Embed Size (px)
Citation preview

International Journal of
Radiation Oncologybiology physics
www.redjournal.org
Clinical Investigation
Incidence of Second Malignancies in ProstateCancer Patients Treated With Low-Dose-RateBrachytherapy and Radical ProstatectomySarah Nicole Hamilton, MD,*,y Scott Tyldesley, MD, FRCPC,*,y
Jeremy Hamm, MSc,z Wei Ning Jiang, BScN,x Mira Keyes, MD, FRCPC,*,y
Tom Pickles, MD, FRCPC,*,y Vince Lapointe, BSc,jj AdamKahnamelli, BSc,y
Michael McKenzie, MD, FRCPC,*,y Stacy Miller, MD, FRCPC,{
and W. James Morris, MD, FRCPC*,y
*Department of Surgery, xFaculty of Medicine, University of British Columbia, Vancouver, BritishColumbia, Canada; Departments of yRadiation Oncology, zPopulation Oncology, and jjMedicalPhysics, British Columbia Cancer AgencyeVancouver Centre, Vancouver, British Columbia, Canada;and {Department of Radiation Oncology, British Columbia Cancer AgencyeCentre for the North,Prince George, British Columbia, Canada
Received Apr 14, 2014, and in revised form Jul 17, 2014. Accepted for publication Jul 21, 2014.
Summary
This retrospective, single-institution study did notdemonstrate a statisticallysignificant increased inci-dence of second malig-nancies in prostate cancerpatients treated with Iodine125 prostate brachytherapywhen compared with pros-tate cancer patients treatedwith radical prostatectomy.
Reprint requests to: W. James Morris, MD
Radiation Oncology, British Columbia Cancer A
Vancouver, BC, Canada V5Z 4E6. Tel: (604) 87
bccancer.bc.ca
Conflicts of interest: T.P. reports personal fe
Amgen, Abbott (now Abbvie), Ferring Pharma
Aventis, Abbott CARO Uro-Oncologic Radiatio
are all outside the submitted work. W.J.M. is
Investigator of a randomized clinical trial
ASCENDE-RT* that is sponsored, in part, by unr
Int J Radiation Oncol Biol Phys, Vol. 90, No. 4
0360-3016/$ - see front matter � 2014 Elsevie
http://dx.doi.org/10.1016/j.ijrobp.2014.07.032
Purpose: To compare the second malignancy incidence in prostate cancer patientstreated with brachytherapy (BT) relative to radical prostatectomy (RP) and to compareboth groups with the cancer incidence in the general population.Methods and Materials: From 1998 to 2010, 2418 patients were treated with Iodine125 prostate BT monotherapy at the British Columbia Cancer Agency, and 4015referred patients were treated with RP. Cancer incidence was compared with theage-matched general population using standardized incidence ratios (SIRs). Pelvic ma-lignancies included invasive and noninvasive bladder cancer and rectal cancer. Coxmultivariable analysis was performed with adjustment for covariates to determinewhether treatment (RP vs BT) was associated with second malignancy risk.Results: The median age at BTwas 66 years and at RP 62 years. The SIR comparing BTpatients with the general population was 1.06 (95% confidence interval [CI] 0.91-1.22) forsecond malignancy and was 1.53 (95% CI 1.12-2.04) for pelvic malignancy. The SIR
, FRCPC, Department of
gency, 600 West 10th Ave,
7-6000; E-mail: jmorris@
es from Astellas, Janssen,
, and grants from Sanofi-
n Award, and Oncura that
the creator and Principal
known by the acronym
estricted educational grants
from Oncura (which makes the stranded 125I sources used in the vast ma-
jority of cases reported in this article) and Sanofi -Aventis (the makers of the
luteinizing hormoneereleasing hormone product used in some of the men
reported in this article). *Morris WJ. ASCENDE-RT: Androgen suppression
combined with elective nodal and dose escalated radiation therapy. Available
at: http://clinicaltrials.gov/show/NCT00175396. Accessed January 30, 2013.
Presented in part at the Canadian Association of Radiation Oncology Annual
Meeting, St John’s, Newfoundland, Canada, August 25-28, 2014 and the
56th Annual Meeting of the American Society for Radiation Oncology, San
Francisco, CA, September 14-17, 2014.
, pp. 934e941, 2014r Inc. All rights reserved.
Volume 90 � Number 4 � 2014 Prostate BT second malignancies 935
comparingRP patients with the general populationwas 1.11 (95%CI 0.98-1.25) for secondmalignancy andwas 1.11 (95%CI 0.82-1.48) for pelvicmalignancy.Onmultivariable anal-ysis, older age (hazard ratio [HR] 1.05) and smoking (HR 1.65) were associated withincreased second malignancy risk (P<.0001). Radical prostatectomy was not associatedwith a decreased second malignancy risk relative to BT (HR 0.90, PZ.43), even whenexcluding patients who received postprostatectomy external beam radiation therapy (HR1.13,PZ.25). Older age (HR1.09,P<.0001) and smoking (HR2.17,PZ.0009)were asso-ciated with increased pelvic malignancy risk. Radical prostatectomy was not associatedwith a decreased pelvicmalignancy risk comparedwithBT (HR0.57,PZ.082), evenwhenexcluding postprostatectomy external beam radiation therapy patients (HR 0.87, PZ.56).Conclusions: After adjustment for covariates, BT patients did not have an increased sec-ondmalignancy risk comparedwith RP patients. Further follow-up of this cohort is neededgiven the potential latency of radiation-induced malignancies. � 2014 Elsevier Inc.
