Embed Size (px)
Citation preview
Volume 121
Number 1, Part 1 Intravenous nifedipinelmetoprolol in unstable angina
bon-11 labeled palmitate and oxygen-15 labeled water. In: Van der Wall EE, ed. Noninvasive imaging of cardiac metabolism. Dordrecht: Martinus Nijhoff, 1987:203-40.
27. Mudge GH, Mills RM, Taegtmeyer H, Gorlin R, Lesch M. Al- terations of myocardial amino acid metabolism in chronic is- chemic heart disease. J Clin Invest 1976;58:1185-92.
28. Theroux P, Taeymans Y, Morissette D, Bosch X, Pelletier GB, Waters DD. A randomized study comparing propranolol and diltiazem in the treatment of unstable angina. J Am Co11 Car- diol 1985;5:717-22.
29. Gottlieb SO, Weisfeldt ML, Ouyang P, et al. Effect of the ad-
dition of propranolol to therapy with nifedipine for unstable angina pectoris: a randomized, double-blind, placebo-con- trolled t&l. Circulation 1986;73:331-7.
30. Kern MJ, Ganz P, Horowitz JD, et al. Potentiation of coronary vasoconstriction by beta-adrenergic blockade in patients with coronary artery disease. Circulation 1983;67:1178-85.
31. Elkavam U. Roth A. Weber L. Kulik D. Kawanishi D, McKav C, Rahimtobla SH. Effects of nifedipine’on hemodynamics anb cardiac function in patients with normal left ventricular ejec- tion fraction already treated with propranolol. Am J Cardiol 1986;58:536-40.
Incidence and clinical significance of ST segment elevation after electrical cardioversion of atrial fibrillation and atrial flutter
To study the incidence and clinical significance of postshock ST segment elevations, we recorded 12-lead ECGs immediately after transthoracic direct-current eiectricai cardioversion in 146 patients with atriai fibrillation or flutter. Among 23 patients (lg%), acute ST segment elevations amounted to 1.4 * 0.8 mV (mean * SD) and occurred after 243 +- 114 joules (cumulative dose) in the precordiai leads only in 14, concomitantly in precordiai and inferior leads in two, and in the precordiai and anteroiaterai leads in seven. They normalized within 1.5 t- 0.8 minutes. Occurrence of ST segment elevation was related to previous pericardiotomy (p < 0.00001) and age (p = 0.01). Estimation of myocardiai enzyme release did not show evidence of myocardiai damage. Patients with ST segment elevations had a lower conversion rate (48% versus 76%, p = 0.005). Long-term maintenance of sinus rhythm was also diminished (35% versus 5g%, p = 0.03). Results of this study show that postcardioversion ST segment elevation occurs predominantly in postpericardiotomy patients and may be associated with an unfavorable arrhythmia prognosis. (AM HEART J 1991;121:51.)
Isabelle C. Van Gelder, MD, Harry J. Crijns, MD, Arnoud Van Der Laarse, PhD, Wiek H. Van Gilst, PhD, and Kong I. Lie, MD. Groningen and Leiden, The Netherlands
Transient ST segment elevation after direct-current (DC) electrical cardioversion has not been studied systematically before.lM3 Irrespective of the underly- ing mechanism, it can be hypothesized that if this
From the Departments of Cardiology and Clinical Pharmacology, Thorax- center, University Hospital Groningen, and the Department of Cardiology, University of Leiden. Received for publication March 12, 1990; accepted July 11, 1990. Reprint requests: Harry J. Crijns, MD, Department of Cardiology, Thorax- center, University Hospital Groningen, Oostersingel59,9713 EZ Groningen, The Netherlands. 4/l/25117
phenomenon indicates local myocardial or epicardial damage, it might cause transient postcardioversion electrical instability, thereby preventing successful cardioversion. To study prospectively the incidence and clinical significance of postshock ST segment el- evation, we obtained continuous 12-lead ECG re- cordings immediately after cardioversion for chronic atria1 fibrillation or atria1 flutter. ECG findings were studied in relation to patient characteristics, cardio- version outcome, and estimates of myocardial creat- ine kinase (CK) and creatine kinase MB isoenzyme (CK-MB) release.

