Embed Size (px)
Citation preview

This article was downloaded by: [University of Cambridge]On: 08 October 2014, At: 17:46Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Global Public Health: An InternationalJournal for Research, Policy andPracticePublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/rgph20
Improving the management ofHypertension in Kazakhstan:implications for improving clinicalpractice, patient behaviours and healthoutcomesA. Nugmanova a , G. Pillai b , D. Nugmanova c & D. Kuter da ZdravPlus Project , Abt Associates Inc. , Almaty, Kazakhstanb ZdravPlus Project , John Snow Inc. , Boston, MA, USAc Kazakhstan Association of Family Physicians and FamilyMedicine, Department of Almaty Postgraduate Institute forPhysicians , Almaty, Kazakhstand ZdravPlus Project , Abt Associates Inc. , Madison, WI, USAPublished online: 03 Apr 2008.
To cite this article: A. Nugmanova , G. Pillai , D. Nugmanova & D. Kuter (2008) Improving themanagement of Hypertension in Kazakhstan: implications for improving clinical practice, patientbehaviours and health outcomes, Global Public Health: An International Journal for Research,Policy and Practice, 3:2, 214-231, DOI: 10.1080/17441690701872664
To link to this article: http://dx.doi.org/10.1080/17441690701872664
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever
or howsoever caused arising directly or indirectly in connection with, in relation to orarising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
17:
46 0
8 O
ctob
er 2
014
Improving the management of Hypertension inKazakhstan: implications for improving clinicalpractice, patient behaviours and health outcomes
A. NUGMANOVA1, G. PILLAI2, D. NUGMANOVA,3 & D. KUTER4
1ZdravPlus Project, Abt Associates Inc., Almaty, Kazakhstan, 2ZdravPlus Project, John
Snow Inc., Boston, MA, USA, 3Kazakhstan Association of Family Physicians and Family
Medicine, Department of Almaty Postgraduate Institute for Physicians, Almaty,
Kazakhstan, and 4ZdravPlus Project, Abt Associates Inc., Madison, WI, USA
AbstractThis paper presents findings from the assessment of a strategy aimed at improving case-finding and management of hypertension patients. Study findings suggest that providers’orientation to clinical guidelines, public information on hypertension risks, promotion ofyearly blood pressure screening, and universal access to an outpatient drug benefitpackage, improve case-finding and management. In addition, training of providers at pilotsites resulted in a substantial and significant difference in patient care and healthoutcomes. Provider training and tools, especially focused on effective patient counselling,made a significant contribution to increased case-finding, patient adherence to prescribeddrugs, reducing salt, and increasing regular exercise. However, further refinements arerequired to achieve the expected adherence of patients to medication and lifestyle advice.In the pilot area, we compared two samples of patients before and after the initiation ofthe intervention. We found an increase in the proportion of patients with blood pressureB140/90 mmHg, and a significant decrease in the proportion of patients with bloodpressure ]160/100 mmHg. The strategy involved the joint efforts of the ResearchInstitute of Cardiology and Internal Diseases, Karaganda Drug Information Centre,Karaganda Oblast Health Department, Kazakhstan Association of Family Physicians,Almaty Postgraduate Institute for Physicians, and USAID ZdravPlus Project in CentralAsia.
Keywords: Hypertension, cardiovascular disease, quality improvement, clinical practiceguideline, Kazakhstan, Central Asia
Correspondence: Azhar Nugmanova, ZdravPlus Project, 39 Begalina Street, Almaty 050010,Kazakhstan. E-mail: [email protected]
Global Public Health, April 2008; 3(2): 214�231
ISSN 1744-1692 print/ISSN 1744-1706 online # 2008 Taylor & Francis
DOI: 10.1080/17441690701872664
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
17:
46 0
8 O
ctob
er 2
014

Introduction and background
Cardiovascular disease (CVD) is responsible for nearly 30% of all deaths
worldwide (Gaziano et al. 2006). Hypertension is the most common CVD, and
its complications (stroke, heart attack, ischemic heart disease, renal dysfunction,
and heart failure) result in death and disability (Kearney et al. 2005). Case-
finding presents a challenge, since patients can live with the condition,
unnoticed and worsening, until a debilitating event occurs. Early diagnosis
and appropriate case management through medication and lifestyle counselling
have been shown to be effective (Lewington et al. 2002, Whelton et al. 2002).
In Kazakhstan, the burden of disease from CVD and hypertension is significant,
and the need to improve the identification and care of patients with
hypertension is paramount. The Research Institute of Cardiology and Internal
Diseases, Karaganda Drug Information Centre, Karaganda Oblast Health
Department, Kazakhstan Association of Family Physicians, Almaty Postgradu-
ate Institute for Physicians, and USAID ZdravPlus Project in Central Asia
combined efforts to develop, test, and scale up a strategy to improve case-
finding, care, and treatment of patients with hypertension. As in other former
Soviet Union countries, in Kazakhstan hypertension was regarded as an
intermittent condition to be treated with rapidly acting medication, often
injected to quickly lower blood pressure and calm the patient, then stopped
until the next hypertensive ‘crisis’. Patients think the purpose of treatment is for
relief of current symptoms, rather than a long-term and continuous treatment to
maintain lower blood pressure.
For practicing physicians clinical practice guidelines, based on randomized
clinical trials, are being introduced and access to current research findings has
improved but remains limited. The development of the clinical practice guide-
lines, used in this study, and the testing of proposed implementation strategies is
new in the health system in Kazakhstan. In addition, this study tests the value of
complementary clinical training and population education to support newly
recommended practice.
The implementation strategy was meant to inform all primary care physicians
of evidence-based guideline, including those in both non-pilot and pilot facilities.
However, additional provider training and patient education occurred only in
pilot facilities. Thus, both non-pilot and pilot facilities were exposed to the
following:
1. Dissemination of an evidence-based clinical practice guideline (CPG) on
management of hypertension, and orientation of primary care providers to its
use, in 2004 (Dzhusipov et al. 2004, ZdravPlus Project 2004).
2. Introduction of a national outpatient drug benefit package, making hyper-
tension drugs available and affordable to patients, in January 2006.
3. Campaigns to raise patient awareness about routine blood pressure
measurements for screening purposes, in June 2006.
Management of Hypertension in Kazakhstan 215
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
17:
46 0
8 O
ctob
er 2
014
Pilot facilities, in addition, were exposed to the following:
1. Training of providers in use of the CPG, with focus on: (a) blood pressure
screening of all adult patients; (b) follow-up blood pressure measurements
for those identified with blood pressure]140/90 mmHg; (c) selection and
prescription of appropriate medications; (d) counselling of patients on
regular and long-term use of medications, and tips to remember daily drug
intake, reduction in salt, fat, cigarettes, and alcohol; and (e) regular exercise,
in October 2005.
2. Introduction of tools to prompt providers to practice according to the CPG
and to clinical training, especially related to patient counselling and
recording of tests, in November 2005.