Introduction
The 5-year relative survival for localized prostate cancerapproaches 100%, and men are often faced with difficultywhen choosing their treatment modality (1). Depending onrisk stratification, treatment options may include activesurveillance, external beam radiation therapy (EBRT),radical prostatectomy (RP), brachytherapy (BT), orcombined-modality therapy. Given the excellent survivalfrom prostate cancer, the side effects and long-term toxicityof treatment play an important role in patients’ and clini-cians’ decision-making process.
Radiation-induced second malignancies constitute a po-tential long-term risk of EBRT and BT. Some studiescomparing prostate cancer survivors treated with EBRT rela-tive to RP have demonstrated an increased risk of pelvic sec-ondmalignancies in patients treatedwithEBRT (2-6). The riskin patients treated with BT is less well studied given therelatively recent popularity of this treatment modality. Twolarge single-institution studies have compared second pelvicmalignancy incidence in BTpatientswith those in RP patients;one did not find an increased risk, and the other found anincreased risk for men �60 years old and 1-4 years aftertreatment (7, 8). The aim of our study was to compare theincidence of second malignancies in a large cohort ofconsecutive prostate cancer patients treatedwith low-dose-rateIodine 125 (125I) prostate BT as monotherapy to prostatecancer patients treated with RP who were referred to theBritish Columbia Cancer Agency (BCCA). The second aimwas to compare both groups with the general, age-matchedmale population.
Methods and Materials
The British Columbia Cancer Agency (BCCA) researchethics board approved this study.
Study setting
This study included 2418 patients treated at the BCCAfrom January 1, 1998 to June 30, 2010 with low-dose-rate
125I prostate BT. Patients were excluded if they were treatedwith a combination of pelvic EBRT and BT (nZ154). Pa-tients with permanent residence outside British Columbiawere also excluded, because second malignancy data werenot available (nZ503). Treatment was delivered using0.424 U 125I seeds with 144 Gy prescribed as the minimumperipheral dose. Further details regarding eligibilitycriteria, follow-up, treatment, and dosimetry have beenpreviously published (9, 10). The comparator group con-sisted of all patients who were referred for prostate cancermanagement to the BCCA and treated with RP betweenJanuary 1, 1998 and June 30, 2010 (nZ4015). A total of2643 patients were treated with RP alone, and 1372 patientswere treated with RP and adjuvant/salvage post-prostatectomy EBRT. The RP and BT cohorts were bothcompared with the age-matched general male population.
A validation cohort consisted of all prostate cancer pa-tients (including nonreferred patients) who underwent RPin B.C. between January 1, 1999 and December 31, 2000(nZ1361). Cases were obtained from a previous study,with research ethics board approval (11). The RP patients inthis cohort were identified by retrospective review of thepathology records of all cases identified in the B.C. cancerregistry during this time period, which included cases notreferred to the BCCA. The purpose of using this group wasto assess whether the second malignancy risk in referred RPpatients is similar to the risk of all prostate cancer patientsin British Columbia who are treated with RP. This groupwill be referred to as the “validation RP cohort.”
Data collection
Demographic, treatment, second malignancy, and deathdata were obtained from the BCCA electronic chart. Sec-ond malignancy data were obtained from the BritishColumbia population cancer registry and linked via thepatient’s identification number to the electronic chart by thepopulation outcomes unit. In this study, second malig-nancies were counted as events if they were diagnosed afterthe date of BT or RP. Nonmelanoma skin cancers andprostate cancers were excluded. Pelvic malignancies

Hamilton et al. International Journal of Radiation Oncology � Biology � Physics936
included rectal cancer and invasive and noninvasive bladdercancer. Electronic charts were individually reviewed toobtain further second malignancy details, including patho-logic confirmation and cause of death. Smoking status wasretrospectively reviewed for all patients. Postimplant chestradiographs were reviewed for BT patients diagnosed withlung cancer to assess for a relationship to 125I seed pul-monary emboli.
Statistical analysis
The BT and RP cohorts were compared using the c2 test forcategoric variables and theMann-Whitney test for continuousvariables. Time at risk for second malignancy was calculatedfrom the date of BT or RP to the first of date of second ma-lignancy, death, or censoring (Dec 31, 2011). This censoringdate was chosen because all second cancers diagnosed beforethis date were linked to the patient’s electronic chart, and allcauses of death were completed in the registry.
Standardized incidence ratios (SIRs) with corresponding95% confidence intervals (CIs) were calculated for allsecond malignancies and for pelvic malignancies bydividing the observed number of second malignancies inBT and RP patients by the expected number. The expectednumbers were assessed by the corresponding age and timeperiod cancer incidence rates in British Columbia’s generalmale population multiplied by the person-years. Ages weregrouped into 10-year groups between 40 and 89 years forthe purpose of assessing age-specific incidence rates.
Kaplan-Meier analysis was performed to determine theactuarial second malignancy and pelvic malignancy rates inpatients treated with BT and RP. Second malignancy rates
Table 1 Characteristics of patients treated with prostate brachyther
Characteristic
Brachytherapy
Number Per
Year of treatment1998-2000 3462001-2003 5802004-2006 5282007-2010 964
Length of follow-up, y0-5 10465-10 911>10 461
Vital statisticsDead 217Alive 2201
Previous/current smokerYes 1340No 920Unknown 156
Median age at treatment, y 66Median follow-up, y 5.8Median time to second malignancy, y 4.2 (IQR 1.5-7.0
Abbreviation: IQR Z interquartile range.
were also calculated for the subgroup of patients treated withRP alone (excluding patients treated with postprostatectomyEBRT) and for the validation RP cohort (12). The time toevent was the date of prostate BT or RP to the date ofdiagnosis of second malignancy. Patients were censored onthe first of date of death or Dec 31, 2011. Kaplan-Meieranalysis was also used to determine death from secondmalignancy. The time to event was the date of prostate BT orRP to the date of death from second malignancy. Death fromsecond pelvic malignancy was defined as the date of prostateBT or RP to the date of death from pelvic malignancy. Pa-tients were censored at date of death from other causes orDec 31, 2011 for living patients, whichever came first.