January 1991 52 Van Gelder et al. American Heart Journal
METHODS Patient population. Between April 1988 and June 1989,
a total of 121 consecutive patients with chronic atria1 fibrillation and 25 patients with atria1 flutter underwent DC electrical cardioversion to restore sinus rhythm. Im- mediately after every attempted cardioversion a continu- ous 12-lead ECG recording (MAC-12, Marquette Electron- ics Inc., Milwaukee, Wis.) was obtained.
DC electrical cardioversion. Our protocol for DC elec- trical cardioversion has been described previously.4 Pa- tients who had previously had heart surgery did not undergo cardioversion until 3 months after the operation. We used a calibrated Hewlett-Packard 78620-A defibril- lator (Hewlett-Packard Co, Andover, Mass.) with hand- held paddle electrodes (11.4 x 11.4 cm) in combination with Littmann defibrillation pads (3M Medical-Surgical Division, St. Paul, Minn.). One paddle electrode was placed right parasternally, the anterior position, and the other was placed in the lateral position in the midaxillary line. According to the protocol we started with 50 joules of stored energy in patients with atria1 fibrillation. Only in patients with atria1 flutter was this step in the protocol preceded by a shock of 30 joules. The energy of subsequent shocks was doubled. The procedure was ended after resto- ration of sinus rhythm or two attempts of 360 joules. Time between subsequent shocks was 1 to 1.5 minutes. Digitalis was discontinued at least 5 days before cardioversion. Ex- cept for amiodarone, no other antiarrhythmic drugs were used at the time of the shock. Echocardiography was per- formed on the day of the electrical cardioversion. Right and left atria1 dimensions and left ventricular dimensions were determined according to the method of Feigenbaum.5
Evaluation of parameters. ST segment elevation was considered significant only if displacement of the ST seg- ment was present in at least two related leads and amounted to 0.5 mV or more above the baseline. The maximum value of ST segment elevation was noted. Also the minimum en- ergy dose at which it occurred was noted. In a subgroup of 26 patients, serum CK and CK-MB activities were moni- tored before, directly after, and at l-hour intervals during 6 hours after the shocks. Finally enzymes were assessed 24 hours after the cardioversion.
Follow-up. After DC electrical cardioversion, patients were monitored for 24 hours in the coronary care unit. Early in-hospital recurrence of arrhythmia was noted, and if necessary antiarrhythmic drugs were instituted prophy- lactically. After discharge from the hospital, patients were evaluated in the outpatient department 1,3, and 6 months after the cardioversion and every 6 months thereafter. An ECG was obtained at each visit, In case of recurrence of atria1 fibrillation or flutter, 24-hour Holter monitoring was performed to document the continuous presence of ar- rhythmia.
Statistical analysis. Univariate analysis of categorical variables was done with two-by-two tables. Continuous variables were analyzed by means of Student’s t test for
independent samples. The Wilcoxon test was used for nonparametric distributed variables.
RESULTS ST segment elevation. In 23 patients (19 % ) ST seg-
ment elevations were found directly after a cumula- tive mean of 243 -t 114 joules (mean +- SD) using 3 it_ 1 shocks. This acute ST segment elevation (1.4 & 0.8 mV) returned to the precardioversion ST segment configuration within 1.5 f 0.8 minutes (range 10 seconds to 3 minutes). The shape of the ST segment mimicked acute transmural ischemia in only four patients (Fig. 1). In the other 19 patients with ST segment elevation, the intrinsicoid deflection of the QRS complex remained present and the ST segments were concave as in acute pericarditis (Fig. 2). ST seg- ment elevations occurred in the anterior chest wall leads in 14 patients, concomitantly in the anterior and lateral leads (I and aVL) in seven, and in both the anterior and inferior leads (II, III, and aVF) in only two patients.