3. Introduction of a quality improvement system, based on self-monitoring, for
doctors and facilities, in November 2005.
Although both non-pilot and pilot facilities were exposed to interventions to
improve hypertension case-finding, patient care, and treatment, only the pilot
area facilities were exposed to the added inputs of provider training and tools.
These added inputs were initiated based on the observation that the dissemina-
tion of the CPG and population campaigns did not seem to generate desired
changes in clinical practice, patient behaviours, or health outcome.
Conceptual framework, study design, and data sources
Our basic premise was that provider training, with emphasis on patient
counselling on regular use of medications and lifestyle changes, was required in
addition to dissemination of clinical guideline, population campaigns, and the
outpatient drug benefit package (Cranney et al. 2001, Cuspidi et al. 2002,
Roumie et al. 2006). To assess this hypothesis, we applied a quasi-experimental,
pre- and post-test, pilot and non-pilot, control groups design (Fisher et al. 1991).
Non-pilot and pilot facilities
Five non-pilot and six pilot government outpatient facilities, with similar
characteristics, were selected from Karaganda, an industrial city with an
estimated population of 450,000. Patients seek care at non-pilot or pilot facilities,
based primarily at the facility closest to their residence. Facilities were selected
following informal discussions with providers and health authorities based on
comparable features, such as staffing and patient load (see Table 1). Non-pilot
facilities included two polyclinics and three family group practices, where 74.5%
of the 170,226 patients were over 18 years old. Pilot facilities included two
polyclinics and four family group practices, where 72.7% of the 115,765 patients
were adults over age 18. The study randomly selected patients from non-pilot and
pilot sites, who were registered and seeking care from these sites.
216 A. Nugmanova et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
17:
46 0
8 O
ctob
er 2
014
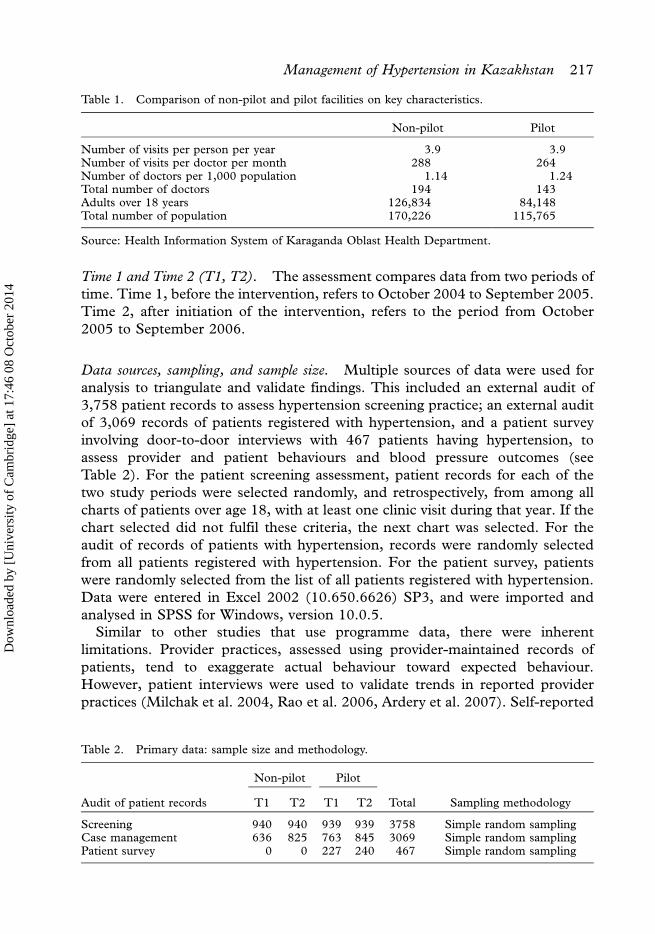
Time 1 and Time 2 (T1, T2). The assessment compares data from two periods of
time. Time 1, before the intervention, refers to October 2004 to September 2005.
Time 2, after initiation of the intervention, refers to the period from October
2005 to September 2006.
Data sources, sampling, and sample size. Multiple sources of data were used for
analysis to triangulate and validate findings. This included an external audit of
3,758 patient records to assess hypertension screening practice; an external audit
of 3,069 records of patients registered with hypertension, and a patient survey
involving door-to-door interviews with 467 patients having hypertension, to
assess provider and patient behaviours and blood pressure outcomes (see
Table 2). For the patient screening assessment, patient records for each of the
two study periods were selected randomly, and retrospectively, from among all
charts of patients over age 18, with at least one clinic visit during that year. If the
chart selected did not fulfil these criteria, the next chart was selected. For the
audit of records of patients with hypertension, records were randomly selected
from all patients registered with hypertension. For the patient survey, patients
were randomly selected from the list of all patients registered with hypertension.
Data were entered in Excel 2002 (10.650.6626) SP3, and were imported and
analysed in SPSS for Windows, version 10.0.5.
Similar to other studies that use programme data, there were inherent
limitations. Provider practices, assessed using provider-maintained records of
patients, tend to exaggerate actual behaviour toward expected behaviour.
However, patient interviews were used to validate trends in reported provider
practices (Milchak et al. 2004, Rao et al. 2006, Ardery et al. 2007). Self-reported
Table 2. Primary data: sample size and methodology.
Non-pilot Pilot
Audit of patient records T1 T2 T1 T2 Total Sampling methodology
Screening 940 940 939 939 3758 Simple random samplingCase management 636 825 763 845 3069 Simple random samplingPatient survey 0 0 227 240 467 Simple random sampling
Table 1. Comparison of non-pilot and pilot facilities on key characteristics.
Non-pilot Pilot
Number of visits per person per year 3.9 3.9Number of visits per doctor per month 288 264Number of doctors per 1,000 population 1.14 1.24Total number of doctors 194 143Adults over 18 years 126,834 84,148Total number of population 170,226 115,765
Source: Health Information System of Karaganda Oblast Health Department.
Management of Hypertension in Kazakhstan 217
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
17:
46 0
8 O
ctob
er 2
014

patient behaviour also carries the bias of responding according to expected
behaviour, and responses in the survey, long after the clinic visit, are vulnerable to
recall bias. However, blood pressure, measured at the end of patient interviews,
provides a biological marker that can be associated with reported behaviour,
allowing us to make stronger conclusions about the effect of the intervention.
Results
Case-finding
Available, feasible, and accurate means of detecting hypertension, and the clear
benefit of treatment, have led to the widespread acceptance of routine blood
pressure screening and the incorporation of this practice in the CPG (Sheridan
et al. 2003). One goal of our intervention strategy was to improve case-finding
among adults by promoting, at least yearly, blood pressure screening of adult
patients. A second goal was to increase follow-up blood pressure monitoring for
persons found to have blood pressure ]140/90 mmHg.
The intervention strategy for increasing the number of cases found included the
following:
1. Provider training in hypertension risk factors, the need for routine blood
pressure measurements, and systems to prompt providers to take and record
blood pressure measurement in patient records.