Cox regression multivariable analysis was performed todetermine whether BT patients had increased risks of secondmalignancy and death from second malignancy comparedwith RP patients after adjusting for covariates. The variablesincluded age (continuous), smoking status (current/previoussmoker vs never smoker vs unknown) and treatment (RPincluding postprostatectomy EBRT patients vs BT, and RPexcluding postprostatectomy EBRT patients vs BT).
Results
Patient characteristics
The characteristics of the BT and RP cohorts are shown inTable 1. Brachytherapy patients were older; the median ageat BT was 66 years (interquartile range, 60-70 years) and atRP was 62 years (interquartile range, 57-66 years). Therewere more current/previous smokers in the BT cohort
apy (nZ2418) and radical prostatectomy (nZ4015)
Radical prostatectomy
Pcentage Number Percentage
<.000114.3 740 18.424.0 943 23.521.8 929 23.139.9 1403 34.9
<.000143.3 1516 37.837.7 1552 38.719.1 947 23.6
.829.0 367 9.191.0 3648 90.9
<.000155.5 1910 47.638.1 1590 39.36.5 515 12.8
62 <.00016.4 <.0001
) 4.7 (IQR 2.5-7.4) .088
Volume 90 � Number 4 � 2014 Prostate BT second malignancies 937
(55.5%) compared with the RP cohort (47.6%). The medianlength of follow-up after BTwas 5.8 years, and 461 patientshad follow-up >10 years. The median length of follow-upafter RP was 6.4 years, and 947 patients had follow-up>10 years. The median follow-up length was greater inRP patients because the BCCA BT program was estab-lished in 1998 and throughout the study period more pa-tients were treated with BT as this technique gainedpopularity. This led to a higher proportion of BT patientsbeing treated in more-recent years. Most (91% of BT and91% of RP) patients were alive at the time of data analysis.
Second malignancies
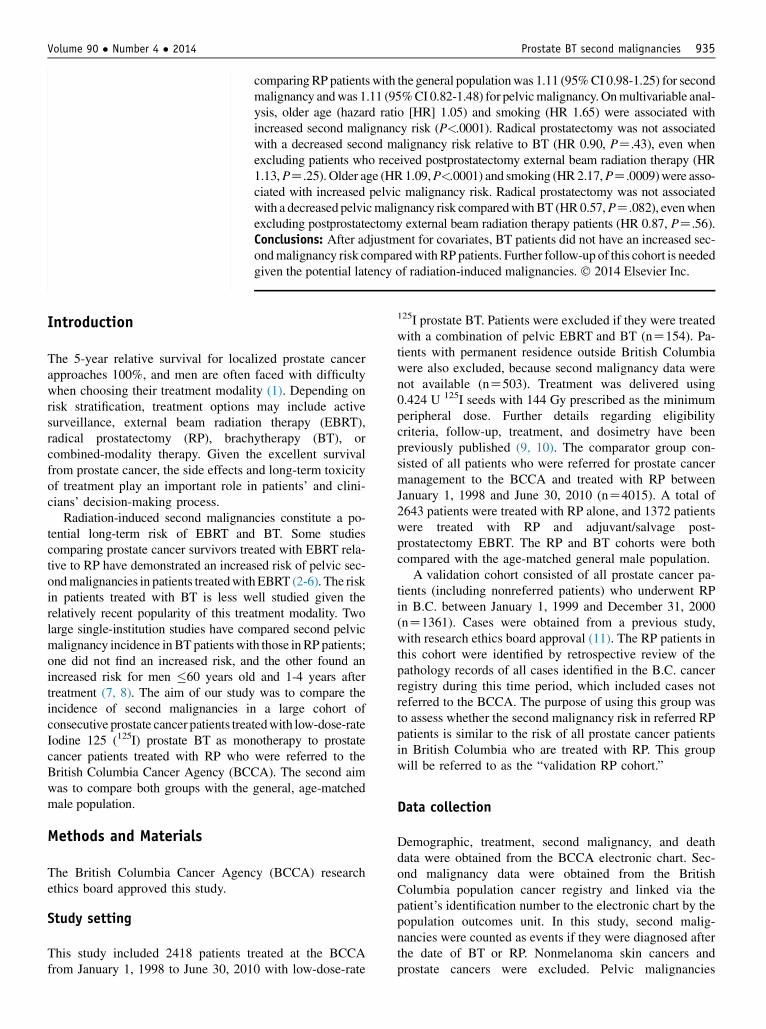
Details regarding cancer subtype, number of patients, andsecond malignancyerelated deaths are reported in Table 2.A total of 202 second malignancies (in 189 patients) wereidentified in the BT cohort and 275 second malignancies (in265 patients) in the RP cohort.