Table I compares patients with and without ST segment elevation. Univariate analysis showed pre- vious pericardiotomy to be the most important pa- rameter (p = 0.00001) related to postcardioversion ST segment elevation. In addition, patients with ST segment elevation were significantly older (mean age 65 versus 60 years, (p = 0.01). There were no differ- ences between groups concerning the incidence of coronary artery disease or the use of drugs affecting ischemic or vasospastic responses. Patients without ST segment elevation received a mean total energy dose of 518 -t 32 joules. This was significantly higher than the dose that induced ST segment elevation in the other group (243 r+_ 114 joules, p = 0.006).
Myocardial enzymes. In 26 randomly selected pa- tients myocardial enzymes were monitored. ST seg- ment elevations were seen in six patients. Baseline CK activities were 39 ? 24 U/L (normal < 60 U/L), and baseline CK-MB levels were all normal (< 10 Ul L). The highest CK and CK-MB levels were found 24 hours after cardioversion and amounted to 715 -t 823 and 23 t- 10 U/L, respectively, in patients with ST segment elevation and to 637 -+_ 857 and 21 t- 17 Ul L, respectively, in those without ST displacement (p = 0.81 and p = 0.83, respectively). The CK activ- ities measured at 24 hours were significantly related to the cumulative energy dose. The CK-MB levels of the patients with and without ST segment elevation differed significantly from the CK-MB levels 24 hours after onset of symptoms in a control group of patients with acute myocardial infarction (63.6 f 38
Volume 121
Number 1, Part 1 ST elevation after conversion of atria1 fibrillation 53
-_ - “‘30X’ -’
‘- _\, -. ._.^ __--- 60s
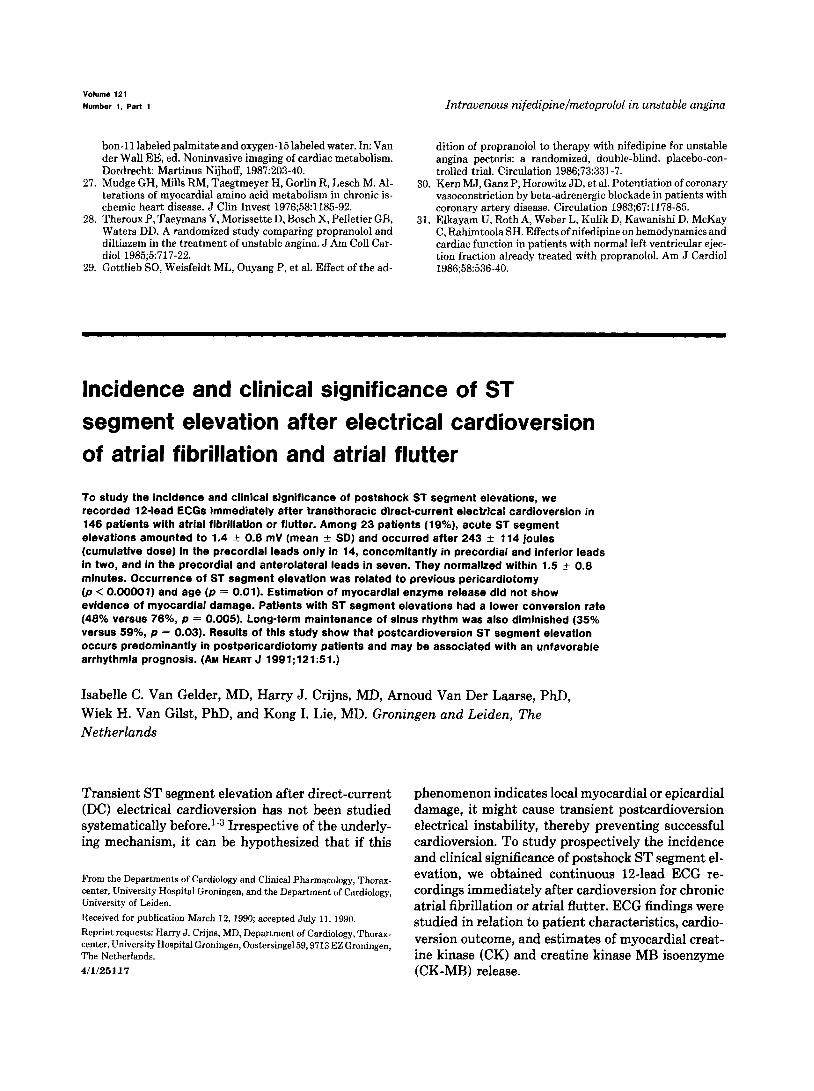
Fig. 1. ECGs during DC electrical cardioversion for atria1 fibrillation in patient who underwent aortic valve replacement 4 years previously. A, Before cardioversion. 6, After two shocks (cumulative dosage of 150 joules) sinus rhythm was restored. Note ST segment elevations in leads V4, Vs, and Vs immediately after second shock. C, D, E, and F, Time course of ST segment changes to baseline within 2 minutes. Paper speed, 25 mm/set; calibration, 10 mm/mV; J, joules; s, seconds.