2. Patient education and counselling about hypertension risk factors and the
need for routine blood pressure measurements.
In addition, in both non-pilot and pilot facilities, in June 2006 a public campaign
was conducted throughout the city to increase awareness of cardiovascular
disease. This campaign included blood pressure measurements and the referral
for people found with blood pressure ]140/90 mmHg or with hypertension risk
factors. It should be noted that the assessment of increased case-finding through
routine blood pressure measurements was limited to clinic patients, and did not
include the general population where there are, undoubtedly, numerous people
with undiagnosed disease.
The comparison of patient records before and after the initiation of the
intervention, in non-pilot and pilot facilities, indicated a clear and significant
improvement in provider practices related to screening adult patients for high
blood pressure. Pilot facilities had a significant increase in: the percentage of adult
patients screened for high blood pressure (70.3�81.0%: pB0.005); the percen-
tage of patients followed-up if discovered to have high blood pressure]140/90
mmHg (71.4�89.9%: pB0.005); and the number of patients who registered for
management of hypertension once the diagnosis was made (53.0�75.1%:
pB0.005). In comparison, non-pilot facilities did not have a significant change
in these indicators.
When we compare non-pilot and pilot facilities at Time 2, pilot facilities are
significantly better than non-pilot facilities in the percentage of patients
218 A. Nugmanova et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
17:
46 0
8 O
ctob
er 2
014
screened and followed, but not in their registration of patients with hypertension
(see Table 3). This comparison at Time 2 should take into consideration that at
Time 1 the non-pilot facilities were significantly better in registering patients
with hypertension compared to the pilot facility (68.5% compared to 53.0%),
while at Time 2 the increased performance of the pilot facilities, following the
intervention, narrowed the difference between non-pilot and pilot facilities
(69.7% vs. 75.1%). Also noteworthy is that among patients with hypertension in
the pilot facilities at Time 2, the mean age is significantly younger in
comparison to Time 1 and to the non-pilot areas (60.690.42 compared to
61.990.44 at Time 1; and in non-pilot facilities the mean age was 63.590.42
[pB0.05] at Time 2 in comparison with 62.490.48 at Time 1). This may
reflect the success of pilot facilities in case-finding among younger people.
Provider and patient practices to manage hypertension
Another goal of the intervention strategy in pilot facilities was to improve case
management among patients with hypertension who were registered for care at
the facility. Previous experience has shown that a clinical guideline alone does not
always lead to improved practice unless additional inputs are present (Cranney
et al. 2001). The intervention strategy and added provider training focused on
achieving improvements in three critical areas of clinical practice: (1) prescription
of evidence-based medications along with advice on their regular and long term
use (ALLHAT 2002); (2) counselling on healthy lifestyles, with emphasis on
reducing salt and fat intake, and increasing regular exercise (Cutler 1993, Miller
et al. 2002); and (3) obtaining and recording ECG, urinalysis, blood glucose,
serum creatinine, and cholesterol tests, for patient management and care
(Cuspidi et al. 2002).
The intervention strategy to improve case management involved:
1. Patient assessment and diagnosis, and related medications and lifestyle
advice for case management, including additional clinical training, doctors’
reminders, and introduction of a quality improvement system.
2. Patient counselling on how to achieve long-term and regular medication use,
regular exercise, control of salt and fat intake, and reductions in smoking
and/or alcohol consumption. Patient counselling was complemented with
written materials and the option to participate in classes for patients with
hypertension.
3. Monitoring physicians’ use of five essential tests, with feedback.
In addition, in both the non-pilot and pilot facilities, the following interventions
influenced provider practices:
1. Dissemination of clinical guideline on diagnosis and management of patients
with hypertension, and informational sessions on their content and use.
2. Introduction of outpatient drugs benefits package that made first-line
medications affordable and available.
Management of Hypertension in Kazakhstan 219
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
17:
46 0
8 O
ctob
er 2
014

Table 3. Case-finding practices.
Comparison of Time 1 to Time 2Comparison of non-pilot(NP) to pilot (P) facilities
Non-pilot Pilot Time 1 Time 2
T1N�940% (n)
T2N�940% (n) T1-T2
T1N�939% (n)
T2N�939% (n) T1-T2 NP-P NP-P
BP measured at least once 68.1 (640) 69.0 (649) x2�0.200p�0.691
70.3 (660) 81.0 (761) x2�29.500p�0.000
x2�1.069p�0.318
x2�36.122p�0.000
If BP ]140/90 mmHgFollow-up measure
78.0 (131) 80.0 (140) x2�0.212p�0.692
71.4 (120) 89.9 (195) x2�21.628p�0.000
x2�0.906p�0.209
x2�7.582p�0.009
If BP ]140/90 Patientregistered
68.5 (115) 69.7 (122) x2�0.064p�0.816
53.0 (89) 75.1 (163) x2�20.526p�0.000
x2�8.435p�0.005
x2�1.424p�0.255
220
A.
Nugm
anov
aet
al.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
17:
46 0
8 O
ctob
er 2
014

The assessment strategy involved the comparison of data from before and after
the initiation of the intervention, in non-pilot and pilot facilities, and a patient
questionnaire, only in pilot facilities. The population sampled was similar in
non-pilot and pilot facilities at Time 1 by sex (p�0.767), but different at Time
2 because of increased case-finding among younger people in the pilot facilities.
At Time 1, it should be noted, the mean age in the non-pilot facilities did not
vary from that of the pilot facilities (62.3590.48 vs. 61.9090.44; F�0.498:
p�0.05).
Hypertension medication: provider prescription and patient adherence. The national
CPG promotes practices which are supported by evidence-based studies,
including: (1) use of thiazide diuretics to prevent cardiovascular complications
of hypertension (ALLHAT 2002); (2) use of beta-blockers, angiotensin-convert-
ing enzyme inhibitors (ACE inhibitors), and long acting dihydropyridine calcium
channel blockers (CCBs) (Neal et al. 2000); (3) use of more than one drug for
patients with moderate or severe hypertension (Law et al. 2003); (4) prioritized
control of systolic blood pressure to successfully prevent complications (Lewing-
ton et al. 2002); and (5) lifestyle interventions are extremely important, along
with the use of medication (Whelton et al. 2002). An emphasis was also placed on
regular, consistent, and long-term use of medication to respond to the usual local
pattern of episodic use. Thus, the CPG encourages the use of thiazide diuretics,
beta-blockers, ACE inhibitors, and CCBs, often in combination, to achieve a
usual blood pressure of less than 140/90 mmHg, with long-term maintenance
therapy, to maintain the improvement, similar to recommendations in other
commonly used guidelines, such as JNC-7 (Chobanian et al. 2003) and BHS-IV
(Williams et al. 2004).
After getting a prescription from the physician, patients go to an assigned
drugstore, where government subsidized medications are available at half price.