Lung cancerwas themost common secondmalignancy andoccurred in 1% of BTand 0.9% of RP patients. Of the patientsdiagnosedwith lung cancer andmesothelioma, 28 of 29 (97%)had a documented smoking history in the BT cohort and 31 of41 (76%) in the RP cohort. The majority (22 of 29) of the BT
Table 2 Second malignancy sites and death from second malignanprostatectomy (nZ4015)
Cancer site
Brachytherapy
Number Death from 2nd malignanc
Pelvic malignanciesBladder (invasive) 11 (0.5) <5Bladder (noninvasive) 21 (0.9) 0Rectum 19 (0.8) 7 (0.3)
Nonpelvic malignanciesLung 26 (1) 21 (0.8)Colon 18 (0.7) 5 (0.2)Hematologic 19 (0.8) 7 (0.3)Lymphoma 13 (0.5) 0Melanoma 15 (0.6) <5Head and neck 10 (0.4) <5Renal/ureter 5 (0.2) <5Pancreas 8 (0.3) 8 (0.3)Gastric 7 (0.3) <5Glioma 5 (0.2) 5 (0.2)Esophagus 5 (0.2) <5Primary unknown 7 (0.3) 7 (0.3)Mesothelioma <5 <5Sarcoma e extremity <5 0Hepatocellular <5 <5Neuroendocrine <5 0Small intestine d dGallbladder d dSpinal glioma <5 0Meningioma <5 0Appendix d d
Total 202/189 (7.8) 77 (3.2)
Values in parentheses are percentages.
patients who were diagnosed with lung cancer or mesotheli-oma had had a postimplant chest radiograph, which wasstandard practice at the BCCA until 2004, and none had evi-dence of radioactive 125I seed pulmonary emboli.
Of the potentially in-field malignancies (sarcoma,bladder, rectal, and anal cancer), 0.9% of BT patientsdeveloped noninvasive bladder cancer, 0.5% invasivebladder cancer, and 0.8% rectal cancer. In comparison,0.2% of RP patients developed noninvasive bladder cancer,0.6% invasive bladder cancer, and 0.3% rectal cancer. Forpatients diagnosed with bladder cancer, 24 of 32 (75%) hada smoking history in the BT cohort and 24 of 32 (75%) inthe RP cohort. Of the patients diagnosed with a secondcancer, 77 BT patients (41%) and 102 RP patients (38%)died because of the second malignancy.
The SIR comparing BT patients to the general popula-tion was 1.06 (95% CI, 0.91-1.22) for second malignancyand was 1.53 (95% CI, 1.12-2.04) for pelvic malignancy.The SIR comparing RP patients with the general populationwas 1.11 (95% CI, 0.98-1.25) for second malignancy andwas 1.11 (95% CI, 0.82-1.48) for pelvic malignancy.
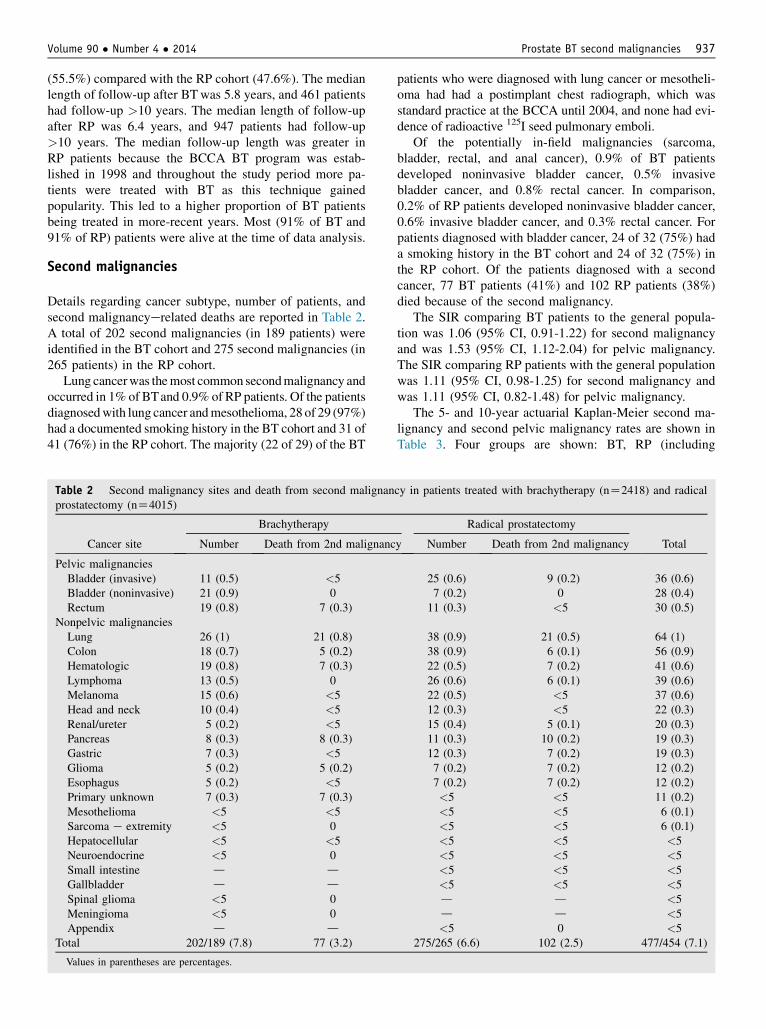
The 5- and 10-year actuarial Kaplan-Meier second ma-lignancy and second pelvic malignancy rates are shown inTable 3. Four groups are shown: BT, RP (including
cy in patients treated with brachytherapy (nZ2418) and radical
Radical prostatectomy
Totaly Number Death from 2nd malignancy
25 (0.6) 9 (0.2) 36 (0.6)7 (0.2) 0 28 (0.4)11 (0.3) <5 30 (0.5)
38 (0.9) 21 (0.5) 64 (1)38 (0.9) 6 (0.1) 56 (0.9)22 (0.5) 7 (0.2) 41 (0.6)26 (0.6) 6 (0.1) 39 (0.6)22 (0.5) <5 37 (0.6)12 (0.3) <5 22 (0.3)15 (0.4) 5 (0.1) 20 (0.3)11 (0.3) 10 (0.2) 19 (0.3)12 (0.3) 7 (0.2) 19 (0.3)7 (0.2) 7 (0.2) 12 (0.2)7 (0.2) 7 (0.2) 12 (0.2)<5 <5 11 (0.2)<5 <5 6 (0.1)<5 <5 6 (0.1)<5 <5 <5<5 <5 <5<5 <5 <5<5 <5 <5d d <5d d <5<5 0 <5
275/265 (6.6) 102 (2.5) 477/454 (7.1)
Hamilton et al. International Journal of Radiation Oncology � Biology � Physics938
postprostatectomy EBRT patients), RP alone (excludingpostprostatectomy EBRT patients), and the validation RPcohort. There were no differences in second malignancyand pelvic malignancy incidence among the cohortsbecause all 95% confidence intervals overlap.