U/L, p = 0.02 and p = 0.0001, respectively). The CK differed significantly from the CK-MB/CK fractions level of this control group amounted to 799 k 452 U/ 24 hours after onset of symptoms in a control group L, which was not significantly different from both of patients with acute myocardial infarction (Fig. 3). other groups (p = 0.70 and p = 0.18, respectively). Immediate and long-term follow-up. The conversion The CK-MB/CK fractions measured at 24 hours af- rate was significantly lower in the patients with ST ter cardioversion did not differ in patients with and segment elevations (48% versus 76%) p = 0.0053). without ST segment elevation. However, these values Consequently the total dose of energy was higher in
54 Van Gelder et al. January 1991
American Heart Journal
350 J
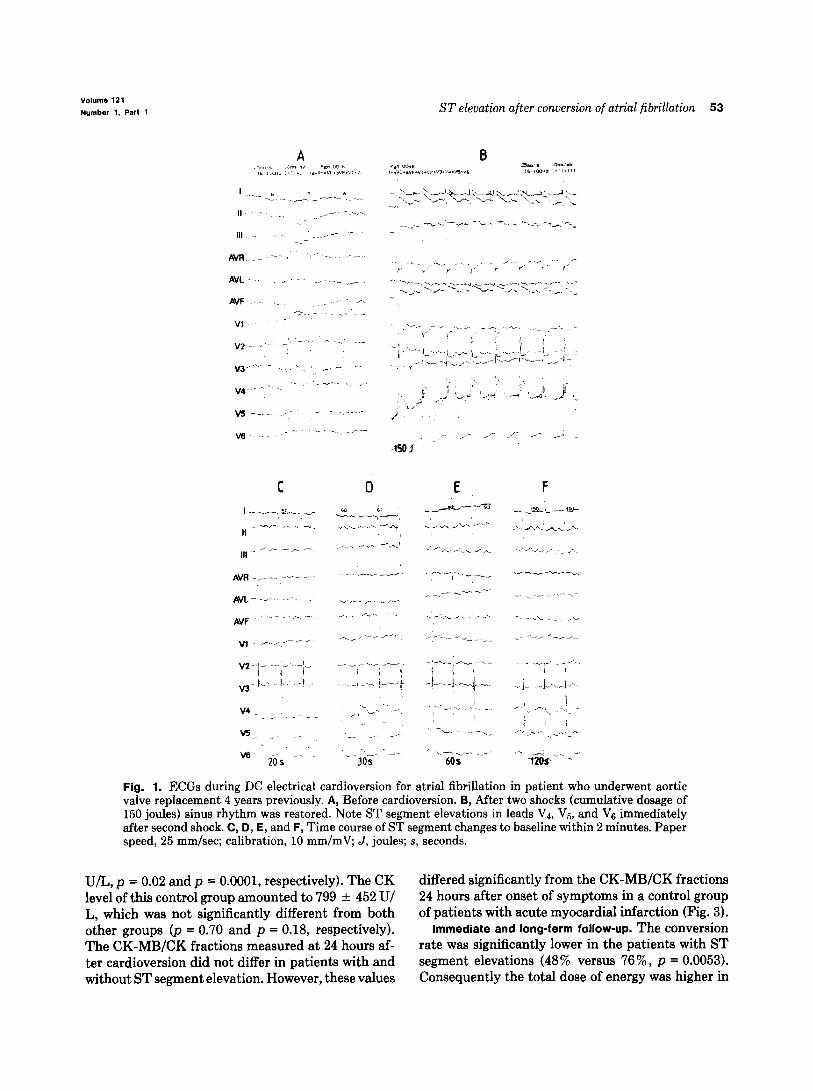
Fig. 2. ECGs during DC electrical cardioversion in patient who underwent mitral and aortic valve replacement 3 years previously. A, Before cardioversion. 6, ST segment elevations occurring after two shocks (cumulative dosage 150 joules). C, ST segment elevations after third shock (cumulative dosage of 350 joules). D and E, Time course of ST segment changes to baseline within 60 seconds. Paper speed, 25 mm/set; calibration, 10 mm/mV; J, joules; s, seconds.
