use, but a great deal of thought and study is still required. Teleradiology clearly has a number of advantages, but it also has the potential to create considerable difficulties for the delivery of a high quality radiological service to patients, unless its role and the legal responsibilities involved are clearly defined. Role of a Diagnostic Radiologist The role of a radiologist providing medical services in a diagnostic imaging service is considerably wider than simply issuing a diagnostic interpretation and report. It includes:
• Evaluating the clinical information produced by referring physician clinicians. • Deciding which test is appropriate. • Establishing and assuming responsibility for the imaging protocols, quality parameters and a
host of other technical factors that are integral to the creation of the diagnostic image and report.
• Being responsible for the technical staff/standards involved in the diagnostic imaging facility. • Optimizing the study and assisting the referring physician colleague. • Evaluating the study and relating it to the clinical findings. • Having knowledge of the practice of referring physicians. • Reviewing previous examinations and their interpretations to compare them with the current
study. • Identifying further appropriate management including diagnostic investigations essential to
obtain a comprehensive diagnosis and treatment, and reviewing. • Those recommendations with referring physicians. • Reviewing all clinical data in a multi-disciplinary environment. • Performing interventional therapeutic and diagnostic procedures
Assuming responsibility for the appropriate management of the patient during the diagnostic imaging procedure.
• Contributing radiological expertise to the management of the diagnostic imaging service to ensure the highest possible quality assurance and quality control.
• Being responsible for patient safety by ensuring minimal exposure to radiation dose and other matters that could compromise patient care.
• Adhering to all provincial and federal regulations, statutes relating to the delivery of medical services generally and diagnostic imaging services provincially.
• Meeting and exceeding the standard of care in the delivery of diagnostic imaging services in the province; maintaining membership in all of the licensing bodies and fulfilling the requirements of that licensure regime.
• Ensuring the selection and use of appropriate and modern equipment, properly trained staff and other elements in the high quality delivery of diagnostic imaging.
• Where relevant, teaching radiology residents and fellows according to national training program requirements.
• Where relevant, participating in radiology research. • Auditing the delivery of radiology services in the sites where the radiologist works
42 The College of Physicians and Surgeons of Ontario
• Ensuring timely communication of urgent findings. • Maintaining appropriate records/confidentiality as mandated by legislation.
In essence, appropriate teleradiology in this era is the same as the whole practice of radiology. The fact that patient data can be moved over a broadband connection does not alter the role or responsibilities of the supervising and interpreting radiologist. The importance of interaction between the referring clinicians and the radiologist cannot be over-emphasized. There are considerable quality patient care and medical-legal implications when teleradiology services are provided by a radiologist outside the patient’s jurisdiction. Regulatory bodies, licensing and credentialing (including the College of Physicians and Surgeons of Ontario, the Royal College of Physicians and Surgeons of Canada, Health Protection Branch, the Ministry of Health’s Independent Health Facility branch, OHIP, X-ray Inspection branch, and other provincial and federal bodies), are unable to enforce regulations outside their jurisdiction yet have a responsibility to patients with respect to the enforcement of a wide spectrum of regulations and statutes inter-linked to the high quality delivery of radiologists’ services in the province. The requirements of these and other related bodies are constantly subject to change requiring the radiologist to comply with a new and more stringent degree of responsibility with respect to the delivery of patient care. Key Principles
1. Diagnostic radiology is an integrated medical service required in every modern health care system.
2. Referring physicians are dependent upon the local availability of diagnostic imaging physicians to assist them to manage the health of their patients.
3. Only fully qualified diagnostic radiologists should provide the teleradiology service. They must be properly accredited, registered, and licenced in Ontario. The radiologist should be subject to licensing and quality assurance requirements of the provincial health authority; legislative and professional requirements of the facility providing the service; the provincial College of Physicians and Surgeons, accreditation and be in good standing with the Royal College of Physicians and Surgeons of Canada.
4. A definitive report is mandatory with the signature of the reporting radiologist. Electronic signatures are acceptable as long as they can be authenticated.
5. In a public hospital the members of the radiology department must be credentialed and be part of the recognized medical staff.
6. The department head via the Medical Advisory Committee (MAC) and Board is responsible for the medical service.
7. In an Independent Health Facility (IHF), the off-site radiologist must be approved by the radiologist Quality Advisor who is legislatively responsible for Quality Control/Quality Assurance (QC/QA) at the IHF.
8. All radiologists providing teleradiology services must be covered by the Canadian Medical Protective Association (CMPA) for medical liability issues and ensure they are compliant with current CMPA guidelines and policies covering diagnostic imaging physicians to safeguard patient interests.
9. Ensure that all radiologists and their staff involved in the delivery of teleradiology services are in full compliance with relevant privacy legislation and facility policies to protect patient confidentiality.
10.Ensure that the information received for a primary read is the full data set and that the reading radiologist should have all of the functionality of the PACS at his/her disposal to do an interpretation.
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 43
Key Management Issues
1. Teleradiology services must be organized between the source radiologists and the off-site radiologist provider to guarantee the proper management of the patient. This will ensure that:
a. The clinical evaluation and data is provided with the request for the examination. b. The requirements of the Healing Arts Radiation Protection Act (HARP) (including justification,
appropriate techniques, optimization, and good procedure) are fulfilled. c. The report of the teleradiology service can be reviewed with clinicians and where applicable,
in multi-disciplinary meetings and integrated with patients’ notes and previous studies. d. The reporting radiologist of the teleradiology service is able to communicate directly with the
referring radiology department and clinicians in order to discuss the clinical background and unexpected diagnosis, which may be relevant to the timely management of the patient.
e. Teleradiology services that are developed to meet the needs of rural, remote and small community areas must be linked to the nearest substantive radiology department and the service is managed by that department. The radiologists involved in providing the service must have a close connection and knowledge of referring clinicians, and technologists, and should understand any particular local disease and cultural factors.
2. Equipment used for teleradiology should provide a similar level of resolution and functionality as is
available in the radiology department/facility. 3. The American College of Radiology’s (ACR) Technical Standard for Teleradiology for equipment and
other supporting technologies used in the delivery of teleradiology is the acknowledged current technical standard. Radiologists delivering teleradiology standards are expected to comply or exceed the ACR Technical Standard for Teleradiology.
Real and Potential Problems
Clinico-Radiological Communication
If reporting of radiographs is taken away from close proximity with the patient, the clinical contact between the referring clinicians and radiologists is substantially reduced. It is imperative that teleradiology facilities have phone links with the hospitals and/or clinics from which images are obtained, and have the ability for direct discussion between a referring clinician and the reporting radiologist on individual cases. Without this, the bond between the patient and the radiologist becomes unclear. If urgent or significant unexpected features are found, the teleradiology service must transmit them directly to the referring clinician. This will be impossible unless there is a clear point of contact for the teleradiology service.
Team Working
The ability to hold multi-disciplinary meetings is much more difficult with teleradiology, even with teleconference links. It is now widely accepted that multi-disciplinary meetings, which are often led by the radiology department, are essential in the management of problematic cases, i.e., cancer care. They maximize the understanding of the clinical problems by radiologists. External reviews of health care disasters have emphasized the importance of teamwork especially in medicine and the need for enhanced teamwork, involving radiology has been highlighted. Interaction between different members of the hospital team with radiology may be impaired, if radiology is undertaken at the long distance by a teleradiology link.

44 The College of Physicians and Surgeons of Ontario
Communication
It is necessary that there be good communication between referring physicians, radiologists and technologists.
Wording of Report and Clinical Impact
Even if radiologists and referring clinicians have a common first language, it has to be recognized that radiological reporting may be subject to regional variation. Radiological reports often rely on verbal expressions of probability and may contain some regionally used expressions. Modern imaging commonly demonstrates an abundance of reportable findings, some of which are clinically relevant and some of which are incidental findings/pseudo-disease. Multiple pathologies can exist in the same patient. The clarity and certainty conveyed in the text is particularly important in converting a report that is merely ‘diagnostically accurate’ into one that has a diagnostic outcome and potentially a therapeutic outcome for the patient. Clinicians are more likely to act on the nuances intended in a report generated by a radiologist with whom they regularly liaise compared with a report generated by a third party teleradiology service from someone they never met. Specific wording of reports for general family doctors may be necessary, which is different from the reports to specialists within their sphere of interest. Familiarity with the referring doctors can make specific reports more appropriate and useful. Health care delivery varies between different jurisdictions. Recommendations for further imaging/specialist referral, which might be appropriate in the locale where a teleradiology service is provided, may be inappropriate in the area where the patient is located. Access to Previous Examinations/Interpretations
The failure to review previous examinations and interpretations has been shown to be a significant cause of errors in both perception and cognition. It is therefore important that previous studies and reports are available to the reporting radiologist where these are relevant. This should be possible if the teleradiology service has access to the referrer’s PACS system. There also has to be access to the hospital information system, so relevant lab data and clinical notes can be reviewed. Downstream Costs
Teleradiology may generate significant downstream costs. There is potentially increased cost from recommendations by the teleradiology service (which may actually be unnecessary) are required due to the inexperience or insecurity of the reader of the initial study or from clinicians responding to reports describing clinically insignificant radiological findings. There may be variations in the style of practice in different jurisdictions that impact the kind or volume of studies ordered. This problem will be compounded by a potential lack of background clinical knowledge of the case and the clinical expectations of the referring clinician by the teleradiology service. Clinicians who are not confident in a report from a teleradiology service may ask radiologists with whom they work to re-report the images and to advise on case management, thus leading to duplication and poor use of financial resources. For all of these reasons, the importance of close communication between the radiologist and the clinician to minimize inappropriate clinical referrals for imaging cannot be over emphasized. Quality Control and Quality Assurance
Quality control is paramount with teleradiology in order to prevent errors in radiology. Learning from mistakes through participation in radiological discrepancy/error meetings is established practice. Much informal feedback occurs at clinico-radiological meetings and corridor encounters. Audit is another potent form of radiological quality assurance. All these activities are much more difficult for a
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 45
teleradiology service which would need a very close link between the radiologists and clinicians at the source hospital/facility. It is difficult for teleradiology services to have a proper feedback of the outcome and undertake satisfactory audit of their reports. Radiologists providing services may provide advice relating to radiation exposure, image quality, patient positioning, and several other quality assurance and quality control (QA/QC) issues based on images they have received for interpretation. They must communicate directly with technologists, often real time, so as to be able to intervene directly to ensure optimal QA and QC. The Radiation Protection Officer, an on-site radiologist, remains responsible for the overall QA and QC and ensuring safe operation of a facility. Legal Issues
There are a number of potential legal issues.
a. The registration of the reporting doctors must be accredited by the regulatory body of the local jurisdiction of a hospital/facility or the health authority purchasing the service. This is an essential requirement in order to maintain proper standards of practice. The reporting radiologists must demonstrate that they undergo appropriate CME and are properly trained in the tasks to be undertaken.
b. The providers of the service must abide by the jurisdiction’s health and safety legislation.
c. The use of radiology also creates difficulties in terms of the medico-legal issues and the medico-legal responsibilities of the referring hospital/facility and that of the reporting teleradiology services must be identified. Any radiologist that reviews images has a responsibility. Liability may also reside with the purchasers of the radiology service and/or the employers of the “radiologist”. It must be clear who maintains responsibility for the patient. It is clear that the “radiologist” has a direct responsibility for the patients whose study they interpret. Teleradiology providers would have to comply with any statutory duty of candor to inform the hospital/facility and patient(s) when they become aware of a negligent act or omission. At present, the legal status of teleradiology remains to be clearly established.
d. Consent. It is not clear whether the patients will be required to give explicit consent for their images to be transferred to another country or different provincial jurisdiction for reporting.
e. Jurisdiction. An individual has the right to sue a company providing electronic services within another country and the suit would be heard in the patient’s own country or provincial jurisdiction.
f. Patient confidentiality. The teleradiology service must ensure patient confidentiality and be of adequate technical specification. It must comply with the data protection legislation in the transmitting and receiving provincial jurisdiction.
g. There is increasing awareness of the need to reduce the radiation dose that many patients receive, particularly CT scanning. When creating teleradiology contracts, it must be made clear who has responsibility for defining the protocol of an individual imaging study, e.g. high or low dose depending on clinical indication. Teleradiology providers need to comply with pertinent directives mandated in the provincial jurisdiction.
46 The College of Physicians and Surgeons of Ontario
OHIP Billing Rule Affecting Teleradiology in Ontario
OHIP added the following rule interpretation commentary to the October 2010 Schedule of Benefits (refer to page D1 of the Diagnostic Radiology section of the Schedule) where the additional note was added and remains in effect: Commentary: As described in Regulation 552 of the Health Insurance Act, for a service to be insured, the interpreting physician must physically be present in Ontario when the interpretation service is rendered. Legal Interpretation
The specific legal reference is found in Subsection 37.1(1) of R.R.O. 1990, Regulation 552 made under the Health Insurance Act, R.S.O., c. H. 6. Section 37.1(1) of the Regulation provides:
A service rendered by a physician in Ontario is an insured service if it is referred to in the schedule of benefits and rendered in such circumstances or under such conditions as my be specified in the Schedule of Benefits. [emphasis added]
Guidelines for the Development and Appropriate Use of Teleradiology
1. The principle that the patient is best served by a close liaison between the patient, the clinicians and the clinical radiology department should be paramount.
2. The radiologist’s expected duty of care to the patient must not be compromised, lowered, or altered in any way by the use of teleradiology.
3. Teleradiology referrals should, be in the majority of cases, organized between clinical radiologists and the teleradiology provider. It is important that the radiologists act as practitioners under the statutes, regulations, directives, policies, bulletins, bylaws issued by provincial and local hospital/clinic authorities in order to ensure that appropriate investigations are performed and to justify any further investigations suggested by the reporting radiologist.
4. The full agreement of radiologists should be obtained in order for the development of teleradiology services to be implemented.
5. Teleradiology services developed for rural, remote and/or under-serviced areas should be linked to other facilities in the province of Ontario and the service should be managed by the receiving department/clinic unless there is a radiologist at the originating centre who may elect to assume that responsibility or share it with the receiving centre radiologist. The radiologists involved in providing the service should have close communication with the referring clinicians and patients and should understand any particular local disease and cultural factors.
6. The radiologists providing the service must be properly accredited and registered within the provincial jurisdiction where the patient receives the service. They should also be registered and subject to quality and revalidation requirements, where applicable.
7. Under no circumstances should teleradiology reports be made by radiologists in training without supervision and the implementation of teleradiology should not be to the detriment of the training in the originating centre.
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 47
8. The use of subspecialty services should be for the benefit of a second opinion or for the immediate transfer of patients to specialist centres and not for the centralization of subspecialty reporting away from general hospitals/clinics.
9. The reporting radiologist of the teleradiology service must be able to communicate directly with the referring radiology department and clinicians in order to discuss the clinical background and unexpected diagnosis which may be relevant to the timely management of the patient. The equipment used to undertake the whole process of teleradiology must be of a quality and standard that provides diagnostic quality images at all times.
10. Proper audit procedures should be in place in order to check the quality of the teleradiology service, the accuracy of the radiological reports and the overall therapeutic and clinical impact of the service. This must include user/clinician feedback.
11. The teleradiology service must comply with all national and provincial data protection standards. Transfer of images outside the province could pose significant problems of data protection. It is essential that the privacy and the integrity of patient information must be preserved at all times.
12. There needs to be clearly defined agreement with the teleradiology service with regard to confidentiality of the images which should allow retention for comparison, proper defense against litigation or other clinically appropriate reason.
13. The legal arrangements must be clearly defined between the user and the provider so that proper restitution may be made to patients, if errors are made. If the service is less than optimal, patients should not be required to litigate in the foreign country in the event of a complaint unless they have consented formally to the transfer of their rights for local litigation in addition to initial image transfer.
14. At all times the provision of teleradiology must be primarily developed in the best interest of the patient care and not as a cost cutting measure which may jeopardize patient safety and standards of health care.
48 The College of Physicians and Surgeons of Ontario
APPENDICES FOR MRI/CT AND GENERAL GUIDANCE
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd Edition 49
Appendix I ACR Guidance Document on MR Safe Practices: 2013
Citation for published article: J Magnetic Resonance Imaging 2013, 37:501–530
Paper provided in cooperation with the publisher, the American College of Radiology (www.acr.org). May, 2015.
http://onlinelibrary.wiley.com/doi/10.1002/jmri.24011/pdf
(Full text version on next page)
Special Communication
ACRGuidance Document on MR Safe Practices: 2013
Expert Panel on MR Safety: Emanuel Kanal, MD,1* A. James Barkovich, MD,2
Charlotte Bell, MD,3 James P. Borgstede, MD,4 William G. Bradley Jr, MD, PhD,5
Jerry W. Froelich, MD,6 J. Rod Gimbel, MD,7 John W. Gosbee, MD,8
Ellisa Kuhni-Kaminski, RT,1 Paul A. Larson, MD,9 James W. Lester Jr, MD,10
John Nyenhuis, PhD,11 Daniel Joe Schaefer, PhD,12 Elizabeth A. Sebek, RN, BSN,1
Jeffrey Weinreb, MD,13 Bruce L. Wilkoff, MD,14 Terry O. Woods, PhD,15
Leonard Lucey, JD,16 and Dina Hernandez, BSRT16
Because there are many potential risks in the MR envi-ronment and reports of adverse incidents involvingpatients, equipment and personnel, the need for a guid-ance document on MR safe practices emerged. Initiallypublished in 2002, the ACR MR Safe Practices Guidelinesestablished de facto industry standards for safe andresponsible practices in clinical and research MR environ-ments. As the MR industry changes the document isreviewed, modified and updated. The most recent versionwill reflect these changes.
Key Words: MR safety; MR; MR safe practicesJ. Magn. Reson. Imaging 2013;37:501–530.VC 2013 Wiley Periodicals, Inc.
THERE ARE POTENTIAL risks in the MR environ-ment, not only for the patient (1,2) but also for theaccompanying family members, attending health careprofessionals, and others who find themselves onlyoccasionally or rarely in the magnetic fields of MRscanners, such as security or housekeeping person-nel, firefighters, police, etc. (3–6). There have beenreports in the medical literature and print-mediadetailing Magnetic Resonance Imaging (MRI) adverseincidents involving patients, equipment and personnelthat spotlighted the need for a safety review by anexpert panel. To this end, the American College ofRadiology originally formed the Blue Ribbon Panel onMR Safety. First constituted in 2001, the panel wascharged with reviewing existing MR safe practices andguidelines (5–8) and issuing new ones as appropriatefor MR examinations. Published initially in 2002 (4),the ACR MR Safe Practice Guidelines established defacto industry standards for safe and responsiblepractices in clinical and research MR environments.These were subsequently reviewed and updated inMay of 2004 (3). After reviewing substantial feedbackfrom the field and installed base, as well as changesthat had transpired throughout the MR industry sincethe publication of the 2004 version of this document,the panel extensively reviewed, modified, and updatedthe entire document in 2006–2007.
The present panel consists of the followingmembers: A. James Barkovich, MD, Charlotte Bell,MD, (American Society of Anesthesiologists), James P.Borgstede, MD, FACR, William G. Bradley, MD, PhD,FACR, Jerry W. Froelich, MD, FACR, J. Rod Gimbel,MD, FACC, Cardiologist, John Gosbee, MD, MS, EllisaKuhni-Kaminski, RT (R)(MR), Emanuel Kanal, MD,FACR, FISMRM (chair), James W. Lester Jr., MD,John Nyenhuis, PhD, Daniel Joe Schaefer, PhD Engi-neer, Elizabeth A. Sebek, RN, BSN, CRN, JeffreyWeinreb, MD, Terry Woods, PhD, FDA, Pamela Wilcox,RN, MBA (ACR Staff), Leonard Lucey, JD, LLM (ACRStaff), and Dina Hernandez, RT (R) (CT) (QM) (ACRStaff). The following represents the most recently
1Department of Radiology, University of Pittsburgh Medical Center,Pittsburgh, Pennsylvania, USA.2Department of Radiology and Biomedical Imaging, University ofCalifornia, San Francisco, California, USA.3Milford Anesthesia Associates, Milford, Connecticut, USA.4University of Colorado, Denver, Colorado, USA.5Department of Radiology, University of California San Diego MedicalCenter, San Diego, California, USA.6Department of Radiology, University of Minnesota, Minneapolis,Minnesota, USA.7Cardiology Associates of E. Tennessee, Knoxville, Tennessee, USA.8University of Michigan Health System and Red Forest Consulting LLC,Ann Arbor, Michigan, USA.9Radiology Associates of the Fox Valley, Neenah, Wisconsin, USA.10Durham Radiology Associates, Raleigh, North Carolina, USA.11Department of Electrical and Computer Engineering, PurdueUniversity, West Lafayette, Indiana, USA.12MR Systems Engineering, GE Healthcare, Waukesha, Wisconsin, USA.13Yale School of Medicine, New Haven, Connecticut, USA.14Cleveland Clinic, Cleveland, Ohio, USA.15FDA Center for Devices & Radiological Health, Silver Spring,Maryland, USA.16American College of Radiology, Reston, Virginia, USA.
Reprint requests to: Department of Quality & Safety, American Col-lege of Radiology, 1891 Preston White Drive, Reston, VA 20191-4397.
*Address reprint requests to: E.K., University of Pittsburgh MedicalCenter, Presbyterian University Hospital\Presbyterian South Tower,Room 4776, Pittsburgh, PA 15213. E-mail: [email protected]
Received October 3, 2012; Accepted December 4, 2012.
DOI 10.1002/jmri.24011View this article online at wileyonlinelibrary.com.
JOURNAL OF MAGNETIC RESONANCE IMAGING 37:501–530 (2013)
CME
VC 2013 Wiley Periodicals, Inc. 501
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 68

modified and updated version of the combined priorthree reports (3,4,9) issued by the American College ofRadiology Blue Ribbon Panel on MR Safety, chaired byEmanuel Kanal, MD, FACR. It is important to note thatnothing that appears herein is the result of a ‘‘majorityvote’’ of the member of this panel. As with each priorpublication of these ACR MR Safe Practice Guidelines,the entire document, from introduction to the mark-edly expanded appendices, represents the unanimousconsensus of each and every member of this SafetyCommittee and the various areas of expertise that theyrepresent. This includes representation from fields andbackgrounds as diverse as MR physicists, research/academic radiologists, private practice radiologists, MRsafety experts, patient safety experts/researchers, MRtechnologists, MR nursing, National Electrical Manu-facturers Association, the Food and Drug Administra-tion, the American Society of Anesthesiologists, legalcounsel, and others. Lay personnel, physicians,Ph.D.s, department chairs and house-staff/residents,government employees and private practitioners,doctors, nurses, technologists, radiologists, anesthesi-ologists, cardiologists, attorneys—these are allrepresented on this Committee. It was believed thatachieving unanimity for these Guidelines was criticalto demonstrate to all that these Guidelines are notonly appropriate from a scientific point of view, butreasonably applicable in the real world in which we allmust live, with all its patient care, financial, andthroughput pressures and considerations. The viewsexpressed in this study are solely those of the authorsand in no way suggest a policy or position of any of theorganizations represented by the authors.
The following MR safe practice guidelines documentis intended to be used as a template for MR facilities tofollow in the development of an MR safety program.These guidelines were developed to help guide MR prac-titioners regarding these issues and to provide a basisfor them to develop and implement their own MR poli-cies and practices. It is intended that these MR safepractice guidelines (and the policies and procedures towhich they give rise) be reviewed and updated on a reg-ular basis as the field of MR safety continues to evolve.
The principles behind these MR Safe PracticeGuidelines are specifically intended to apply not onlyto diagnostic settings but also to patient, researchsubject, and health care personnel safety for all MRIsettings, including those designed for clinical diagnos-tic imaging, research, interventional, and intraopera-tive MR applications.
With the increasing advent and use of 3.0-Tesla andhigher strength magnets, users need to recognize thatone should never assume MR compatibility or safetyinformation about a device if it is not clearly docu-mented in writing. Decisions based on published MRsafety and compatibility claims should recognize thatall such claims apply only to specifically tested condi-tions, such as static magnetic field strengths, staticgradient magnetic field strengths and spatial distribu-tions, and the strengths and rates of change of gradi-ent and radiofrequency (RF) magnetic fields.
Finally, there are many issues that impact MRsafety which should be considered during site
planning for a given MR installation. We include inthis manuscript, as separate appendices, sectionsthat address such issues as well, including cryogenemergency vent locations and pathways, 5-Gaussline, siting considerations, patient access pathways,etc. Yet despite their appearance herein, these issues,and many others, should be reviewed with those expe-rienced with MR site planning and familiar with thepatient safety and patient flow considerations beforecommitting construction to a specific site design. Inthis regard, enlisting the assistance of an architec-tural firm experienced in this area, and doing so earlyin the design stages of the planning process, mayprove most valuable.
It remains the intent of the ACR that these MR SafePractice Guidelines will prove helpful as the field ofMRI continues to evolve and mature, providing MRservices that are among the most powerful, yet safest,of all diagnostic procedures to be developed in thehistory of modern medicine.
ACR GUIDANCE DOCUMENT ON MR SAFEPRACTICES: 2013
A. Establish, Implement, and Maintain CurrentMR Safety Policies and Procedures
1. All clinical and research MR sites, irrespective ofmagnet format or field strength, including instal-lations for diagnostic, research, interventional,and/or surgical applications, should maintainMR safety policies.
2. These policies and procedures should also bereviewed concurrently with the introduction ofany significant changes in safety parameters ofthe MR environment of the site (e.g., addingfaster or stronger gradient capabilities or higherRF duty cycle studies) and updated as needed. Inthis review process, national and internationalstandards and recommendations should betaken into consideration before establishing localguidelines, policies, and procedures
3. Each site will name a MR medical director whoseresponsibilities will include ensuring that MRsafe practice guidelines are established andmaintained as current and appropriate for thesite. It is the responsibility of the site’s adminis-tration to ensure that the policies and proceduresthat result from these MR safe practice guide-lines are implemented and adhered to at all timesby all of the site’s personnel.
4. Procedures should be in place to ensure that anyand all adverse events, MR safety incidents, or‘‘near incidents’’ that occur in the MR site are tobe reported to the medical director in a timelymanner (e.g., within 24 hours or 1 business dayof their occurrence) and used in continuous qual-ity improvement efforts. It should be stressedthat the Food and Drug Administration statesthat it is incumbent upon the sites to also reportadverse events and incidents to them by meansof their Medwatch program. The ACR supportsthis requirement and believes that it is in the
502 Kanal et al.
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 69
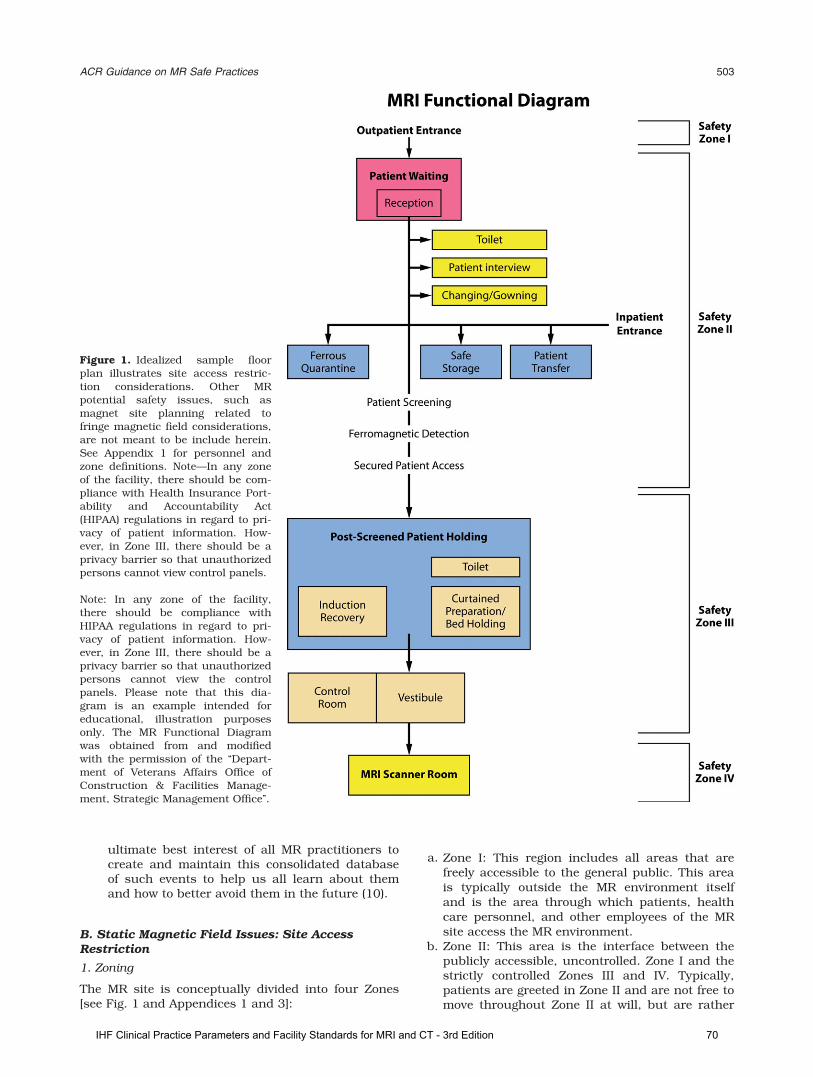
ultimate best interest of all MR practitioners tocreate and maintain this consolidated databaseof such events to help us all learn about themand how to better avoid them in the future (10).
B. Static Magnetic Field Issues: Site AccessRestriction
1. Zoning
The MR site is conceptually divided into four Zones[see Fig. 1 and Appendices 1 and 3]:
a. Zone I: This region includes all areas that arefreely accessible to the general public. This areais typically outside the MR environment itselfand is the area through which patients, healthcare personnel, and other employees of the MRsite access the MR environment.
b. Zone II: This area is the interface between thepublicly accessible, uncontrolled. Zone I and thestrictly controlled Zones III and IV. Typically,patients are greeted in Zone II and are not free tomove throughout Zone II at will, but are rather
Figure 1. Idealized sample floorplan illustrates site access restric-tion considerations. Other MRpotential safety issues, such asmagnet site planning related tofringe magnetic field considerations,are not meant to be include herein.See Appendix 1 for personnel andzone definitions. Note—In any zoneof the facility, there should be com-pliance with Health Insurance Port-ability and Accountability Act(HIPAA) regulations in regard to pri-vacy of patient information. How-ever, in Zone III, there should be aprivacy barrier so that unauthorizedpersons cannot view control panels.
Note: In any zone of the facility,there should be compliance withHIPAA regulations in regard to pri-vacy of patient information. How-ever, in Zone III, there should be aprivacy barrier so that unauthorizedpersons cannot view the controlpanels. Please note that this dia-gram is an example intended foreducational, illustration purposesonly. The MR Functional Diagramwas obtained from and modifiedwith the permission of the ‘‘Depart-ment of Veterans Affairs Office ofConstruction & Facilities Manage-ment, Strategic Management Office’’.
ACR Guidance on MR Safe Practices 503
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 70