ACE inhibitors, thiazides, beta-blockers, and CCBs are all included in CPG, and
are available at subsidized cost, but ACE inhibitors continue to be most
commonly used, similar to other countries (Cuspidi et al. 2002). Both non-pilot
and pilot facilities, demonstrated a significant increase in prescribing practices of
appropriate first-line medications for hypertension (see Table 4). This effect is
attributed to both non-pilot and pilot facilities having an orientation to the correct
choice of hypertensive drugs, and to increased availability and affordability of
these drugs as a result of the outpatient drugs benefit package.
There was a significant increase in the use of thiazides in the pilot facilities
(p�0.000), whereas there was no significant increase in the non-pilot facilities.
This may be due to the emphasis given in the clinical trainings on thiazides
being unsurpassed in preventing cardiovascular complications in clinical trials.
Also noteworthy is the dramatic difference between non-pilot and pilot facilities,
in provider advice on the importance of regular and long-term use of
hypertensive medications (p�1.000 in non-pilot facilities and pB0.000 in pilot
facilities). At Time 2, in non-pilot facilities, 5.8% recorded giving advice on
Management of Hypertension in Kazakhstan 221
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
17:
46 0
8 O
ctob
er 2
014
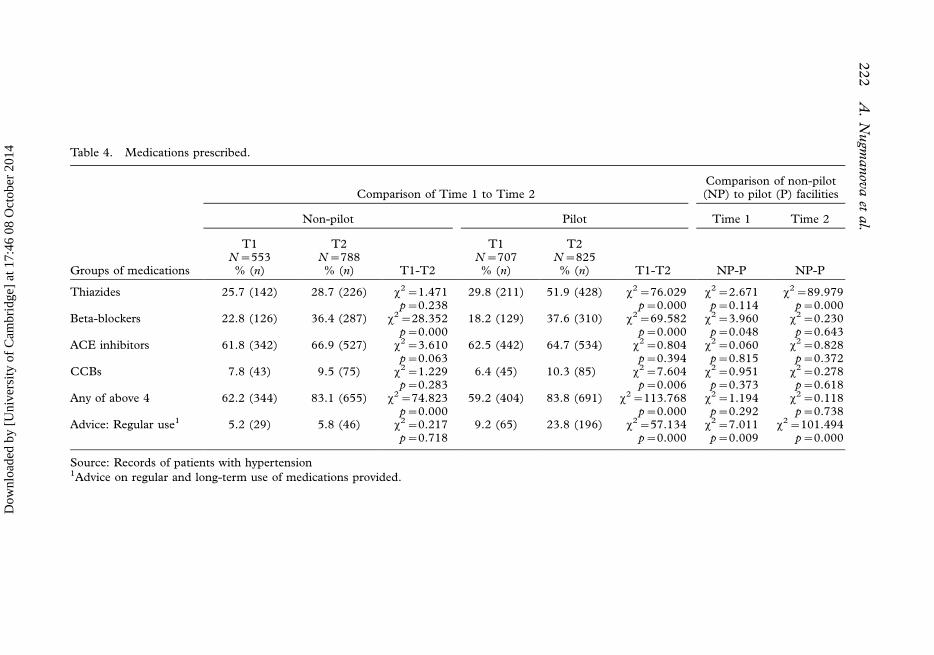
Table 4. Medications prescribed.
Comparison of Time 1 to Time 2Comparison of non-pilot(NP) to pilot (P) facilities
Non-pilot Pilot Time 1 Time 2
T1 T2 T1 T2N�553 N�788 N�707 N�825
Groups of medications % (n) % (n) T1-T2 % (n) % (n) T1-T2 NP-P NP-P
Thiazides 25.7 (142) 28.7 (226) x2�1.471 29.8 (211) 51.9 (428) x2�76.029 x2�2.671 x2�89.979p�0.238 p�0.000 p�0.114 p�0.000
Beta-blockers 22.8 (126) 36.4 (287) x2�28.352 18.2 (129) 37.6 (310) x2�69.582 x2�3.960 x2�0.230p�0.000 p�0.000 p�0.048 p�0.643
ACE inhibitors 61.8 (342) 66.9 (527) x2�3.610 62.5 (442) 64.7 (534) x2�0.804 x2�0.060 x2�0.828p�0.063 p�0.394 p�0.815 p�0.372
CCBs 7.8 (43) 9.5 (75) x2�1.229 6.4 (45) 10.3 (85) x2�7.604 x2�0.951 x2�0.278p�0.283 p�0.006 p�0.373 p�0.618
Any of above 4 62.2 (344) 83.1 (655) x2�74.823 59.2 (404) 83.8 (691) x2�113.768 x2�1.194 x2�0.118p�0.000 p�0.000 p�0.292 p�0.738
Advice: Regular use1 5.2 (29) 5.8 (46) x2�0.217 9.2 (65) 23.8 (196) x2�57.134 x2�7.011 x2�101.494p�0.718 p�0.000 p�0.009 p�0.000
Source: Records of patients with hypertension1Advice on regular and long-term use of medications provided.
222
A.
Nugm
anov
aet
al.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
17:
46 0
8 O
ctob
er 2
014
regular and long-term use of medications, in comparison with 23.8% in pilot
facilities (pB0.05).
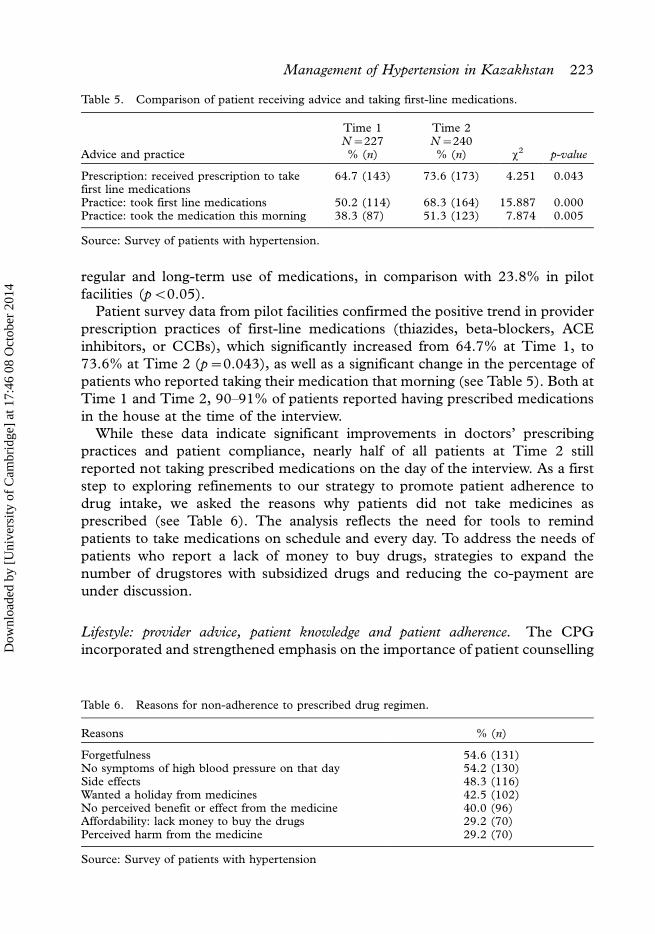
Patient survey data from pilot facilities confirmed the positive trend in provider
prescription practices of first-line medications (thiazides, beta-blockers, ACE
inhibitors, or CCBs), which significantly increased from 64.7% at Time 1, to
73.6% at Time 2 (p�0.043), as well as a significant change in the percentage of
patients who reported taking their medication that morning (see Table 5). Both at
Time 1 and Time 2, 90�91% of patients reported having prescribed medications
in the house at the time of the interview.