Multivariable analysis of actuarial second malignancyincidence is shown in Table 4. Older age (HR, 1.05) andsmoking history (HR, 1.65) were associated with increasedsecondmalignancy risk (P<.0001).Radical prostatectomywasnot associated with a decreased second malignancy risk rela-tive to BT (HR, 0.90; PZ.43), even when excluding patientswho received postprostatectomy EBRT (HR, 1.13; PZ.25).
Multivariable analysis of actuarial second pelvic malig-nancy incidence is also shown inTable 4. Older age (HR, 1.09;P<.0001) and smoking (HR, 2.17; PZ.0009) were associatedwith increased pelvic malignancy risk. Radical prostatectomywas not associated with a decreased pelvic malignancy riskrelative to BT (HR, 0.57; PZ.082), even when excludingpostprostatectomy EBRT patients (HR, 0.87; PZ.56).Smoking status was unknown for more patients in the RPcohort owing to less-complete documentation in the surgicalrecords. Therefore, multivariate analysis was repeatedcensoring patients with an unknown smoking status, and thehazard ratios were similar to those shown in Table 4.
Mortality from second malignancy
The 5- and 10-year actuarial Kaplan-Meier rates of deathfrom second malignancy were 2.5% (95% CI, 2.1%-2.9%)and 4.7% (95% CI, 4.1%-5.3%) in BT patients and 1.4%(95% CI, 1.2%-1.6%) and 4.3% (95% CI, 3.8%-4.8%) inRP patients (PZ.04). However, BT patients did not have an
Table 3 Actuarial Kaplan-Meier 5- and 10-year rates of second ma
Age Year BT cohort, %RP cohort, i
EBRT,
All second malignancies40-49 5 0 4 (0-840-49 10 0 6 (0-150-59 5 3 (1-5) 3 (2-450-59 10 9 (5-14) 6 (4-860-69 5 4 (2-5) 5 (4-660-69 10 10 (8-13) 11 (9-170-79 5 8 (6-11) 7 (5-170-79 10 17 (13-21) 17 (12-
All second pelvic malignancies40-49 5 0 040-49 10 0 050-59 5 1 (0-2) 050-59 10 1 (0-2) 1 (0-260-69 5 1 (0-1) 0 (0-160-69 10 3 (2-5) 2 (1-370-79 5 2 (1-4) 3 (1-470-79 10 6 (3-9) 5 (2-8
Rates are shown with corresponding 95% confidence intervals (in parenthes
(RP) cohort (including patients treated with postprostatectomy external beam r
treated with postprostatectomy EBRT, nZ2643), and validation RP cohort (nZ
increased risk of death from second malignancy comparedwith RP patients after adjusting for age and smoking status(Table 5).
The 5- and 10-year actuarial Kaplan-Meier rates ofdeath from second pelvic malignancy were 0.2% (95% CI,0.1%-0.3%) and 0.7% (95% CI, 0.5%-0.9%) in BT patientsand 0.2% (95% CI, 0.1%-0.3%) and 0.4% (95% CI, 0.3%-0.5%) in RP patients (PZ.07). However, BT patients didnot have an increased risk of death from second pelvicmalignancy compared with RP patients after adjusting forage and smoking status (Table 5).
Discussion
This is, to our knowledge, the largest single-institutionstudy exploring the incidence of subsequent malignanciesin men with prostate cancer treated with BT and RP. Thesemen may have baseline risks of subsequent cancers due toknown and unknown genes (eg, BRCA1), increased sur-veillance (bladder cancer for a man under active care of anurologist) and lifestyle factors (smoking, obesity, andalcohol usage) (13). The estimates in this study thereforerepresent all subsequent cancers that occur after BT and arenot limited to radiation-induced cancers, because the la-tency period for radiation-induced malignancy has beenestimated at between 5 and 15 years (14).