this group (844 -t 69 versus 518 & 32 joules, p = 0.0004). Th e percentage of patients treated pro- phylactically with antiarrhythmic drugs after cardio- version was comparable in both groups (55% versus 66%) p = 0.46). During long-term follow-up signifi- cantly more patients with postshock ST segment el- evations had a documented recurrence of arrhythmia (65% versus 41%, p = 0.03).
DISCUSSION Incidence and clinical significance of postshock ST
segment elevation. Postcardioversion ST segment el- evation has been reported on an occasional basis only. Review of the literature showed a total of six well- documented cases.le3 Results of the present study show that this phenomenon may occur in almost 20% of patients undergoing DC electrical cardioversion
Volume 121 Number 1. Part 1 ST elevation after conversion of atria1 fibrillation 55
CK (U/L)
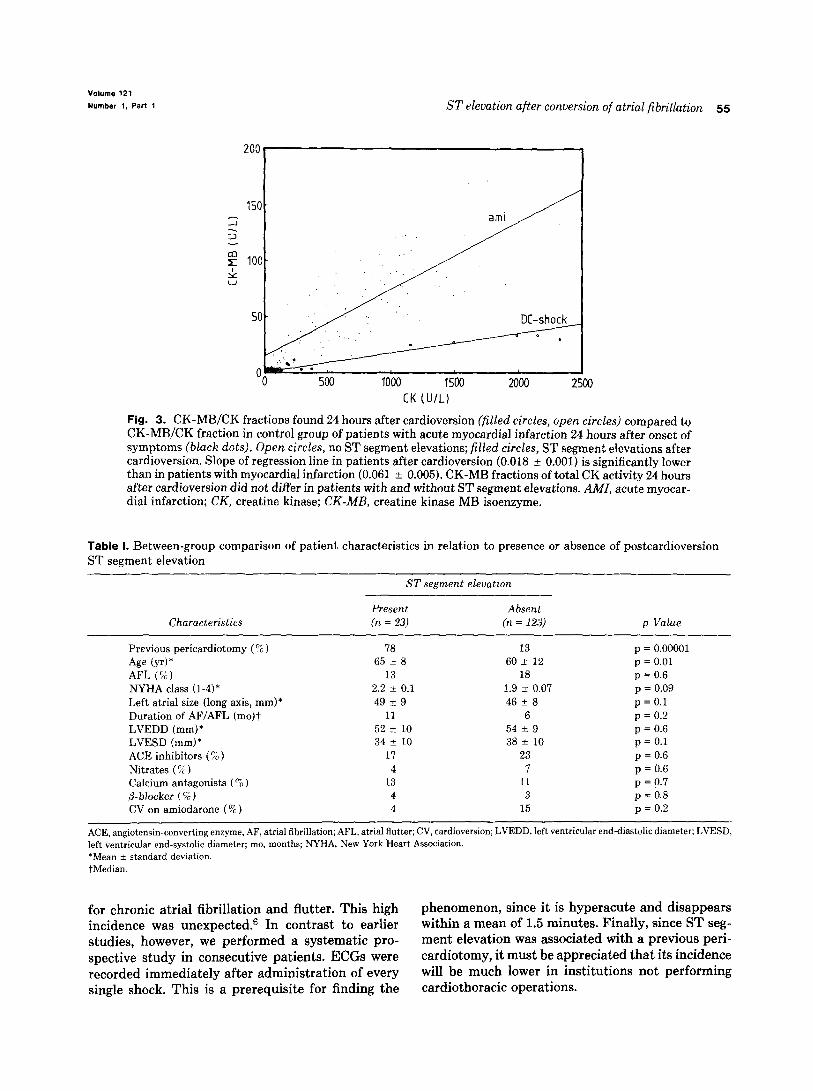
Fig. 3. CK-MB/CK fractions found 24 hours after cardioversion (filled circles, open circles) compared to CK-MBJCK fraction in control group of patients with acute myocardial infarction 24 hours after onset of symptoms (black dots). Open circles, no ST segment elevations; filled circles, ST segment elevations after cardioversion. Slope of regression line in patients after cardioversion (0.018 ? 0.001) is significantly lower than in patients with myocardial infarction (0.061 -t 0.005). CK-MB fractions of total CK activity 24 hours after cardioversion did not differ in patients with and without ST segment elevations. AMI, acute myocar- dial infarction; CK, creatine kinase; CK-MB, creatine kinase MB isoenzyme.