While these data indicate significant improvements in doctors’ prescribing
practices and patient compliance, nearly half of all patients at Time 2 still
reported not taking prescribed medications on the day of the interview. As a first
step to exploring refinements to our strategy to promote patient adherence to
drug intake, we asked the reasons why patients did not take medicines as
prescribed (see Table 6). The analysis reflects the need for tools to remind
patients to take medications on schedule and every day. To address the needs of
patients who report a lack of money to buy drugs, strategies to expand the
number of drugstores with subsidized drugs and reducing the co-payment are
under discussion.
Lifestyle: provider advice, patient knowledge and patient adherence. The CPG
incorporated and strengthened emphasis on the importance of patient counselling
Table 5. Comparison of patient receiving advice and taking first-line medications.
Advice and practice
Time 1N�227% (n)
Time 2N�240% (n) x2 p-value
Prescription: received prescription to takefirst line medications
64.7 (143) 73.6 (173) 4.251 0.043
Practice: took first line medications 50.2 (114) 68.3 (164) 15.887 0.000Practice: took the medication this morning 38.3 (87) 51.3 (123) 7.874 0.005
Source: Survey of patients with hypertension.
Table 6. Reasons for non-adherence to prescribed drug regimen.
Reasons % (n)
Forgetfulness 54.6 (131)No symptoms of high blood pressure on that day 54.2 (130)Side effects 48.3 (116)Wanted a holiday from medicines 42.5 (102)No perceived benefit or effect from the medicine 40.0 (96)Affordability: lack money to buy the drugs 29.2 (70)Perceived harm from the medicine 29.2 (70)
Source: Survey of patients with hypertension
Management of Hypertension in Kazakhstan 223
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
17:
46 0
8 O
ctob
er 2
014

on non-pharmacological lifestyle factors, that impact the management of
hypertension, based on evidence that supports the important role of reducing
salt, fat, alcohol, and cigarettes, controlling weight, and increasing regular
exercise (Sheridan et al. 2003).
In pilot facilities, there was a substantial and significant change in the
proportion of patients with hypertension who received counselling on salt
intake, exercise, and diet/weight control (pB0.005). In non-pilot facilities, an
increase was also observed, but this increase is not statistically significant,
except for advice on salt intake (pB0.005) (see Table 7). At Time 2, pilot
facilities compared to non-pilot facilities had a significantly larger proportion of
patients receiving advice on salt intake (pB0.05), exercise (pB0.100), and diet/
weight control (pB0.01), which is impressive considering the significantly
poorer baseline status of pilot facilities compared to non-pilot facilities at Time
1 (pB0.005).
Patient survey data from pilot facilities confirmed an increase in the receipt of
lifestyle advice on salt intake, diet and weight control, regular exercise, and
smoking cessation, and an increase in patient knowledge of salt reduction and
weight control as a means of controlling hypertension (see Table 8). However,
with the exception of an increase in the percentage of patients who report
exercising at least two times in the past 7 days, there were no significant changes
in reported lifestyle practices related to salt intake, diet or weight control, or
smoking. While the results on health worker compliance to providing patient
advice is encouraging, the change in self-reported patient behaviours is
discouraging, and suggests the need to develop more effective and targeted
counselling on lifestyle changes associated with hypertension control.
Monitoring health condition using biomedical tests: provider advice and patient
adherence. The national CPG incorporated the recommendation that patients
with hypertension be monitored, at least annually, using the following tests:
ECG, urinalysis, blood glucose, serum creatinine, and cholesterol. This was
based on the understanding that doing these tests helps doctors and patients
evaluate the risk of cardiovascular events, helps address and treat common co-
existing conditions, helps identify target organ damage resulting from hyperten-
sion, and provides regular feedback on patient and provider efforts to manage
the condition (Cuspidi et al. 2002). Assessment of provider compliance to tests,
suggested in the CPG and patient compliance to doctors’ advice to complete
the tests, was measured by test results being attached, or recorded, in patient
records (see Table 9).
In both non-pilot and pilot facilities, access to tests was equally available and
there was an increase, from Time 1 to Time 2, in the percentage of patients
with tests recorded. However, in the non-pilot facilities, the change was
significant only for cholesterol (pB0.05) and serum creatinine (pB0.10), while
in the pilot facilities the change was significant for all five of the tests
(pB0.005). It should be noted that at Time 1, non-pilot facilities had a higher
224 A. Nugmanova et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
17:
46 0
8 O
ctob
er 2
014
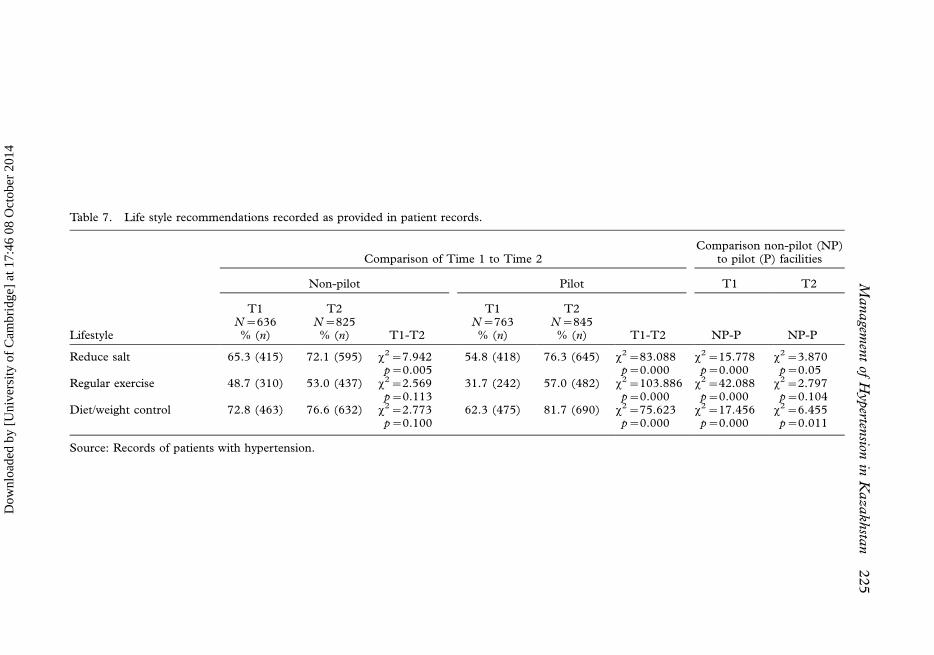
Table 7. Life style recommendations recorded as provided in patient records.