under the supervision of MR personnel (seesection B.2.b, below). It is in Zone II that theanswers to MR screening questions, patienthistories, medical insurance questions, etc. aretypically obtained.
c. Zone III: This area is the region in which freeaccess by unscreened non-MR personnel orferromagnetic objects or equipment can result inserious injury or death as a result of interactionsbetween the individuals or equipment and theMR scanner’s particular environment. Theseinteractions include, but are not limited to, thoseinvolving the MR scanner’s static and time-vary-ing magnetic fields. All access to Zone III is to bestrictly restricted, with access to regions within it(including Zone IV see below) controlled by, andentirely under the supervision of, MR personnel(see Section B.2.b, below). Specifically identifiedMR personnel (typically, but not necessarily only,the MR technologists) are to be charged withensuring that this MR safe practice guideline isstrictly adhered to for the safety of the patientsand other non-MR personnel, the health care per-sonnel, and the equipment itself. This function ofthe MR personnel is directly under the authorityand responsibility of the MR medical director orthe level 2-designated (see section B.2.b, below)physician of the day for the MR site.Zone III regions should be physically restrictedfrom general public access by, for example, keylocks, passkey locking systems, or any other reli-able, physically restricting method that can dif-ferentiate between MR personnel and non-MRpersonnel. The use of combination locks is dis-couraged as combinations often become morewidely distributed than initially intended, result-ing in site restriction violations being more likelywith these devices. Only MR personnel shall beprovided free access, such as the access keys orpasskeys, to Zone III.There should be no exceptions to this guideline.Specifically, this includes hospital or site adminis-tration, physician, security, and other non-MR per-sonnel (see section B.2.c, below). Non-MRpersonnel are not to be provided with independentZone III access until such time as they undergo theproper education and training to become MR per-sonnel themselves. Zone III, or at the very least thearea within it wherein the static magnetic field’sstrength exceeds 5-Gauss should be demarcatedand clearly marked as being potentially hazardous.Because magnetic fields are three-dimensionalvolumes, Zone III controlled access areas mayproject through floors and ceilings of MRI suites,imposing magnetic field hazards on persons onfloors other than that of the MR scanner. Zonesof magnetic field hazard should be clearlydelineated, even in typically nonoccupied areassuch as rooftops or storage rooms, and access tothese Zone III areas should be similarly restrictedfrom non-MR personnel as they would be insideany other Zone III region associated with the MRIsuite. For this reason, magnetic field strength
plots for all MRI systems should be analyzed invertical section as well as in horizontal plan,identifying areas above or below, in addition toareas on the same level, where persons may beat risk of interactions with the magnetic field.
d. Zone IV: This area is synonymous with the MRscanner magnet room itself, i.e., the physicalconfines of the room within which the MRscanner is located (see Appendix 3). Zone IV, bydefinition, will always be located within Zone III,as it is the MR magnet and its associated mag-netic field that generates the existence of ZoneIII. Zone IV should also be demarcated andclearly marked as being potentially hazardousdue to the presence of very strong magneticfields. As part of the Zone IV site restriction, allMR installations should provide for direct visualobservation by level 2 personnel to access path-ways into Zone IV. By means of illustration only,the MR technologists would be able to directlyobserve and control, by means of line of site orby means of video monitors, the entrances oraccess corridors to Zone IV from their normalpositions when stationed at their desks in thescan control room.Zone IV should be clearly marked with a red lightand lighted sign stating, ‘‘The Magnet is On’’.Ideally, signage should inform the public that themagnetic field is active even when power to thefacility is deactivated. Except for resistive sys-tems, this light and sign should be illuminated atall times and should be provided with a batterybackup energy source to continue to remainilluminated in the event of a loss of power tothe site.In case of cardiac or respiratory arrest or othermedical emergency within Zone IV for whichemergent medical intervention or resuscitation isrequired, appropriately trained and certified MRpersonnel should immediately initiate basic lifesupport or CPR as required by the situationwhile the patient is being emergently removedfrom Zone IV to a predetermined, magneticallysafe location. All priorities should be focused onstabilizing (e.g., basic life support with cardiaccompressions and manual ventilation) and thenevacuating the patient as rapidly and safely aspossible from the magnetic environment thatmight restrict safe resuscitative efforts.Furthermore, for logistical safety reasons, thepatient should always be moved from Zone IV to theprospectively identified location where full resusci-tative efforts are to continue (see Appendix 3).Quenching the magnet (for superconducting sys-tems only) is not routinely advised for cardiac orrespiratory arrest or other medical emergency,because quenching the magnet and having themagnetic field dissipate could easily take morethan a minute. Furthermore, as quenching amagnet can theoretically be hazardous, ideallyone should evacuate the magnet room, whenpossible, for an intentional quench. One shouldrather use that time wisely to initiate life support
504 Kanal et al.
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 71
measures while removing the patient from ZoneIV to a location where the strength of the mag-netic field is insufficient to be a medical concern.Zones III and IV site access restriction must bemaintained during resuscitation and other emer-gent situations for the protection of all involved.
2. MR Personnel and non-MR personnel
a. All individuals working within at least Zone III of theMR environment should be documented as havingsuccessfully completed at least one of the MR safetylive lectures or prerecorded presentations approvedby the MR medical director. Attendance should berepeated at least annually, and appropriate docu-mentation should be provided to confirm theseongoing educational efforts. These individuals shallbe referred to henceforth as MR personnel.
b. There are two levels of MR personnel:1. Level 1 MR personnel: Those who have passed
minimal safety educational efforts to ensure theirown safety as they work within Zone III will bereferred to henceforth as level 1 MR personnel.
2. Level 2 MR personnel: Those who have beenmore extensively trained and educated in thebroader aspects of MR safety issues, including,for example, issues related to the potential forthermal loading or burns and direct neuromus-cular excitation from rapidly changing gradients,will be referred to henceforth as level 2 MR per-sonnel. It is the responsibility of the MR medicaldirector not only to identify the necessary train-ing, but also to identify those individuals whoqualify as level 2 MR personnel. It is understoodthat the medical director will have the necessaryeducation and experience in MR safety to qualifyas level 2 MR personnel. (See Appendix 1.)
c. All those not having successfully complied withthese MR safety instruction guidelines shall bereferred to henceforth as non-MR personnel. Specifi-cally, non-MR personnel will be the terminologyused to refer to any individual or group who has notwithin the previous 12 months undergone the desig-nated formal training in MR safety issues defined bythe MR safety director of that installation.
3. Patient and non-MR personnel screening
a. All non-MR personnel wishing to enter Zone IIImust first pass an MR safety screening process.Only MR personnel are authorized to perform anMR safety screen before permitting non-MR per-sonnel into Zone III.
b. The screening process and screening forms forpatients, non-MR personnel, and MR personnelshould be essentially identical. Specifically, oneshould assume that screened non-MR personnel,health care practitioners, or MR personnel mayenter the bore of the MR imager during the MRimaging process.Examples of this might include if a pediatricpatient cries for his mother, who then leans into
the bore, or if the anesthetist leans into the boreto manually ventilate a patient in the event of aproblem.
c. Metal detectorsThe usage in MR environments of conventionalmetal detectors which do not differentiate betweenferrous and nonferromagnetic materials is not rec-ommended. Reasons for this recommendationagainst conventional metal detector usage include,among others:1. They have varied—and variable—sensitivity
settings.2. The skills of the operators can vary.3. Today’s conventional metal detectors cannot
detect, for example, a 2 � 3 mm, potentiallydangerous ferromagnetic metal fragment in theorbit or near the spinal cord or heart.
4. Today’s conventional metal detectors do not dif-ferentiate between ferromagnetic and nonferro-magnetic metallic objects, implants, or foreignbodies.
5. Metal detectors should not be necessary for thedetection of large metallic objects, such as oxy-gen tanks on the gurney with the patients.These objects are fully expected to be detected –and physically excluded – during the routinepatient screening process.
However, ferromagnetic detection systems are cur-rently available that are simple to operate, capableof detecting even very small ferromagnetic objectsexternal to the patient, and differentiating betweenferromagnetic and non-ferromagnetic materials.While the use of conventional metal detectors isnot recommended, the use of ferromagnetic detec-tion systems is recommended as an adjunct tothorough and conscientious screening of personsand devices approaching Zone IV. It should be reit-erated that their use is in no way meant to replacea thorough screening practice, which rathershould be supplemented by their usage.
d. Non-MR personnel should be accompanied by, orunder the immediate supervision of and in visualor verbal contact with, one specifically identifiedlevel 2 MR person for the entirety of their durationwithin Zone III or IV restricted regions. However, itis acceptable to have them in a changing room orrestroom in Zone III without visual contact as longas the personnel and the patient can communicateverbally with each other.Level 1 MR personnel are permitted unaccompa-nied access throughout Zones III and IV. Level 1MR personnel are also explicitly permitted to beresponsible for accompanying non-MR personnelinto and throughout Zone III, excluding Zone IV.However, level 1 MR personnel are not permittedto directly admit, or be designated responsible for,non-MR personnel in Zone IV.In the event of a shift change, lunch break, etc.,no level 2 MR personnel shall relinquish theirresponsibility to supervise non-MR personnel stillwithin Zone III or IV until such supervision hasbeen formally transferred to another of the site’slevel 2 MR personnel.
ACR Guidance on MR Safe Practices 505
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 72
e. Nonemergent patients should be MR safety screenedon site by a minimum of 2 separate individuals. Atleast one of these individuals should be level 2 MRpersonnel. At least one of these 2 screens should beperformed verbally or interactively.Emergent patients and their accompanying non-MR personnel may be screened only once, provid-ing the screening individual is level 2 MR person-nel. There should be no exceptions to this.
f. Any individual undergoing an MR procedure mustremove all readily removable metallic personalbelongings and devices on or in them (e.g.,watches, jewelry, pagers, cell phones, body pierc-ings (if removable), contraceptive diaphragms, me-tallic drug delivery patches (see Section I, below),cosmetics containing metallic particles (such aseye make-up), and clothing items which maycontain metallic fasteners, hooks, zippers, loosemetallic components or metallic threads). It istherefore advisable to require that the patients orresearch subjects wear a site-supplied gown withno metal fasteners when feasible.
g. All patients and non-MR personnel with a historyof potential ferromagnetic foreign object penetra-tion must undergo further investigation beforebeing permitted entrance to Zone III. Examples ofacceptable methods of screening include patienthistory, plain X-ray films, prior CT or MR studiesof the questioned anatomic area, or access to writ-ten documentation as to the type of implant or for-eign object that might be present. Once positiveidentification has been made as to the type ofimplant or foreign object that is within a patient,best effort assessments should be made to identifythe MR compatibility or MR safety of the implantor object. Efforts at identification might includewritten records of the results of formal testing ofthe implant before implantation (preferred), prod-uct labeling regarding the implant or object, andpeer-reviewed publications regarding MR compati-bility and MR safety testing of the specific make,model, and type of the object. MR safety testingwould be of value only if the object or device hadnot been altered since such testing had beenpublished and only if it can be confirmed that thetesting was performed on an object of precisely thesame make, model, and type.All patients who have a history of orbit trauma bya potential ferromagnetic foreign body for whichthey sought medical attention are to have theirorbits cleared by either plain X-ray orbit films(2 views) (11,12) or by a radiologist’s review andassessment of contiguous cut prior CT or MRimages (obtained since the suspected traumaticevent) if available.
h. Conscious, nonemergent patients and researchand volunteer subjects are to complete written MRsafety screening questionnaires before their intro-duction to Zone III. Family or guardians of nonres-ponsive patients or of patients who cannot reliablyprovide their own medical histories are to completea written MR safety screening questionnaire beforetheir introduction to Zone III. These completed
questionnaires are then to be reviewed orally withthe patient, guardian, or research subject in theirentirety before permitting the patient or researchsubject to be cleared into Zone III.The patient, guardian, or research subject as wellas the screening MR staff member must both signthe completed form. This form should then becomepart of the patient’s medical record. No emptyresponses will be accepted—each question must beanswered with a ‘‘yes’’ or ‘‘no’’ or specific further in-formation must be provided as requested. A sam-ple pre-MR screening form is provided (seeAppendix 2). This is the minimum information tobe obtained; more may be added if the site sodesires.
i. Screening of the patient or non-MR personnelwith, or suspected of having, an intracranial aneu-rysm clip should be performed as per the separateMR safe practice guideline addressing this particu-lar topic (see section M, below).
j. Screening of patients for whom an MR examina-tion is deemed clinically indicated or necessary,but who are unconscious or unresponsive, whocannot provide their own reliable histories regard-ing prior possible exposures to surgery, trauma, ormetallic foreign objects, and for whom such histor-ies cannot be reliably obtained from others:1. If no reliable patient metal exposure history can
be obtained, and if the requested MR examina-tion cannot reasonably wait until a reliable his-tory might be obtained, it is recommended thatsuch patients be physically examined by level 2MR personnel. All areas of scars or deformitiesthat might be anatomically indicative of animplant, such as on the chest or spine region,and whose origins are unknown and which mayhave been caused by ferromagnetic foreignbodies, implants, etc., should be subject toplain-film radiography (if recently obtainedplain films or CT or MR studies of such areasare not already available). The investigationdescribed above should be made to ensurethere are no potentially harmful embedded orimplanted metallic foreign objects or devices. Allsuch patients should also undergo plain filmimaging of the skull or orbits and chest toexclude metallic foreign objects (if recentlyobtained such radiographic or MR informationnot already available).
2. Monitoring of patients in the MR scanner issometimes necessary. However, monitoringmethods should be chosen carefully due to therisk of thermal injury associated with monitor-ing equipment in the MR environment. Sedated,anesthetized, or unconscious patients may notbe able to express symptoms of such injury.This potential for injury is greater on especiallyhigher field whole body scanners (e.g., 1 Teslaand above), but exists at least theoretically atall MR imaging field strengths. MR ConditionalEKG electrodes should be used and leadsshould be kept from touching the patients dur-ing the scan. Patients who require EKG
506 Kanal et al.
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 73

monitoring and who are unconscious, sedated,or anesthetized should be examined after eachimaging sequence with potential repositioningof the EKG leads and any other electrically con-ductive material with which the patient is incontact. Alternatively, cold compresses or icepacks could be placed upon all necessary elec-trically conductive material that touches thepatient during scanning.
Distortion of the electrocardiogram within themagnetic field can make interpretation of the ECGcomplex unreliable, even with filtering used bycontemporary monitoring systems. Routine moni-toring of heart rate and rhythm may also beaccomplished using pulse oximetry, which wouldeliminate the risks of thermal injury fromelectrocardiography.
k. Final determination of whether or not to scan anygiven patient with any given implant, foreign body,etc. is to be made by the level 2 designated attend-ing MR radiologist, the MR medical director, orspecifically designated level 2 MR personnel follow-ing criteria for acceptability predetermined by themedical director. These risks include, amongothers, consideration of mechanical and thermalrisks associated with MR imaging of implants, aswell as assessments of the safety of exposure ofthe device to the electromagnetic forces used inthe MR imaging process.For implants that are strongly ferromagnetic, anobvious concern is that of magnetic translationaland rotational forces upon the implant whichmight move or dislodge the device from itsimplanted position If an implant has demonstratedweak ferromagnetic forces on formal testing, itmight be prudent to wait several weeks for fibrousscarring to set in, as this may help anchor theimplant in position and help it resist such weaklyattractive magnetic forces that might arise in MRenvironments.For all implants that have been demonstrated tobe nonferrous in nature, however, the risk ofimplant motion is essentially reduced to thoseresulting from Lenz’s forces alone. These tend tobe quite trivial for typical metallic implant sizes ofa few centimeters or less. Thus, a waiting periodfor fibrous scarring to set in is far less important,and the advisability for such a waiting period maywell be easily outweighed by the potential clinicalbenefits of undergoing an MR examination at thattime. As always, clinical assessment of the riskbenefit ratio for the particular clinical situationand patient at hand are paramount for appropriatemedical decision making in these scenarios.It is possible that during the course of a magneticresonance imaging examination an unanticipatedferromagnetic implant or foreign body is discov-ered within a patient or research subject under-going the examination. This is typically suspectedor detected by means of a sizable field-distortingartifact seen on spin echo imaging techniques thatgrows more obvious on longer TE studies andexpands markedly on typical moderate or long TE
gradient echo imaging sequences. In such cases, itis imperative that the medical director, safety offi-cer, and/or physician in charge be immediatelynotified of the suspected findings. This individualshould then assess the situation, review the imag-ing information obtained, and decide what thebest course of action might be.It should be noted that there are numerous poten-tially acceptable courses that might be recom-mended which in turn are dependent upon manyfactors, including the status of the patient, the loca-tion of the suspected ferromagnetic implant/foreignbody relative to local anatomic structures, the massof the implant, etc. Appropriate course of actionsmight include proceeding with the scan under way,immobilizing the patient and the immediate re-moval from the scanner, or other intermediatesteps. Regardless of the course of action selected, itis important to note that the forces on the implantwill change, and may actually increase, during theattempt to remove the patient from the scannerbore. Furthermore, the greater the rate of motion ofthe patient/device through the magnetic fields ofthe scanner bore the greater the forces acting uponthat device will likely be. Thus it is prudent toensure that if at all possible, immobilization of thedevice during patient extraction from the bore, andslow, cautious, deliberate rate of extricating thepatient from the bore, will likely result in weakerand potentially less harmful forces on the device asit traverses the various static magnetic field gra-dients associated with the MR imager.It is also worthy of note that the magnetic fieldsassociated with the MR scanner are three dimen-sional. Thus, especially for superconducting sys-tems, one should avoid the temptation to have thepatient sit up as soon as they are physically out ofthe bore. Doing so may expose the ferrous objectto still significant torque- and translation-relatedforces despite their being physically outside thescanner bore. It is therefore advisable to continueto extract the patient along a straight line courseparallel to the center of the magnet while thepatient remains immobilized until they are as faras physically possible from the MR imager itself,before any other patient/object motion vector isattempted or permitted.
l. All non-MR personnel (e.g., patients, volunteers,varied site employees and professionals) withimplanted cardiac pacemakers, implantable cardi-overter defibrillators (ICDs), diaphragmatic pace-makers, electromechanically activated devices, orother electrically conductive devices upon whichthe non-MR personnel is dependent should be pre-cluded from Zone IV and physically restrainedfrom the 5-Gauss line unless specifically clearedin writing by a level 2 designated attending radiol-ogist or the medical director of the MR site. Insuch circumstances, specific defending risk-bene-fit rationale should be provided in writing andsigned by the authorizing radiologist.Should it be determined that non-MR personnelwishing to accompany a patient into an MR scan
ACR Guidance on MR Safe Practices 507
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 74

room require their orbits to be cleared by plain-filmradiography, a radiologist must first discuss withthe non-MR personnel that plain X-ray films of theirorbits are required before permitting them access tothe MR scan room. Should they still wish to proceedwith access to Zone IV or within the 5-G line, andshould the attending radiologist deem it medicallyadvisable that they do so (e.g., for the care of theirchild about to undergo an MR study), writteninformed consent should be provided by theseaccompanying non-MR personnel before theirundergoing X-ray examination of their orbits.
m. MR scanning of patients, prisoners, or paroleeswith metallic prisoner-restraining devices or RF IDor tracking bracelets could lead to theoreticaladverse events, including: (i) ferromagnetic attrac-tive effects and resultant patient injury, (ii) possi-ble ferromagnetic attractive effects and potentialdamage to the device or its battery pack, (iii) RFinterference with the MRI study and secondaryimage artifact, (iv) RF interference with the func-tionality of the device, (v) RF power deposition andheating of the bracelet or tagging device or its cir-cuitry and secondary patient injury (if the braceletwould be in the anatomic volume of the RF trans-mitter coil being used for imaging). Therefore, incases where requested to scan a patient, prisoner,or parolee wearing RF bracelets or metallic hand-cuffs or anklecuffs, request that the patient beaccompanied by the appropriate authorities whocan and will remove the restraining device beforethe MR study and be charged with its replacementfollowing the examination.
n. Firefighter, police, and security safety considera-tions: For the safety of firefighters and other emer-gent services responding to an emergent call at theMR site, it is recommended that all fire alarms,cardiac arrests, or other emergent service responsecalls originating from or located in the MR siteshould be forwarded simultaneously to a specifi-cally designated individual from amongst the site’sMR personnel. This individual should, if possible,be on site before the arrival of the firefighters oremergent responders to ensure that they do nothave free access to Zone III or IV. The site mightconsider assigning appropriately trained securitypersonnel, who have been trained and designatedas MR personnel, to respond to such calls.In any case, all MR sites should arrange to pro-spectively educate their local fire marshals, fire-fighters associations, and police or securitypersonnel about the potential hazards of respond-ing to emergencies in the MR suite.It should be stressed that even in the presence of atrue fire (or other emergency) in Zone III or IV, themagnetic fields may be present and fully operational.Therefore, free access to Zone III or IV by firefightersor other non-MR personnel with air tanks, axes,crowbars, other firefighting equipment, guns, etcmight prove catastrophic or even lethal to thoseresponding or others in the vicinity.As part of the Zone III and IV restrictions, all MRsites must have clearly marked, readily accessible
MR Conditional or MR Safe fire extinguishing equip-ment physically stored within Zone III or IV.All conventional fire extinguishers and other fire-fighting equipment not tested and verified safe inthe MR environment should be restricted fromZone III.For superconducting magnets, the helium (and thenitrogen as well, in older MR magnets) is not flam-mable and does not pose a fire hazard directly.However, the liquid oxygen that can result fromthe supercooled air in the vicinity of the releasedgases might well increase the fire hazard in thisarea. If there are appropriately trained and knowl-edgeable MR personnel available during an emer-gency to ensure that emergency responsepersonnel are kept out of the MR scanner or mag-net room and 5-Gauss line, quenching the magnetduring a response to an emergency or fire shouldnot be a requirement.However, if the fire is in such a location whereZone III or IV needs to be entered for whatever rea-son by firefighting or emergency response person-nel and their firefighting and emergent equipment,such as air tanks, crowbars, axes, defibrillators, adecision to quench a superconducting magnetshould be very seriously considered to protect thehealth and lives of the emergent responding per-sonnel. Should a quench be performed, appropri-ately designated MR personnel still need to ensurethat all non-MR personnel (including and espe-cially emergently response personnel) continue tobe restricted from Zones III and IV until the desig-nated MR personnel has personally verified thatthe static field is either no longer detectable or atleast sufficiently attenuated as to no longer pres-ent a potential hazard to one moving by it with, forexample, large ferromagnetic objects such as airtanks or axes.For resistive systems, the magnetic field of the MRscanner should be shut down as completely aspossible and verified as such before permitting theemergency response personnel access to Zone IV.For permanent, resistive, or hybrid systems whosemagnetic fields cannot be completely shut down,MR personnel should ideally be available to warnthe emergency response personnel that a verypowerful magnetic field is still operational in themagnet room.
4. MR Personnel Screening
All MR personnel are to undergo an MR-screeningprocess as part of their employment interview processto ensure their safety in the MR environment. Fortheir own protection and for the protection of the non-MR personnel under their supervision, all MR person-nel must immediately report to the MR medical direc-tor any trauma, procedure, or surgery they experienceor undergo where a ferromagnetic object or devicemay have become introduced within or on them. Thiswill permit appropriate screening to be performed onthe employee to determine the safety of permittingthat employee into Zone III.
508 Kanal et al.
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 75
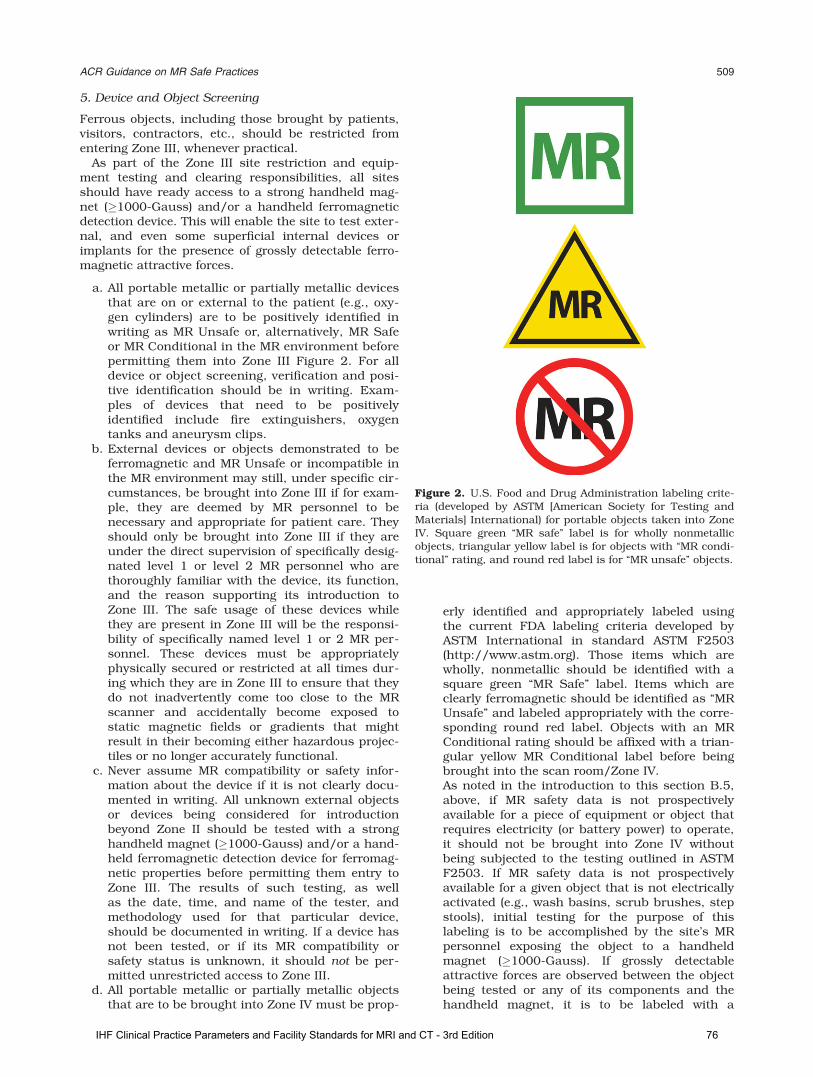
5. Device and Object Screening
Ferrous objects, including those brought by patients,visitors, contractors, etc., should be restricted fromentering Zone III, whenever practical.
As part of the Zone III site restriction and equip-ment testing and clearing responsibilities, all sitesshould have ready access to a strong handheld mag-net (�1000-Gauss) and/or a handheld ferromagneticdetection device. This will enable the site to test exter-nal, and even some superficial internal devices orimplants for the presence of grossly detectable ferro-magnetic attractive forces.
a. All portable metallic or partially metallic devicesthat are on or external to the patient (e.g., oxy-gen cylinders) are to be positively identified inwriting as MR Unsafe or, alternatively, MR Safeor MR Conditional in the MR environment beforepermitting them into Zone III Figure 2. For alldevice or object screening, verification and posi-tive identification should be in writing. Exam-ples of devices that need to be positivelyidentified include fire extinguishers, oxygentanks and aneurysm clips.
b. External devices or objects demonstrated to beferromagnetic and MR Unsafe or incompatible inthe MR environment may still, under specific cir-cumstances, be brought into Zone III if for exam-ple, they are deemed by MR personnel to benecessary and appropriate for patient care. Theyshould only be brought into Zone III if they areunder the direct supervision of specifically desig-nated level 1 or level 2 MR personnel who arethoroughly familiar with the device, its function,and the reason supporting its introduction toZone III. The safe usage of these devices whilethey are present in Zone III will be the responsi-bility of specifically named level 1 or 2 MR per-sonnel. These devices must be appropriatelyphysically secured or restricted at all times dur-ing which they are in Zone III to ensure that theydo not inadvertently come too close to the MRscanner and accidentally become exposed tostatic magnetic fields or gradients that mightresult in their becoming either hazardous projec-tiles or no longer accurately functional.
c. Never assume MR compatibility or safety infor-mation about the device if it is not clearly docu-mented in writing. All unknown external objectsor devices being considered for introductionbeyond Zone II should be tested with a stronghandheld magnet (�1000-Gauss) and/or a hand-held ferromagnetic detection device for ferromag-netic properties before permitting them entry toZone III. The results of such testing, as wellas the date, time, and name of the tester, andmethodology used for that particular device,should be documented in writing. If a device hasnot been tested, or if its MR compatibility orsafety status is unknown, it should not be per-mitted unrestricted access to Zone III.
d. All portable metallic or partially metallic objectsthat are to be brought into Zone IV must be prop-
erly identified and appropriately labeled usingthe current FDA labeling criteria developed byASTM International in standard ASTM F2503(http://www.astm.org). Those items which arewholly, nonmetallic should be identified with asquare green ‘‘MR Safe’’ label. Items which areclearly ferromagnetic should be identified as ‘‘MRUnsafe’’ and labeled appropriately with the corre-sponding round red label. Objects with an MRConditional rating should be affixed with a trian-gular yellow MR Conditional label before beingbrought into the scan room/Zone IV.As noted in the introduction to this section B.5,above, if MR safety data is not prospectivelyavailable for a piece of equipment or object thatrequires electricity (or battery power) to operate,it should not be brought into Zone IV withoutbeing subjected to the testing outlined in ASTMF2503. If MR safety data is not prospectivelyavailable for a given object that is not electricallyactivated (e.g., wash basins, scrub brushes, stepstools), initial testing for the purpose of thislabeling is to be accomplished by the site’s MRpersonnel exposing the object to a handheldmagnet (�1000-Gauss). If grossly detectableattractive forces are observed between the objectbeing tested or any of its components and thehandheld magnet, it is to be labeled with a
Figure 2. U.S. Food and Drug Administration labeling crite-ria (developed by ASTM [American Society for Testing andMaterials] International) for portable objects taken into ZoneIV. Square green ‘‘MR safe’’ label is for wholly nonmetallicobjects, triangular yellow label is for objects with ‘‘MR condi-tional’’ rating, and round red label is for ‘‘MR unsafe’’ objects.
ACR Guidance on MR Safe Practices 509
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 76