There were no differences in the second malignancyincidence in the BT and RP cohorts compared with thecancer incidence in the general population. Although thecrude number of second malignancies was greater in BTpatients (Table 2), there were no differences in actuarialsecond malignancy rates in the BT and RP cohorts when
lignancy and second pelvic malignancy
ncluding%
RP cohort, excludingEBRT, %
Validation RPcohort, %
) 4 (0-8) 3 (0-9)1) 4 (0-8) 6 (0-14)) 3 (2-5) 4 (2-6)) 6 (4-8) 7 (4-10)) 5 (4-7) 7 (5-9)3) 11 (9-13) 12 (9-15)0) 8 (5-11) 6 (1-10)22) 16 (10-22) 9 (3-14)
0 00 00 1 (0-2)
) 1 (0-2) 2 (0-3)) 1 (0-1) 2 (1-3)) 1 (0-4) 3 (1-4)) 3 (1-5) 3 (0-6)) 4 (1-7) 3 (0-6)
es) for the brachytherapy (BT) cohort (nZ2418), radical prostatectomy
adiation therapy [EBRT], nZ4015), RP-alone cohort (excluding patients
1361).

Table 4 Cox multivariable analysis of actuarial second malignancy incidence and actuarial second pelvic malignancy incidence
Variable Hazard ratio95% Confidence
interval P
All second malignanciesAge (continuous) 1.05 1.04-1.07 <.0001Smoker vs nonsmoker 1.65 1.35-2.02 <.0001Radical prostatectomy (including postprostatectomy EBRT) vs brachytherapy 0.90 0.69-1.17 .43Radical prostatectomy (excluding postprostatectomy EBRT) vs brachytherapy 1.13 0.91-1.40 .25
Second pelvic malignanciesAge (continuous) 1.09 1.05-1.12 <.0001Smoker vs nonsmoker 2.17 1.37-3.44 .0009Radical prostatectomy (including postprostatectomy EBRT) vs brachytherapy 0.57 0.31-1.07 .082Radical prostatectomy (excluding postprostatectomy EBRT) vs brachytherapy 0.87 0.56-1.38 .56
Abbreviation as in Table 1.
Volume 90 � Number 4 � 2014 Prostate BT second malignancies 939
adjusting for age, even when excluding postprostatectomyEBRT patients from the RP cohort. In addition, the vali-dation RP cohort second malignancy rates did not differfrom those in the RP cohort. This implies that the secondmalignancy incidence in RP patients who were referred tothe BCCA was very similar to the risk in nonreferred pa-tients who undergo RP in British Columbia. The 10-yearsecond malignancy rates in the RP and BT cohorts werequite similar to the rates reported by Zelefsky et al and byHinnen et al (7, 8). Our results are also supported by aprevious study at the BCCA and a large Surveillance,Epidemiology, and End Results (SEER) study, which didnot demonstrate an overall difference in second malig-nancies in prostate cancer patients treated with EBRTcompared with patients treated without EBRT and thegeneral population (2, 3).
Table 5 Cox multivariable analysis of actuarial death fromsecond malignancy and death from second pelvic malignancy
Variable
Hazard
ratio
95%Confidence
interval P
All second malignancies
Age (continuous) 1.05 1.03-1.08 <.0001Smoker vs nonsmoker 2.06 1.48-2.88 <.0001
Radical prostatectomy(including postprostatectomy
EBRT) vs brachytherapy
0.80 0.51-1.24 .32
Radical prostatectomy
(excluding postprostatectomyEBRT) vs brachytherapy
1.40 0.91-2.15 .13
Second pelvic malignancies*
Age (continuous) 1.05 0.98-1.13 .15
Smoker vs nonsmoker 2.73 1.01-7.42 .048Radical prostatectomy
(including postprostatectomyEBRT) vs brachytherapy
0.58 0.24-1.45 .25
Abbreviation as in Table 1.
* Radical prostatectomy alone (excluding postprostatectomy EBRT
patients) versus brachytherapy could not be included in this model
owing to no events occurring in patients treated with both radical
prostatectomy and EBRT.
When comparing the incidence of second pelvic ma-lignancy in BT patients with the general population, theSIR was 1.53 (95% CI, 1.12-2.04). A potential explanationfor this observation may be lead-time bias from increasedurologic surveillance due to urinary symptoms and colo-noscopies due to rectal bleeding after BT. Some studieshave suggested that prostate cancer patients may be athigher risk for subsequent bladder cancers than the generalpopulation, even after accounting for diagnostic and treat-ment biases (15, 16). We did not detect an increased inci-dence of pelvic malignancies in the RP cohort comparedwith the general population (SIR, 1.11; 95% CI, 0.82-1.48).However, there was overlap of the SIR confidence intervalsof the BT cohort and RP cohort, which indicates that theSIRs were not statistically significantly different.
We did not detect an increased risk of second pelvicmalignancy when comparing the BT cohort with the RPcohort, even when excluding postprostatectomy EBRT pa-tients from the RP cohort. In addition, the validation RPcohort second pelvic malignancy rates did not differ fromthe RP cohort. This implies that the pelvic malignancyincidence in RP patients who were referred to the BCCAwas very similar to the risk in nonreferred patients whoundergo RP in B.C.
The 10-year likelihoods of rectal and bladder cancers inour cohort were similar to the 2% RP and 3% BT risk re-ported by Zelefsky et al and the 1.8% BT risk reported byMusunuru et al (7, 17, 18). Similarly, 2 other single-institution studies did not demonstrate an overallincreased risk of pelvic malignancies after BT comparedwith RP (8, 19). Liauw et al (20) detected an increased riskof bladder cancer after BT compared with the generalpopulation; however, all cases occurred in patients treatedwith both EBRT and BT. Studies based on SEER data havebeen conflicting. Nieder et al (21) found an increased riskof bladder cancer in patients treated with BT relative to RP,whereas Moon et al (22) and Abdel-Wahab et al (23) didnot identify a difference in bladder cancer in patientstreated with BT compared with patients treated withoutradiation therapy. On the basis of these studies and ourfindings, it is possible that a small increased risk of pelvic

Hamilton et al. International Journal of Radiation Oncology � Biology � Physics940
malignancies after BT exists that single-institution serieslack the statistical power to detect. In addition, case reportshave demonstrated unusual second malignancies in thetreatment field after BT, including penile sarcoma, rectalsquamous cell carcinoma, and prostate squamous cell car-cinoma, which implies that radiation-induced cancers afterBT occur (24-27).