Comparison of Time 1 to Time 2Comparison non-pilot (NP)
to pilot (P) facilities
Non-pilot Pilot T1 T2
Lifestyle
T1N�636% (n)
T2N�825% (n) T1-T2
T1N�763% (n)
T2N�845% (n) T1-T2 NP-P NP-P
Reduce salt 65.3 (415) 72.1 (595) x2�7.942p�0.005
54.8 (418) 76.3 (645) x2�83.088p�0.000
x2�15.778p�0.000
x2�3.870p�0.05
Regular exercise 48.7 (310) 53.0 (437) x2�2.569p�0.113
31.7 (242) 57.0 (482) x2�103.886p�0.000
x2�42.088p�0.000
x2�2.797p�0.104
Diet/weight control 72.8 (463) 76.6 (632) x2�2.773p�0.100
62.3 (475) 81.7 (690) x2�75.623p�0.000
x2�17.456p�0.000
x2�6.455p�0.011
Source: Records of patients with hypertension.
Managem
ent
ofH
yperten
sionin
Kazakhsta
n225
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
17:
46 0
8 O
ctob
er 2
014
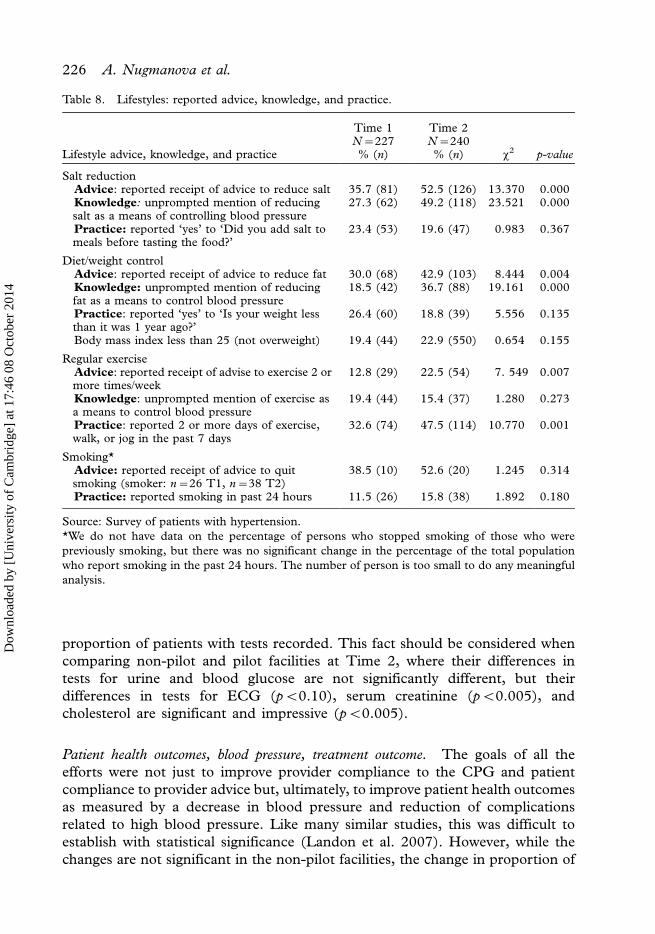
proportion of patients with tests recorded. This fact should be considered when
comparing non-pilot and pilot facilities at Time 2, where their differences in
tests for urine and blood glucose are not significantly different, but their
differences in tests for ECG (pB0.10), serum creatinine (pB0.005), and
cholesterol are significant and impressive (pB0.005).
Patient health outcomes, blood pressure, treatment outcome. The goals of all the
efforts were not just to improve provider compliance to the CPG and patient
compliance to provider advice but, ultimately, to improve patient health outcomes
as measured by a decrease in blood pressure and reduction of complications
related to high blood pressure. Like many similar studies, this was difficult to
establish with statistical significance (Landon et al. 2007). However, while the
changes are not significant in the non-pilot facilities, the change in proportion of
Table 8. Lifestyles: reported advice, knowledge, and practice.
Lifestyle advice, knowledge, and practice
Time 1N�227% (n)
Time 2N�240% (n) x2 p-value
Salt reductionAdvice: reported receipt of advice to reduce salt 35.7 (81) 52.5 (126) 13.370 0.000Knowledge: unprompted mention of reducingsalt as a means of controlling blood pressure
27.3 (62) 49.2 (118) 23.521 0.000
Practice: reported ‘yes’ to ‘Did you add salt tomeals before tasting the food?’
23.4 (53) 19.6 (47) 0.983 0.367
Diet/weight controlAdvice: reported receipt of advice to reduce fat 30.0 (68) 42.9 (103) 8.444 0.004Knowledge: unprompted mention of reducingfat as a means to control blood pressure
18.5 (42) 36.7 (88) 19.161 0.000
Practice: reported ‘yes’ to ‘Is your weight lessthan it was 1 year ago?’
26.4 (60) 18.8 (39) 5.556 0.135
Body mass index less than 25 (not overweight) 19.4 (44) 22.9 (550) 0.654 0.155
Regular exerciseAdvice: reported receipt of advise to exercise 2 ormore times/week
12.8 (29) 22.5 (54) 7. 549 0.007
Knowledge: unprompted mention of exercise asa means to control blood pressure
19.4 (44) 15.4 (37) 1.280 0.273
Practice: reported 2 or more days of exercise,walk, or jog in the past 7 days
32.6 (74) 47.5 (114) 10.770 0.001
Smoking*Advice: reported receipt of advice to quitsmoking (smoker: n�26 T1, n�38 T2)
38.5 (10) 52.6 (20) 1.245 0.314
Practice: reported smoking in past 24 hours 11.5 (26) 15.8 (38) 1.892 0.180
Source: Survey of patients with hypertension.
*We do not have data on the percentage of persons who stopped smoking of those who were
previously smoking, but there was no significant change in the percentage of the total population
who report smoking in the past 24 hours. The number of person is too small to do any meaningful
analysis.
226 A. Nugmanova et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
17:
46 0
8 O
ctob
er 2
014

Table 9. Tests recommended, completed, and recorded in patient records.
Comparison of Time 1 to Time 2Comparison of non-pilot(NP) to pilot (P) facilities
Non-pilot Pilot Time 1 Time 2
Tests
T1N�636% (n)
T2N�825% (n) T1-T2
T1N�763% (n)
T2N�845% (n) T1-T2 NP-P NP-P
ECG 65.3 (415) 64.2 (530) x2�0.160p�0.699
61.7 (471) 68.6 (580) x2�8.454p�0.004
x2�1.852p�0.181
x2�3.620p�0.062
Urinalysis 75.2 (478) 76.5 (631) x2�0.36p�0.579
71.2 (543) 78.9 (667) x2�12.992p�0.000
x2�2.802p�0.103
x2�1.447p�0.240
Blood Glucose 74.5 (474) 75.4 (622) x2�0.144p�0.715
67.9 (518) 77.5 (655) x2�18.822p�0.000
x2�7.410p�0.007
x2�1.043p�0.327
Serum creatinine 34.7 (221) 39.8 (328) x2�3.842p�0.057
19.8 (151) 51.8 (438) x2�177.367p�0.000
x2�39.759p�0.000
x2�24.521p�0.000
Cholesterol 33.6 (214) 39.9 (329) x2�5.972p�0.016
16.6 (127) 50.1 (423) x2�198.923p�0.000
x2�54.401p�0.000
x2�17.478p�0.000
Source: Records of patients with hypertension.