circular red ‘‘MR Unsafe’’ label. If no attractiveforces are observed, a triangular yellow ‘‘MR Con-ditional’’ label is to be attached to the object. It isonly when the composition of an object and itscomponents are known to be nonmetallic andnot electrically conductive that the green ‘‘MRSafe’’ label is to be affixed to a device or object.Particularly with regard to nonclinical and inci-dental equipment, current products marketedwith ill-defined terminology such as ‘‘nonmag-netic’’, or outdated classifications such as ‘‘MRcompatible’’, should not be presumed to conformto a particular current ASTM classification. Simi-larly, any product marketed as ‘‘MR safe’’ butwith metallic construction or components shouldbe treated with suspicion. Objects intended foruse in Zone IV, including nonclinical incidentalproducts such as stepping stools or ladders,which are not accompanied by manufacturer orthird-party MR safety test results under theASTM F2503 criteria, should be site tested asdescribed above.
e. Decisions based on published MR compatibilityor safety claims should recognize that all suchclaims apply to specifically tested static field andstatic gradient field, strengths and only to theprecise model, make, and identification of thetested object. For example, ‘‘MR Conditional hav-ing been tested to be safe at 3.0 Tesla at gradientstrengths of 400-G/cm or less and normal oper-ating mode.’’,
f. It should be noted that alterations performed bythe site on MR Safe, MR Unsafe, and MR Condi-tional equipment or devices may alter the MRsafety or compatibility properties of the device.For example, tying a ferromagnetic metallic twist-ing binder onto a sign labeling the device as MRConditional or MR Safe might result in artifactinduction – or worse – if introduced into the MRscanner.
Lenz’s Forces:
Faraday’s Law states that a moving or changing mag-netic field will induce a voltage in a perpendicularlyoriented electrical conductor. Lenz’s Law builds uponthis and states that the induced voltage will itself besuch that it will secondarily generate its own magneticfield whose orientation and magnitude will opposethat of the initial time varying magnetic field that cre-ated it in the first place. For example, if an electricalconductor is moved perpendicularly toward the mag-netic field B0 of an MR scanner, even if this conductoris not grossly ferromagnetic, the motion itself willresult in the generation of voltages within this con-ductor whose magnitude is directly proportional tothe rate of motion as well as the spatial gradient ofmagnetic field B0 through which it is being moved.Conducting objects turning in the static field will alsoexperience a torque due to the induced eddy currents.Lenz’s law states that this induced current will inturn create a magnetic field whose orientation will
oppose the B0 magnetic field that created thiscurrent.
Thus, moving a large metallic but nonferromagneticelectrical conductor toward the magnet bore willresult in the induction of a voltage and associatedmagnetic field which will orient in such a manner andat such a strength to oppose the motion of the metal-lic object into the bore of the MR scanner. If, for exam-ple, one tries to move a nonferrous oxygen tank intothe bore of an MR scanner, as the scanner bore isapproached Lenz’s forces will be sufficiently strong tovirtually stop forward progress of the tank. Further-more, the faster one moves the tank into the bore, thegreater the opposing force that is created to stop thismotion.
This also has potential consequence for largeimplanted metallic devices such as certain metallicnonferrous infusion pumps. Although they may notpose a projectile hazard, rapid motion of the patient/implant perpendicular to the magnetic field of the MRimager can be expected to result in forces on theimplant that would oppose this motion and may likelybe detected by the patient. If the patient were to com-plain of experiencing forces tugging or pulling on theimplant, this might bring the patient or health carepersonnel to erroneously conclude that there wereferrous components to the device, and possible can-cellation of the examination. Slowly moving such largemetallic devices into and out of the bore is a keyfactor in decreasing any Lenz’s forces that might beinduced, and decrease the likelihood of a misunder-standing or unnecessary study cancellation.
C. MR Technologist
1. MR technologists should be in compliance withthe technologist qualifications listed in the MRAccreditation Program Requirements.
2. Except for emergent coverage, there will be aminimum of 2 MR technologists or one MR tech-nologist and one other individual with the desig-nation of MR personnel in the immediate Zone IIthrough Zone IV MR environment. For emergentcoverage, the MR technologist can scan with noother individuals in their Zone II through Zone IVenvironment as long as there is in-house, readyemergent coverage by designated department ofradiology MR personnel (e.g., radiology housestaff or radiology attending).
D. Pregnancy Related Issues
1. Health Care Practitioner Pregnancies:
Pregnant health care practitioners are permitted towork in and around the MR environment throughoutall stages of their pregnancy (13). Acceptable activitiesinclude, but are not limited to, positioning patients,scanning, archiving, injecting contrast, and enteringthe MR scan room in response to an emergency.Although permitted to work in and around the MRenvironment, pregnant health care practitioners are
510 Kanal et al.
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 77
requested not to remain within the MR scannerbore or Zone IV during actual data acquisition orscanning.
2. Patient Pregnancies
Present data have not conclusively documented anydeleterious effects of MR imaging exposure on thedeveloping fetus. Therefore no special consideration isrecommended for the first, versus any other, trimesterin pregnancy. Nevertheless, as with all interventionsduring pregnancy, it is prudent to screen females ofreproductive age for pregnancy before permittingthem access to MR imaging environments. If preg-nancy is established consideration should be given toreassessing the potential risks versus benefits of thepending study in determining whether the requestedMR examination could safely wait to the end of thepregnancy before being performed.
a. Pregnant patients can be accepted to undergo MRscans at any stage of pregnancy if, in the determi-nation of a level 2 MR personnel-designated attend-ing radiologist, the risk–benefit ratio to the patientwarrants that the study be performed. The radiol-ogist should confer with the referring physicianand document the following in the radiology reportor the patient’s medical record:1. The information requested from the MR study
cannot be acquired by means of nonionizingmeans (e.g., ultrasonography).
2. The data is needed to potentially affect the careof the patient or fetus during the pregnancy.
3. The referring physician believes that it is notprudent to wait until the patient is no longerpregnant to obtain this data.
b. MR contrast agents should not be routinely pro-vided to pregnant patients. This decision too, is onthat must be made on a case-by-case basis by thecovering level 2 MR personnel-designated attendingradiologist who will assess the risk–benefit ratio forthat particular patient.The decision to administer a gadolinium-based MRcontrast agent to pregnant patients should beaccompanied by a well-documented and thoughtfulrisk–benefit analysis. This analysis should be ableto defend a decision to administer the contrastagent based on overwhelming potential benefit tothe patient or fetus outweighing the theoretical butpotentially real risks of long-term exposure of thedeveloping fetus to free gadolinium ions.Studies have demonstrated that at least some ofthe gadolinium-based MR contrast agents readilypass through the placental barrier and enter the fe-tal circulation. From here, they are filtered in thefetal kidneys and then excreted into the amnioticfluid. In this location the gadolinium-chelate mole-cules are in a relatively protected space and mayremain in this amniotic fluid for an indeterminateamount of time before finally being reabsorbed andeliminated. As with any equilibrium situationinvolving any dissociation constant, the longer thechelated molecule remains in this space, thegreater the potential for dissociation of the poten-
tially toxic gadolinium ion from its ligand. It isunclear what impact such free gadolinium ionsmight have if they were to be released in any quan-tity in the amniotic fluid. Certainly, deposition intothe developing fetus would raise concerns of possi-ble secondary adverse effects.The risk to the fetus of gadolinium based MR con-trast agent administration remains unknown andmay be harmful.
E. Pediatric MR Safety Concerns
1. Sedation and Monitoring Issues
Children form the largest group requiring sedation forMRI, largely because of their inability to remainmotionless during scans. Sedation protocols may varyfrom institution to institution according to proceduresperformed (diagnostic vs. interventional), the complex-ity of the patient population (healthy preschoolers vs.premature infants), the method of sedation (mildsedation vs. general anesthesia) and the qualificationsof the sedation provider.
Adherence to standards of care mandates followingthe sedation guidelines developed by the AmericanAcademy of Pediatrics (14,15), the American Societyof Anesthesiologists (16), and the Joint Commissionon Accreditation of Healthcare Organizations (17). Inaddition, sedation providers must comply withprotocols established by the individual state and thepracticing institution. These guidelines require the fol-lowing provisions:
a. Preprocedural medical history and examinationfor each patient
b. Fasting guidelines appropriate for agec. Uniform training and credentialing for sedation
providersd. Intraprocedural and post procedural monitors
with adaptors appropriately sized for children(MR Conditional equipment)
e. Method of patient observation (window, camera)f. Resuscitation equipment, including oxygen deliv-
ery and suctiong. Uniform system of record keeping and charting
(with continuous assessment and recording ofvital signs)
h. Location and protocol for recovery and dischargei. Quality assurance program that tracks complica-
tions and morbidity.
For the neonatal and the young pediatric population,special attention is needed in monitoring body temper-ature for both hypo- and hyperthermia in addition toother vital signs (18). Temperature monitoring equip-ment that is approved for use in the MR suite is readilyavailable. Commercially available, MR-approved neo-natal isolation transport units and other warming devi-ces are also available for use during MR scans.
2. Pediatric Screening Issues
Children may not be reliable historians and, espe-cially for older children and teenagers, should be
ACR Guidance on MR Safe Practices 511
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 78

questioned both in the presence of parents or guardi-ans and separately to maximize the possibility that allpotential dangers are disclosed. Therefore, it is recom-mended that they be gowned before entering Zone IVto help ensure that no metallic objects, toys, etc. inad-vertently find their way into Zone IV. Pillows, stuffedanimals, and other comfort items brought from homerepresent real risks and should be discouraged fromentering Zone IV. If unavoidable, each should be care-fully checked with a powerful handheld magnet and/or ferromagnetic detector and perhaps again in theMR scanner before permitting the patient to enterZone IV with them to ensure that they do not containany objectionable metallic components.
3. MR Safety of Accompanying Family or Personnel:
Although any age patient might request that othersaccompany them for their MR examination, this is farmore common in the pediatric population. Thoseaccompanying or remaining with the patient shouldbe screened using the same criteria as anyone elseentering Zone IV.
In general, it would be prudent to limit accompany-ing adults to a single individual. Only a qualified,responsible MR physician should make screeningcriteria exceptions.
Hearing protection and MR safe/MR conditionalseating are recommended for accompanying familymembers within the MR scan room.
F. Time Varying Gradient Magnetic Field RelatedIssues: Induced Voltages
Types of patients needing extra caution:
Patients with implanted or retained wires in anatomi-cally or functionally sensitive areas (e.g., myocardiumor epicardium, implanted electrodes in the brain)should be considered at higher risk, especially fromfaster MRI sequences, such as echo planar imaging(which may be used in such sequences as diffusion-weighted imaging, functional imaging, perfusionweighted imaging, MR angiographic imaging, etc.).The decision to limit the dB/dt (rate of magnetic fieldchange) and maximum strength of the magnetic fieldof the gradient subsystems during imaging of suchpatients should be reviewed by the level 2 MR person-nel-designated attending radiologist supervising thecase or patient.
G. Time Varying Gradient Magnetic Field RelatedIssues: Auditory Considerations
1. All patients and volunteers should be offered andencouraged to use hearing protection beforeundergoing any imaging in any MR scanners.FDA’s current MR Guidance Document (Attach-ment B entitled, ‘‘Recommended User Instruc-tions for a Magnetic Resonance DiagnosticDevice’’) states that instructions from manufac-turers of MR equipment should state that hear-ing protection is required for all patients studiedon MR imaging systems capable of producing
sound pressures that exceed 99 dB(A). The Inter-national standard on this issue (IEC 60601-2-33:‘‘Particular requirements for the basic safety andessential performance of magnetic resonanceequipment for medical diagnosis’’), also statesthat, for all equipment capable of producingmore than an A-weighted rms sound pressurelevel of 99dB(A), hearing protection shall be usedfor the safety of the patient and that this hearingprotection shall be sufficient to reduce the A-weighted r.m.s. sound pressure level to below 99dB(A).
2. All patients or volunteers in whom researchsequences are to be performed (i.e., MR scansequences that have not yet been approved bythe Food and Drug Administration) are to havehearing protective devices in place before initiat-ing any MR sequences. Without hearing protec-tion in place, MRI sequences that are not FDAapproved should not be performed on patients orvolunteers.
H. Time Varying Radiofrequency Magnetic FieldRelated Issues: Thermal
1. All unnecessary or unused electrically conductivematerials external to the patient should beremoved from the MR system before the onset ofimaging. It is not sufficient to merely to ‘‘unplug’’or disconnect unused, unnecessary electricallyconductive material and leave it within the MRscanner with the patient during imaging. All elec-trical connections, such as on surface coil leadsor monitoring devices must be visually checkedby the scanning MR technologist before eachusage to ensure the integrity of the thermal andelectrical insulation.
2. Electrical voltages and currents can be inducedwithin electrically conductive materials that arewithin the bore of the MR imager during the MRimaging process. This might result in the heatingof this material by resistive losses. This heatmight be of a caliber sufficient to cause injury tohuman tissue. As noted in section H.9, among thevariables that determine the amount of inducedvoltage or current is the consideration that thelarger the diameter of the conductive loops thegreater the potential induced voltages or currentsand, thus the greater the potential for resultantthermal injury to adjacent or contiguous patienttissue.Therefore, when electrically conductive material(wires, leads, implants, etc.), are required toremain within the bore of the MR scanner withthe patient during imaging, care should be takento ensure that no large-caliber electrically con-ducting loops (including patient tissue; see sec-tion H. 5, below) are formed within the MRscanner during imaging. Furthermore, it is possi-ble, with the appropriate configuration, leadlength, static magnetic field strength, and othersettings, to introduce resonant circuitry between
512 Kanal et al.
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 79
the transmitted RF power and the lead. This couldresult in very rapid and clinically significant leadheating, especially at the lead tips, in a matter ofseconds to a magnitude sufficient to result in tis-sue thermal injury or burns. This can also theo-retically occur with implanted leads or wires evenwhen they are not connected to any other deviceat either end. For illustration, the FDA has notedseveral reports of serious injury including comaand permanent neurological impairment inpatients with implanted neurological stimulatorswho underwent MR imaging examinations. Theinjuries in these instances resulted from heatingof the electrode tips (19,20).Furthermore, it is entirely possible for a lead orwire to demonstrate no significant heating whileundergoing MR imaging examinations at 1.5 Teslayet demonstrate clinically significant and poten-tially harmful degrees of heating within secondsat, for example, 3 Tesla. It has also been demon-strated that leads may demonstrate no significantheating at 3 Tesla yet may rapidly heat to hazard-ous levels when undergoing MR imaging at, forexample, 1.5 Tesla. (Personal Observation, MRSafety testing, E. Kanal, MD, University of Pitts-burgh Medical Center MR Research Center, 8/28/05) Thus at no time should a label of MR Condi-tional for thermal issues at a given field strengthbe applied to any field strength, higher or lower,other than the specific one at which safety wasdemonstrated.Thus, exposure of electrically conductive leads orwires to the RF transmitted power during MRscanning should only be performed with cautionand with appropriate steps taken to ensure signif-icant lead or tissue heating does not result (seesection H.9, below).
3. When electrically conductive materials external tothe patient are required to be within the bore ofthe MR scanner with the patient during imaging,care should be taken to place thermal insulation(including air, pads, etc.) between the patient andthe electrically conductive material, while simulta-neously attempting to (as much as feasible) keepthe electrical conductor from directly contactingthe patient during imaging. It is also appropriateto try to position the leads or wires as far as pos-sible from the inner walls of the MR scanner if thebody coil is being used for RF transmission. Whenit is necessary that electrically conductive leadsdirectly contact the patient during imaging, con-sideration should be given to prophylactic appli-cation of cold compresses or ice packs to suchareas.
4. There have been rare reports of thermal injuries/burns associated with clothing that containedelectrically conductive materials, such as metallicthreads, electrically conductive designs, and silverimpregnated clothing. As such, considerationshould be given to having all patients removetheir own clothing and instead change into pro-vided gowns to cover at the very least the region/volume of the patient that is scheduled to undergo
MR imaging and, therefore, RF irradiation.5. To help safeguard against thermal injuries or
burns, depending on specific magnet designs,care may be needed to ensure that the patient’stissue(s) do not directly come into contact withthe inner bore of the MR imager during the MRIprocess. This is especially important for severalhigher field MR scanners. The manufacturers ofthese devices provide pads and other such insu-lating devices for this purpose, and manufacturerguidelines should be strictly adhered to for theseunits.
6. It is important to ensure the patient’s tissues donot form large conductive loops. Therefore, careshould be taken to ensure that the patient’s armsor legs are not positioned in such a way as toform a large caliber loop within the bore of theMR imager during the imaging process. For thisreason, it is preferable that patients be instructednot to cross their arms or legs in the MR scanner.We are also aware of unpublished reports of ther-mal injury that seem to have been associated withskin-to-skin contact such as in the region of theinner thighs. It might be prudent to considerensuring that skin-to-skin contact instances areminimized or eliminated in or near the regionsundergoing radiofrequency energy irradiation.
7. Skin staples and superficial metallic sutures:Patients requested to undergo MR studies inwhom there are skin staples or superficial metal-lic sutures (SMS) may be permitted to undergothe MR examination if the skin staples or SMSare not ferromagnetic and are not in or near theanatomic volume of RF power deposition for thestudy to be performed. If the nonferromagneticskin staples or SMS are within the volume to beRF irradiated for the requested MR study, severalprecautions are recommended.a. Warn the patient and make sure that they are
especially aware of the possibility that theymay experience warmth or even burning alongthe skin staple or SMS distribution. Thepatient should be instructed to report immedi-ately if they experience warmth or burningsensations during the study (and not, forexample, wait until the ‘‘end of the knockingnoise’’).
b. It is recommended that a cold compress or icepack be placed along the skin staples or SMS ifthis can be safely clinically accomplished dur-ing the MRI examination. This will help to serveas a heat sink for any focal power depositionthat may occur, thus decreasing the likelihoodof a clinically significant thermal injury or burnto adjacent tissue.
8. For patients with extensive or dark tattoos,including tattooed eyeliner, to decrease the poten-tial for RF heating of the tattooed tissue, it is rec-ommended that cold compresses or ice packs beplaced on the tattooed areas and kept in placethroughout the MRI process if these tattoos arewithin the volume in which the body coil is beingused for RF transmission. This approach is
ACR Guidance on MR Safe Practices 513
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 80

especially appropriate if fast spin echo (or otherhigh RF duty cycle) MRI sequences are antici-pated in the study. If another coil is being usedfor RF transmission, a decision must be made ifhigh RF transmitted power is to be anticipated bythe study protocol design. If so, then the aboveprecautions should be followed. Additionally,patients with tattoos that had been placed within48 h before the pending MR examination shouldbe advised of the potential for smearing or smudg-ing of the edges of the freshly placed tattoo.
9. The unconscious or unresponsive patient shouldhave all attached leads covered with a cold com-press or ice pack at the lead attachment site forthe duration of the MR study.
10. As noted above, it has been demonstrated thatresonant circuitry can be established during MRIbetween the RF energies being transmitted andspecific lengths of long electrically conductivewires or leads, which can thus act as efficientantennae. This can result in heating of the tips ofthese wires or leads to temperatures in excess of90� C in a few seconds. Therefore, patients inwhom there are long electrically conductive leads,such as Swan-Ganz thermodilution cardiac out-put capable catheters or Foley catheters with elec-trically conductive leads as well as electricallyactive implants containing leads such as pace-makers, ICDs, neurostimulators, and cochlearimplants, let alone electrically active implant suchas pacemakers,, should be considered at risk forMR studies if the body coil is to be used for RFtransmission over the region of the electricallyconductive lead, even if only part of the lead path-way is within the volume to undergo RF irradia-tion. This is especially true for higher-fieldsystems (e.g., greater than 0.5 T) and for imagingprotocols using fast spin echo or other high-RFduty cycle MRI sequences. Each such patientshould be reviewed and cleared by an attendinglevel 2 radiologist and a risk benefit ratio assess-ment performed before permitting them access tothe MR scanner.
11. The potential to establish substantial heating isitself dependent upon multiple factors, including,among others, the static magnetic field strength ofthe MR scanner (as this determines the transmit-ted radiofrequencies (RF) at which the device oper-ates) and the length, orientation, and inductanceof the electrical conductor in the RF irradiatedvolume being studied. Virtually any lead lengthscan produce substantial heating. Innumerable fac-tors can affect the potential for tissue heating forany given lead. It is therefore critical to recognizethat of all electrically conductive implants, it isspecifically wires, or leads, that pose the greatestpotential hazard for establishing substantialpower deposition/heating considerations.Another important consideration is that as a directresult of the above, it has already been demon-strated in vitro that heating of certain implants orwires may be clinically insignificant at, for example,1.5 Tesla but quite significant at 3.0 Tesla. How-
ever, it has also been demonstrated that specificimplants might demonstrate no significant thermalissues or heating at 3.0 Tesla, but may heat to clini-cally significant or very significant levels in secondsat, for example, 1.5 Tesla. Thus, it is important tofollow established product MR Conditional labelingand safety guidelines carefully and precisely, apply-ing them to and only to the static magnetic fieldstrengths at which they had been tested. MR scan-ning at either stronger and/or weaker magneticfield strengths than those tested may result in sig-nificant heating where none had been observed atthe tested field strength(s).
I. Drug Delivery Patches and Pads
Some drug delivery patches contain metallic foil.Scanning the region of the metallic foil may result inthermal injury (21). Because removal or repositioningcan result in altering of patient dose, consultationwith the patient’s prescribing physician would be indi-cated in assessing how to best manage the patient. Ifthe metallic foil of the patch delivery system ispositioned on the patient so that it is in the volume ofexcitation of the transmitting RF coil, the case shouldbe specifically reviewed with the radiologist or physi-cian covering the case. Alternative options mayinclude placing an ice pack directly on the patch. Thissolution may still substantially alter the rate ofdelivery or absorption of the medication to the patient(and be less comfortable to the patient, as well). Thisramification should therefore not be treated lightly,and a decision to proceed in this manner should bemade by a knowledgeable radiologist attendingthe patient and with the concurrence of the referringphysician as well.
If the patch is removed, a specific staff membershould be given responsibility for ensuring that it isreplaced or repositioned at the conclusion of the MRexamination.
J. Cryogen-Related Issues
1. For superconducting systems, in the event of asystem quench, it is imperative that all personneland patients be evacuated from the MR scanroom as quickly as safely feasible and the siteaccess be immediately restricted to all individu-als until the arrival of MR equipment servicepersonnel. This is especially so if cryogenic gasesare observed to have vented partially or com-pletely into the scan room, as evidenced in partby the sudden appearance of white ‘‘clouds’’ or‘‘fog’’ around or above the MR scanner. As notedin section B.3.n above, it is especially importantto ensure that all police and fire responsepersonnel are restricted from entering the MRscan room with their equipment (axes, air tanks,guns, etc.) until it can be confirmed that themagnetic field has been successfully dissipated,as there may still be considerable static magneticfield present despite a quench or partial quench
514 Kanal et al.
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 81

of the magnet (22).2. It should be pointed out that room oxygen moni-
toring was discussed by the MR Blue RibbonPanel and rejected at this time because the pres-ent oxygen monitoring technology was consideredby industry experts not to be sufficiently reliableto allow for continued operation during situa-tions of power outages, etc.
K. Claustrophobia, Anxiety, Sedation, Analgesiaand Anesthesia
Adult and pediatric patient anxiolysis, sedation, anal-gesia, and anesthesia for any reason should followestablished ACR (23), American Society of Anesthesi-ologists (ASA) (15,24–26), and TJC standards (17).
L. Contrast Agent Safety
1. Contrast agent administration issues:
No patient is to be administered prescription MRcontrast agents without orders from a duly licensedphysician. Intravenous injection-qualified MR technol-ogists may start and attend to peripheral IV accesslines if they have undergone the requisite site-speci-fied training in peripheral IV access and have demon-strated and documented appropriate proficiency inthis area. IV-qualified MR technologists may adminis-ter FDA-approved gadolinium-based MR contrastagents by means of peripheral IV routes as a bolus orslow or continuous injection as directed by the ordersof a duly licensed site physician.
Administration of these agents is to be performed asper the ACR policy. The ACR approves of the injectionof contrast material and diagnostic levels of radio-pharmaceuticals by certified and/or licensed radio-logic technologists and radiologic nurses under thedirection of a radiologist or his or her physician desig-nee who is personally and immediately available, ifthe practice is in compliance with institutional andstate regulations. There must also be prior writtenapproval by the medical director of the radiologydepartment/service of such individuals. Such ap-proval process must follow established policies andprocedures, and the radiologic technologists andnurses who have been so approved must maintaindocumentation of continuing medical educationrelated to materials injected and to the proceduresbeing performed (27).
The name of the administered contrast agent, theadministered dose, and the route (and, if applicable,rate) of administration as well as any adverse reac-tions, if any, should be recorded for all contrastagents administered as part of the executed MRexamination.
2. Prior Contrast Agent Reaction Issues:
a. According to the ACR Manual on Contrast Media(28) adverse events after intravenous injection ofgadolinium seem to be more common in patientswho had previous reactions to an MR contrast
agent. In one study, 16 (21%) of 75 patients whohad previous adverse reactions to MR contrastagents reacted to subsequent injections of gado-linium. Patients with asthma also seem to bemore likely to have an adverse reaction to admin-istration of a gadolinium-based MR contrastagent. Patients with allergies also seemed to be atincreased risk (�2.0–3.7 times, compared withpatients without allergies). Patients who have hadadverse reactions to iodinated contrast media aremore than twice as likely to have an adverse reac-tion to gadolinium (6.3% of 857 patients).
b. At present, there are no well-defined policiesfor patients who are considered to be atincreased risk for having adverse reaction toMR contrast agents. However, the followingrecommendations are suggested: patients whohave previously reacted to one MR contrastagent can be injected with another agent if theyare restudied, and at-risk patients can be pre-medicated with corticosteroids and, occasion-ally, antihistamines.
c. All patients with asthma, allergic respiratoryhistories, prior iodinated or gadolinium-basedcontrast reactions, etc. should be followed moreclosely as they are at a demonstrably higher riskof adverse reaction.
3. Severe Renal Disease, Gadolinium-Based MRContrast Agents, and Nephrogenic FibrosingDermopathy/Nephrogenic Systemic Fibrosis(NFD/NSF)
Since the prior version of this document the ACRdecided that MR safety issues related to gadoliniumbased contrast agents (GBCA) and NSF would be thepurview of the ACR Committee on Drugs and ContrastMedia. For the recommendations of the ACR Commit-tee on Drugs and Contrast Media regarding GBCAand NSF, the reader is referred to the most recentpublication of that committee in this regard whichappears in the ACR Manual on Contrast Media, Ver-sion 8, Chapter 13, Nephrogenic Systemic Fibrosis.The most recent version of the ACR Manual on Con-trast Media may be downloaded from the AmericanCollege of Radiology website at http://www.acr.org/Quality-Safety/Resources.
M. Patients in Whom There Are or May BeIntracranial Aneurysm Clips
1. In the event that it is unclear whether a patientdoes or does not have an aneurysm clip in place,plain films should be obtained. Alternatively, ifavailable, any cranial plain films, CT or MRexamination that may have taken in the recentpast (i.e., subsequent to the suspected surgicaldate) should be reviewed to assess for a possibleintracranial aneurysm clip.
2. In the event that a patient is identified to have anintracranial aneurysm clip in place, the MR ex-amination should not be performed until it canbe documented that the specific manufacturer,
ACR Guidance on MR Safe Practices 515
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 82

model, and type of aneurysm clip within thatpatient is MR Safe or MR Conditional. Alldocumentation of types of implanted clips, dates,etc. must be in writing and signed by a licensedphysician. Phone or verbal histories and historiesprovided by a nonphysician are not acceptable.Fax copies of operative reports, physician state-ments, etc. are acceptable as long as a legiblephysician signature accompanies the requisitedocumentation. A written history of the clip itselfhaving been appropriately tested for ferromag-netic properties (and description of the testingmethodology used) before implantation by theoperating surgeon is also considered acceptableif the testing follows the standard test methodsestablished by ASTM International.
3. All intracranial aneurysm clips manufactured1995 or later for which the manufacturer’s prod-uct labeling continues to claim MR Conditionallabeling may be accepted for MR scanning with-out further testing.
4. Clips manufactured before 1995 require eitherpretesting (as per the ASTM F2503 standardpractice guidelines) before implantation or indi-vidual review of previous MRI of the clip or brainin that particular case, if available. By assessingthe size of the artifact associated with the cliprelative to the static field strength on which itwas studied, the sequence type, and the MRIparameters selected, an opinion may be issuedby one of the site’s level 2 MR attending radiolog-ists as to whether the clip demonstrates signifi-cant ferromagnetic properties or not. Access tothe MR scanner would then be based on thatopinion.
5. A patient with an aneurysm clip (or otherimplant) may have safely undergone a prior MRexamination at any given static magnetic fieldstrength. This fact in and of itself is not sufficientevidence of the implant’s MR safety and shouldnot solely be relied upon to determine the MRsafety or compatibility status of that aneurysmclip (or other implant).Variations in static magnetic field strength, staticmagnetic field spatial gradient, orientation of theaneurysm clip (or other implant) to the staticmagnetic field or static field gradient, rate ofmotion through the spatial static field gradient,etc. are all variables that are virtually impossibleto control or reproduce. These variables may nothave resulted in adverse event in one circum-stance but may result in significant injury ordeath on a subsequent exposure. For example, apatient who went blind from interactions betweenthe metallic foreign body in his retina and thespatial static fields of the MR scanner enteredthe magnet and underwent the entire MR exami-nation without difficulty; he only went blindupon exiting the MR scanner at the completion ofthe examination.
6. Barring availability of either pretesting or priorMRI data of the clip in question, a risk–benefitassessment and review must be performed in
each case individually. Furthermore, forpatients with intracranial clips with no availableferromagnetic or imaging data, should the risk–benefit ratio favor the performance of the MRstudy, the patient or guardian should providewritten informed consent that includes death asa potential risk of the MRI procedure before per-mitting that patient to undergo an MRexamination.
N. Patients in Whom There are or May BeCardiac Pacemakers or ImplantableCardioverter Defibrillators
MRI of Cardiac Implantable Devices
Background: Cardiac implantable electronic devices(CIEDs) have expanded in number and complexitysince their introduction in 1958 and now include car-diac pacemakers, implantable cardioverter-defibrilla-tors (ICD), implantable cardiovascular monitors (ICM)and implantable loop recorders (ILR). Pacemakers(pulse generators) and leads that are FDA labeled MRconditional became available in the U.S., February of2011 and both commercially available ILRs arelabeled also ‘‘MR Conditional’’ The vast majority ofCIEDs, however, are not labeled as MR Conditional.No ICDs are currently labeled ‘‘MR Conditional’’ andnone are expected to be clinically available for severalyears. Patient product wallet identification cards,industry maintained databases, plain film lead andpulse generator X-ray identifiers, and operative notesmay assist in identification of MR Conditional patienthardware.
Radiologists and cardiovascular specialists must befamiliar with restrictions for each device, recognizingthat because each MR conditional device is unique,there are no ‘‘universal’’ labeling guidelines that areapplicable for all. Failure to follow the product label-ing for a particular device is ‘‘off-label’’ and couldresult in an adverse event.
Potential Complications: Unexpected programmingchanges, inhibition of pacemaker output, failure topace, transient asynchronous pacing, rapid cardiacpacing, the induction of ventricular fibrillation, heat-ing of the tissue adjacent to the pacing or ICD systemand especially cardiac tissue near the lead tip, earlybattery depletion, and outright device failure requiringreplacement may occur during MRI of patients withpacemakers or ICDs (18,29–31). Multiple deaths havebeen documented to occur under poorly and incom-pletely characterized circumstances when CIEDpatients underwent MRI (32–34). These deaths mayhave occurred as a result of pacemaker inhibition,failure to capture or device failure (resulting in pro-longed asystole) and or rapid cardiac pacing or asyn-chronous pacing (resulting in the initiation of ventric-ular tachycardia or fibrillation).
Patient Assessment: Most CIEDs can be viewed ashaving a pacing or defibrillator ‘‘system’’ comprised ofa pulse generator and one or more leads. Currentinsertable loop recorders are leadless and are formonitoring (not therapeutic) purposes alone.
516 Kanal et al.
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 83