Table I. Between-group comparison of patient characteristics in relation to presence or absence of postcardioversion ST segment elevation
ST segment elevation
Characteristics Present Absent (n = 23) (n = 123) p Value
Previous pericardiotomy (‘Z) 78 13 p = 0.00001 Age (yr)* 65 i 8 60 +- 12 p = 0.01 AFL (r,) 13 18 p = 0.6 NYHA class (l-4)* 2.2 t 0.1 1.9 +- 0.07 p = 0.09 Left atria1 size (long axis, mm)* 49 * 9 46 t 8 p=O.l
Duration of AF/AFL (mo)t 11 6 p = 0.2 LVEDD (mm)* 52 + 10 54 * 9 p = 0.6 LVESD (mm)* 34 + 10 38 f 10 p = 0.1
ACE inhibitors (7;) ) 17 23 p = 0.6 Nitrates (%) 4 7 p = 0.6 Calcium antagonists (% ) 13 11 p = 0.7 P-blocker (‘“a) 4 3 p = 0.8
CV on amiodarone (% ) 4 15 p = 0.2
ACE, angiotensin-converting enzyme, AF, atria1 fibrillation; AFL, atria1 flutter; CV, cardioversion; LVEDD, left ventricular end-diastolic diameter; LVESD. left ventricular end-systolic diameter; mo, months; NYHA, New York Heart Association. *Mean + standard deviation. tMedian.
for chronic atria1 fibrillation and flutter. This high phenomenon, since it is hyperacute and disappears incidence was unexpected.6 In contrast to earlier within a mean of 1.5 minutes. Finally, since ST seg- studies, however, we performed a systematic pro- ment elevation was associated with a previous peri- spective study in consecutive patients. ECGs were cardiotomy, it must be appreciated that its incidence recorded immediately after administration of every will be much lower in institutions not performing single shock. This is a prerequisite for finding the cardiothoracic operations.

56 Van Gelder et al.
The clinical significance of postcardioversion ST segment elevation lies in the fact that it is associated with a poorer immediate and long-term arrhythmia outcome, This finding has not been reported before and is difficult to explain. Concerning the lower car- dioversion rates in these patients, it might be specu- lated that despite the absence of myocardial enzyme increases, shock-induced atria1 injury may have oc- curred, giving rise to spontaneous arrhythmias in- stantaneously after the shock. These instantaneous arrhythmias might reinduce atria1 fibrillation or flutter, thereby preventing successful cardioversion. Whether this also plays a role in the genesis of out- of-hospital recurrences is questionable. However, ir- respective of the mechanism causing intractability of the arrhythmia, it may be worthwhile to consider prophylactic antiarrhythmic drug therapy in pa- tients undergoing successful cardioversion with tran- sient ST segment elevations after the cardioversion.