Managem
ent
ofH
yperten
sionin
Kazakhsta
n227
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
17:
46 0
8 O
ctob
er 2
014
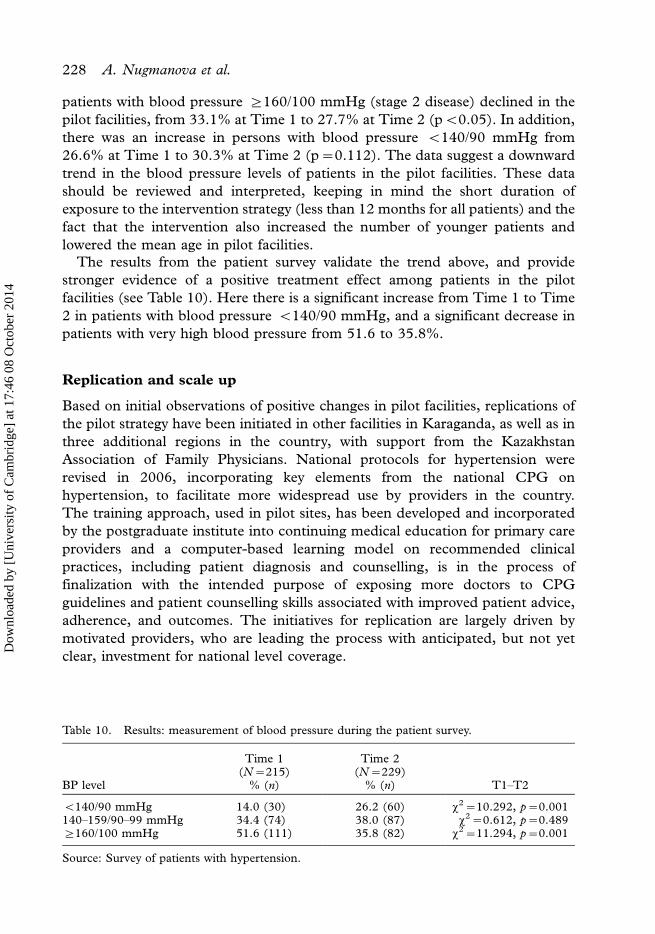
patients with blood pressure ]160/100 mmHg (stage 2 disease) declined in the
pilot facilities, from 33.1% at Time 1 to 27.7% at Time 2 (pB0.05). In addition,
there was an increase in persons with blood pressure B140/90 mmHg from
26.6% at Time 1 to 30.3% at Time 2 (p�0.112). The data suggest a downward
trend in the blood pressure levels of patients in the pilot facilities. These data
should be reviewed and interpreted, keeping in mind the short duration of
exposure to the intervention strategy (less than 12 months for all patients) and the
fact that the intervention also increased the number of younger patients and
lowered the mean age in pilot facilities.
The results from the patient survey validate the trend above, and provide
stronger evidence of a positive treatment effect among patients in the pilot
facilities (see Table 10). Here there is a significant increase from Time 1 to Time
2 in patients with blood pressure B140/90 mmHg, and a significant decrease in
patients with very high blood pressure from 51.6 to 35.8%.
Replication and scale up
Based on initial observations of positive changes in pilot facilities, replications of
the pilot strategy have been initiated in other facilities in Karaganda, as well as in
three additional regions in the country, with support from the Kazakhstan
Association of Family Physicians. National protocols for hypertension were
revised in 2006, incorporating key elements from the national CPG on
hypertension, to facilitate more widespread use by providers in the country.
The training approach, used in pilot sites, has been developed and incorporated
by the postgraduate institute into continuing medical education for primary care
providers and a computer-based learning model on recommended clinical
practices, including patient diagnosis and counselling, is in the process of
finalization with the intended purpose of exposing more doctors to CPG
guidelines and patient counselling skills associated with improved patient advice,
adherence, and outcomes. The initiatives for replication are largely driven by
motivated providers, who are leading the process with anticipated, but not yet
clear, investment for national level coverage.
Table 10. Results: measurement of blood pressure during the patient survey.
BP level
Time 1(N�215)
% (n)
Time 2(N�229)
% (n) T1�T2
B140/90 mmHg 14.0 (30) 26.2 (60) x2�10.292, p�0.001140�159/90�99 mmHg 34.4 (74) 38.0 (87) x2�0.612, p�0.489]160/100 mmHg 51.6 (111) 35.8 (82) x2�11.294, p�0.001
Source: Survey of patients with hypertension.
228 A. Nugmanova et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
17:
46 0
8 O
ctob
er 2
014
Conclusion
In both non-pilot and pilot areas, a basic package of health system inputs,
including orientation of providers to the clinical guideline, information to the
public on hypertension risks and annual screening, and an outpatient drug
benefit package, increased the number of new patients found and the use of
recommended medications. The strategy used in pilot facilities included
additional training to providers, as well as tools to prompt recommended
practices for doctors and to encourage compliance by patients. In pilot sites,
there were significantly greater improvements in case-finding, recommended
clinical practices, patient compliance to advice on medications and regular
exercise, and on blood pressure outcomes. However, study findings also suggest
the need for refinements in patient counselling, to further improve patient
adherence to regular use of required medications and lifestyle practices. Using
only patient survey information, where we compared two samples of patients,
before and after initiation of the intervention, we also found that in the pilot
area there was an increase in the proportion of patients with blood pressure
B140/90 mmHg, and a significant decrease in the proportion of patients with
stage two disease, or blood pressure]160/100 mmHg. The study results
demonstrate the added, and significant, value of complementing CPG with
clinical training and patient education, as well as tools to prompt provider and
patient behaviour. In addition, re-orientation of providers to client-oriented care
facilitates patient behaviours associated with improved health status.
Acknowledgements
We would like to express our appreciation to the United States Agency of
International Development (USAID); Sheila O’Dougherty (Regional Project
Director, ZdravPlus Project); Liza Myglina (Kazakhstan Country Manager/
Regional Programme Manager, ZdravPlus Project); Karaganda Oblast Health
Department for supporting all activities done within the project; Drug Informa-
tion Centre in Karaganda, Dr. Bahytgul Emekbaeva and Dr. Alexander Gulyaev
for participating in all stages of the project; Director of the Cardiology Institute,
Dr.Alikhan Dzhusipov, and his staff for collaboration in project implementation;
Kazakhstan Association of Family Physicians and its Karaganda branch (Dr.