Importantly, leads and occasionally pulse generatorsmay have been ‘‘abandoned’’ in the patient from previ-ous implants. As such, each patient may have a ‘‘sys-tem’’ that includes both active and inactive (aban-doned) hardware. While electrically andtherapeutically inactive with regard to pacing func-tionality outside the MR suite, abandoned hardwaremay pose a substantial risk if exposed to MRI energiesirrespective of the MR compatibility of the active pac-ing hardware (35). Indeed, abandoned leads may wellpose a greater relative risk of lead tip heating ifexposed to the MR imaging process than leads thatare part of an actively implanted system.
The experience with MR imaging in patients whohave retained metallic materials after cardiac surgerysuch as epicardial pacing leads is perhaps helpful(36). While some have produced survey data suggest-ing that in the case of postoperatively retained cardiacpacing wires, ‘‘the absence of reported complicationsin thousands of exposed patients suggests that therisk is low (37), others have voiced appropriate con-cern as to the general relevance of this data to theoverall population (38).’’
Patient Assessment for MRI
All device hardware should be included in the practi-tioner’s assessment of the patient’s suitability for MRscanning. Coordination with the physician managingthe device (cardiologist/electrophysiologist) and arepresentative from the device manufacturer is ofparamount importance to determine whether thesystem (pulse generator and leads) is MR Condi-tional. Practitioners and their staff should note thatthe entire system (pulse generator and leads) mustbe labeled ‘‘MR Conditional’’ for a system to in factbe considered MR conditionally safe. Furthermore,an MR Conditional system is only considered safe ifall of the MR conditions for safe use are followed.The presence of abandoned leads from previous non-labeled systems or ‘‘mix-and-match’’ systems (com-bined MR Conditional labeled and nonlabeled hard-ware) renders the system as a whole MR Unsafe orat best ‘‘MR unknown’’. Importantly, because of thepotential for heating, an abandoned (unattached to apulse generator) MR Conditional lead should be con-sidered, and from a risk assessment point of view,treated as, MR Unsafe.
The patient’s attestations as to their device MR com-patibility is not sufficient to establish MR safety. Toprovide for the safest scanning experience, to mini-mize confusion and disappointment, to prevent delaysin diagnosis due to rescheduling, and to limit thepotential for throughput disruption in an alreadybusy MR schedule, we recommend the development ofinstitutional policies, protocols and care pathways forall patients with implantable rhythm devices irrespec-tive of their labeling. Careful, thoughtful advanceplanning and close collaboration between the radiol-ogy and cardiology staffs and the industry representa-tives of the device manufacturers will provide thegreatest likelihood for a consistent, safe experience.
Unlabeled Cardiac Devices: Amongst the patientswith MR unsafe CIEDs, many have conditions thatwould ordinarily be assessed with MRI. While manycan have their medical conditions managed withoutMRI, in some instances, specific clinical circumstan-ces may present compelling reasons for undergoingan MR examination (39). Should MRI be considered, itshould be evaluated on a case-by-case and site-by-site basis and only if the site is manned with individu-als with the appropriate radiology and cardiologyknowledge and expertise on hand.
The committee eschews the term ‘‘modern’’ whenreferring to a particular device, recognizing that alldevices not labeled for use in the MRI contain legacycomponents and designs that may not be resistant tothe forces and electromagnetic interference present inthe MRI suite. All devices, unless appropriately testedand labeled, should never be regarded as safe forMRI simply because they are ‘‘modern’’ or recentlymanufactured.
Consent: The patient with a pacemaker or ICD thatis not labeled as MR Conditional should be apprisedof the risks associated with MRI and should provideinformed consent. While the majority of reporteddeliberate scans of device patients have proceededwithout adverse effects when appropriate precau-tions were undertaken, several have not, and thereis under-reporting of adverse events, includingdeaths. Thus, assignment of a risk benefit ratio tothe performance of MRI in any given device patientis difficult. While the risk may be low, patients withdevices that are not labeled as MR Conditionalshould be advised that life-threatening arrhythmiasmight occur during MRI and serious device malfunc-tion might occur requiring replacement of the device.
Precautions during MRI with CIEDs: Should any MRIexamination be contemplated for a patient with animplanted pacemaker or ICD, it is recommended thatradiology and cardiology personnel and a fully stockedcrash cart be readily available throughout the proce-dure in case a significant arrhythmia develops duringthe examination that does not terminate with thecessation of the MR study. The cardiologist should befamiliar with the patient’s arrhythmia history and theimplanted device. A programmer that can be used toadjust the device should be readily available. The goalof pre-MRI programming should be to mitigate therisk to the patient and the device while undergoingMRI (40,41). All such patients should be activelymonitored throughout the examination. A centralmonitoring facility located in the hospital with appro-priately trained staff may be sufficient to monitorappropriately selected low risk device patients under-going MR scanning.
At a minimum, EKG and pulse oximetry should beused for monitoring these patients. At the conclusionof the examination, the device should be interrogatedto confirm that the function is consistent withthe pre-examination state. In the absence of detectedpost MR anomalies, the value of repeating devicere-evaluation is controversial. However, the clinicianmay recommend a post-scan follow-up check of thepatient’s device (1–6 weeks) following the scan to
ACR Guidance on MR Safe Practices 517
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 84

confirm appropriate function. For appropriatelyselected patients who have no post-MRI device abnor-malities demonstrated, remote follow-up throughhome monitoring seems appropriate. There is no com-pelling evidence that post MRI defibrillation thresholdtesting is required if the MR-exposed ICD shows nopost MRI anomalies (42).
Should an MRI (or entry into the magnet area) beperformed inadvertently on a patient with a pace-maker or ICD, the patient’s cardiologist should becontacted before the patient’s discharge from the MRIsuite. Exposure to the static magnetic field alone mayadversely affect device function or alter its program-ming (43–45). The importance of interrogation of thedevice before the patient’s leaving the MRI suite can-not be overstated.
APPENDIX 1
Personnel Definitions
Non-MR Personnel
Patients, visitors or facility staff who do not meet thecriteria of level 1 or level 2 MR personnel will bereferred to as non-MR personnel. Specifically, non-MRpersonnel will be the terminology used to refer to anyindividual or group who has not within the previous12 months undergone the designated formal trainingin MR safety issues defined by the MR safety directorof that installation.
Level 1 MR Personnel
Individuals who have passed minimal safety educa-tional efforts to ensure their own safety as they workwithin Zone III will be referred to as level 1 MR per-sonnel (e.g., MRI department office staff, and patientaides.)
Level 2 MR Personnel
Individuals who have been more extensively trainedand educated in the broader aspects of MR safetyissues, including, issues related to the potential forthermal loading or burns and direct neuromuscularexcitation from rapidly changing gradients, will bereferred to as level 2 MR personnel (e.g., MRI technol-ogists, radiologists, radiology department nursingstaff.)
ZONE DEFINITIONS
Zone I
This region includes all areas that are freely accessi-ble to the general public. This area is typically outsidethe MR environment itself and is the area throughwhich patients, health care personnel, and otheremployees of the MR site access the MR environment.
Zone II
This area is the interface between the publicly acces-sible uncontrolled Zone I and the strictly controlledZone III (see below). Typically, the patients are greetedin Zone II and are not free to move throughout Zone IIat will, but rather are under the supervision of MRpersonnel. It is in Zone II that the answers to MRscreening questions, patient histories, medical insur-ance questions, etc. are typically obtained.
Zone III
This area is the region in which free access byunscreened non-MR personnel or ferromagneticobjects or equipment can result in serious injury ordeath as a result of interactions between the individu-als or equipment and the MR scanner’s particular envi-ronment. These interactions include, but are notlimited to, those with the MR scanner’s static and timevarying magnetic fields. All access to Zone III is to bestrictly physically restricted, with access to regionswithin it (including Zone IV; see below) controlled by,and entirely under the supervision of, MR personnel.
Zone IV
This area is synonymous with the MR scanner magnetroom itself. Zone IV, by definition, will always belocated within Zone III as it is the MR magnet and itsassociated magnetic field which generates the exis-tence of Zone III.
Non-MR Personnel should be accompanied by, orunder the immediate supervision of and visual con-tact with, one specifically identified level 2 MR personfor the entirety of their duration within Zone III or IVrestricted regions.
Level 1 and 2 MR personnel may move freely aboutall zones.
518 Kanal et al.
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 85
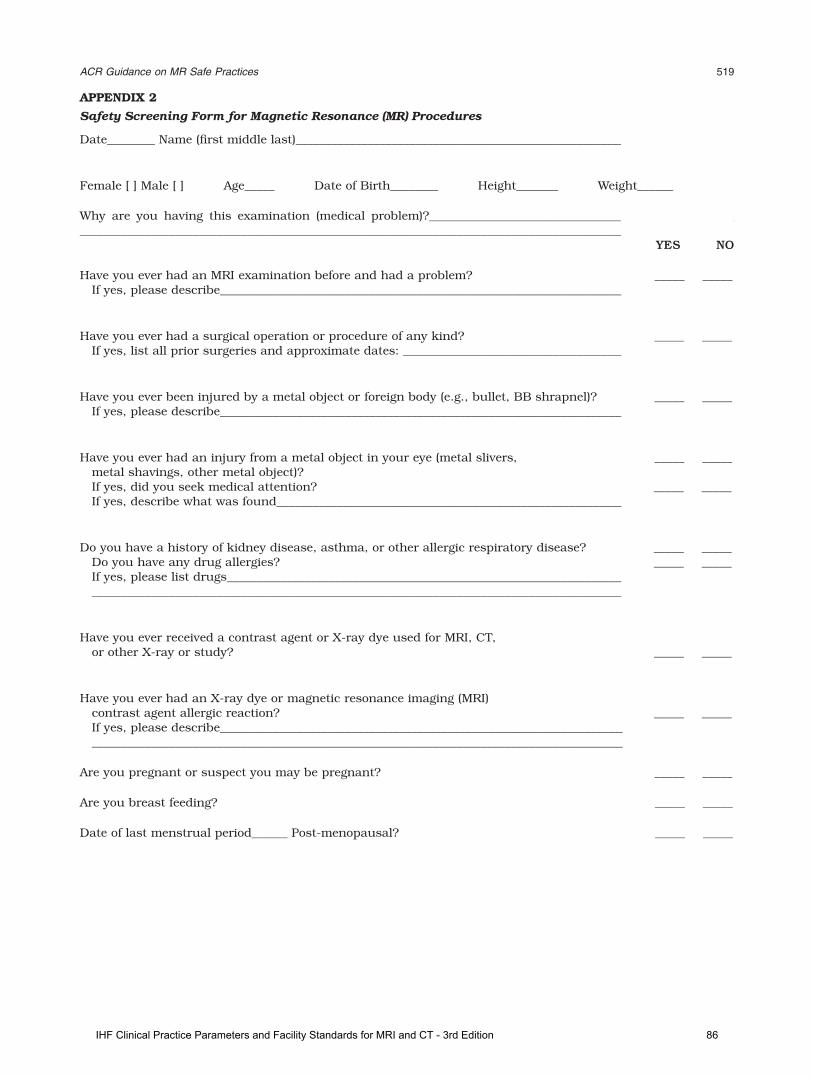
APPENDIX 2
Safety Screening Form for Magnetic Resonance (MR) Procedures
Date________ Name (first middle last)_________________________________________________________________________
Female [ ] Male [ ] Age_____ Date of Birth________ Height_______ Weight______
Why are you having this examination (medical problem)?________________________________________________________________________________________________________________________________________________________________
YES NO
Have you ever had an MRI examination before and had a problem? _____ _____If yes, please describe_____________________________________________________________________________________
Have you ever had a surgical operation or procedure of any kind? _____ _____If yes, list all prior surgeries and approximate dates: _______________________________________________________
Have you ever been injured by a metal object or foreign body (e.g., bullet, BB shrapnel)? _____ _____If yes, please describe_____________________________________________________________________________________
Have you ever had an injury from a metal object in your eye (metal slivers, _____ _____metal shavings, other metal object)?If yes, did you seek medical attention? _____ _____If yes, describe what was found__________________________________________________________
Do you have a history of kidney disease, asthma, or other allergic respiratory disease? _____ _____Do you have any drug allergies? _____ _____If yes, please list drugs_______________________________________________________________________________________________________________________________________________________________________________________________
Have you ever received a contrast agent or X-ray dye used for MRI, CT,or other X-ray or study? _____ _____
Have you ever had an X-ray dye or magnetic resonance imaging (MRI)contrast agent allergic reaction? _____ _____If yes, please describe________________________________________________________________________________________________________________________________________________________________________________________________
Are you pregnant or suspect you may be pregnant? _____ _____
Are you breast feeding? _____ _____
Date of last menstrual period______ Post-menopausal? _____ _____
ACR Guidance on MR Safe Practices 519
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 86
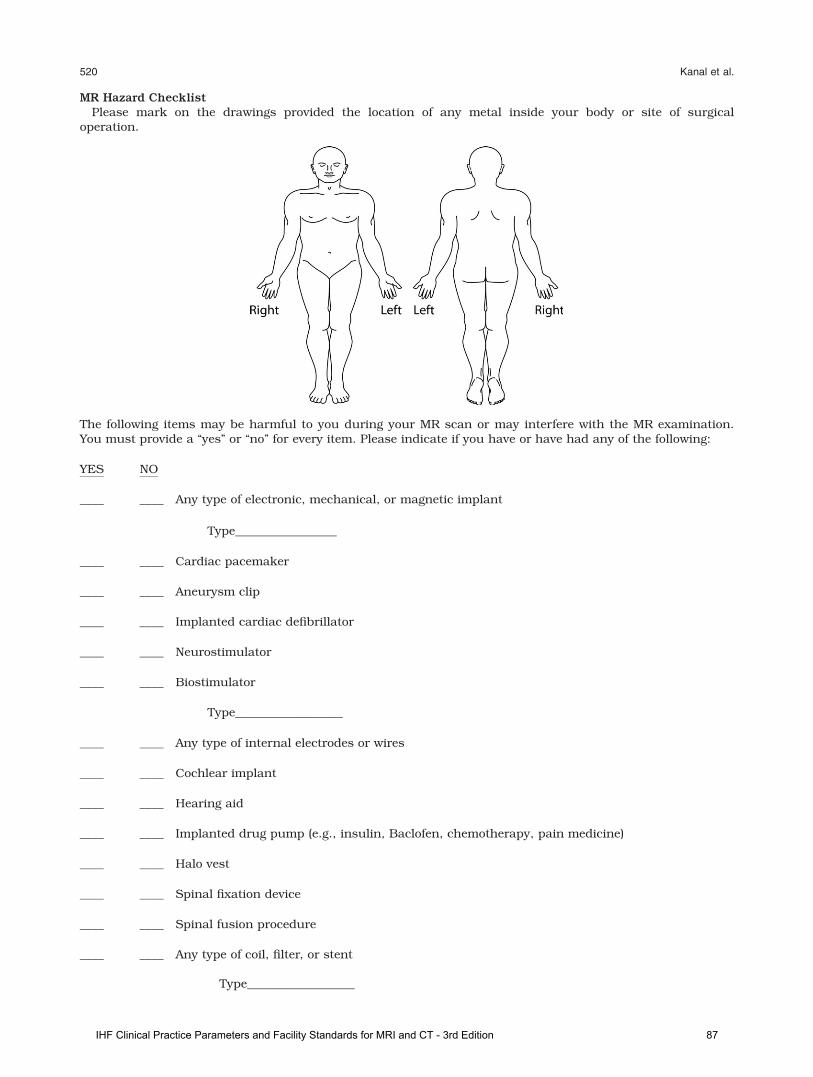
MR Hazard ChecklistPlease mark on the drawings provided the location of any metal inside your body or site of surgical
operation.
The following items may be harmful to you during your MR scan or may interfere with the MR examination.You must provide a ‘‘yes’’ or ‘‘no’’ for every item. Please indicate if you have or have had any of the following:
YES NO
____ ____ Any type of electronic, mechanical, or magnetic implant
Type_________________
____ ____ Cardiac pacemaker
____ ____ Aneurysm clip
____ ____ Implanted cardiac defibrillator
____ ____ Neurostimulator
____ ____ Biostimulator
Type__________________
____ ____ Any type of internal electrodes or wires
____ ____ Cochlear implant
____ ____ Hearing aid
____ ____ Implanted drug pump (e.g., insulin, Baclofen, chemotherapy, pain medicine)
____ ____ Halo vest
____ ____ Spinal fixation device
____ ____ Spinal fusion procedure
____ ____ Any type of coil, filter, or stent
Type__________________
520 Kanal et al.
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 87
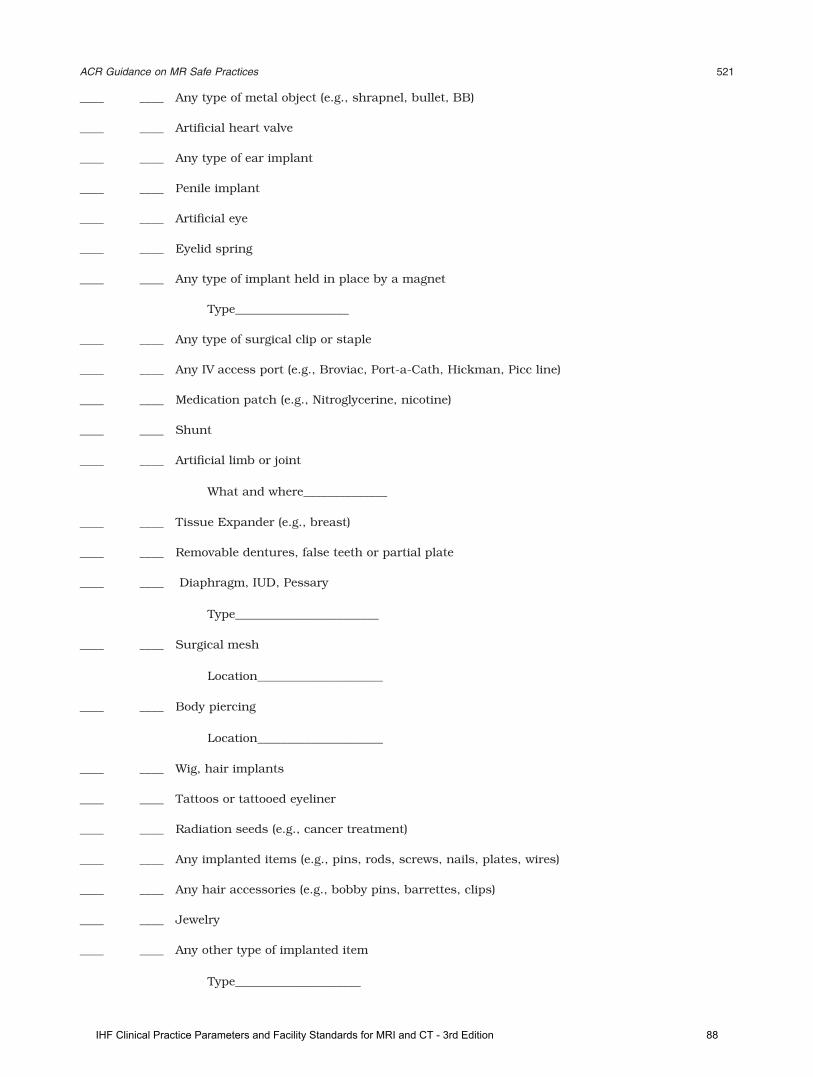
____ ____ Any type of metal object (e.g., shrapnel, bullet, BB)
____ ____ Artificial heart valve
____ ____ Any type of ear implant
____ ____ Penile implant
____ ____ Artificial eye
____ ____ Eyelid spring
____ ____ Any type of implant held in place by a magnet
Type___________________
____ ____ Any type of surgical clip or staple
____ ____ Any IV access port (e.g., Broviac, Port-a-Cath, Hickman, Picc line)
____ ____ Medication patch (e.g., Nitroglycerine, nicotine)
____ ____ Shunt
____ ____ Artificial limb or joint
What and where______________
____ ____ Tissue Expander (e.g., breast)
____ ____ Removable dentures, false teeth or partial plate
____ ____ Diaphragm, IUD, Pessary
Type________________________
____ ____ Surgical mesh
Location_____________________
____ ____ Body piercing
Location_____________________
____ ____ Wig, hair implants
____ ____ Tattoos or tattooed eyeliner
____ ____ Radiation seeds (e.g., cancer treatment)
____ ____ Any implanted items (e.g., pins, rods, screws, nails, plates, wires)
____ ____ Any hair accessories (e.g., bobby pins, barrettes, clips)
____ ____ Jewelry
____ ____ Any other type of implanted item
Type_____________________
ACR Guidance on MR Safe Practices 521
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 88
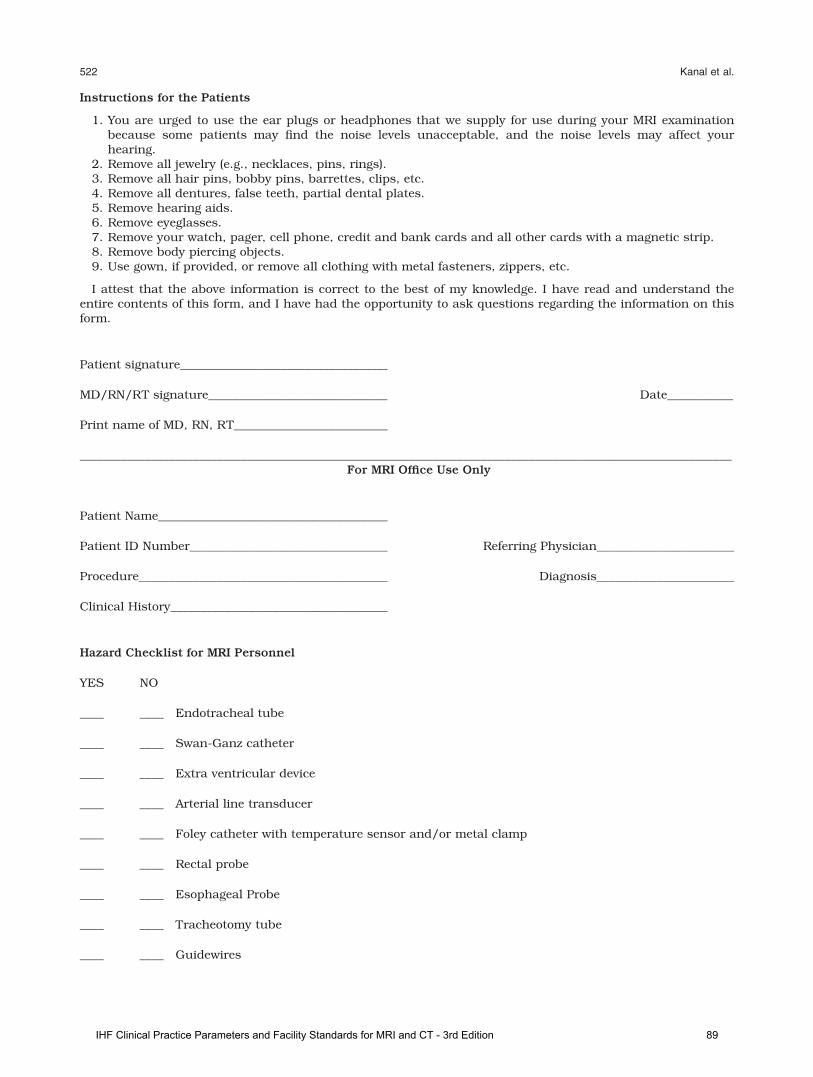
Instructions for the Patients
1. You are urged to use the ear plugs or headphones that we supply for use during your MRI examinationbecause some patients may find the noise levels unacceptable, and the noise levels may affect yourhearing.
2. Remove all jewelry (e.g., necklaces, pins, rings).3. Remove all hair pins, bobby pins, barrettes, clips, etc.4. Remove all dentures, false teeth, partial dental plates.5. Remove hearing aids.6. Remove eyeglasses.7. Remove your watch, pager, cell phone, credit and bank cards and all other cards with a magnetic strip.8. Remove body piercing objects.9. Use gown, if provided, or remove all clothing with metal fasteners, zippers, etc.
I attest that the above information is correct to the best of my knowledge. I have read and understand theentire contents of this form, and I have had the opportunity to ask questions regarding the information on thisform.
Patient signature___________________________________
MD/RN/RT signature______________________________ Date___________
Print name of MD, RN, RT__________________________
_____________________________________________________________________________________________________________For MRI Office Use Only
Patient Name________________________________________
Patient ID Number__________________________________ Referring Physician_______________________
Procedure__________________________________________ Diagnosis_______________________
Clinical History_____________________________________
Hazard Checklist for MRI Personnel
YES NO
____ ____ Endotracheal tube
____ ____ Swan-Ganz catheter
____ ____ Extra ventricular device
____ ____ Arterial line transducer
____ ____ Foley catheter with temperature sensor and/or metal clamp
____ ____ Rectal probe
____ ____ Esophageal Probe
____ ____ Tracheotomy tube
____ ____ Guidewires
522 Kanal et al.
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 89

APPENDIX 3
MR Facility Safety Design Guidelines
The goal of MR safety is to prevent harm to patients,though a MR facility cannot simply adopt one or twointerventions and hope to successfully attain thisobjective. According to safety and human factors engi-neering principles, multiple safety strategies must beadopted to be effective. This approach is sometimestermed ‘‘defense in depth.’’ The safety strategies out-lined in the main body of this MR Safe Practice Guide-lines document include, for instance, policies thatrestrict personnel access, specialized training anddrills for MR personnel, and warning labels for devi-ces to be brought into Zone IV regions.
Along with these people-oriented strategies of poli-cies and training, organizations need also to adopt thestrategies of safety-oriented architectural and interiordesign. These design elements can support the othersafety strategies, by making them easier or moreobvious to follow. The architectural enhancementsdescribed herein add one or more strong barriers toenhance ‘‘defense in depth’’.
This appendix includes descriptions of architecturaland interior design recommendations organizedaround the many MR suite functional areas. Note thata facility’s design can encourage safety and best prac-tices by improving the flow of patients, various health-care personnel, and equipment and devices, and notjust by to preventing MR unsafe items from becomingmissiles, or screening out patients with hazardousimplanted devices.
Placing design elements strategically in a suite lay-out such that the element supports best practiceworkflow patterns will increase compliance with saferpractices. For example, having a private area forpatient screening interviews will make it more likelythe patients will disclose sensitive types of implants.Another example of designing for safety is to includededicated space and temporary storage for MR Unsafeequipment (e.g., ferromagnetic IV poles, transportstretchers) out of direct sight and away from peopleflow patterns.
Effective and safe MRI suites must balance thetechnical demands of the MR equipment with localand state building codes, standards of accreditingbodies, clinical and patient population needs, payorrequirements and a collage of civil requirements fromHealth Insurance Portability and Accountability Act(HIPAA) to the Americans with Disabilities Act (ADA).
In an effort to better match appropriate facilitydesign guidelines with levels of patient acuity andcare, the ACR MR Safety Committee is currentlydeveloping level designations for MRI facilities in con-junction with the efforts of Committees from otherSocieties and Organizations. These will address cus-tomization of requirements for sites with varyinganticipated patient care sedation, anesthesia, and/orinterventional activities.
While it would be desirable to provide a universalMRI suite safety design, the variables are too numer-ous to adequately address in a single template. Thefollowing MRI Facility Safety Design Guidelines are
provided to provide information in support of plan-ning, design and construction of MR facilities, includ-ing updates to existing MR facilities, which enhancethe safety of patients, visitors and staff. This informa-tion is intended to supplement and expand uponpatient safety guidance provided throughout the ACRMR Safe Practice Guidelines document.
1. MR Equipment Vendor Templates
Design templates provided by MR equipment manu-facturers are invaluable in developing suites thatmeet the minimum technical siting requirements forthe specific equipment. Vendor design templates,however, typically depict only the control and equip-ment rooms, in addition to the magnet room, Zone IV.
Patient/family waiting, interview areas, physicalscreening/changing areas, access controls, storage,crash carts, induction, medical gas services,postscreened patient holding areas, infection controlprovisions, and interventional applications, amongmany other issues, are not addressed in typical ven-dor provided drawings. These issues are left to facilityowners, operators and their design professionals toresolve. The guidance which follows is designed toaddress many of these issues which directly impactsafety within the MR suite.
2. Patient interview/clinical screening areas (Zone II)
Reviewing the patient Safety Screening Form and MRHazard Checklist requires discussing confidential per-sonal information. To facilitate full and completepatient disclosure of their medical history, this clini-cal screening should be conducted in an area whichprovides auditory and visual privacy for the patient.Facilities should prospectively plan for electronicpatient medical records, which are useful in clinicalscreening, and should provide for access to records inthe MR suite in support of clinical patient screening.
Clinical screening of inpatients may be completed inthe patient room for hospital-based MR facilities.However, all screenings are to be double-checked andverified by appropriately trained MR Personnel beforeMR examination.
3. Physical screening and patient changing/gowningrooms (Zone II)
All persons and objects entering Zone III should bephysically screened for the presence of ferromagneticmaterials which, irrespective of size, can becomethreats in proximity to the MR. A location should beprovided for patients in which they may change out oftheir street clothes and into a facility provided gownor scrubs, if/as deemed appropriate. For those facili-ties which either do not provide space for, or do notrequire, patient changing, the facility must provide al-ternative means of identifying and removing itemswhich the patient may have brought with them thatmight pose threats in the MR environment.
A high-strength hand-held magnet is a recom-mended tool to evaluate the gross magnetic character-istics of objects of unknown composition. Magnetic
ACR Guidance on MR Safe Practices 523
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 90

strength for these permanent magnets fall off quicklyas one moves away from the face of the magnet. Thus,these may not demonstrate attraction for ferromag-netic components which are not superficially locatedor cannot for whatever reason be brought into closeproximity with the surface of this hand-held magnet.
Ferromagnetic detection systems have been demon-strated to be highly effective as a quality assurancetool, verifying the successful screen and identifyingferromagnetic objects which were not discovered byconventional screening methods. It is recommendedthat new facility construction anticipate the use offerromagnetic detection screening in Zone II and pro-vide for installation of the devices in a location whichfacilitates use and throughput. Many current ferro-magnetic detection devices are capable of being posi-tioned within Zone III, even at the door to the magnetroom, however a recommended use of ferromagneticdetection is to verify the screening of patients beforepassing through the controlled point of access intoZone III.
Physical screening of patients should consist of re-moval of all jewelry, metallic/ferromagnetic objects,onplants and prostheses (as indicated by manufac-turer’s conditional use requirements and physicianinstructions), and either having patients change outof their street clothes into facility provided gowns/scrubs or thorough screening of street clothes, includ-ing identifying the contents of pockets and composi-tion of metallic fibers, fasteners, and reinforcing.
While gowning maybe helpful, it is certainly not foolproof in precluding a patient from entering with ferro-magnetic material on them.
4. Transfer Area/Ferrous Quarantine Storage (Zone II)
Patients arriving with wheelchairs, walkers, portableoxygen and other appliances that may be unsafe inthe MR environment should be provided by the facilitywith appropriate MR safe or MR conditional applian-ces. An area should be provided to transfer thepatient from unsafe appliances to ones appropriate tothe MR environment. Unsafe appliances brought bythe patient should be secured in a ‘ferrous quaran-tine’ storage area, distinct from storage areas for MRsafe and MR conditional equipment and ideally lockedout of sight. Patient belongings should be retrievedfrom the ‘ferrous quarantine’ only when dischargingthe patient to whom the objects belong from the MRsuite.
5. Access control (Zone III/Zone IV)
Means of physically securing and restricting access toZone III from all adjacent areas must be provided. In-dependent access into Zone III must be limited to onlyappropriately trained MR personnel.
6. Patient Holding (Zone III)
Depending upon facility capacity and patient volume,it may be advisable to provide a postscreened patientholding area. Zone III holding areas should beequipped and appointed to prevent patient exit and
subsequent re-entry. This will help prevent the inad-vertent—or even intentional—introduction of un-screened objects and personnel.
Many multi-modal radiology facilities combinepatient holding and/or induction areas for patients ofdifferent modalities. This presents safety challengeswhen, for example, patients scheduled to receive a CTare held in a patient holding area shared bypostscreened MR patients. As CT patients would nottypically be screened for MR contraindications or fer-rous materials, this poses risks to both the CT patientwith a contraindicated implant and to those in theMRI zone IV should an unscreened individual inad-vertently enter with a ferrous object or implant.
Unless all persons in patient holding areas used forpostscreened MR patients are screened for MRI, thepractice of shared patient holding areas between MRand other modalities is discouraged. Ultimately it isthe responsibility of trained MR staff to verify thescreening of any co-mingled patient before permittingthem access to Zone III and Zone IV.
In all MR facilities, Zone III is required to be physi-cally secured and access limited to only MR personneland successfully MR prescreened non-MR personnelaccompanied by MR personnel. Ideally, facilitiesshould be designed such that patients for othermodalities are not co-mingled with postscreened MRpatients.
7. Lines of Sight/Situational Awareness (Zone III)
Trained MR personnel are arguably the single greatestsafety resource of MR facilities. These individualsshould be afforded visual control over all personsentering or exiting Zones III or IV. The technologistseated at the MR operator console should therefore beable to view not only the patient in the MR scannerbut also the approach and entrance into Zone IV. Lineof sight between the MR system operator console andboth the Zone IV entrance(s) and the patient withinthe MR scanner are requirements of the 2010 editionof Guidelines for Design and Construction of HealthCare Facilities (46). When practical, suites shouldalso be prospectively designed to provide a view fromthe MR operator’s console to patient holding areas. Ifthis cannot be satisfactorily achieved by direct line ofsight, remote video viewing devices are an acceptablesubstitute toward accomplishing this objective.
The technologist at the console should also be pro-vided with a view to induction/recovery areas withinthe MR suite, as applicable.
8. Emergency Resuscitation Equipment(Zone II or Zone III)
Because of risks associated with contrast agents,sedation, anesthesia, and even the frail health ofpatients undergoing MR examinations, it is advisedthat each facility have appropriate provisions for sta-bilization and resuscitation of patients.
It is recommended that crash carts and emergencyresuscitation equipment be stored in a readily acces-sible area within either Zone II or Zone III. This emer-gency resuscitation equipment is to be appropriately
524 Kanal et al.
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 91
labeled and also tested and verified as safe for usagein the MR environment for the anticipated conditionsof usage.
MR facilities should maintain a supply of emergencymedications to treat adverse reactions to administeredcontrast agents.
MR facilities providing care to patients who requireclinical support during the MR examination shouldhave emergency response equipment and personnel,trained in MR safety issues as well as trained torespond to anticipatable adverse events, readily avail-able to respond to patient adverse events or distressin the MR arena.
9. Fringe Magnetic Field Hazards (Zone III)
For many MR system installations, magnetic fringefields which project beyond the confines of the magnetroom superimpose potential hazards on spaces whichmay be outside the MR suite, potentially on levelsabove or below the MR site and perhaps even outsidethe building. Facilities must identify all occupy-ableareas, including those outside the MR suite (includingrooftops, storage areas, mechanical closets, etc.)which are exposed to potentially hazardous magneticfringe field strengths. Areas of potential hazard mustbe clearly identified and access to these areasrestricted, just as they would be within the MR suite.
10. Cryogen Safety (Zone IV)
Liquid helium and liquid nitrogen represent the mostcommonly used cryogens in MR environments. Thephysical properties of these cryogenic liquids presentsignificant potential safety hazards. If exposed toroom air these cryogenic liquids will rapidly boil offand expand into a gaseous state. This produces sev-eral potential safety concerns, including:
• Asphyxiation potential as cryogenic gases replaceoxygenated air.
• Frostbite considerations at the exceedingly lowtemperatures of these cryogenic liquids.
• Fire hazards can exist in the unlikely event of aquench, especially if some of the cryogenic gasesescape into the magnet room/Zone IV
• Pressure considerations within Zone IV can rarelyexist in the unlikely event of a quench in whichsome of the cryogenic gases escape into the mag-net room/Zone IV.
a. Cryogen Fills. Though contemporary supercon-ducting magnets require cryogen re-fills only infre-quently, there is still almost always the need toperiodically bring hundreds of liters of liquid cryogento the magnet. It is because of the risks to personsnear the magnet and storage/transport dewars thattrans-fill operations should be undertaken with greatcare and only by appropriately trained personnel.
• Dewars containing cryogenic liquids should neverbe stored inside an MRI facility or indeed in anyenclosed facility unless it is in a facility specifi-cally designed to obviate the associated pressure,temperature, and asphyxiation risks.
• A cryogen transfill should never be attempted byuntrained personnel or even with any unneces-sary personnel in attendance, including MR per-sonnel staff and patients, within Zone IV.
• Cryogen transfills should only be performed withappropriate precautions in place to preventagainst pressure entrapment and asphyxiation.
b. Magnet Room Cryogen Safety. For most MRI sys-tems if the magnet quenches, the escaping cryogenicgases are ducted outside the building to an unoccu-pied discharge area. However, there have been docu-mented failures of cryogen vent/quench pipeassemblies which have led to considerable quantitiesof cryogenic gases being inadvertently discharged intothe magnet room/Zone IV. The thermal expansion ofthe cryogens, if released into the magnet room, canpositively pressurize the magnet room and entrap per-sons inside until such time that the pressure isequalized.
The following recommended MRI suite design andconstruction elements reduce patient and staff risksin the unlikely event of a quench in which the cryogenvent pathway (quench pipe) ruptures or leaks intoZone IV:
• All magnet rooms/Zone IV regions for supercon-ducting magnets should be provided with anemergency exhaust pathway. The emergencyexhaust grille is to be located in the ceiling oppo-site the entrance to the magnet room (Zone IV)door. At this location, when activated in theunlikely event of a quench breach, the exhaustfan is positioned to draw the vaporous cloud ofcryogenic gas away from the door exiting from themagnet room.
• Many MR manufacturers are now requiring thatmagnet rooms for superconducting magnets alsobe provided with an additional form of passivepressure relief/pressure equalization to minimizethe risks of positive-pressure entrapment. Designsfor passive pressure relief mechanisms should fol-low design criteria similar to that of cryogen ventpathway and active exhaust, including dischargeto a protected area as described in section 10.cbelow.
Some MR facilities are constructed without openwaveguides or glass observation windows to Zone IVregions. In these facilities the potential risks ofentrapment are even greater and may warrant anadditional degree of attention in this regard.
While it can provide a degree of redundancy, itshould be noted that, even with an exhaust fan,designing the door to Zone IV to swing outward is not,by itself, an appropriate means of pressure relief. In asevere positive pressure situation unlatching an out-ward-swinging door might permit the door to burstopen with tremendous pressure, potentially injuringperson(s) opening the door. If used as the only meansof pressure equalization, an outward-swinging doormay actually introduce new hazards to any staff per-son attempting to open the door to a pressurized mag-net room from the outside.
ACR Guidance on MR Safe Practices 525
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 92