An elevated risk of lung cancer has been reported inpatients receiving EBRT when compared with RP, evenwhen smoking rates are similar, which is potentially relatedto scatter radiation (3). A hypothetical source of increasedrisk of lung cancer after BT is secondary to 125I seed pul-monary emboli. None of the available postimplant chestradiographs of BT patients who developed lung cancer hadevidence of 125I seed emboli. The BT cohort in our studyhad more smokers than the RP cohort, and as expected,smoking history was associated with increased risks ofsecond malignancy and pelvic malignancy on multivariableanalysis.
The proportion of patients who died from second ma-lignancies seemed to be greater in the BT group (Table 2),especially for colorectal cancers. However, smoking andolder age are established prognostic factors for cancer-specific survival for many malignancies, including colo-rectal cancer (28-30). After adjusting these variables, BTpatients did not have an increased risk of death from secondmalignancy compared with RP patients. The risk of deathfrom second malignancy was <5% at 10 years in ouranalysis. This was similar to the 7% risk of death fromsecond malignancy previously reported (31). The risk ofdeath from pelvic malignancy was very low in both the RPand BT cohort at <1% at 10 years after therapy, which canbe put in perspective with the 0.5%-1% 30-day mortalityrisk after RP (32, 33).
The strengths of this study include the uniform patienteligibility, standardized treatment protocol used in themodern prostate-specific antigen era, and the relativelylarge sample size for a single-institution study. The BCCAdelivers all radiation therapy in British Columbia, so wewere able to accurately identify all patients receivingsalvage or adjuvant EBRT. Second malignancies werelinked via the population cancer registry, and a censoringdate of 18 months before data analysis was chosen toensure that all second malignancies were captured. Wewere able to demonstrate that referred patients treated withRP have similar second malignancy and pelvic malignancyrates as nonreferred patients based on the validation RPcohort. Although studies from SEER databases have amuch larger sample size and are able to obtain greaterstatistical power, individual chart review is not performed,and second malignancy reporting may be incomplete, inaddition, the eligibility criteria, technique, radioisotopesused, and dose are unknown and likely heterogeneous (21,22). Finally, adjuvant and salvage EBRT are not reported inSEER, and this is a potential confounding factor (21, 22).
The main limitations of this study include the smallsample size compared with SEER studies and the
relatively short follow-up length for patients. A criticalconsideration in our analysis, and in all analyses of secondmalignancies after BT, is that longer follow-up of ourcohort is required to assess the true long-term risk (14).Brenner et al (4) found that the risk of radiation-inducedsecond malignancy increased from 1 of 290 at 5 years to1 of 70 after 10 years. Huang et al (19) had similar find-ings: they found the increased risk of second malignanciesin RT patients relative to RP patients was greater after10 years. It is possible that with longer follow-up anincreased risk of second malignancies in the BT groupwill be detected. Given that prostate cancer generally af-fects older men, prolonged follow-up is often difficult toachieve. This study will serve as a baseline, and repeatanalysis of the cohort will be performed given the po-tential latency of radiation-induced malignancies. Inaddition, although we were able to ascertain smokingstatus, details regarding patient comorbidities were notavailable, and these factors (which influence malignancyrisk) could have differed between the treatment groups.
Conclusion
Our study demonstrated that after adjusting for age andsmoking history, there was no increased risk of secondmalignancies or pelvic malignancies in prostate cancerpatients undergoing BT when directly compared with pa-tients undergoing RP, even when excluding post-prostatectomy EBRT patients. Given the sample size andfollow-up, we are unable to exclude the possibility of anincreased risk of pelvic malignancies after BT. However,clinicians and patients can be reassured that the plausibleattributable increased risk in second malignancy in the10 years after BT is very small, and the second pelvicmalignancy death rate was overall very low at <1% at10 years. However, given the relatively short follow-up inthe study and the potential latency of radiation-inducedmalignancies, repeat analysis will be undertaken in 5-10 years.
References
1. Surveillance, Epidemiology and End Results. Cancer of the prostated
SEER stat fact sheets. Available at: http://seer.cancer.gov/statfacts/html/
prost.html. Accessed March 24, 2014.
2. Pickles T, Phillips N. The risk of second malignancy in men with
prostate cancer treated with or without radiation in British Columbia,
1984e2000. Radiother Oncol 2002;65:145-151.
3. Brenner D, Curtis R, Hall E, et al. Second malignancies in prostate
carcinoma patients after radiotherapy compared with surgery. Cancer
2000;88:398-406.
4. Bhojani N, Capitanio U, Suardi N, et al. The rate of secondary ma-
lignancies after radical prostatectomy versus external beam radiation
therapy for localized prostate cancer: A population-based study on
17,845 patients. Int J Radiat Oncol 2010;76:342-348.
5. Boorjian S, Cowan J, Konety B, et al. Bladder cancer incidence
and risk factors in men with prostate cancer: Results from cancer
Volume 90 � Number 4 � 2014 Prostate BT second malignancies 941
of the prostate strategic urologic research endeavor. J Urol 2007;
177:883-887.