Lyudmila Makazhanova and Dr. Baurzhan Omarkulov); and doctors from
Karaganda PHC facilities for active participation in all activities described;
Oleg Storozhenko (Regional EBM/CPG Director, ZdravPlus Project) for help
and comments given during project planning and implementation; the Health
Information System team of Karaganda oblast, for data collection and presenta-
tion; Hilda Kuter, for editing and giving recommendations in writing the article;
Timur Balabaev, for help in providing statistical analyses; and all patients with
hypertension who participated in the surveys. We thank the staff of the family
medicine departments of Almaty Postgraduate Institute for Physicians and
Karaganda State Medical Academy for providing clinical training and support.
Management of Hypertension in Kazakhstan 229
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
17:
46 0
8 O
ctob
er 2
014
References
ALLHAT (2002) Major Outcomes in High-Risk Hypertensive Patients Randomised to Angioten-sin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs. Diuretic: The Antihyper-tensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA, 288,2981�2997.
Ardery, G., Carter, B.L., Milchak, J.L., Bergus, G.R., Dawson, J.D., James, P.A., et al. (2007)Explicit and Implicit Evaluation of Physician Adherence to Hypertension Guidelines. Journal ofClinical Hypertension, 9, 113�119.
Chobanian, A.V., Bakris, G.L., Black, H.R., Cushman, W.C., Green, L.A., Izzo, J.I., Jr., et al.(2003) The Seventh Report of the Joint National Committee on Prevention, Detection,Evaluation, and Treatment of High Blood Pressure. The JNC 7 Report. JAMA, 289, 2560�2572.
Cutler, J.A. (1993) Combinations of Lifestyle Modification and Drug Treatment in Management ofMild-Moderate Hypertension: A Review of Randomised Clinical Trials. Clinical and Experi-mental Hypertension, 15, 1193�1204.
Cranney, M., Warren, E., Barton, S., Gardner, K. and Walley, T. (2001) Why do GPs notImplement Evidence-Based Guidelines? A Descriptive Study. Family Practice, 18, 359�363.
Cuspidi, C., Michev, I., Lonati, L., Vaccarella, A., Cristofari, M., Garavelli, G., et al. (2002)Compliance to Hypertension Guidelines in Clinical Practice: A Multicentre Pilot Study in Italy.Journal of Human Hypertension, 16, 699�703.
Dzhusipov, A.K., Gulyaev, A.E. and Alikhanova, K.A. (eds) (2004) Clinical Practice Guideline forProviding Care for Patients with Arterial Hypertension on the PHC Level (Astana: Vertsalex).
Fisher, A.A., Laing, J.E., Stoeckel, J.E. and Townsend, J.W. (1991) Handbook for Family PlanningOperations Research Design (New York: The Population Council).
Gaziano, T.A., Reddy, K.S., Paccaud, F., Horton, S. and Chaturvedi, V. (2006) Cardiovasculardisease. In D.T. Jamison, Breman, J.G., Measham, A.R., Alleyne, G., Claeson, M., Evans,D.B., et al. (eds) Disease Control Priorities in Developing Countries (Washington, DC: TheInternational Bank for Reconstruction and Development/The World Bank, , 645�662).
Kearney, P.M., Whelton, M., Reynolds, K., Muntner, P., Whelton, P.K. and He, J. (2005) GlobalBurden of Hypertension: Analysis of Worldwide Data. Lancet, 365, 217�223.
Landon, B.E., Hicks, L.S., O’Malley, A.J., Lieu, T.A., Keegan, T., McNeil, B.J., et al. (2007)Improving the Management of Chronic Disease at Community Health Centers. New EnglandJournal of Medicine, 356, 921�934.
Law, M.R., Wald, N.J., Morris, J.K. and Jordan, R.E. (2003) Value of Low Dose CombinationTreatment with Blood Pressure Lowering Drugs. British Medical Journal, 326, 1427�1431.
Lewington, S., Clarke, R., Qizilbash, N., Peto, R. and Collins, R. (2002) Age-Specific Relevance ofUsual Blood Pressure to Vascular Mortality: A Meta-Analysis of Individual Data for OneMillion Adults in 61 Prospective Studies. Lancet, 360, 1903�1913.
Milchak, J.L., Carter, B.L., James, P.A. and Ardery, G. (2004) Measuring Adherence to PracticeGuidelines for the Management of Hypertension: An Evaluation of the Literature. Hypertension,44, 602�608.
Miller, E.R., 3rd, Erlinger, T.P., Young, D.R., Jehn, M., Charleston, J., Rhodes, D. et al. (2002)Results of the Diet, Exercise, and Weight Loss Intervention Trial (DEW-IT). Hypertension, 40,612�618.
Neal, B., MacMahon, S. and Chapman, N. (2000) Effects of ACE Inhibitors, Calcium Antagonists,and other Blood-Pressure-Lowering Drugs: Results of Prospectively Designed Overviews ofRandomised Trials. Blood Pressure Lowering Treatment Trialists’ Collaboration. Lancet, 356,1955�1964.
Rao, M., Clarke, A., Sanderson, C. and Hammersley, R. (2006) Patients’ Own Assessments ofQuality of Primary Care Compared with Objective Records Based Measures of TechnicalQuality of Care: Cross Sectional Study. British Medical Journal, 333, 19�23.
Roumie, C.L., Elasy, T.A., Greevy, R., Griffin, M.R., Liu, X., Stone, W.J., et al. (2006) ImprovingBlood Pressure Control through Provider Education, Provider Alerts, and Patient Education.Annals of Internal Medicine, 145, 165�175.
Sheridan, S., Pignone, M. and Donahue, K. (2003) Screening for High Blood Pressure: A Reviewof the Evidence for the US Preventive Services Task Force. American Journal of PreventiveMedicine, 25, 151�158.
230 A. Nugmanova et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
17:
46 0
8 O
ctob
er 2
014

Whelton, P.K., He, J., Appel, L.J., Cutler, J.A., Havas, S., Kotchen, T.A., et al. (2002) The NationalHigh Blood Pressure Education Program. Primary Prevention of Hypertension: Clinical andPublic Health Advisory from the National High Blood Pressure Education Program. JAMA,288, 1882�1888.
Williams, B., Poulter, N.R., Brown, M.J., Davis, M., McInnes, G.T., Potter, J.F., et al. (2004)Guidelines for Management of Hypertension: Report of the Fourth Working Party of the BritishHypertension Society, 2004�BHS-IV. Journal of Human Hypertension, 18, 139�185.
ZdravPlus Project, Road to Results (2004) Clinical Practice Guideline Approved by the Ministry ofHealth. Accessed 27 February 2008, available at http://zplus.kz/Success/RTR_Clinical%20-Guidelines%20KZ_eng.pdf
Management of Hypertension in Kazakhstan 231
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
17:
46 0
8 O
ctob
er 2
014





