Similarly, though it has proven effective in life-threatening situations, breaking a control windowshould not be advocated as a primary means of reliev-ing/equalizing Zone IV pressure in a quench situa-tion. It should be noted that the current constructionof many RF shielded observation windows is suchthat it would make breaking the window very difficult,further diminishing it as a viable means of timelypressure relief.
Once provided with appropriate pressure equaliza-tion and emergency exhaust, magnet room door swingdirection and design should be left to the discretion ofa facility and their design professionals.c. Cryogen Vent Pathway. Obstructions, inappropri-ate pipe materials, insufficient pipe caliber and/orlength, or faulty connections in the length of the cryo-gen vent pathway can cause failure between the mag-net and point of discharge. An evaluation of thecurrent cryogen vent piping/ducting assembly is rec-ommended to help identify and correct potentialweaknesses that could potentially fail in a quench.Facilities are advised to evaluate the design andinspect the construction of their cryogen vent system.
Because minimum design requirements for somecryogen vent systems have been revised by magnetsystem vendors, facilities should obtain currentstandards from the original equipment manufacturersto use in evaluating their cryogen vent assembly andnot rely on original siting requirements.
Beyond the assessment of the current construction ofthe cryogen vent system, it is prudent for MRI facilities:
• To inspect cryogen vent systems at least annually,identifying stress/wear of pipe sections andcouplings, loose fittings and supports or signs ofcondensation/water within the cryogen vent path-way which may indicate a blockage.
• Following any quench of a superconducting mag-net, to conduct a thorough inspection of cryogenvent system, including pipe sections, fittings,couplings, hangers and clamps, before returningthe magnet to service.Because obstructions/occlusions of the cryogenvent can increase the likelihood of rupture in aquench event, facilities should ensure that:
• The discharge point has an appropriate weather-head which prevents horizontal, wind-driven pre-cipitation from entering, collecting, or freezing inthe quench exhaust pipe.
• The discharge point is high enough off of the roofor ground surface that snow or debris cannotenter or occlude the pipe.
• The discharge is covered by a material of suffi-ciently small openings to prevent birds or otheranimals from entering the quench pipe, while notoccluding cryogenic gaseous egress in a quenchsituation.
Facilities that discover failings in any of these basicprotections of the cryogen discharge point should im-mediately take additional steps to verify the patencyof the cryogen vent and provide the minimum currentdischarge protections recommended by the originalequipment manufacturer.
To protect persons from cryogen exposure at thepoint of discharge:
• At the point of cryogen discharge, a quench safetyexclusion zone with a minimum clear radius of 25feet (8 meters) should be established and clearlymarked with surface warnings and signage.
• The quench safety exclusion zone should bedevoid of serviceable equipment, air intakes, oper-able windows or unsecured doors that eitherrequire servicing or offer a pathway for cryogenicgasses to re-enter the building.
• Persons who must enter this quench safety exclu-sion zone, including incidental maintenance per-sonnel and contractors, should be permitted to doso only after receiving specific instruction onquench risks and response.
11. MR Conditional Devices (Zone IV)
The normal or safe operation of many medical devicesdesigned for use in the MR environment may be dis-rupted by exposure to conditions exceeding the device’sconditional rating threshold. It is advisable for MR facili-ties to identify the allowable conditional rating for staticfield and spatial gradient exposure for each MR Condi-tional device which may be brought into Zones III andIV. MR Conditional devices may be conditionally safe forone specific field strength, but unsafe at higher or lowerfield strength. For prospective installations it is recom-mended that the location of critical isogauss line(s) beidentified for MR Conditional equipment and devicesused within the MR suite and delineated on the floorand walls of the magnet room to aid in the positioningand safe and effective operation of said equipment.
All MR facilities should evaluate all MR Conditionalpatient monitoring, ventilators, medication pumps,anesthesia machines, monitoring devices, biopsy andother devices and equipment which may be broughtinto the magnet room for magnetic field tolerances.Facilities should consider providing physical indica-tions of critical gauss lines in the construction of themagnet room to promote the safe and effective use ofMR Conditional equipment, as appropriate.
12. Infection control (Zone IV)
Because of safety concerns regarding incidental per-sonnel within the MR suite, restricting housekeepingand cleaning personnel from Zone III and/or IVregions may give rise to concerns regarding the clean-liness of the MR suite. Magnet room finishes and con-struction details should be designed to facilitatecleaning by appropriately trained staff with nonmotor-ized equipment. Additionally, as the numbers of MR-guided procedures and interventional applicationsgrow, basic infection control protocols, such as seam-less floorings, scrub-able surfaces and hand washingstations should be considered.
13. Limits of applicability/recommended designassistance
The facility design issues identified in this documentaddress only general safety design issues for MRI
526 Kanal et al.
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 93

suites. There are a multitude of site-specific and mag-net-specific operational and technical design consider-ations relevant to MR facility design and constructionthat are not addressed in these Guidelines. Theseissues include, but are not limited to, patient acuity,staff access, modality conflicts, vibration sensitivity,throughput/efficiency, HIPAA considerations, magneticcontamination, sound transmission, magnet shim tol-erances, shielding design, moving metal interferences,MR equipment upgrades, electromagnetic interference,and many others.
In addition to incorporating the guidance from thisdocument, a facility would be well advised to seekexpert assistance in the planning and design of MRIand multi-modal radiology suites.
APPENDIX 4
MR Facility Emergency Preparedness Guidelines
Healthcare facilities have a unique obligation to mini-mize the disruption from disasters and hasten theirability to restore critical patient care services wheninterrupted.
Those charged with the operation of MRI facilitieshave the added complexities of protecting not only thestaff and structure, but also the equipment whichmay be extraordinarily sensitive to changes in itsenvironment, including vibration, power supply, andwater damage.
In the fall of 2005, many watched as hurricanesKatrina and Rita devastated vast swathes of theUnited States’ Gulf Coast. Those facilities which werewell prepared for the damage, loss of power, and otherfailures of infrastructure fared far better than thosethat that were not.
Even those not in the likely path of future Gulf hur-ricanes may have to contend with earthquakes, torna-does, fires, ice storms, snowstorms, or blackouts, atsome point. Particularly those involved in providingpatient care should look to how we will provide careat the times when it is most widely and desperatelyneeded. We may find that the facilities, equipmentand infrastructure required to provide clinical carehave not been adequately protected.
1. Water Damage:
Whether from roof-failure, burst pipes, storm surge orrising rivers, every facility has the potential for waterdamage to equipment and facilities. Damages canrange from inconveniences cured by a couple of hourswith a wet-dry vacuum, to flooding of equipment elec-tronics. It takes only a small quantity of water in con-tact with an MRI scanner to incapacitate or destroythe equipment.
To keep leaking roofs, burst pipes or other overheaddamage from dousing MRI equipment, it is recom-mended that facilities prepare by covering gantriesand equipment with sturdy plastic, taped in place,when water damage is an anticipated possibility. Tokeep processors and gradient cabinets from becomingswamped in a flood situation, electronics that can belifted up off the ground should be moved as far up off
of the floor as possible. RF shields, particularly thefloor assembly, may be significantly damaged andneed to be replaced in a flood situation if not designedto protect against water damage.
During the 2005 hurricanes, many hospitals andimaging facilities that had emergency generators tohelp restore power discovered that their sites had gen-erators, or other critical supplies, in basements orother low-lying areas that were flooded. Facilitiesshould evaluate risks from water damage and assesstheir preparations for failure of the building enclosureas well as the potential for a flood situation.
2. Structural damage:
MRI presents a particular challenge with structuralfailure. Though unlikely with current magnet systems,vibrations from seismic events do have the potentialto initiate a quench of the magnet system. Structuraldamage or motion may also damage the RF shield en-closure, potentially degrading image quality until theshield is repaired.
3. Power Outage:
Without electrical power to the vacuum pump / coldhead to keep the cryogen within a superconductingMRI liquefied, the cryogen will begin to boil off at anaccelerated rate. Depending upon cryogen vent designand boil off rate, the additional cryogenic gas dis-charge may freeze solid any accumulated water in thecryogen vent, occluding the pipe and increasing thepossibility for a cryogen vent breach in the event of aquench.
At some point if power to the vacuum pump is notrestored, likely a couple days to perhaps a week afterpower is lost, the magnet will spontaneously quench,discharging most or all of its remaining cryogenic gas-ses. This poses a safety risk to anyone near the dis-charge and runs a small but finite risk of potentiallypermanently damaging the magnet coils.
However, if power to the vacuum pump/cold headand cryogen levels is restored before a quench, thereshould be no long-term consequences to the magnet’soperation from a power interruption.
Temporary electrical power may be provided eitherthrough on-site or portable generators. Co-generation,or generating one’s own electricity all the time, maynot be economically feasible for smaller or stand-alone sites, but is increasingly appealing to hospitalsfor several reasons, with emergency capacity beingonly one.
4. Quench:
During the 2005 hurricanes, facilities, fearing exten-sive damage to their MRI systems from water or pro-tracted power outages, manually initiated pre-emptivequenches. Under the best circumstances, a quenchsubjects a magnet to a change of 500�F thermal shockwithin a few dozen seconds, which can cause majorphysical damage. Rarely, it is possible for the ventingcryogenic gases to breach the quench tube and causesignificant damage to the magnet room and/or
ACR Guidance on MR Safe Practices 527
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 94

jeopardize the safety of those in the vicinity. At oneNew Orleans area facility that elected to preemptivelyquench its magnets, the quench tube reportedly failedand the pressure from the expanding cryogen blewout the control room radiofrequency window (personalcommunication, Tobias Gilk, October 2005).
Because of the risks to personnel, equipment andphysical facilities, manual magnet quenches are to beinitiated only after careful consideration and prepara-tion. In addition to following those specific recommen-dations provided by the MRI manufacturer, a facilityshould initiate a pre-emptive quench in nonemergentsituations only after verifying the function of emer-gency exhaust systems, verifying or providing meansof pressure relief and a preliminary visual inspectionof the cryogen vent pipe as it leaves the MR unit tocheck for signs of water or ice inside the pipe (includ-ing water leaking from fittings or condensation form-ing on vent pipe sections). If/when feasible, adiscussion with the device manufacturer regarding anintentional controlled static magnetic field ramp-downmay be advisable.
5. Fire/Police:
Though very infrequent, MR suites have been thescene of emergencies requiring fire and/or policeresponse. While it is highly likely that this will be thefirst time many of the responders have been to an MRsuite, this should not be the first time that respondingorganizations have been introduced to the safetyissues for MR. Sites are encouraged to invite policeand fire representatives to presentations on MR safetyand to provide them with facility tours.
6. Code:
In the event that a person within the MR suite shouldrequire emergency medical attention, it is imperativethat those responding to a call for assistance areaware of, and comply with, MR safety protocols. Thisincludes nurses, physicians, respiratory technicians,paramedics, security, and others.
The impulse to respond immediately must be tem-pered by an orderly and efficient process to minimizerisks to patients, staff and equipment. This requiresspecialized training for code teams and, as with Fire/Police responses, clear lines of authority for screen-ing, access restrictions and quench authority. Fullresuscitation of patients within Zone IV is complicatedby the inability to accurately interpret electrocardio-graphic data. Furthermore, this may place at risk ofinjury all within the Zone IV from ferromagneticobjects which may be on, within, or brought into ZoneIV by emergency response personnel responding to acode if one is called in that area. Therefore, after ini-tiating basic cardiopulmonary resuscitation (airway,breathing, chest compressions), the patient should beimmediately moved out of Zone IV to a prospectivelydesignated location where the code can be run orwhere the patient will remain until the arrival ofemergent response personnel.
It is strongly advised that all MR facilities performregular drills to rehearse and refine emergency
response protocols to protect patients, MR staff andresponders.
7. Prevention:
While it is the nature of emergencies to be surprises,we can anticipate the types of incidents that havehigher likelihoods given our facilities, practices andlocations. Every facility can anticipate the potentialfor flooding, fire and code situations. In addition tothese, many areas (California and coastal Alaska, forexample) can expect earthquakes. The central andsouthern plains states of the U.S. can anticipate tor-nados. Colder climates can expect massive snows orice storms.
State and federal offices of emergency preparednessare dedicated to anticipating and preparing for thespecific threats to your region. These can serve as anexcellent resource regarding risks and strategies forpreparation.
Once a disaster has struck, it is important to assesswhat the immediate needs of the community are andto restore those critical patient care services first.
Damage to MRI equipment and facilities may not berepaired as quickly. For gravely incapacitated facili-ties, semi-trailer based MRI units may be the onlymeans of quickly restoring radiology capacity.
All healthcare facilities should have emergency pre-paredness plans. The healthcare plans for MRI facili-ties should specifically address the unique aspects ofMRI equipment. These plans should define who hasthe authority to authorize nonemergent quenches,procedures for emergency or backup power for vac-uum pump/cold head, as well as instructions on howto protect gantries and sensitive electronics. Facilitiesshould have the necessary supplies prepositioned andchecklists for preparatory and responsive actions.Emergency preparedness plans should also includeinformation necessary for restoring clinical services,including contacts for MRI system vendor, RF shieldvendor, cryogen contractor, MR suite architect andconstruction contractor, local and state officials, andaffiliated hospital and professional organizations.
Below are a few questions that may facilitate the de-velopment of an emergency preparedness plan specificto the needs of a facility.
• What are the likely/possible natural disasters toaffect the area?
• What are the likely/possible man-made disastersto affect the area?
• Is electrical power likely to be interrupted?• Would other utilities (natural gas, telecommunica-tions, etc.) likely be interrupted?
• What equipment would be inoperative during theemergency?
• What equipment could be damaged by theemergency?
• What equipment should be provided with criticalor backup power?
• If the utility service is not quickly restored, whatother risks may arise?
• Would patients and staff be able to get to thefacility?
528 Kanal et al.
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 95

• Would patients or staff be trapped at the facility?• How critical is each patient care service providedat the facility?
• How does the facility protect the equipmentneeded to support each service?
• How does the facility protect the patient data(including such options as off site storage) fromeach service?
• If the facility does not have the resources on site,who can provide them?
REFERENCES
1. Patient death illustrates the importance of adhering to safety pre-cautions in magnetic resonance environments. Health Devices2001;30:311–314.
2. Chaljub G, Kramer LA, Johnson RF III, Johnson RF Jr, Singh H,Crow WN. Projectile cylinder accidents resulting from the pres-ence of ferromagnetic nitrous oxide or oxygen tanks in the MRsuite. AJR Am J Roentgenol 2001;177:27–30.
3. Kanal E, Borgstede JP, Barkovich AJ, et al. American College ofRadiology White Paper on MR Safety: 2004 update and revisions.AJR Am J Roentgenol 2004;182:1111–1114.
4. Kanal E, Borgstede JP, Barkovich AJ, et al. American College ofRadiology White Paper on MR Safety. AJR Am J Roentgenol2002;178:1335–1347.
5. Kanal E, Shellock FG. Policies, guidelines, and recommendationsfor MR imaging safety and patient management. SMRI SafetyCommittee. J Magn Reson Imaging 1992;2:247–248.
6. Shellock FG, Kanal E. Policies, guidelines, and recommendationsfor MR imaging safety and patient management. SMRI SafetyCommittee. J Magn Reson Imaging 1991;1:97–101.
7. ACR practice guideline for performing and interpreting magneticresonance imaging (MRI). Available at: http://www.acr.org/SecondaryMainMenuCategories/quality_safety/guidelines/dx/mri_performing_interpreting.aspx. Accessed September 13, 2011.
8. Shellock FG, Kanal E. Guidelines and recommendations for MRimaging safety and patient management. III. Questionnaire forscreening patients before MR procedures. The SMRI Safety Com-mittee. J Magn Reson Imaging 1994;4:749–751.
9. Kanal E, Barkovich AJ, Bell C, et al. ACR guidance document forsafe MR practices: 2007. AJR Am J Roentgenol 2007;188:1447–1474.
10. Device Advice: Comprehensive regulatory assistance. Available at:http://www.fda.gov/MedicalDevices/DeviceRegulationandGuidance/default.htm. Accessed September 19, 2011.
11. Jarvik JG, Ramsey S. Radiographic screening for orbital foreignbodies prior to MR imaging: is it worth it? AJNR Am J Neurora-diol 2000;21:245–247.
12. Seidenwurm DJ, McDonnell CH III, Raghavan N, Breslau J. Costutility analysis of radiographic screening for an orbital foreignbody before MR imaging. AJNR Am J Neuroradiol 2000;21:426–433.
13. Kanal E, Gillen J, Evans JA, Savitz DA, Shellock FG. Survey ofreproductive health among female MR workers. Radiology 1993;187:395–399.
14. American Academy of Pediatrics Committee on Drugs: Guidelinesfor monitoring and management of pediatric patients during andafter sedation for diagnostic and therapeutic procedures. Pedia-trics 1992;89:1110–1115.
15. Guidelines for monitoring and management of pediatric patientsduring and after sedation for diagnostic and therapeutic proce-dures: addendum. Pediatrics 2002;110:836–838.
16. Practice guidelines for sedation and analgesia by non-anesthesi-ologists: An updated report by the American Society of Anesthesi-ologists Task Force on Sedation and Analgesia by Non-Anesthesiologists. Anesthesiology 2002;96:1004–1017.
17. Standards and intents for sedation and anesthesia care. Compre-hensive Accreditation Manual for Hospitals. Chicago, IL: JointCommission on Accreditation of Healthcare Organizations; 2002:Report no. TX 2–2.
18. US Food and Drug Administration Manufacturer and User FacilityDevice Experience (MAUDE) Data Base (MDR Report Key 434259,
489264, 410913). Available at: http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfMAUDE/TextSearch.cfm. Accessed Septem-ber 8, 2011.
19. Gandhi OP, Chen XB. Specific absorption rates and inducedcurrent densities for an anatomy-based model of the human forexposure to time-varying magnetic fields of MRI. Magn ResonMed 1999;41:816–823.
20. Konings MK, Bartels LW, Smits HF, Bakker CJ. Heating aroundintravascular guidewires by resonating RF waves. J Magn ResonImaging 2000;12:79–85.
21. Food and Drug Administration Public Health Advisory: Risk ofBurns during MRI Scans from Transdermal Drug Patcheswith Metallic Backings, March 5, 2009, Updated March 9, 2009.Available at: http://www.fda.gov/Drugs/DrugSafety/Postmarket-DrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/PublicHealthAdvisories/ucm111313.htm. Accessed May 15, 2012.
22. IEC 60601–2-33, Ed. 2.0 Medical Electrical Equipment-Part 2:Particular requirements for the safety of magnetic resonanceequipment for medical diagnosis. Geneva, Switzerland: Interna-tional Electrotechnical Commission (IEC); 2002.
23. ACR-SIR practice guideline for adult sedation/analgesia.Available at: http://www.acr.org/SecondaryMainMenuCatego-ries/quality_safety/guidelines/iv/adult_sedation.aspx. AccessedSeptember 13, 2011.
24. Standards for basic anesthesic monitoring. (Approved by the ASAHouse of Delegates on October 21, 1986, and last amended onOctober 20, 2010 with an effective date of July 1, 2011.) ParkRidge, IL: American Society of Anesthesiologists.
25. Standards for postanesthesia care. (Approved by the ASA Houseof Delegates on October 27, 2004, and last amended on October21, 2009.) Park Ridge, IL: American Society of Anesthesiologists.
26. Statement on non-operating room anesthetizing locations.(Approved by the ASA House of Delegates on October 19, 1994and last amended on October 22, 2008.) Park Ridge, IL: Ameri-can Society of Anesthesiologists.
27. American College of Radiology. ACR digest of council actions.Reston, VA: ACR, 1999:126 (Res 1-H 1987, 1997).
28. American College of Radiology. ACR Manual on Contrast Media,Version 8, 2012. Available at: http://www.acr.org/SecondaryMainMenuCategories/quality_safety/contrast_manual.aspx. AccessedSeptember 13, 2011.
29. Al-Sabagh KH, Christensen BE, Thogersen AM, et al. [Safety ofmagnetic resonance imaging in patients with pacemaker andimplantable defibrillator]. Ugeskr Laeger 2010;172:1740–1744.
30. Gimbel JR. Unexpected asystole during 3T magnetic resonanceimaging of a pacemaker-dependent patient with a ’modern’ pace-maker. Europace 2009;11:1241–1242.
31. Gotte MJ, Russel IK, de Roest GJ, et al. Magnetic resonanceimaging, pacemakers and implantable cardioverter-defibrillators:current situation and clinical perspective. Neth Heart J 2010;18:31–37.
32. Avery JK. Loss Prevention case of the month. Not my responsibil-ity! J Tenn Med Assoc 1988;81:523.
33. Ferris NJ, Kavnoudias H, Thiel C, Stuckey S. The 2005 Austra-lian MRI safety survey. AJR Am J Roentgenol 2007;188:1388–1394.
34. Irnich W, Irnich B, Bartsch C, Stertmann WA, Gufler H, Weiler G.Do we need pacemakers resistant to magnetic resonance imag-ing? Europace 2005;7:353–365.
35. Langman DA, Goldberg IB, Finn JP, Ennis DB. Pacemaker leadtip heating in abandoned and pacemaker-attached leads at 1.5Tesla MRI. J Magn Reson Imaging 2011;33:426–431.
36. Hartnell GG, Spence L, Hughes LA, Cohen MC, Saouaf R, Buff B.Safety of MR imaging in patients who have retained metallicmaterials after cardiac surgery. AJR Am J Roentgenol 1997;168:1157–1159.
37. Murphy KJ, Cohan RH, Ellis JH. MR imaging in patients withepicardial pacemaker wires. AJR Am J Roentgenol 1999;172:727–728.
38. Kanal E. Safety of MR imaging in patients with retained epicar-dial pacer wires. AJR Am J Roentgenol 1998;170:213–214.
39. Faris OP, Shein M. Food and Drug Administration perspective:Magnetic resonance imaging of pacemaker and implantable car-dioverter-defibrillator patients. Circulation 2006;114:1232–1233.
ACR Guidance on MR Safe Practices 529
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 96