6. Baxter N, Tepper J, Durham S, et al. Increased risk of rectal cancer
after prostate radiation: A population-based study. Gastroenterology
2005;128:818-824.
7. Zelefsky M, Pei X, Teslova T, et al. Secondary cancers after intensity-
modulated radiotherapy, brachytherapy and radical prostatectomy for
the treatment of prostate cancer: Incidence and cause-specific survival
outcomes according to the initial treatment intervention. Br J Urol
2012;110:1696-1701.
8. Hinnen K, Schaapveld M, van Vulpen M, et al. Prostate brachytherapy
and second primary cancer risk: A competitive risk analysis. J Clin
Oncol 2011;29:4510-4515.
9. Morris WJ, Keyes M, Palma D, et al. Evaluation of dosimetric pa-
rameters and disease response after 125-Iodine transperineal brachy-
therapy for low and intermediate risk prostate cancer. Int J Radiat
Oncol Biol Phys 2009;73:1432-1438.
10. Morris WJ, Keyes M, Spadinger I, et al. Population-Based 10-Year
Oncologic Outcomes After Low-Dose-Rate Brachytherapy for Low-
Risk and Intermediate-Risk Prostate Cancer. Cancer 2013;119:1537-
1546.
11. Tyldesley S, Quirt J, Morris WJ, et al. Population-based 10 year event-
free survival after radical prostatectomy for patients with prostate
cancer in British Columbia. Radiother Oncol 2012;104(Supplement
2). Abstract 145.
12. Kaplan EL, Meier P. Nonparametric estimation from incomplete ob-
servations. J Am Stat Assoc 1958;53:457-481.
13. Ford D, Easton D, Bishop D, et al. Risks of cancer in BRCA1 mu-
tation carriers. Lancet 1994;343:692-695.
14. Xu XG, Bednarz B, Paganetti H. A review of dosimetry studies on
external-beam radiation treatment with respect to second cancer in-
duction. Phys Med Biol 2008;53:R193-R241.
15. Singh A, Kinoshita Y, Rovito P, et al. Higher than expected association
of clinical prostate and bladder cancers. J Urol 2005;173:1526-1529.
16. Chun T. Coincidence of bladder and prostate cancer. J Urol 1997;157:
65-67.
17. Zelesfksy M, Housman D, Pei X, et al. Incidence of secondary cancer
development after high-dose intensity-modulated radiotherapy and
image-guided brachytherapy for the treatment of localized prostate
cancer. Int J Radiat Oncol 2012;83:953-959.
18. Musunuru H, Mason M, Murray L. Second primary cancers occurring
after I-125 brachytherapy as monotherapy for early prostate cancer.
Clin Oncol 2014;26:210-215.
19. Huang J, Kestin L, Ye H, et al. Analysis of second malignancies after
modern radiotherapy versus prostatectomy for localized prostate
cancer. Radiother Oncol 2011;98:81-86.
20. Liauw S, Sylvester J, Morris C, et al. Second malignancies after prostate
brachytherapy: Incidence of bladder and colorectal cancers in patients
with 15 years of potential follow-up. Int J Radiat Oncol 2006;66:669-673.
21. Nieder A, Porter M, Soloway M. Radiation therapy for prostate cancer
increases subsequent risk of bladder and rectal cancer: A population
based cohort study. J Urol 2008;180:2005-2009.
22. Moon K, Stukenborg G, Keim J, et al. Cancer incidence after localized
therapy for prostate cancer. Cancer 2006;107:991-998.
23. Abdel-Wahab M, Reis I, Hamilton K. Second primary cancer after
radiotherapy for prostate cancerda SEER analysis of brachytherapy
versus external beam radiotherapy. Int J Radiat Oncol 2008;72:58-68.
24. Hakky T, Espiritu P, Rodriguez A, et al. Surgical management of a
locally advanced symptomatic recurrence of penile sarcoma secondary
to prostate brachytherapy. Int Braz J Urol 2013;39:293-294.
25. Yurkdakul G, de Reijke T, Blank L, et al. Rectal squamous cell car-
cinoma 11 years after brachytherapy for carcinoma of the prostate. J
Urol 2003;169:280.
26. Miller V, Reuter V, Scher H. Primary squamous cell of the prostate
after radiation seed implantation for adenocarcinoma. Urology 1995;
46:111-113.
27. Aaltomaa S, Karja V, Kainulainen S. Secondary squamous cell pros-
tate cancer after prostate brachytherapy treatment. Scand J Urol
Nephrol 2011;45:356-358.
28. Phipps AI, Shi Q, Newcomb PA, et al. Associations between cigarette
smoking status and colon cancer prognosis among participants in
North Central Cancer Treatment Group phase III trial N0147. J Clin
Oncol 2013;31:2016-2023.
29. Lee YC, Lee YL, Chuang JP, et al. Differences in survival between
colon and rectal cancer from SEER data. PLOS One 2013;8:e78709.
30. Kobrinsky NL, Klug MG, Hokanson PJ, et al. Impact of smoking on
cancer stage at diagnosis. J Clin Oncol 2003;21:907-913.
31. Bittner N, Merrick G, Galbreath R, et al. Primary causes of death
after permanent prostate brachytherapy. Int J Radiat Oncol 2008;72:
433-440.
32. Alibhai S, Leach M, Tomlinson G, et al. Rethinking 30-day mortality
risk after radical prostatectomy. Urol 2006;68:1057-1060.
33. Lu-Yao G, Albertsen P, Warren J, et al. Effect of age and sur-
gical approach on complications and short-term mortality after
radical prostatectomyea population-based study. Adult Urol
1999;54:301-307.