Possible underlying mechanism for postcardioversion ST segment elevation. Chun et a1.l excluded myocar- dial damage as a cause for ST segment elevation af- ter cardioversion but could not offer an alternative explanation. Also other clinical studies could not demonstrate myocardial damage by means of differ- ent detection techniques. 2, 3, 7-g It has been suggested that a sustained depolarization of a critical mass of myocardial cells might be the cause, but definite proof is lacking.’ Variant angina seems an unlikely mechanism, since it does not account for the hyper- acute onset of ST segment elevation. In general it takes at least 1 minute for ST segment elevation to occur after the onset of coronary spasm.
The present study shows that a previous pericar- diotomy was the most important parameter related to ST segment elevation. After pericardiotomy ad- hesions develop between the subepicardium, the epi- cardium, the pericardium, and extrapericardial struc- tures. This connection may lead to shock-induced traction on subepicardial and epicardial structures during cardioversion. At this point it is important to note that ST segment elevation can occur only if electrically active cells are involved in the process.iO Combining these facts it seems justified to assume that the pericardial-to-subepicardial region plays an important role in the genesis of postcardioversion ST segment elevation. Whether this also signifies actual shock-induced injury or even cell death in the epi- cardial-subepicardial region cannot be inferred from
January 1991 American Heart Journal
the present study, but it is supported by experimen- tal findings of Doherty et al.]’ These investigators showed that shock-induced damage may indeed oc- cur and that the subepicardial layers are the most vulnerable.
Limitations of the present study. We could not dem- onstrate the presence of myocardial damage by means of estimations of CK and CK-MB release. However, this method may be too insensitive to de- tect local damage. l2 In addition, the time course of blood sampling used may have precluded detection of an acute increase in the postshock release of CK-MB in patients with a normal myocardial washout. My- ocardial scintigraphy may also be too insensitive to detect small localized areas of necrosis, and damage may occur in the absence of significant isotope accumulation.”
REFERENCES
Chun PKC, Davia JE, Donohue DJ. ST-segment elevation with elective DC cardioversion. Circulation i981;63:220-4. Zelinger AB, Falk RH. Hood WB. Electrical-induced sus- tained myocardial depolarization as a possible cause for tran- sient ST elevation post-DC elective cardioversion. AM HEART J 1982;103:1073-4. Ovsyshcher IA, Ilia R, Wanderman KL. Conduction distur- bance and ST-elevation following cardioversion. Isr J Med Sci 1984;20:736-8. Van Gelder IC, Crijns HJGM, Van Gilst WH, De Langen CDJ, Van Wijk LM, Lie KI. Effects of flecainide on the atria1 defibrillation threshold. Am J Cardiol 1989;63:112-4.
5. Feigenbaum H. Echocardiographic evaluation of cardiac cham- bers. In: Feinenbaum H. ed. Echocardiomauhv. 4th ed. Phil- adelphia: Lea & Febiger, Publishers, 19%27-87.
6. Lepeschkin E, Jones JL, Rush S, Jones RE. Analysis of cardiac damage following elective cardiac defibrillation, Cardiac De- fibrillation Conference. Lafavette. Ind.: Purdue Universitv, October 1975:85-90. ”
‘7. Reiffel JA, Gambino SR, McCarthy DM, Leahey Jr EB. Direct current cardioversion. Effect on creatine kinase, lactic dehy- drogenase and myocardial enzymes. JAMA 1978;239:122-4.
8. Konttinen A, Hupli V, Louhija A, Hartel G. Origin of elevated serum enzyme activities after direct-current countershock. N Engl J Med 1969;281:231-4.
9. Metcalfe MJ, Smith F, Jennings K. Does cardioversion of atria1 fibrillation result in myocardial damage? Br Med J 1988;296:1364-5.
10. Samson WE, Scher AM. Mechanism of ST-segment alteration during acute myocardial injury. Circ Res 1960;8:780-7.
11. Doherty PW, McLaughlin PR, Billingham M, Kernoff R, Goris ML, Harrison DC. Cardiac damage produced by direct current counter shock applied to the heart. Am J Cardiol1979;43:225- 32.
12. Tacker Jr WA, Van Vleet JF, Geddes LA. Electrocardio- graphic and serum enzymic alterations associated with cardiac alterations induced in dogs by single transthoracic damped si- nusoidal defibrillator shocks of various strengths. AM HEART J 1979:98:185-93.