40. Gimbel JR. Magnetic resonance imaging of implantable cardiacrhythm devices at 3.0 tesla. Pacing Clin Electrophysiol 2008;31:795–801.
41. Nazarian S, Halperin HR. How to perform magnetic resonanceimaging on patients with implantable cardiac arrhythmia devices.Heart Rhythm 2009;6:138–143.
42. Gimbel JR. Guidelines and the growing service burden. J IntervCard Electrophysiol 2010;28:83–85.
43. Hauser RG, Kallinen L. Deaths associated with implantable car-dioverter defibrillator failure and deactivation reported in theUnited States Food and Drug Administration Manufacturer and
User Facility Device Experience Database. Heart Rhythm 2004;1:399–405.
44. Jilek C, Tzeis S, Reents T, et al. Safety of implantable pace-makers and cardioverter defibrillators in the magnetic field of anovel remote magnetic navigation system. J Cardiovasc Electro-physiol 2010;21:1136–1141.
45. Gimbel JR. Unexpected pacing inhibition upon exposure to the3T static magnetic field prior to imaging acquisition: what is themechanism? Heart Rhythm 2011;8:944–945.
46. The Facility Guidelines Institute. Guidelines for the Design andConstruction of Health Care Facilities, 2010 edition. Chicago:American Society for Healthcare Engineering; 2010.
530 Kanal et al.
IHF Clinical Practice Parameters and Facility Standards for MRI and CT - 3rd Edition 97
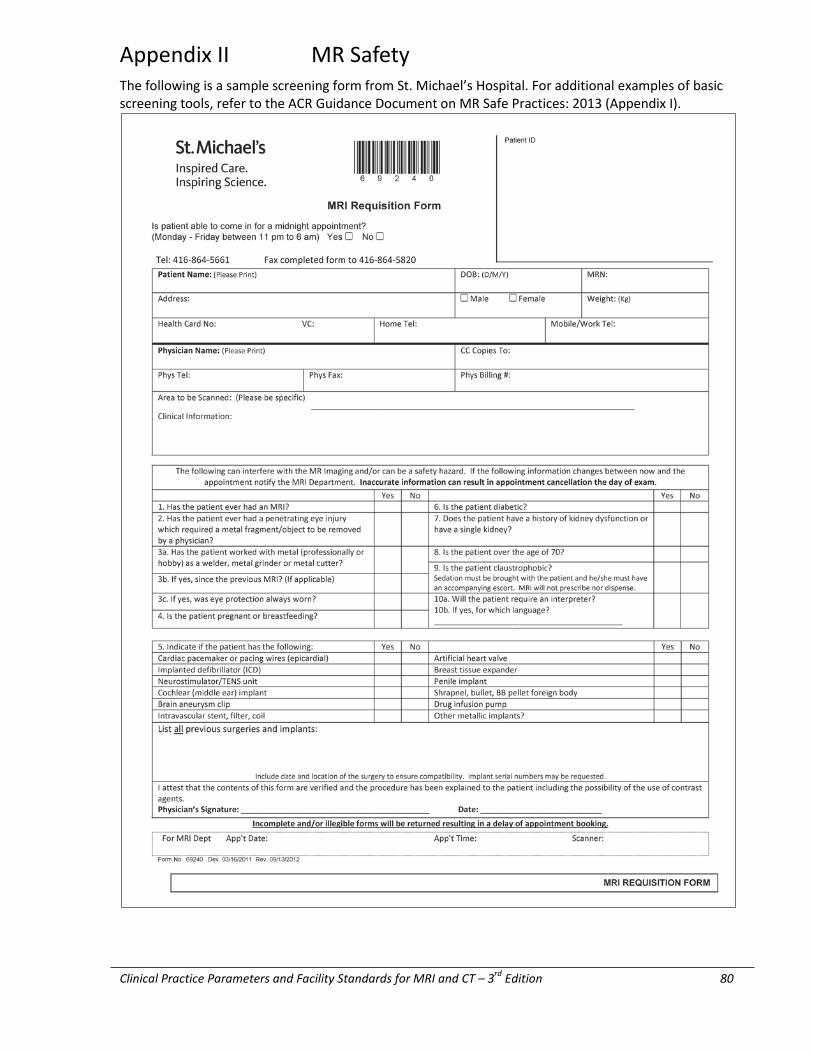
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd Edition 80
Appendix II MR Safety The following is a sample screening form from St. Michael’s Hospital. For additional examples of basic screening tools, refer to the ACR Guidance Document on MR Safe Practices: 2013 (Appendix I).
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 81
Appendix III Report of the Diagnostic Imaging Safety Committee for Computed Tomography (CT) – February 2007
Executive Summary
Computed tomography (CT) has revolutionized the investigation of patients who have a wide variety of medical conditions and has led to more efficient patient care. The technology for this imaging modality has advanced rapidly over the past decade and as a result, there has been a significant increase in the use of CT in Ontario and around the world. Ionizing radiation, as used for CT, can increase an individual’s lifetime risk of developing cancer. This risk increases as the dose increases, is greater for children than for adults, and is greater for females than for males. As with all medical procedures, the small potential risk from a CT examination must be weighed against the potential benefits. As with all medical imaging technology involving ionizing radiation, the principle of ALARA (As Low As Reasonably Achievable) should be applied in CT. In other words, CT examinations should be performed using sufficient dose to achieve acceptable image quality given the clinical context, but without exposing patients to unnecessary amounts of ionizing radiation. It is recognized that this is often a complex balancing act. Much effort needs to be focused now and in the future on dose management and optimization so that CT technology continues to be used appropriately in Ontario. The recommendations in this report are intended to be applicable to any diagnostic CT scanner in Ontario that is used for the purpose of medical imaging of humans, and include a section focusing on the pediatric population. Because of the rapid changes in CT technology, the emphasis in this report is on the newer multidetector CT (MDCT) scanners. In the future, newer imaging technologies that use ionizing radiation will need to be assessed in light of existing regulations, and safety standards will need to be developed for their use. The Healing Arts and Radiation Protection (HARP) Act, Revised Statutes of Ontario, 1990, and the X-ray Safety Code (Regulation 543) cover the use of x-rays for the irradiation of human beings in the province of Ontario. Under the X-ray Safety Code, a “computed transaxial tomography x-ray machine” is specifically excluded from the definition of a “diagnostic x-ray machine.” At the same time, a “computed axial tomography (CT) scanner or machine” is not defined in the HARP Act. Due to the rapid technological developments and increase in CT use, any future revisions to the HARP Act should define what a CT scanner is and should recognize that the radiation doses associated with CT examinations are generally higher than those associated with conventional x-ray examinations.
Recommendations The Committee recommends that the province of Ontario put in place regulations and/or legislation as follows:
82 The College of Physicians and Surgeons of Ontario
HARP Act 1. The HARP Act should be revised to include a definition of a “computed axial tomography (CT) scanner or machine.” Future revisions to the HARP Act should also recognize that the radiation doses associated with CT examinations are generally higher than those associated with conventional x-ray examinations. Dose Reduction Strategies This section focuses on strategies and recommendations that can be used to manage and reduce the radiation dose related to CT scanning.
Alternative Imaging Methods The decision to perform a CT examination must be justified based on the clinical setting and is a shared responsibility between the referring clinician and the radiologist. Alternative imaging methods that do not use ionizing radiation — such as ultrasound (US) or magnetic resonance imaging (MRI) — should be considered if appropriate.
Prescribing or Requesting a CT Scan CT examinations should specifically be excluded from Medical Directives. The larger radiation doses generally associated with CT compared to those associated with conventional x-rays pose patient safety concerns in the use of Medical Directives for CT examinations.
4. The HARP Act should be revised to ensure that only individuals who have the appropriate clinical knowledge and training in radiation safety are permitted to prescribe or request CT examinations. Pregnancy 5. Each CT facility shall have a policy for screening women of childbearing age for pregnancy before performing a CT examination. If the patient is pregnant or possibly pregnant, the benefits of performing the CT must be weighed against any potential risk to the fetus.
Patient Shielding
6. The Radiation Protection Officer (RPO) at each facility shall develop a policy for patient shielding specifically for CT. The policy should be appropriate for the facility’s CT equipment and patient population, and comprise protocols for in-beam and out-of-beam shielding accessories. The policy should be reviewed on a regular basis, taking into consideration changes in practice and technological innovations. 7. The Committee recommends that in-beam shielding not be used under the following conditions:
a) when real-time dose modulation is used and the presence of the shield will cause the CT scanner to compensate by increasing dose; or
b) where there is proof that in-beam shielding will interfere with the imaging objectives.
Anatomic Coverage
8. The anatomic coverage of a CT examination should be limited to the area of clinical interest.
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 83
CT Protocols
9. CT protocols should be designed to obtain the necessary diagnostic information based on the clinical indication of each situation. CT protocols should be reviewed periodically by radiologists and CT technologists to ensure dose optimization.
CT Scanning Parameters
10. CT technologists and radiologists must be knowledgeable about how the manipulation of various scanning parameters may influence dose and image quality in their CT scanners.
Multiphase Image Acquisition
11. The acquisition of more than one set of images from the same anatomic region must be justified based on detailed medical and radiological knowledge.
Repeat CT Examinations
12. When a follow-up or repeat CT examination is requested, the referring clinician and the radiologist must first consider other imaging modalities that do not use ionizing radiation, such as US or MRI. Repeat CT examinations must be justified based on the clinical indication. If a follow-up CT examination is justified, the examination may be modified to reduce the dose, as long as clinical care is not compromised.
CT Manufacturers/Vendors
13. Upon installation of a new CT scanner, a facility’s Radiation Protection Officer (RPO) shall provide the X-ray Inspection Service (XRIS) of MOHLTC proof that the technologists and physicians operating that specific make and model of CT scanner have received training on dose reduction strategies appropriate to the planned clinical operation of the scanner. This proof would be in the form of a certificate of training provided by the vendor. In addition, the RPO must keep a permanent record of authorized operators and their training status on installed CT scanners for review by MOHLTC and its enforcement agents for at least six years.
Diagnostic Reference Levels
14. Ontario should establish Diagnostic Reference Levels for the following CT examinations: head CT, chest CT, and abdominal/pelvic CT. A team consisting of members from professional medical bodies should be established to review the methods for establishing DRLs, administer the survey, collect the data, determine the DRLs, and disseminate the information to all stakeholders. Once established, DRLs should be reviewed periodically. Funding that is appropriate to the scope of the project will be required.
84 The College of Physicians and Surgeons of Ontario
15. Manufacturers of CT scanners (including Positron Emission Tomography/CT units) must display the dose for each CT examination on the control console.
16. The dose for each CT examination must be recorded. This record must be kept and be available for periodic audit.
17. In pediatric cases, the size of the CT phantom used in calculating dose information must be displayed.
Pediatric CT
18. All requests for CT examinations for children must be reviewed by a radiologist prior to booking to ensure that the referral is appropriate and that possible alternative imaging modalities have been considered.
19. Each CT facility must establish local protocols for use in pediatric scanning. The Radiation Protection Officer must demonstrate to MOHLTC that technologists and radiologists operating the CT scanner have received instruction on the appropriate use of pediatric protocols.
20. All CT manufacturers must have suggested protocols specific to children of varying ages available on all models of scanner, for all commonly performed examinations.
21. As an additional safeguard to promote the use of weight-adjusted protocols in children, it is recommended that all manufacturers adapt CT software to promote protocol adjustments based on patient weight.
CT Technologist Training
22. MOHLTC should continue to provide support for a standardized CT curriculum for all undergraduate/college Medical Radiation Technologist (MRT) programs and for access to the same curriculum for MRT graduates in Ontario.
23. The CT curriculum shall include training in radiation safety and dose management.
CT Personnel and the Work Environment
24. In addition to existing legislation and policies, CT facilities shall adopt the following safety guidelines:
a) Doors accessible to the general public that enter into a CT scan room must be locked during scanner operation.
b) CT operators must be within arm’s length of the scan abort button during image acquisition.
c) CT operators must be in visual contact with the patient during image acquisition.
CT Scanner Testing and Inspection
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 85
25. The testing and inspection of CT scanners should be specifically incorporated into the HARP Act. This may require a major revision to the HARP Act and the X-ray Safety Code. The role and duties of the X-ray Inspection Service may also need to be modified so that XRIS is able to perform and audit the inspection and maintenance of CT scanners, including dental cone beam CT, in Ontario. The appropriate resources to expand this service will be necessary.
Education Materials
Health Care Workers
26. The province should designate an organization to develop and disseminate information for physicians and other health care workers that helps them to better weigh the benefits and risks of CT studies for their patients. The topic of benefits and risks of procedures that use ionizing radiation such as CT should be included in the training programs of health care providers who are involved in the prescribing or performing of such procedures.
Patients
27. The province should designate an organization to develop and disseminate information concerning the benefits and risks of imaging studies involving ionizing radiation, specifically CT, to patients and the general public.
Monitoring Patient Dose
28. At this time, the Committee does not recommend attempting to establish a permanent, portable record of the cumulative dose that each patient in Ontario receives.
Dental Cone Beam CT
29. The HARP Act should be revised to reflect the newer technology of dental CBCT.
30. MOHLTC should lift the current moratorium on approval of dental CBCT scanners, but approval should be restricted to Oral and Maxillofacial Radiologists and graduate Oral Radiology academic centres.
31. Dental CBCT scanners must be operated under the supervision of an Oral and Maxillofacial Radiologist.
32. All requests for dental CBCT examinations must be reviewed and approved according to protocol by an Oral and Maxillofacial Radiologist prior to performing the examination.
Research
33. Close collaboration among CT manufacturers, imaging scientists, and radiologists is encouraged to further explore and promote methods of dose management for CT.
86 The College of Physicians and Surgeons of Ontario
Full Report
BACKGROUND
The Ontario Health Technology Advisory Committee (OHTAC) recommended that a study of the safety aspects of computed tomography (CT) and magnetic resonance imaging (MRI) be conducted. The Ministry of Health and Long-Term Care (MOHLTC) provided a research grant to the Healthcare Human Factors Group at the University Health Network to investigate and provide safety recommendations on CT and MRI for OHTAC’s consideration. Recommendations from the two reports, covering CT and MRI safety, were endorsed by OHTAC [1,2]. One of the recommendations was to create a Diagnostic Imaging Safety Committee for CT and MRI. The CT Safety Committee would be responsible for the development of recommendations concerning standards and best practices for CT, including methods of dose reduction to patients and medical imaging staff, as well as the testing and inspection of CT scanners in Ontario.
INTRODUCTION
The use of CT imaging has revolutionized the investigation of patients who have a wide variety of medical conditions, including cancer, trauma, and cardiovascular, neurological, respiratory, gastrointestinal, urological, and musculoskeletal illnesses. CT technology has advanced rapidly in the past decade, creating an even wider application of this imaging modality and enabling more efficient patient care. As a result, there has been a significant increase in the use of CT for medical imaging in the province of Ontario and around the world [3,4].
Although there will always be some debate in an issue involving risk estimates, it is accepted from the consensus of scientific literature that there is no level of ionizing radiation that can be considered completely safe. Ionizing radiation, as used for diagnostic CT imaging, carries the potential of increasing an individual’s lifetime risk of developing cancer. The Biological Effects of Ionizing Radiation (BEIR) VII report estimates that “approximately one individual per thousand would develop cancer from an exposure of 0.01Sv,” which is the dose estimate from an abdominal CT scan. To put the risk in perspective, in the United States, the overall lifetime risk of cancer in the general population is 42 out of 100 people. In other words, a person’s risk of developing cancer related to the radiation from an abdominal CT scan would increase to 42.1% from 42.0%. It is also recognized that the risk increases as the dose increases, that the risk is greater for children than for adults, and that the risk is slightly greater for girls than for boys [5]. The relative risk from exposure to low levels of radiation should be weighed against the potential clinical benefits of a CT examination by a qualified health care practitioner. The recommendations of this report should not be a substitute for clinical judgment and it is recognized that each patient and clinical scenario is unique.
As with all medical imaging technology involving ionizing radiation, the principle of ALARA (As Low As Reasonably Achievable) should be applied. In other words, CT imaging studies should be performed using sufficient dose to achieve acceptable image quality given the clinical context, but without exposing patients to unnecessary amounts of ionizing radiation. It is recognized that this is often a complex balancing act and that a great deal of effort needs to be focused now and in the future on dose management and optimization, so that CT technology continues to be used appropriately in Ontario. The recommendations contained in this report are intended to be applicable to any diagnostic CT scanner in Ontario that is used for the purpose of medical imaging of humans for routine clinical practice. The recommendations apply to all patients and include a section focusing on the pediatric
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 87
population. Because of the rapid changes in CT technology, the emphasis in this report is on the newer multidetector CT (MDCT)scanners.
Generally, a CT scanner is considered an x-ray device that uses a rotating fan-beam and detector system to acquire data that can be reconstructed into a three-dimensional (3D)image. The 2006 Annual Report of the Office of the Auditor General of Ontario considered safety issues relevant to fan-beam devices [3]. There is a wider class of specialty device that is able to acquire images that can be reconstructed into 3D images, but these devices are not considered CT scanners for billing purposes under the Ontario Health Insurance Plan (OHIP). However, they meet the functional definition of CT in the eyes of MOHLTC. Primarily, these devices are described as cone-beam imagers, volume imagers, or cone-beam CT. Presently, any x-ray device that has the ability to take precisely positioned angled views and that is fitted with a digital receptor is potentially able to produce 3D images with the addition of appropriate reconstruction software. Therefore, x-ray devices being produced now and in the future that meet these specifications may potentially be considered CT scanners. In the future, specific recommendations for the use of cone-beam devices and other imaging devices that use ionizing radiation will be needed.
It is the responsibility of the Radiation Protection Officer (RPO) of a CT facility to assess new technology in light of existing regulations and to develop safety standards for its use. Facilities owning and operating cone-beam technology should have policies in place that address issues of dose monitoring, dose reduction, and quality control, consistent with the Healing Arts Radiation Protection (HARP) Act. Patient dose monitoring is a particularly important issue because cone-beam devices do not estimate dose in the same manner that fan-beam CT scanners estimate and display dose.
The HARP Act, Revised Statutes of Ontario, 1990, and the X-ray Safety Code (Regulation 543) cover the use of x-rays for the irradiation of human beings in the province of Ontario. Under the X-ray Safety Code, a “computed transaxial tomography xray machine” is specifically excluded from the definition of a “diagnostic x-ray machine.” At the same time, a “computed axial tomography (CT) scanner or machine” is not defined in the HARP Act. Due to the rapid technological developments and increase in CT use, any future revisions to the HARP Act should define what a CT scanner is and should recognize that the radiation doses associated with CT examinations are generally higher than those associated with conventional x-ray examinations.
At the national level, a Safety Code for Radiation Protection in Radiology for Large Facilities is currently being prepared by Health Canada. It is anticipated that this Safety Code will contain recommended safety procedures for the installation, use, and control of x-ray equipment, including CT scanners, in large radiological facilities. There are a number of other national and international bodies also currently working on guidelines for managing patient dose with MDCT scanners, including the International Commission on Radiological Protection (ICRP) [6]. These reports and guidelines will need to be taken into consideration as they become available.
RECOMMENDATIONS
For the purposes of this report, it is intended that recommendations made to “Ontario” or to “the province of Ontario” be understood as being made to Ontario’s Ministry of Health and Long-Term Care (MOHLTC) or any other provincial body responsible for governing CT facilities.
The Committee recommends that the province of Ontario put in place regulations and/or legislation as follows:
88 The College of Physicians and Surgeons of Ontario
HARP ACT
1. The HARP Act should be revised to include a definition of a “computed axial tomography (CT) scanner or machine.” Future revisions to the HARP Act should also recognize that the radiation doses associated with CT examinations are generally higher than those associated with conventional x-ray examinations.
DOSE REDUCTION STRATEGIES
This section focuses on strategies that can be used to manage and reduce the radiation dose related to CT scanning. The discussion includes specific recommendations to pursue the goal of dose reduction.
Alternative Imaging Methods
Radiation protection includes justification for medical imaging studies that use ionizing radiation [6]. When a CT scan is requested, the referring clinician and the radiologist should consider the clinical question and determine whether an alternative imaging method that does not use ionizing radiation — such as ultrasound or MRI — might be more appropriate. This is particularly important for the pediatric population. The clinical setting, patient age and gender, local expertise, and available resources will influence the determination. There are national published guidelines that may help referring clinicians and radiologists to determine the appropriateness of imaging studies for a variety of clinical scenarios. These publications include:
• Diagnostic Imaging Referral Guidelines (Canadian Association of Radiologists) [7]
• American College of Radiology Appropriateness Criteria, 2000 (American College of Radiology) [8]
• Royal College of Radiologists, 2003 – Making the Best Use of a Department of Clinical Radiology: Guidelines for Doctors (Royal College of Radiologists, United Kingdom) [9]
• European Guidelines for Multislice Computed Tomography, 2004 – CT Quality Criteria (European Commission) [10]
2. The decision to perform a CT examination must be justified based on the clinical setting and is a shared responsibility between the referring clinician and the radiologist. Alternative imaging methods that do not use ionizing radiation — such as ultrasound or magnetic resonance imaging (MRI) — should be considered if appropriate.
Prescribing or Requesting a CT Scan
The draft of the Safety Code being prepared by Health Canada outlines the responsibility of the referring physician with regards to prescribing or requesting x-ray procedures and states: “The main responsibility of the referring physician is to ensure that the use of xrays is justified.” In Ontario, the HARP Act indicates who can prescribe or request the operation of an x-ray machine for the irradiation of a human being. At some institutions, a member of the College of Nurses of Ontario who holds an extended certificate of registration may request an x-ray examination. Currently, where a local Medical Directive is in place, some nurses or other authorized health care professionals may be requesting x-ray examinations, including CT scans.
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 89
3. CT examinations should specifically be excluded from Medical Directives. The larger radiation doses generally associated with CT compared to those associated with conventional x-rays pose patient safety concerns in the use of Medical Directives for CT examinations.
4. The HARP Act should be revised to ensure that only individuals who have the appropriate clinical knowledge and training in radiation safety are permitted to prescribe or request CT examinations.
Pregnancy
Ionizing radiation is recognized to be potentially harmful to the developing fetus and is dose-dependent [5].
5. Each CT facility shall have a policy for screening women of childbearing age for pregnancy before performing a CT examination. If the patient is pregnant or possibly pregnant, the benefits of performing the CT must be weighed against any potential risk to the fetus.
Patient Shielding
Patient shielding devices are designed to reduce the amount of radiation absorbed by a particular body part. Shielding devices can be used to cover anatomic structures outside the area of irradiation that may receive scatter radiation (out-of-beam) or within the area of irradiation (in-beam). With state-of-the-art MDCT scanners, the x-ray beam is narrowly collimated. As a result, the majority of the radiation exposure that organs receive outside of the primary beam comes from internal scatter. The exception to this principle is when contiguous anatomy is significantly higher or lower than the area being scanned. Therefore, with MDCT scanners, the use of “out-of-beam” shielding is often of little or no practical benefit with regards to patient dose reduction. The Health Physics Society, an American scientific and professional organization whose members specialize in radiation safety, currently is of the opinion that the practice of out-of-beam shielding is of limited or no benefit but its use may provide psychological reassurance to the patient [11].
In-beam shields, however, are believed to provide a benefit in terms of dose reduction. Studies have shown that in-beam shielding can significantly reduce the dose to the breasts, thyroid gland, and eyes [12, 13]. However, in-beam shielding devices may interfere with image quality [14]. In addition, one of the features of MDCT scanners is automatic tube current modulation (also known as automatic exposure control or AEC), which aims to optimize the dose according to patient size and desired image quality. The technology for dose optimization with MDCT scanners, including AEC, is rapidly evolving and there is variation among vendors in the methods used for automatic tube current modulation [15]. Currently, there is a paucity of literature on the subject of inbeam shielding for state-of-the-art MDCT scanners, including a discussion of the interaction between such shields and AEC, and the resulting impact on dose and image quality.
Some in-beam shielding devices, such as eye shields, are intended for single use, while others, such as breast shields, are designed for multiple uses. When considering the use of patient shielding devices, the cost and disposability of these devices, the impact on workflow, and any infection control issues should be taken into consideration.
All facilities with CT scanners should consider maintaining an inventory of the following protective accessories:
o In-beam protection:
• eye shields; • breast shields (in sizes appropriate to the patient population — small, medium, large);
90 The College of Physicians and Surgeons of Ontario
• thyroid shields; • gonadal shields;
o Out-of-beam protection:
• wrap-around skirts or lead sheets that meet provincial standards.
6. The Radiation Protection Officer (RPO) at each facility shall develop a policy for patient shielding specifically for CT. The policy should be appropriate for the facility’s CT equipment and patient population, and include protocols for in-beam and out-of-beam shielding accessories. The policy should be reviewed on a regular basis, taking into consideration changes in practice and technological innovations. The analysis leading to the facility’s shielding policy should be documented and explained to front-line staff so that they may answer patients’ questions. The policy should cite each available shielding option and why it is, or is not, appropriate for the stated use.
If in-beam shielding is observed to increase repeat examinations, the facility’s shielding policy should be re-evaluated.
7. The Committee recommends that in-beam shielding not be used under the following conditions:
a) when real-time dose modulation is used and the presence of the shield will cause the CT scanner to compensate by increasing dose; or
b) where there is proof that in-beam shielding will interfere with the imaging objectives.
Anatomic Coverage
The unnecessary irradiation of organs outside the area of clinical interest can be minimized by limiting scanning to the anatomic area in question. For example, in most patients with renal colic, it would be appropriate to limit anatomic coverage from the top of the kidneys to the bladder base. On the other hand, for a patient with a suspected or proven intra-abdominal malignancy, for example, larger anatomic coverage, extending from the top of the diaphragm to the bottom of the bony pelvis, would be more appropriate.
8. The anatomic coverage of a CT examination should be limited to the area of clinical interest.
CT Protocols
CT protocols should be designed to obtain the necessary diagnostic information based on the clinical indication of each situation. In keeping with the ALARA principle, the dose should be optimized according to the clinical indication. For example, “low dose” protocols have been successfully used in scenarios with inherent high contrast such as evaluating urinary tract stones or screening for lung or colon cancer (CT colonography) [16-18]. Other clinical indications may require a higher dose with “low noise” to ensure optimum image quality. These situations occur when there is inherent low contrast between tumors and background structures. For example, when performing a preoperative CT for liver tumors or when evaluating a possible pancreatic tumor, the benefits of optimum image quality clearly justify any risks from irradiation. Finally, the majority of other protocols will fall into a “standard dose” category. Thus, CT protocols can be generally grouped into three categories: low dose, standard dose, and low noise.
Weight- and age-adjusted protocols should be developed and used for pediatric patients (see Pediatric CT) and small adults.

Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 91
9. CT protocols should be designed to obtain the necessary diagnostic information based on the clinical indication of each situation. CT protocols should be reviewed periodically by radiologists and CT technologists to ensure dose optimization.
CT Scanning Parameters
CT technologists and radiologists should be knowledgeable about how the manipulation of various scanning parameters may influence dose and image quality. With the rapid changes in CT technology, technologists, radiologists, and medical physicists need to work closely with CT vendors because there will be parameters unique to each make and model of CT scanner that will influence dose and image quality. Parameters that can influence dose and image quality include, but are not limited to: tube current (milliamperes or mA), tube rotation time, tube potential (peak kilovoltage or kVp), collimation, table speed, pitch, scanner geometry, x-ray filters, and reconstruction kernel or algorithm [19]. A common and effective method of reducing dose while maintaining diagnostic image quality with MDCT scanners is the use of automatic tube current modulation, also known as automatic exposure control (AEC). Each make and model of CT scanner may construct and apply AEC differently. Therefore, it is imperative that technologists and radiologists understand how this feature influences dose and image quality in their specific equipment. In newer MDCT scanners that can be adjusted to reduce dose, the ability to select a user-defined noise level that will influence image quality is an important parameter that is closely related to the AEC feature [15].
10. CT technologists and radiologists must be knowledgeable about how the manipulation of various scanning parameters may influence dose and image quality in their CT scanner.
Multiphase Image Acquisition
The acquisition of more than one set of images from the same anatomic region should be justified based on detailed medical and radiological knowledge. For example, multiple phases are often needed to detect and characterize liver nodules in patients with cirrhosis [20]. As another example, when performing CT urography for evaluating the urinary tract, some published protocols have used up to four acquisitions through the kidneys [21], while others have used only two [22]. This reduction in phases of image acquisition has been accomplished by altering the sequence of intravenous (IV) contrast injection and image acquisition, thereby reducing the total potential dose to the patient without significantly diminishing the goals of the examination.
11. The acquisition of more than one set of images from the same anatomic region should be justified based on detailed medical and radiological knowledge.
Repeat CT Studies
12. When a follow-up or repeat CT examination is requested, the referring clinician and the radiologist must first consider other imaging modalities that do not use ionizing radiation, such as ultrasound or MRI. Repeat CT examinations must be justified based on the clinical indication. If a follow-up CT examination is justified, the examination may be modified to reduce the dose, as long as clinical care is not compromised.
CT Manufacturers/Vendors
In Ontario and elsewhere, when a new CT scanner is installed, CT technologists are trained in the operation of that specific CT scanner by the vendor. Like most sophisticated machinery that
92 The College of Physicians and Surgeons of Ontario
incorporates powerful computers and state-of-the-art engineering, CT scanners have manufacturer-specific features. In recent years, manufacturers of MDCT scanners have focused more attention on dose optimization and have introduced new features to reduce dose while maintaining diagnostic image quality.
CT technologists and radiologists need to work closely with the vendor when a new make or model of CT scanner is installed in order to properly understand the features that determine dose and image quality in the new CT scanner.
Although MOHLTC approves the installation of CT scanners, the vendor typically conducts training and equipment maintenance.
13. Upon installation of a new CT scanner, a facility’s Radiation Protection Officer (RPO) shall provide the X-ray Inspection Service (XRIS) of MOHLTC proof that the technologists and physicians operating that specific make and model of CT scanner have received training on dose reduction strategies appropriate to the planned clinical operation of that scanner. This proof would be in the form of a certificate of training provided by the vendor. In addition, the RPO must keep a permanent record of authorized operators and their training status on installed CT scanners for review by MOHLTC and its enforcement agents for at least six years, in keeping with Section 8(7) of Regulation 543 of the HARP Act.
Diagnostic Reference Levels
There is tremendous variation in CT protocols and in the engineering of CT machines. Thus, the dose related to a given CT protocol can vary greatly among CT scanners and health care facilities. A number of factors will influence the protocols used at each facility, including, but not limited to: the make and model of CT scanner, the range of clinical indications and their complexity, local expertise, efficient patient throughput, and the spectrum of patients (including their age, gender, and body habitus).
The implementation of Diagnostic Reference Levels (DRLs) is one tool for radiation dose management [23, 24]. DRLs are determined by means of a survey of current practice to establish typical dose levels in a given geographic region. They are used to provide guidance for dose management rather than to set limits. A survey of patients of a standardized size is conducted, often with further measurements performed using phantoms designed for the procedure. Common CT studies such as for the head, chest, and abdomen/pelvis are chosen and a survey is conducted of the doses associated with these studies, at multiple hospitals. A threshold, such as the 80th percentile of recorded radiation doses, or more than twice the standard error of the mean, is then selected as the Diagnostic Reference Level. Institutions are then able to compare their standard doses to the DRL for each of the standard studies. If doses routinely exceed the suggested DRL, an investigation can be conducted to determine if the doses are justified or if the CT protocols can be further optimized. Thus, the purpose of DRLs is to reduce the overall radiation burden to the population over time. Diagnostic Reference Levels have been established in the United Kingdom, the European Union, and the province of British Colombia [25]. In the United States, the American Association of Physicians in Medicine recommends reference values for CT [26] and the American College of Radiology currently incorporates reference values into their accreditation program for CT [27]. The Phase II Report of the MRI and CT Expert Panel submitted to MOHLTC in December 2006 recommended that all existing CT facilities obtain American College of Radiology (ACR) accreditation within a three-year timeframe and that all future CT facilities obtain ACR accreditation within two years of CT installation.
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 93
Diagnostic Reference Levels can be expressed in various units, including CTDIvol (CT dose index volume) and DLP (dose length product). The CTDIvol and DLP values can then be converted to estimate the effective dose. The International Commission on Radiation Protection (ICRP) draft emphasizes that “effective dose is intended for use as a protection quantity on the basis of reference values and therefore should not be used for epidemiological evaluations, nor should it be used for any specific investigations of human exposure. ...The use of effective dose for assessing the exposure of patients has severe limitations”[28].
The ICRP states that it is inappropriate to use DRLs for regulatory or commercial purposes. Moreover, the values should be selected by professional medical bodies and be reviewed periodically [28].
14. Ontario should establish Diagnostic Reference Levels for the following CT examinations: head CT, chest CT, and abdominal/pelvic CT. A team consisting of members from professional medical bodies should be established to review the methods for establishing DRLs, administer the survey, collect the data, determine the DRLs, and disseminate the information to all stakeholders. Once established, DRLs should be reviewed periodically. Funding that is appropriate to the scope of the project will be required.
15. Manufacturers of CT scanners (including Positron Emission Tomography/CT units) must display the dose, which follows a currently accepted standard, for each CT examination on the control console.
16. The dose for each CT examination must be recorded. This record must be kept and be available for periodic audit for a minimum period of time, such as six years, in accordance with the HARP Act.
17. In pediatric cases, the size of the CT phantom used in calculating dose information must be displayed.
PEDIATRIC CT
The use of CT in children is increasing throughout the world, probably even more rapidly than in adults, with an estimated 2.7 million pediatric CT examinations per year in the U.S., with 30% of these patients undergoing at least three scans [29]. This increase in practice is seen in pediatric hospitals as well as in general community hospitals. Children undergoing repeated CT scans in the follow-up of chronic illnesses are of particular concern with regards to cumulative dose.
Multidetector CT technology enables much faster scanning than previous single slice technology, with a significant reduction in the need for sedation or anesthesia in children. This has made the CT scanning of children more accessible and user-friendly compared to a decade ago. The ever-increasing capabilities and diagnostic quality of CT have also broadened its applications in pediatric care. For example, CT angiography, high resolution chest CT, trauma care, and oncology (cancer) follow-up scans are all significantly easier to perform and are of higher diagnostic quality now than in the past.
However, the concerns related to the use of ionizing radiation are of particular importance in children because their sensitivity to its effects is greater than that of adults.
There is an exponential increase in lifetime cancer risk with decreasing age [30, 31]. This means that a child is more likely to develop a malignancy later in life than an adult exposed to the same amount of radiation, and the younger the child, the greater the risk he/she would have. Multiple factors contribute to this increased sensitivity in children, including the patients’ size, their organ development, and their greater life expectancy, over which any resultant malignancies can manifest. As a result, children are between two and ten times more vulnerable than adults to the effects of ionizing radiation.
Many imaging needs in children can be achieved using modalities that do not use ionizing radiation, namely, ultrasound and MRI. The applications of ultrasound in children are often wider than in adults
94 The College of Physicians and Surgeons of Ontario
due to smaller patient size and thinner body habitus. MRI also has a significant role, although there is an ongoing need for greater availability and expertise. Pediatric patients frequently require sedation or anesthesia for MRI examinations due to the longer time required for image acquisition. This carries its own risks, and requires resources for the administration of sedation or anesthesia and for patient monitoring.
In 2001, several scientific articles highlighted the risks associated with the levels of ionizing radiation involved in pediatric CT and the importance of reducing radiation dose when scanning children [32-34]. There is now increased awareness internationally among radiologists of the need to adjust CT settings for pediatric patients rather than using standard adult protocols, which results in unnecessarily high radiation doses to children.
However, there remains considerable variation among institutions in the technical parameters used in pediatric scanning. This has been demonstrated in many countries, including the U.K., the E. U., and the U.S. [10,24,33], and was also recently highlighted in the 2006 Annual Report of the Office of the Auditor General of Ontario [3]. This variability in technical parameters and patient dose is not confined to pediatric patients but is of particular concern in children, given their increased vulnerability to ionizing radiation.
CT manufacturers are making progress in developing specific pediatric protocols with dose-saving features, and new approaches continue to evolve. Such development, along with ongoing, collaborative research with clinical users, should be actively encouraged.
The variability in performance characteristics among CT manufacturers and scanner types means that one particular set of pediatric protocols will not optimize the performance characteristics of all scanners. Scanner performance and dose implications are affected by multiple factors, including type and number of detectors, scanner geometry, and filtration. It is therefore necessary for CT users to work in conjunction with their vendor to establish appropriately optimized pediatric protocols for their scanner.
General guidelines on the principles of achieving dose reductions in pediatric CT are available from sources in Canada, the U.S., and Europe [34-39]. These include using weight-adjusted tube current (mAs); reducing kVp, pitch, and slice width selection; using AEC (automatic exposure control) technology; avoiding pre-contrast scans and multiphase imaging when possible; limiting region of anatomic coverage; and establishing further dose-reducing protocols for specific clinical indications or follow-up examinations. Examples of institution-specific pediatric protocols are also available [34-
40].
Pediatric CT dosimetry is a developing area of scientific research. The variability in the size of pediatric patients — from premature babies to teenagers — increases the complexity of establishing dose measures and risk estimates. Commonly displayed dose measures such as CTDIvol and DLP are often based on phantoms intended for adult patients. Further work on the validity of dose measures, on the most appropriate phantoms and dose measures for use in pediatric CT, and on a uniform method of dose display among manufacturers, is needed.
Diagnostic Reference Levels for two pediatric studies (CT head and thorax) have been suggested recently in the U.K [24]. These are not yet in widespread use, partly due to the complexities given above. This is, however, an area of ongoing international development, and institutions in Ontario and across Canada should be encouraged tocontribute to these advances.
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 95
18. All requests for CT examinations for children must be reviewed by a radiologist prior to booking to ensure that the referral is appropriate and that possible alternative imaging modalities have been considered. It is the joint responsibility of the referring physician and the radiologist to ensure that the optimal imaging management occurs for each patient, taking into account both benefits and risks.
19. Each CT facility must establish local protocols for use in pediatric scanning. These protocols may be suggested by the manufacturer or be developed based on local expertise. The establishment of further dose-reducing protocols for specific clinical indications should be encouraged. The RPO must demonstrate to MOHLTC that technologists and radiologists operating the CT scanner have received instruction on the appropriate use of pediatric protocols.
20. All CT manufacturers must have suggested protocols specific to children of varying ages available on all models of scanner, for all commonly performed examinations.
21. As an additional safeguard to promote the use of weight-adjusted protocols in children, it is recommended that all manufacturers adapt CT software to promote protocol adjustments based on patient weight.
CT TECHNOLOGIST TRAINING
Medical Radiation Technologists (MRTs) working in CT in Ontario are primarily Radiological (x-ray) Technologists with enhanced CT knowledge, skill, and judgment.
MRTs, including those who perform CT, are governed by national standards developed by the national professional association, the Canadian Association of Medical Radiation Technologists (CAMRT). These standards are identified in the competency profile provided by CAMRT. In some provinces, including Ontario, MRTs are also regulated by provincial standards. The College of Medical Radiation Technologists of Ontario (CMRTO) is the regulatory body for MRTs in Ontario. In order to practice medical radiation technology in Ontario, an MRT must possess a CMRTO certificate of registration.
There are four specialties within CMRTO: Radiography, Nuclear Medicine, Radiation Therapy, and Magnetic Resonance Imaging. CT is not a specialty within the College. MRTs in any specialty registered with CMRTO can perform CT, assuming they have the knowledge, skill, and judgment to perform CT.
The educational requirements for MRTs are covered by the registration regulations. For a CT technologist, basic CT knowledge is acquired in their initial undergraduate/college program in one of the specialties. Most CT training is presently acquired “on the job,”during employment as an MRT. Employers/hospitals usually set minimum requirements for knowledge, skill, and judgment, but there are no standards. CAMRT offers a specialty certificate in computed tomography imaging (CTIC). The specialty certificate demonstrates that a higher level of CT knowledge has been achieved. CAMRT has recently revised all MRT competency profiles to reflect current and future MRT practice, including the practice of CT by MRTs in all specialties. These new profiles will be effective for the 2011 certification examinations. The level of CT expertise within each discipline’s competency profile differs depending on the CT practice within that specialty. For example, the Radiological Technology profile includes in-depth CT competencies related to diagnostic CT, whereas the Nuclear Medicine profile includes competencies related to the performance of PET/CT (positron emission tomography/CT), and the Radiation Therapy
96 The College of Physicians and Surgeons of Ontario
profile includes CT competencies related to radiation therapy planning. With the advent of hybrid imaging such as PET/CT, all specialties will be performing CT to some degree and level.
In October 2004, MOHLTC established an MRI and CT Expert Panel. A Phase I Report, submitted in April 2005, provided recommendations on the education of CT technologists. This report included a recommendation (Recommendation 10) for Ontario MRT programs to expand their curricula to include CT competencies and to provide training to current technologists to upgrade their skills. The report is posted on the MOHLTC website: http://www.health.gov.on.ca/renouvellement/wait_timesf/wt_reportsf/mri_ct.pdf.
In response to this recommendation, MOHLTC has provided funding to The Michener Institute in Toronto to develop a CT curriculum. The curriculum will provide a standard level of education for CT technologists across Ontario by offering CT courses as part of full-time undergraduate imaging programs and by providing graduate MRTs access to the same CT educational opportunities. Course development has begun, with input from a variety of stakeholders.
The following are key elements of the curriculum development:
a) the curriculum receives funding and support from MOHLTC for its development;
b) the curriculum establishes a standard level of education for CT technologists in Ontario;
c) the curriculum recognizes the increased complexity of knowledge and skill required of CT technologists;
d) the curriculum’s CT theory component includes optimization of image quality and dose management;
e) the curriculum includes management of quality control for CT equipment;
f) the curriculum recognizes the recent significant advances in CT technology;
g) the curriculum includes a hands-on laboratory component (most CT courses presently available focus on theory only); and
h) the curriculum is offered in distance format to ensure accessibility for all MRTs in Ontario.
The first course of the CT program will begin in May 2007. The curriculum will be available for inclusion in undergraduate MRT programs in Ontario.
The MRI and CT Expert Panel Phase II Report, submitted in December 2006, recommended that MRT programs continue to incorporate full CT competency into their curriculum.
22. MOHLTC should continue to provide support for a standardized CT curriculum for all undergraduate/college MRT programs and for access to the same curriculum for MRT graduates in Ontario.
23. The CT curriculum shall include training in radiation safety and dose management.
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 97
CT PERSONNEL AND THE WORK ENVIRONMENT
The safety of personnel in the CT environment is governed by provincial legislation. Federal guidelines and internal policy and procedures may be used as complementary measures and best practice standards. The current status of safety for CT personnel is attached in Appendix A, “Worker Radiation Protection in CT Applications.”
24. In addition to existing legislation and policies, CT facilities shall adopt the following safety guidelines:
a) Doors accessible to the general public that enter into a CT scan room must be locked during scanner operation. This will diminish the potential for unnecessary exposure to personnel working in the CT environment or to the general public. Locked doors also prevent interruption of a scan in progress.
b) CT operators must be within arm’s length of the scan abort button during image acquisition.
c) CT operators must be in visual contact with the patient during image acquisition.
CT SCANNER TESTING AND INSPECTION
The X-ray Inspection Service (XRIS) is a unit within MOHLTC and is the enforcement body for the HARP Act. XRIS works at arm’s length from the HARP Commission.
Currently, CT scanners are not inspected by XRIS and are excluded from the HARP Act in this regard.
25. The testing and inspection of CT scanners should be specifically incorporated into the HARP Act. This may require a major revision to the HARP Act and the X-ray Safety Code. The role and duties of X-ray Inspection Service may also need to be modified so that XRIS is able to perform and audit the inspection and maintenance of CT scanners, including dental cone beam CT, in Ontario. The appropriate resources to expand this service will be necessary.
EDUCATION MATERIALS
Health Care Workers
Recent studies have shown that there is a lack of awareness among patients and physicians regarding the magnitude of radiation doses involved in CT and its associated risks [41, 42]. An increased awareness of the risks and benefits of procedures using ionizing radiation would help health care workers make appropriate decisions for their patients and would reduce the risk of unnecessary patient exposure to radiation. The draft of the Safety Code currently being prepared by Health Canada states that the referring physician, who is the individual authorized to prescribe or request x-ray procedures, should “be aware of the risks associated with x-ray procedures.”
98 The College of Physicians and Surgeons of Ontario
26. The province should designate an organization to develop and disseminate information to physicians and other health care workers that helps them to better weigh the benefits and risks of CT studies for their patients. The topic of benefits and risks of procedures that use ionizing radiation such as CT should be included in the training programs of health care providers who are involved in the prescribing or performing of such procedures.
Patients
Health care is a shared responsibility between health care providers and patients. In order to participate in the decision-making process, patients should be aware of the basic benefits and risks of a CT scan and, indeed, of any test for diagnostic or therapeutic purposes. Any material provided for patients should be presented in a way that does not provoke anxiety in patients, but rather provides an appropriate perspective for making decisions.
27. The province should designate an organization to develop and disseminate information concerning the benefits and risks of imaging studies involving ionizing radiation, specifically CT, to patients and the general public.
Using a website to provide the above information would be an effective way to disseminate educational materials to patients and health care workers. The educational material for patients would be accessible to the general public, whereas the educational material for health care workers would be available through professional organizations such as the College of Physicians and Surgeons of Ontario (CPSO) and CMRTO. The content of these educational materials would require input from several groups, including, but not necessarily limited to: Ontario Association of Radiologists (OAR), CPSO, and CMRTO. Such a website would require funding for its development and maintenance.
MONITORING PATIENT DOSE
Increased awareness among patients and health care workers that any amount of ionizing radiation is potentially harmful is, in and of itself, likely to help promote the safe and appropriate use of CT scanners and other devices that use ionizing radiation. It is recognized that there is a cumulative risk from multiple examinations or procedures that use ionizing radiation. If it were possible to collect the data and monitor the cumulative dose from all radiation emitting devices that patients were exposed to, patients may be more likely to avoid investigations and procedures that use ionizing radiation. One potential method of monitoring patient dose is the concept of a “dose card” that could document cumulative dose.
The concept of a “dose card” for each patient was reviewed by the Committee. A “dose card” would be part of a patient’s permanent medical record. Each time an investigation or procedure using ionizing radiation was performed, the dose would be recorded. The advantage of such a system would be that a patient’s cumulative dose could be monitored. However, there are a number of important issues and limitations to such a proposal. Currently, dose information is captured in different units by different radiation emitting devices. The dose information from a CT examination can be expressed in various units, the two most common being CTDIvol (CT dose index volume) and DLP (dose length product). Typically, both these measurements are displayed on the CT console for each CT examination. It must be noted, however, that these measurements are an indirect estimate of dose. More work on the validity of DLP estimates, especially in children, is needed.
Exact measurements of dose in a given patient for a given CT study would be difficult to determine and could involve time-consuming and complex measurements and calculations. In addition, new methods and standards to quantify dose for MDCT may be introduced in the future. The current lack of
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 99
measurement standardization across the range of radiation emitting devices and the fact that doses are typically indirectly estimated are major obstacles to implementing a system for monitoring patient dose. Other issues include: who would be responsible for monitoring dose information; who would be responsible for calculating the risks for patients before they undergo an investigation or procedure using ionizing radiation; and how useful would this information be if patients forget to bring their dose card to an examination/procedure. Furthermore, setting an absolute dose limit would not be appropriate because the benefits and risks of each procedure must be assessed on an individual basis in the context of the patient’s overall care.
28. At this time, given the above limitations, the Committee does not recommend attempting to establish a permanent, portable record of the cumulative dose that each patient in Ontario receives. Once a comprehensive, electronic record-keeping system is in place for the citizens of Ontario, it would allow for at least a record to be kept of the type and frequency of x-ray examinations. This information may influence a physician’s decision when considering a request for imaging tests.
DENTAL CONE-BEAM CT (CBCT)
Currently, panoramic radiology is used for many conventional diagnostic dental examinations and is associated with a significantly lower radiation dose compared to dental cone-beam (CBCT) scanners, which use cone-beam CT technology [43]. Dental CBCT scanners are specifically designed for advanced dental applications and are used primarily for dental implant and orthognathic surgical planning. Other applications include 3D localization of impacted teeth and diagnosis of pathology related to the maxilla and mandible. Compared to CT scanners used for “body” imaging, dental CBCT scanners are relatively simple and use significantly lower radiation doses to produce high-resolution images. Image acquisition is almost completely automated, with a limited number of parameters that can be adjusted.
However, if dental CBCT scanners become readily available for use by general dentistry practices, it is possible that this technology will replace panoramic radiology for conventional diagnostic dental examinations. This raises concerns about a potential increase in patient and population exposure to radiation. Also of concern is the current lack of training for general dentists in the interpretation of images generated by dental CBCT scanners. Within the dental profession, the specialty of Oral and Maxillofacial Radiology has training in both the application and the interpretation of images produced by dental CBCT scanners.
The HARP Act currently states who is qualified to operate an x-ray machine [Section 5 (1) (2)] and who can prescribe the operation of an x-ray machine (Section 6). The HARP Act does not specifically state who can operate a dental CBCT scanner or who can prescribe the operation of a dental CBCT scanner. Currently, MOHLTC does not approve requests for installation and operation of additional dental CBCT scanners in Ontario.
29. The HARP Act should be revised to reflect the newer technology of dental CBCT.
30. MOHLTC should lift the current moratorium on approval of dental CBCT scanners, but approval should be restricted to Oral and Maxillofacial Radiologists and graduate Oral Radiology academic centres.
100 The College of Physicians and Surgeons of Ontario
31. Dental CBCT scanners must be operated under the supervision of an Oral and Maxillofacial Radiologist.
32. All requests for dental CBCT examinations must be reviewed and approved according to protocol by an Oral and Maxillofacial Radiologist prior to performing the examination.
RESEARCH
Because CT technology is advancing rapidly, the current research base for clinical guidance is limited. Close collaboration among CT manufacturers, imaging scientists, and radiologists should be encouraged to further explore and promote methods of dose management for CT. Therefore, the appropriate resources will be required to keep pace with these changes.
33. Close collaboration among CT manufacturers, imaging scientists, and radiologists is encouraged to further explore and promote methods of dose management for CT.
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 101
REFERENCES
1. Computed Tomography Radiation Safety Issues in Ontario. Available at: www.health.gov.on.ca
2. Magnetic Resonance Imaging Environment Safety in Ontario. Available at: www.health.gov.on.ca
3. 2006 Annual Report of the Office of the Auditor General of Ontario. Chapter 3, Section 3.06. Hospitals – Management and Use of Diagnostic Imaging Equipment. Available at: www.auditor.on.ca
4. United Nations Scientific Committee on the Effects of Atomic Radiation to the General Assembly, 2000. Sources and effects of ionizing radiation, Volume 2, Effects. Available at: www.unscear.org
5. Health Risks from Exposure to Low Levels of Ionizing Radiation: BEIR VII – Phase 2 Report. Available at: www.nap.edu/catalog/11340.html
6. International Commission on Radiological Protection. New draft report for consultation: multidetector computed tomography. Available at: www.icrp.org
7. Diagnostic Imaging Referral Guidelines (Canadian Association of Radiologists).First Edition, 2005.
8. American College of Radiology Appropriateness Criteria 2000 (AmericanCollege of Radiology).
Available at: www.acr.org
9. Royal College of Radiologists 2003 – Making the Best Use of a Department of Clinical Radiology: Guidelines for Doctors. 5th Edition. London: The Royal College of Radiologists, United Kingdom.
10. European Guidelines for Multislice Computed Tomography 2004 – CT Quality Criteria (European Commission).Available at: www.msct.eu
11. Health Physics Society. “Ask the Experts,” Category: Medical and Dental Equipment/Sheilding.
Available at: www.hps.org
12. Hohl C, Wildberger JE, Suss C, Thomas C, Muhlenbruch G, Schmidt T et al. Radiation dose reduction to breast and thyroid during MDCT: effectiveness of an in-plane bismuth shield. Acta Radiologica 2006 July; 47:562–567
13. Fricke BL, Donnelly LF, Frush DP et al. In-Plane bismuth breast shields for pediatric CT: effects on radiation dose and image quality using experimental and clinical data. AJR Feb 2003; 180:407–411
14. Geleijns J, Salvado Artells M, Veldkamp WJH, Lopez Tortosa M, Calzado Cantera A. Quantitative assessment of selective in-plane shielding of tissues in computed tomography through evaluation of absorbed dose and image quality. European Radiology Oct 2006; 16:2334–2340
15. McCollough CH, Bruesewitz MR, Kofler JM. CT dose reduction and dose management tools: overview of available options. Radiographics 2006; 26: 503–512
16. Heneghan JP, McGuire KA, Leder RA et al. Helical CT for nephrolithiasis and ureterolithiasis: comparison of conventional and reduced radiation-dose techniques. Radiology 2003; 229:575–580
17. Kaneko M, Kusumoto M, Kobayashi T et al. Computed tomography screening for lung carcinoma in Japan. Cancer 2000; 89:2485–2488
18. van Gelder RE, Venema HW, Serlie IW et al. CT colonography at different radiation dose levels: feasibility of dose reduction. Radiology 2002; 224:25–33
19. Kalra MK, Maher MM, Toth TL et al. Strategies for CT radiation dose optimization. Radiology 2004; 230:619–628
102 The College of Physicians and Surgeons of Ontario
20. Iannaccone R, Laghi A, Catalano C et al. Hepatocellular carcinoma: role of unenhanced and delayed phase multi-detector row helical CT in patients with cirrhosis. Radiology 2005; 234:460–467
21. Caoili EM, Cohan RH, Inampudi P et al. MDCT urography of upper tract urothelial neoplasms. AJR 2005; 184:1873–1881
22. Chai RY, Jhaveri K, Saini S, Hahn PF, Nichols S, Mueller PR. Comprehensive evaluation of patients with haematuria on multi-slice computed tomography scanner: protocol design and preliminary observations. Australasian Radiology 2001; 45:536–538
23. Gray JE, Archer BR, Butler PF et al. Reference values for diagnostic radiology: application and impact. Radiology May 2005; 235:354–358
24. Shrimpton PC, Hillier MC, Lewis MA, Dunn M. Doses from computed tomography examinations in the UK – 2003 review. NRPB – W67, NRPB Publications. Available at: www.hpa.org.uk
25. Aldrich JE, Bilawich AM, Mayo JR. Radiation doses to patients receiving computed tomography examinations in British Colombia. CARJ 2005; 57:79–85
26. American Association of Physicists in Medicine.Available at: www.aapm.org
27. American College of Radiology. Available at: www.acr.org
28. Radiological Protection and Safety in Medicine. Annals of the ICRP, 1997.
29. Mettler Jr. FA, Wiest PW, Locken JA, Kelsey CA. CT scanning: patterns of use and dose. J Radiol Prot 2000; 20:353–359
30. Khursheed A, Hillier MC, Shrimpton PC et al. Influence of patient age on normalized effective doses calculated for CT examinations. Br J Radiol 1997; 75: 819–830
31. Huda W, Atherton JV, Ware DE, Cumming WA. An approach for the estimation of effective radiation dose at CT in pediatric patients. Radiology 1997; 203(2):417–422
32. Brenner DJ, Elliston CD, Hall EJ, Berdon WE. Estimated risks of radiation-induced fatal cancer from pediatric CT. AJR 2001; 176:289–296
33. Paterson A, Frush DP, Donnelly LF. Helical CT of the body: are settings adjusted for pediatric patients? AJR 2001; 176:297–301
34. Donnelly LF, Emery KH, Brody AS et al. Minimizing radiation dose for pediatric body applications of single-detector helical CT: strategies at a large children’s hospital. AJR 2001; 176:303–306
35. Strategies for minimizing radiation dose in pediatric CT. Guidelines from the Hospital for Sick Children, Toronto.Available at: www.sickkids.ca/diagnosticimaging
36. Frush DP, Soden B, Frush KS, Lowry C. Improved pediatric multidetector CT using a size-based color-coded format. AJR 2002; 178: 721–726
37. Verdun FR, Lepori D, Monnin P, Valley JF, Schnyder P, Gudinchet F. Management of patient dose and image noise in pediatric CT abdominal examinations. Eur Radiol 2004; 14:835–841
38. Cody DC, Moxley DM, Krugh KT, O’Daniel JC, Wagner LK, Eftekhari F. Strategies for formulating appropriate MDCT techniques when imaging the chest, abdomen, and pelvis in pediatric patients. AJR 2004; 182:849–859
39. Voch P. CT dose reduction in children. Eur Radiol 2005; 15:2330–2340
40. Adult and pediatric CT protocols from the Johns Hopkins Hospital. Available at: www.CTisus.com

Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 103
41. Lee CI, Haims AH, Monico EP, Brink JA, Forman HP. Diagnostic CT scans: assessment of patient, physician, and radiologist awareness of radiation dose and possible risks. Radiology 2004; 231:393–398
42. Thomas KE, Parnell-Parmley JE, Haidar S, Moineddin R, Charkot E, BenDavid G et al. Assessment of radiation dose awareness among pediatricians. Pediatric Radiology 2006; 36:823–832
43. Ludlow JB, Davies-Ludlow LE, Brooks SL, Howerton WB. Dosimetry of three CBCT devices for oral and maxillofacial radiology: CB Mercuray, NewTom 3G, and i-CAT. Dentomaxillofacial Radiology 2006; 35:219–226
104 The College of Physicians and Surgeons of Ontario
Appendix A - Worker Radiation Protection in CT Applications Installation Approval
The MOHLTC’s current policy is that any x-ray machine used to irradiate a human being —
including CT scanners — for any purpose, including research and analysis, is covered
by the HARP Act and must be approved and designated according to the HARP Act prior
to installation and operation. Proposed installations are reviewed by the X-ray Inspection
Service of the MOHLTC and must comply with Regulation 543: X-ray Safety Code
under the HARP Act, as well as with Appendix 2 of Safety Code 20A (federal legislation).
For facilities under Ministry of Labour jurisdiction (e.g., veterinary, forensic, training
exclusively with phantoms, research), CT installations are further required to have locks
or interlocks on all entry doors.
The following radiation protection requirements are subject to Regulation 861/90,
respecting X-ray Safety and Regulation 67/93 for Health Care and Residential Facilities,
made under the Ministry of Labour’s Occupational Health and Safety Act.
Radiation Safety Training
As required under the Occupational Health and Safety Act, Section 25 (2) (a) and (d)
state:
25 (2) Without limiting the strict duty imposed by subsection (1), an employer shall:
(a) provide information, instruction and supervision to a worker to protect the health or
safety of the worker;
(d) acquaint a worker or a person in authority over a worker with any hazard in the work
and in the handling, storage, use, disposal and transport of any article, device, equipment
or biological, chemical or physical agent;
(x-rays are defined as a physical agent)
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 105
Further, under the Health Care and Residential Facilities Regulation (Regulation 67/93),
Section 9 (4) states:
The employer, in consultation with and in consideration of the recommendation of the
joint health and safety committee or health and safety representative, if any, shall
develop, establish and provide training and educational programs in health and safety
measures and procedures for workers that are relevant to the workers' work. O. Reg.
67/93, s. 9.
General Duty to Establish Measures and Procedures In consultation with the joint health and safety committee or representative, an employer
shall develop, establish, and put into effect measures and procedures for the health and
safety of workers.
Under the Health Care and Residential Facilities Regulation (Regulation 67/93), Section
9 (1) states:
The employer shall reduce the measures and procedures for the health and safety
of workers established under section 8 to writing and such measures and procedures
may deal with, but are not limited to, the following:
7. The hazards of biological, chemical and physical agents present in the workplace,
including the hazards of dispensing or administering such agents.
8. Measures to protect workers from exposure to a biological, chemical or physical agent
that is or may be a hazard to the reproductive capacity of a worker, the pregnancy of a
worker or the nursing of a child of a worker.
9. The proper use, maintenance and operation of equipment.
10. The reporting of unsafe or defective devices, equipment or work surfaces.
11. The purchasing of equipment that is properly designed and constructed.
12. The use, wearing and care of personal protective equipment and its limitations.
106 The College of Physicians and Surgeons of Ontario
Personal Radio-Protective Equipment The Ministry of Labour Radiation Protection Service has a written policy on personal
radio-protective equipment. For workers remaining in the room during a CT examination,
wrap-around aprons, along with thyroid collars having 0.5 mm lead equivalency at the
highest used kVp, are required to be worn.
Under the Health Care and Residential Facilities Regulation (Regulation 67/93), Section
10 states:
(1) A worker who is required by his or her employer or by this Regulation to wear or use
any protective clothing, equipment or device shall be instructed and trained in its care,
use and limitations before wearing or using it for the first time and at regular intervals
thereafter and the worker shall participate in such instruction and training.
(2) Personal protective equipment that is to be provided, worn or used shall:
(a) (a) be properly used and maintained;
(b) be a proper fit;
(c) be inspected for damage or deterioration; and
(d) be stored in a convenient, clean and sanitary location when not in use.
O. Reg. 67/93, s. 10.
Dosimetry Under the X-ray Safety Regulation 861/90, Section 12 states:
12. (1) An employer shall provide to each x-ray worker a suitable personal dosimeter that
will provide an accurate measure of the dose equivalent received by the x-ray worker.
(2) An x-ray worker shall use the personal dosimeter as instructed by the employer.
(3) An employer shall ensure that the personal dosimeter provided to an x-ray worker is
read accurately to give a measure of the dose equivalent received by the worker and shall furnish to the worker the record of the worker's radiation exposure.
(4) An employer shall verify that the dose equivalent mentioned in subsection (3) is
reasonable and appropriate in the circumstances, and shall notify an inspector of any dose
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 107
equivalent that does not appear reasonable and appropriate.
(5) An employer shall retain an x-ray worker's personal dosimeter records for a period of
at least three years. R.R.O. 1990, Reg. 861, s. 12.
The word "suitable" is defined by the Ministry of Labour as a personal dosimeter that
provides a measure of dose received by the exposed part of the body. All x-ray workers working
with fluoroscopic or other unshielded open-beam x-ray sources (including CT
systems, if remaining in the room) shall be provided with an additional head/collar badge
(worn on the exterior of the thyroid collar) and/or an extremity badge (worn as a ring on a
hand), where deemed appropriate.
Dosimetry is required for all persons who meet the definition of an x-ray worker,
including external workers who may service or test the CT machine.
Reporting of a high exposure or possible overexposure Under the X-ray Safety Regulation 861/90, Section 13 and 14 state:
13. Where a worker has received a dose equivalent in excess of the annual limits set out
in Column 4 of the Schedule in a period of three months, the employer shall forthwith
investigate the cause of the exposure and shall provide a report in writing of the findings
of the investigation and of the corrective action taken to the Director and to the joint
health and safety committee or health and safety representative, if any. R.R.O. 1990, Reg.
861, s. 13.
14. Where an accident, failure of any equipment or other incident occurs that may have
resulted in a worker receiving a dose equivalent in excess of the annual limits set out in
Column 3 of the Schedule, the employer shall notify immediately by telephone, telegram or other
direct means the Director and the joint health and safety committee or health and
safety representative, if any, of the accident or failure and the employer shall, within
forty-eight hours after the accident or failure, send to the Director a written report of the
circumstances of the accident or failure. R.R.O. 1990, Reg. 861, s. 14.
108 The College of Physicians and Surgeons of Ontario
Warning Signs Under the Health Care and Residential Facilities Regulation (Regulation 67/93),
Section 16 states:
A warning sign shall be posted on any door, corridor or stairway,
(a) that is not a means of egress but that is located or arranged so that it could be
mistaken for one; or
(b) that leads to a hazardous, restricted or unsafe area. O. Reg. 67/93, s. 16.
Under the X-ray Safety Regulation 861/90, Section 11 (1) and (3) state:
The following measures and procedures shall be carried out in a workplace where an xray
source is used:
1. X-ray warning signs or warning devices shall be posted or installed in
conspicuous locations.
3. Where the air kerma in an area may exceed 100 micrograys in any
one hour, access to the area shall be controlled by,
i. locks or interlocks if the x-ray source is one to which
subsection 6 (1) applies or is described in subsection 6 (2);
and
ii. barriers and x-ray warning signs if the x-ray source is
portable or mobile and is being so used.

Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 109
110 The College of Physicians and Surgeons of Ontario
Appendix V Sample Emergency Safety Policy Safety Training for all staff should be carried out. In addition, an emergency safety policy should be included in the policies and procedures manual. This appendix has been provided as a sample of what the policy may look like and include. Each policy must be site specific to the facility and may include but is not limited to the following areas: Employer Responsibilities (in all incident cases): Provide first aid in accordance with the regulations. Record first aid attention, adverse effects, incident report. Assist to provide immediate transportation to the hospital, doctor, worker/patient’s home, when/as necessary. Employee Responsibilities: Acute Care Transfer Should a patient, visitor, and/or staff become ill while in the clinic the following is carried out:
1. Immediately, the technologist or clerical staff will alert the attending Radiologist of the problem.
2. In the event that the attending Radiologist is not available, contact a local GP (agreement should be made prior between facility and physician – contact numbers should be available for staff).
3. If the physician is not immediately available, call 911, identify yourself and request transfer to the nearest hospital.
Fire Prevention and Control Plan
1. All staff members employed at the facility is required to know the fire plan. To facilitate this, an annual review of the plan will be carried out and is mandatory for all staff members.
2. The fire plan is site-specific for the facility. Staff members are required to familiarize themselves with the plan for this location.
3. Each employee should have the ability to assess the situation quickly and initiate appropriate measures upon discovering a fire. This may vary from using a fire extinguisher to contain a fire or alerting others, evacuating the building and calling the fire department.
If you discover a fire in your area:
1. Remove patients from rooms and out of danger. 2. Turn off lights, any electrical equipment, gases, and close windows and doors. 3. Pull the alarm located closest to you. 4. Dial 911 and advise the Fire Department of the Emergency. Give them your name, location of
the fire and type of fire to the communications operator (electrical, gas, other).
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 111
5. If possible (i.e the fire is contained to a specific area) go back to the room and attempt to put out the fire using a fire extinguisher.
DO NOT ATTEMPT TO USE THE FIRE HOSE. Everyone should be removed from the office. Have a staff member positioned at the main corridor junction to direct fire fighters. If you hear a fire alarm:
1. Collect all patients, visitors, and staff members in the facility and guide them to the closest exits.
2. DO NOT USE THE ELEVATOR. All staff members along with anyone in the office at the time of the evacuation alarm, must meet at a predetermined assembly point outside of the building.
3. Personnel will be requested to assist with duties such as checking the office before leaving ensuring that everyone is accounted for, turning off lights in the fire area, turning off gases (oxygen), turning off all electrical equipment and closing doors and windows.
The First Aid Box As a minimum the first aid box should contain:
• A current edition of a first aid manual. • One card of safety pins. • Dressings, consisting of:
o 12 adhesive dressings, individually wrapped o 4 sterile gauze pads, 3 inches square o 2 rolls of gauze bandages, 2 inches wide
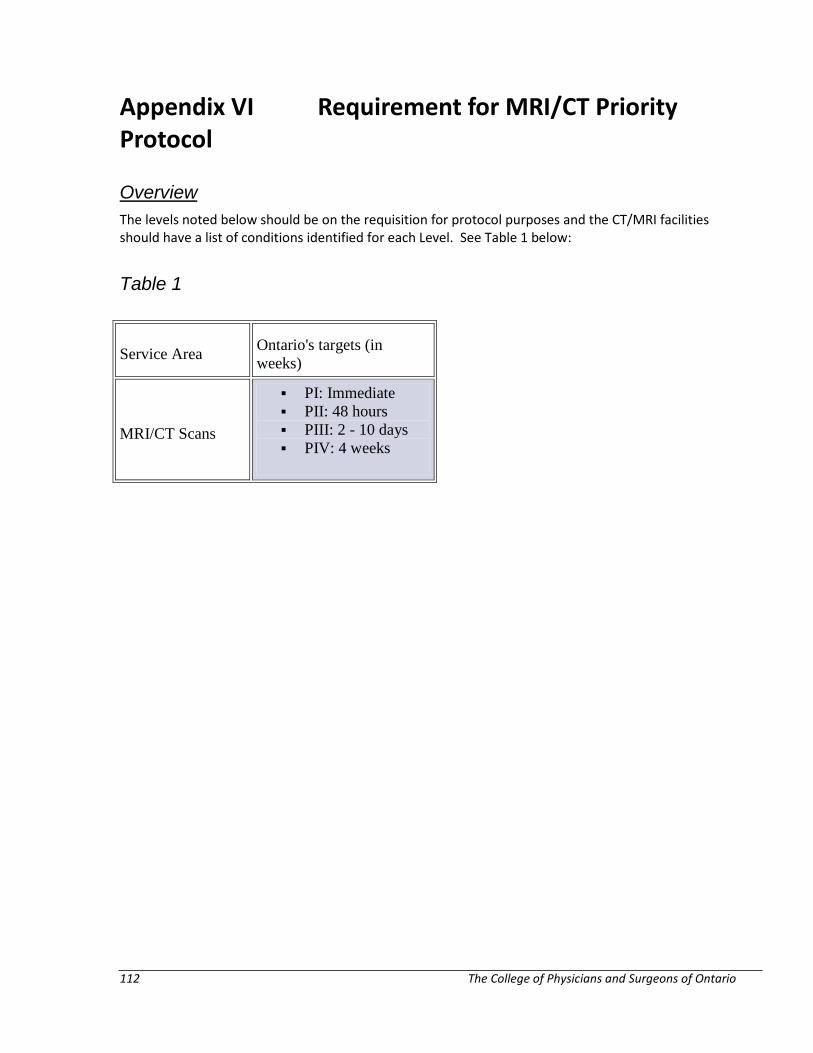
112 The College of Physicians and Surgeons of Ontario
Appendix VI Requirement for MRI/CT Priority Protocol Overview The levels noted below should be on the requisition for protocol purposes and the CT/MRI facilities should have a list of conditions identified for each Level. See Table 1 below:
Table 1
Service Area Ontario's targets (in weeks)
MRI/CT Scans
PI: Immediate PII: 48 hours PIII: 2 - 10 days PIV: 4 weeks
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 113
Appendix VII Prevention of IV Contrast Reaction Protocol ACR Manual on Contrast Media, Version 9: http://www.acr.org/quality-safety/resources/contrast-manual
For reference, below is a list of the Chapters and Tables that can be found in the ACR Manual on Contrast Media; all Chapters and Tables can be accessed using the above link:
Preface
Introduction
Chapter 1. Patient Selection and Preparation Strategies
Chapter 2. Injection of Contrast Media
Chapter 3. Extravasation of Contrast Media
Chapter 4. Allergic-Like and Physiologic Reactions to Intravascular Iodinated Contrast Media
Chapter 5. Contrast Media Warming
Chapter 6. Contrast-Induced Nephrotoxicity
Chapter 7. Metformin
Chapter 8. Contrast Media in Children
Chapter 9. Gastrointestinal (GI) Contrast Media in Adults: Indications and Guidelines
Chapter 10. Adverse Reactions to Gadolinium-Based Contrast Media
Chapter 11. Nephrogenic Systemic Fibrosis (NSF)
Chapter 12. Treatment of Contrast Reactions
Chapter 13. Administration of Contrast Media to Pregnant or Potentially Pregnant Patients
Chapter 14. Administration of Contrast Media to Women Who are Breast Feeding
114 The College of Physicians and Surgeons of Ontario
Tables
Table 1: Indications for Use of Iodinated Contrast Media
Table 2: Organ or System-Specific Adverse Effects from the Administration of Iodine-Based or Gadolinium-Based Contrast Agents
Table 3: Categories of Acute Reactions
Table 4: Treatment of Acute Reactions to Contrast Media in Children
Table 5: Management of Acute Reactions to Contrast Media in Adults
Table 6: Equipment for Contrast Reaction Kits in Radiology
APPENDIX A: Contrast Media Specifications
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 115
Appendix VIII Independent Health Facilities Act - Ontario Regulation 57/92 Note: Ontario Regulation 57/92 has previously been amended. Those amendments are listed in the Table of Regulations - Legislative History Overview which can be found at www.e-laws.gov.on.ca. Facilities are encouraged to check the Government Website for updates.
Quality Advisor and Advisory Committee 1(1) Every licensee shall appoint a quality advisor to advise the licensee with respect to the quality and standards of services provided in the independent health facility.
(2)If the quality advisor dies or ceases to be the quality advisor, the licensee shall appoint a new quality advisor forthwith.
(3)The quality advisor must be a health professional who ordinarily provides insured services in or in connection with the independent health facility and whose training enables him or her to advise the licensee with respect to the quality and standards of services provided in the facility.
(4)It is a condition of a licence that the quality advisor be a physician if all the insured services provided in the independent health facility that support the facility fees that the licensee may charge are provided by physicians.
(5)In subsection (4), an insured service supports a facility fee if the facility fee is for or in respect of a service or operating cost that supports, assists or is a necessary adjunct to the insured service.
(6)A licensee who is qualified under subsection (3) may appoint himself or herself as the quality advisor only if there is no other health professional who is qualified to be the quality advisor who will consent to be the quality advisor. O. Reg 57/92, s.1.
2(1)Every licencee shall appoint an advisory committee to advise the quality advisor.
(2)The advisory committee shall consist of health professionals who provide health services in or in connection with the independent health facility.
(3)The quality advisor shall be the chair of the advisory committee.
(4)Every licensee shall use his or her best efforts to ensure that there is a representative on the advisory committee from the health profession and each specialty and sub-specialty of medicine, practitioners of which provide health services in or in connection with the independent health facility. O.Reg. 57/92, s.2.
3(1)Every licensee shall give the Director the name of the quality advisor in writing forthwith after the quality advisor is appointed.
(2)If the quality advisor dies or ceases to be the quality advisor, the licensee shall inform the Director in writing forthwith.
(3)Every licensee shall give the Director, on request, the names of the members of the advisory committee in writing. O. Reg. 57/92, s.3.
116 The College of Physicians and Surgeons of Ontario
Standards 4 (1)Every licensee shall ensure that all aspects of the services provided in the independent health facility are provided in accordance with generally accepted professional standards.
(2)Every licensee shall ensure that the persons who provide services in the independent health facility are qualified, according to generally accepted professional standards, to provide those services.
(3)If the quality advisor has reasonable grounds to believe that this section is not being complied with, he or she shall inform the Director forthwith. O.Reg. 57/92, s.4.
5 Every licensee shall keep a system to monitor the results of the services provided in the independent health facility. O. Reg. 57/92, s.5.
6(1)Every licensee shall ensure that all tissues removed from a patient during an operation or curettage performed in an independent health facility are sent to a laboratory for examination and report unless the physician performing the operation or curettage is of the opinion that it is not necessary according to generally accepted medical standards.
(2)The licensee shall ensure that a short history of the case and a statement of the findings of the operation or curettage are sent with the tissues. O. Reg. 57/92, s.6.
Records of Employees 7 (1)Every licensee of an independent health facility shall maintain, for each employee of the facility who is not a physician, an employment record setting out the employee’s qualifications and employment history including a record of any registration with or licensing by the governing body of a health profession.
(2) Every licensee shall retain an employee’s employment record for at least two years after the employee ceases to be an employee. O.Reg. 57/92, s.7.
8 (1)Every licensee of an independent health facility shall maintain a record of qualifications and work history for:
(A) each person the licensee contracts with to manage the facility; and
(B) each person who is not a physician who the licensee contracts with to provide patient-related services in the facility.
(2)The record shall include a record of any registration with or licensing by the governing body of a health profession.
(3) Every licensee shall retain the record for a person the licensee contracts with for at least two years after the licensee ceases to contract with the person. O. Reg. 57/92, s.8.
9 (1)Every licensee shall maintain a declaration of professional standing for each physician who provides professional services in the independent health facility.
(2)A declaration of professional standing must include the following information:
1. The physician’s name
2. The physician’s registration number with the College of Physicians and Surgeons of Ontario
3. The physician’s number registered with the Health Insurance Division of the Ministry of Health.
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 117
4. The class of the physician’s licence issued under Part III of the Health Disciplines Act and any terms and conditions attached to it.
5. The physician’s specialty.
(3)Every licensee shall give the Director a copy of each declaration of professional standing, forthwith after the obligation to maintain it begins under subsection (1).
(4)Every licensee shall give the Director a written statement of any change in a declaration of professional standing forthwith after the change.
(5)Subsections (3) and (4) do not apply with respect to physicians providing services on a temporary basis for less than twelve weeks. O.Reg. 57/92, s.9.
Patient Records 10 (1) Every licensee of an independent health facility shall keep, for each person who is or was a patient, a health record relating to the health services provided in the facility.
(2)A patient’s health record must include:
(a) the patient’s name and home address
(b) the patient’s date of birth
(c) the patient’s health number
(d) the name of any attending physician or practitioner and his or her number as registered with the Health Insurance Division of the Ministry of Health
(e) the name of any referring physician or practitioner and his or her number as registered with the Health Insurance Division of the Ministry of Health
(f) a history of the patient
(g) a written record of any orders for examinations, tests, consultations or treatments
(h) particulars of any examination of the patient
(i) any reports of examinations, tests or consultations including any imaging media from examinations and any physicians’ interpretive or operative reports
(j) any reports of treatment including any physicians’ operative reports
(k) any orders for and reports of any discharge of the patient from supervised care
(l) any consents; and
(m) any diagnoses of the patient.
(3)A) patient’s health record need not contain a history of the patient if the patient came to the independent health facility for diagnostic services only and received on such service.
(4)Every licensee shall ensure that every part of a patient’s record has a reference on it identifying the patient or the record.
(5)If information in a patient’s record is kept in the form of a chart, each entry in the chart must be dated and it must be initialled by the person authorizing the entry. O.Reg. 57/92, s.10.
11 (1) Every licensee shall retain a patient’s health record or a copy of it for at least six years following:
118 The College of Physicians and Surgeons of Ontario
(a) the patient’s last visit; or
(b) if the patient was less than eighteen years old when he or she last visited the facility, the day the patient became or would have become eighteen years old.
(2)Despite subsection (1), a licensee is not required to retain imaging media from any examination other than a mammography for more than three years following:
(a) the patient’s last visit; or
(b) if the patient was less than eighteen years old when he or she last visited the facility, the day the patient became or would have become eighteen years old.
(3)Every licensee shall retain the film from a mammography for at least ten years following the patient’s last visit. O.Reg. 57/92, s.11.
(4)On the transfer of a licence under section 11 of the Act, the transferor of the licence shall transfer to the transferee of the licence, in a manner that will protect the privacy of the records, the records maintained under section 10 of this Regulation, and the transferee of the licence shall retain those records in accordance with this section.
Section 12 of the Regulation is revoked and the following substituted:
12 (1)No licensee shall allow any person to have access to any information concerning a patient that is not subject to the Personal Health Information Protection Act, 2004 except in accordance with subsection (3).
(2)The reference to “information concerning a patient” in subsection (1) includes information or copies from a health record, even if anything that could identify the patient is removed.
(3)A) licensee may provide information described in subsection (1) to the following persons if anything that could identify the patient is removed from the information:
1. Any person, if the information is to be used for health administration or planning or health research or epidemiological studies and the use is in the public interest as determined by the Minister.
2. Cancer Care Ontario. O Reg. 346/04, s.2.
Books and Accounts 12.1(1)This section applies to licensees of independent health facilities that are funded under section 24 of the Act, other than independent health facilities whose funding is based solely on the Ministry of Health publication titled “Schedule of Facility Fees”.
(2)Every licensee shall keep the following records in relation to the independent health facility:
1. Current financial records showing:
(i) the amounts paid by the Minister to the licensee under section 24 of the Act.
(ii) the revenue earned by the licensee from facility fees charged by the licensee for or in respect of services or operating costs that support, assist or are a necessary adjunct to the primary insured services set out in the licensee’s licence, and
(iii) the expenditures, assets and liabilities of the facility that relate to the costs paid by the Minister under section 24 of the Act.
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 119
2. A reporting record listing each service provided in the facility that is a primary insured service set out in the licensee’s licence and each service provided in the facility that is a funded service under section 24 of the Act and showing how many of each of such services are provided.
3. An annual income and expense statement showing the income received and the expenses incurred by the licensee in connection with the services mentioned in paragraph 2.
4. An annual inventory of the assets of the facility that have an acquisition cost exceeding $3,500 and that relate to the costs paid by the Minister under section 24 of the Act.
(3)Every licensee shall ensure that the records required under section (2):
(a) are kept in the independent health facility; and
(b) are kept in a bound or loose-leaf book or are recorded by a system of mechanical or electronic data processing or any other information storage device.
(4)Every licensee shall ensure that any part of a record required under subsection (2) that relates to a period of time is retained for at least six years following the end of the period.
(5)Every licensee shall ensure that the accounts of the independent health facility are audited by a person licensed under the Public Accountancy Act. O.Reg. 283/94, s.1, part.
12.2 Every licensee of an independent health facility shall furnish such information and accounts as the Director may require. O. Reg. 283/ 94, s.1, part.
Notices 13 Every licensee of an independent health facility,
(a) who decides to cease operating the facility at a future date shall give the Director, as soon as possible, written notice of the date; and
(b) who ceases to operate the facility shall give the Director, within seven days after the date the licensee ceases to operate the facility, written notice of the date. O. Reg. 57/92, s.13.
14 Every licensee of an independent health facility shall give the Director:
(a) if the licensee is a corporation, written notice of any change in the location of the licensee’s head office within ten days after the change; and
(b) written notice of any change in the name under which the licensee carries on business within ten days after the change. O.Reg. 57/ 92, s.14.
Miscellaneous 15 It is a condition of a licence that the licensee post the first page of the licence in a conspicuous place in the independent health facility. O. Reg. 57/92, s.15.
16(1) The fee for a licence is $100.
(2) The fee for the transfer of a licence is $100.
(3) The fee for the renewal of a licence is $100. O. Reg. 57/92, s.16.
17 The administrative charge for the purposes of section 36 of the Act is $50. O. Reg. 57/92, s.17.

120 The College of Physicians and Surgeons of Ontario
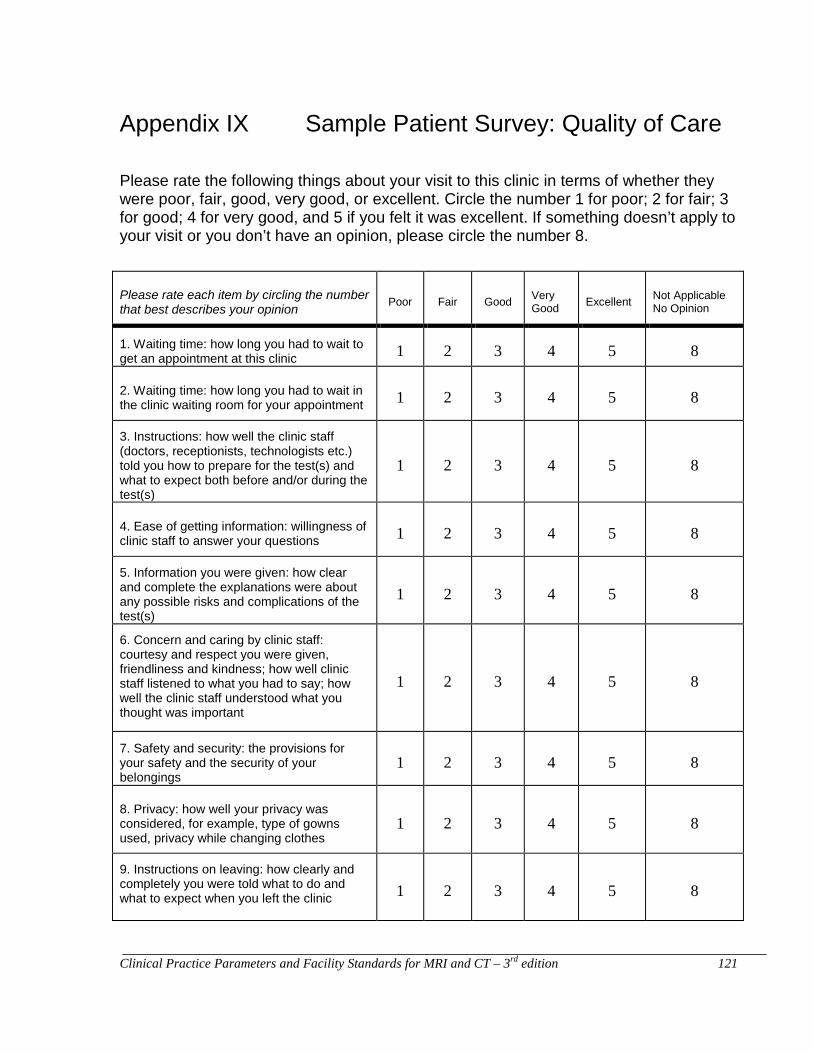
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 121
Appendix IX Sample Patient Survey: Quality of Care Please rate the following things about your visit to this clinic in terms of whether they were poor, fair, good, very good, or excellent. Circle the number 1 for poor; 2 for fair; 3 for good; 4 for very good, and 5 if you felt it was excellent. If something doesn’t apply to your visit or you don’t have an opinion, please circle the number 8.
Please rate each item by circling the number that best describes your opinion Poor Fair Good Very
Good Excellent Not Applicable No Opinion
1. Waiting time: how long you had to wait to get an appointment at this clinic 1 2 3 4 5 8
2. Waiting time: how long you had to wait in the clinic waiting room for your appointment 1 2 3 4 5 8
3. Instructions: how well the clinic staff (doctors, receptionists, technologists etc.) told you how to prepare for the test(s) and what to expect both before and/or during the test(s)
1 2 3 4 5 8
4. Ease of getting information: willingness of clinic staff to answer your questions 1 2 3 4 5 8
5. Information you were given: how clear and complete the explanations were about any possible risks and complications of the test(s)
1 2 3 4 5 8
6. Concern and caring by clinic staff: courtesy and respect you were given, friendliness and kindness; how well clinic staff listened to what you had to say; how well the clinic staff understood what you thought was important
1 2 3 4 5 8
7. Safety and security: the provisions for your safety and the security of your belongings
1 2 3 4 5 8
8. Privacy: how well your privacy was considered, for example, type of gowns used, privacy while changing clothes
1 2 3 4 5 8
9. Instructions on leaving: how clearly and completely you were told what to do and what to expect when you left the clinic 1 2 3 4 5 8
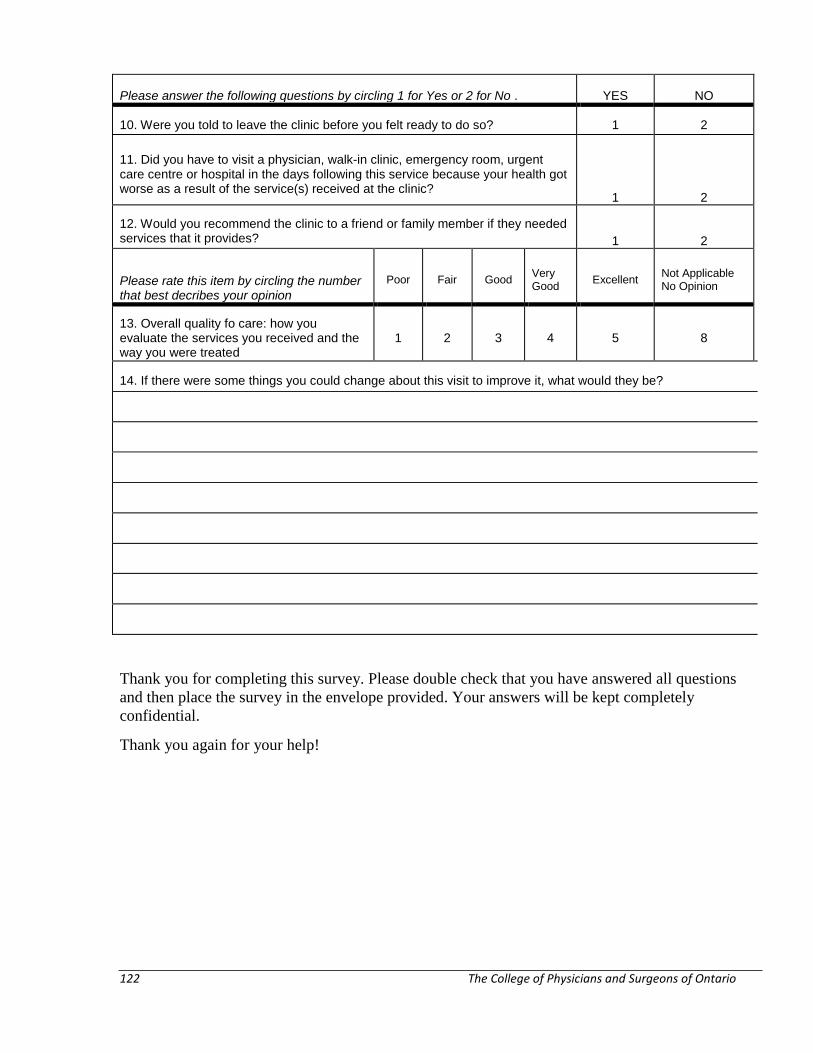
122 The College of Physicians and Surgeons of Ontario
Please answer the following questions by circling 1 for Yes or 2 for No . YES NO
10. Were you told to leave the clinic before you felt ready to do so? 1 2
11. Did you have to visit a physician, walk-in clinic, emergency room, urgent care centre or hospital in the days following this service because your health got worse as a result of the service(s) received at the clinic?
1 2
12. Would you recommend the clinic to a friend or family member if they needed services that it provides? 1 2
Please rate this item by circling the number that best decribes your opinion
Poor Fair Good Very Good Excellent Not Applicable
No Opinion
13. Overall quality fo care: how you evaluate the services you received and the way you were treated
1 2 3 4 5 8
14. If there were some things you could change about this visit to improve it, what would they be?
Thank you for completing this survey. Please double check that you have answered all questions and then place the survey in the envelope provided. Your answers will be kept completely confidential.
Thank you again for your help!
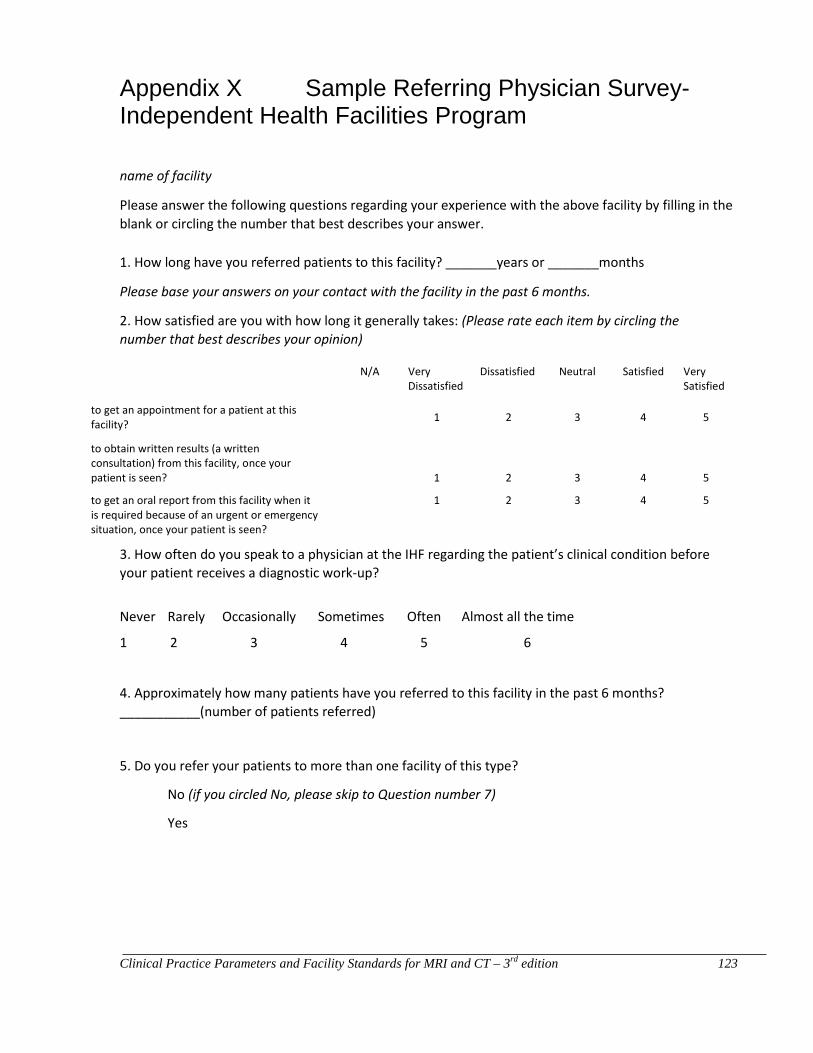
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 123
Appendix X Sample Referring Physician Survey-Independent Health Facilities Program
name of facility
Please answer the following questions regarding your experience with the above facility by filling in the blank or circling the number that best describes your answer.
1. How long have you referred patients to this facility? _______years or _______months
Please base your answers on your contact with the facility in the past 6 months.
2. How satisfied are you with how long it generally takes: (Please rate each item by circling the number that best describes your opinion)
N/A Very Dissatisfied
Dissatisfied Neutral Satisfied Very Satisfied
to get an appointment for a patient at this facility?
1 2 3 4 5
to obtain written results (a written consultation) from this facility, once your patient is seen?
1 2 3 4 5
to get an oral report from this facility when it is required because of an urgent or emergency situation, once your patient is seen?
1 2 3 4 5
3. How often do you speak to a physician at the IHF regarding the patient’s clinical condition before your patient receives a diagnostic work-up?
Never Rarely Occasionally Sometimes Often Almost all the time
1 2 3 4 5 6
4. Approximately how many patients have you referred to this facility in the past 6 months? ___________(number of patients referred)
5. Do you refer your patients to more than one facility of this type?
No (if you circled No, please skip to Question number 7)
Yes
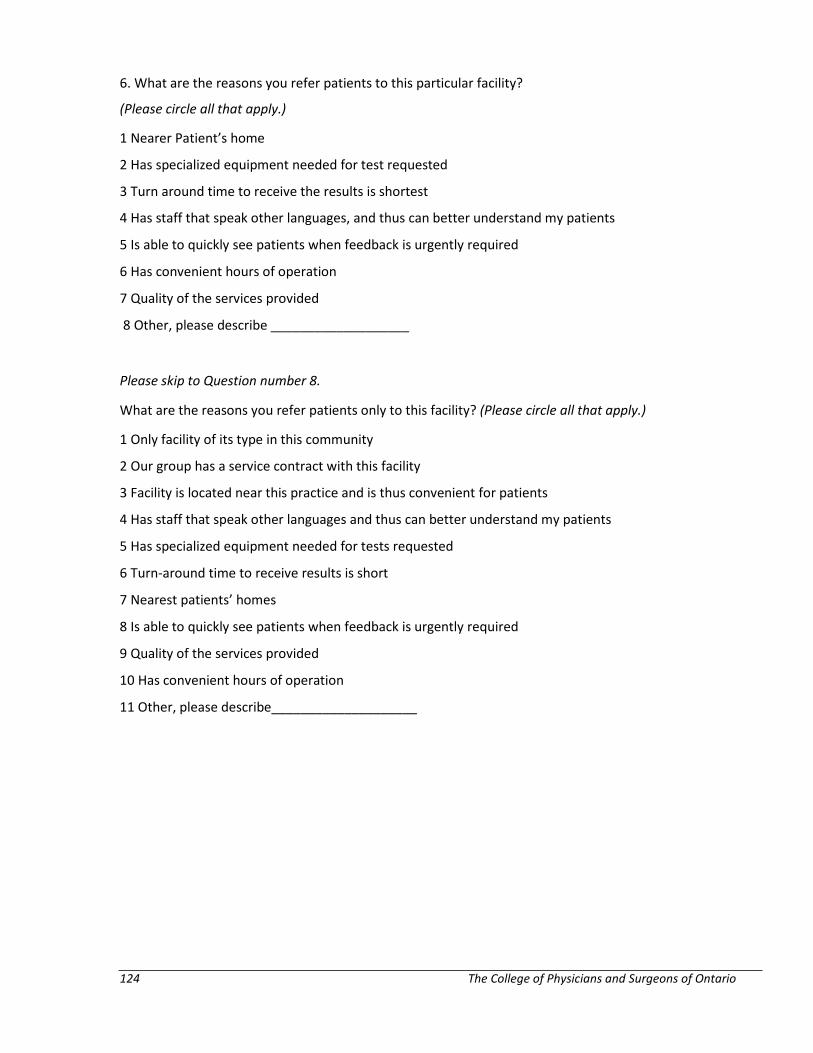
124 The College of Physicians and Surgeons of Ontario
6. What are the reasons you refer patients to this particular facility?
(Please circle all that apply.)
1 Nearer Patient’s home
2 Has specialized equipment needed for test requested
3 Turn around time to receive the results is shortest
4 Has staff that speak other languages, and thus can better understand my patients
5 Is able to quickly see patients when feedback is urgently required
6 Has convenient hours of operation
7 Quality of the services provided
8 Other, please describe ___________________
Please skip to Question number 8.
What are the reasons you refer patients only to this facility? (Please circle all that apply.)
1 Only facility of its type in this community
2 Our group has a service contract with this facility
3 Facility is located near this practice and is thus convenient for patients
4 Has staff that speak other languages and thus can better understand my patients
5 Has specialized equipment needed for tests requested
6 Turn-around time to receive results is short
7 Nearest patients’ homes
8 Is able to quickly see patients when feedback is urgently required
9 Quality of the services provided
10 Has convenient hours of operation
11 Other, please describe____________________
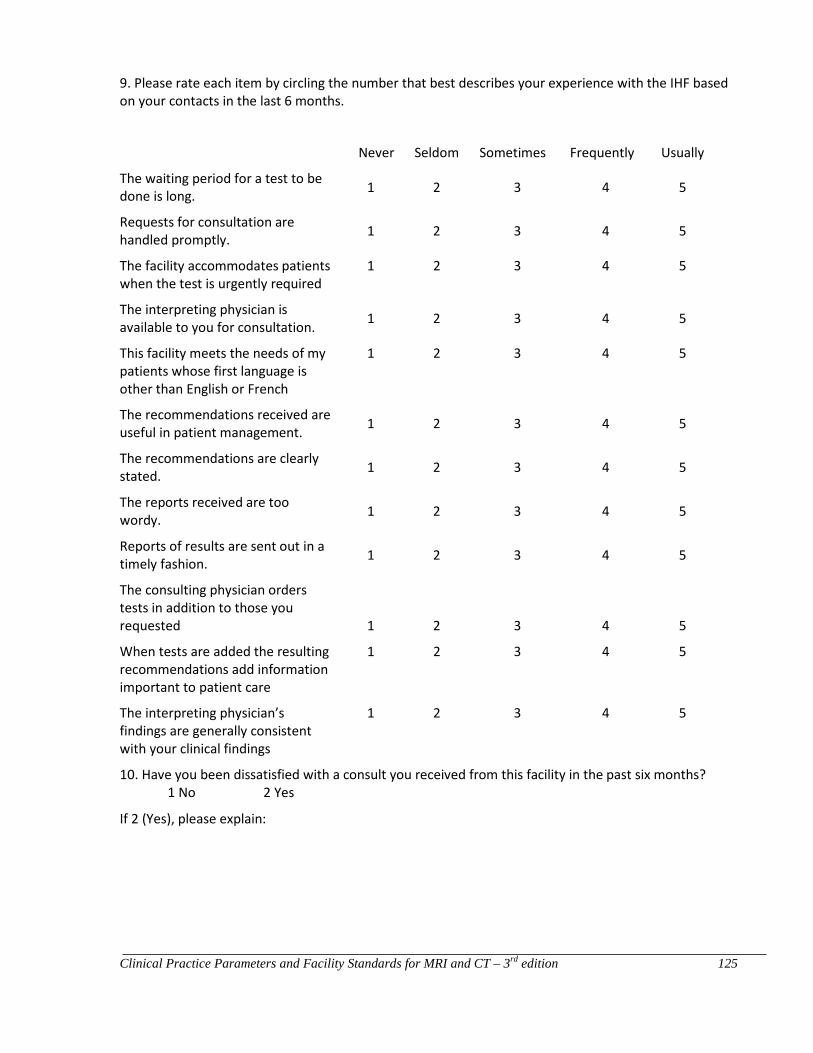
Clinical Practice Parameters and Facility Standards for MRI and CT – 3rd edition 125
9. Please rate each item by circling the number that best describes your experience with the IHF based on your contacts in the last 6 months.
Never Seldom Sometimes Frequently Usually
The waiting period for a test to be done is long. 1 2 3 4 5
Requests for consultation are handled promptly. 1 2 3 4 5
The facility accommodates patients when the test is urgently required
1 2 3 4 5
The interpreting physician is available to you for consultation. 1 2 3 4 5
This facility meets the needs of my patients whose first language is other than English or French
1 2 3 4 5
The recommendations received are useful in patient management. 1 2 3 4 5
The recommendations are clearly stated. 1 2 3 4 5
The reports received are too wordy. 1 2 3 4 5
Reports of results are sent out in a timely fashion. 1 2 3 4 5
The consulting physician orders tests in addition to those you requested 1 2 3 4 5
When tests are added the resulting recommendations add information important to patient care
1 2 3 4 5
The interpreting physician’s findings are generally consistent with your clinical findings
1 2 3 4 5
10. Have you been dissatisfied with a consult you received from this facility in the past six months? 1 No 2 Yes
If 2 (Yes), please explain:
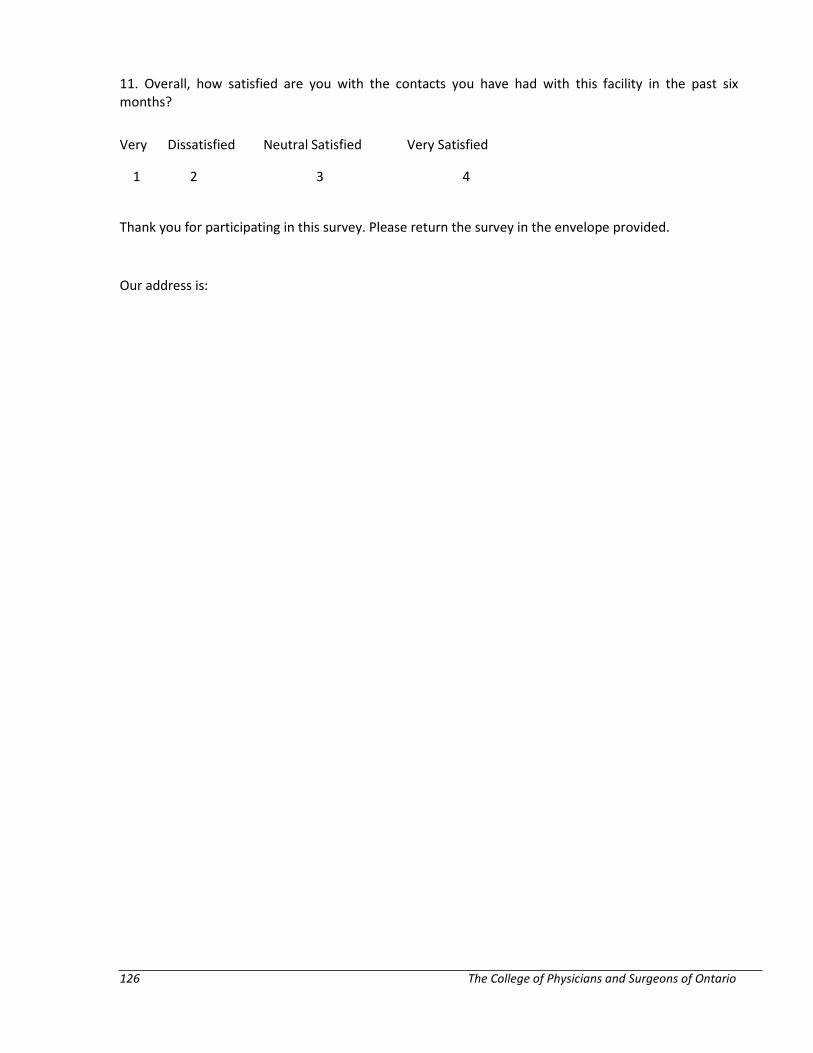
126 The College of Physicians and Surgeons of Ontario
11. Overall, how satisfied are you with the contacts you have had with this facility in the past six months?
Very Dissatisfied Neutral Satisfied Very Satisfied
1 2 3 4
Thank you for participating in this survey. Please return the survey in the envelope provided.
Our address is:





























