Embed Size (px)
Citation preview
Herz 2013 · 38:387–390DOI 10.1007/s00059-012-3712-zReceived: 5 May 2012Revised: 27 September 2012Accepted: 3 October 2012Published online: 18 January 2013© Urban & Vogel 2013
R. Höllriegel1 · A. Linke1 · M. Hochadel2 · G. Schuler1 · S. Kerber3 · R. Hambrecht4 · E. Grube5 · K.E. Hauptmann6 · R. Zahn7 · U. Zeymer7 · J. Senges2
1 Department of Internal Medicine/Cardiology, University of Leipzig – Heart Center, Leipzig2 Institut für Herzinfarktforschung Ludwigshafen, University of Heidelberg, Ludwigshafen3 Department of Cardiology, Herz- und Gefäßklinik, Bad Neustadt (Saale)4 Heart Center Bremen, Klinikum Links der Weser, Bremen5 Department of Cardiology, Helios Heart Center, Siegburg6 IIIrd Medical Department – Cardiology, Krankenhaus der Barmherzigen Brüder, Trier7 Medical Department B, Klinikum Ludwigshafen, Ludwigshafen
Impact of coronary artery disease on in-hospital mortality in patients with aortic valve disease
Results from the German ALKK registry
Introduction
Aortic valve disease (AVD) has become the most frequent type of valvular heart disease in Europe and North America. In older adults, the predominant etiology is calcified aortic valve stenosis (AS; 2–7% of the population >65 years) [1, 2, 3, 4]. Comorbidities are frequent in this pop-ulation, especially coronary artery dis-ease (CAD). This is explained by the fact that especially AS and CAD share a num-ber of common pathophysiological path-ways and are associated with classical risk factors of atherosclerosis [5]. There-fore, AVD and especially AS are frequent-ly associated with CAD and coronary an-giography is widely used to detect or ex-clude CAD in those patients. Due to its potential risks, the invasive measurement of pressures and cardiac output is not rec-ommended routinely in patients with AVD, although it is still common in clini-cal practice [6].
We analyzed data of the coronary an-giography registry of the “Arbeitsgemein-schaft Leitende Kardiologische Kranken-hausärzte” (ALKK, Germany), to eluci-date the influence of concomitant CAD on in-hospital mortality rate in patients with AVD who underwent left heart cath-eterization.
Methods
The coronary angiography registry of the ALKK contains all consecutive diagnostic invasive and interventional procedures from a number of non-university centers in Germany since 2002. Rationale and de-tails of the registry have been published previously [7, 8]. In brief, the registry contains all consecutive procedures of the participating hospitals on an intention-to-treat basis. Data collection was performed with standardized electronic case record forms. All complications occurring in the catheterization laboratory and during the hospital stay were reported. The data were checked for completeness and consistency and queries for the centers were generated.
For this analysis, a total of 1427 con-secutive patients, who underwent an elec-tive diagnostic invasive procedure for the
evaluation of AVD in 2006, were analyzed regarding an accompanying CAD. All patients with acute coronary syndrome, cardiogenic shock or percutaneous coronary intervention during the hospital stay were excluded from the analysis.
Definitions
CAD was defined as at least one stenosis >50% in at least one coronary artery or previous coronary intervention.
Major adverse cardiac and cerebrovas-cular events (MACCE) and major adverse cardiac events (MACE) were defined as follows:FMACCE: major adverse cardiac and
cerebrovascular events, defined as the composite of death (cardiac and non-cardiac), nonfatal myocardial infarc-tion, and nonfatal stroke.
Original article
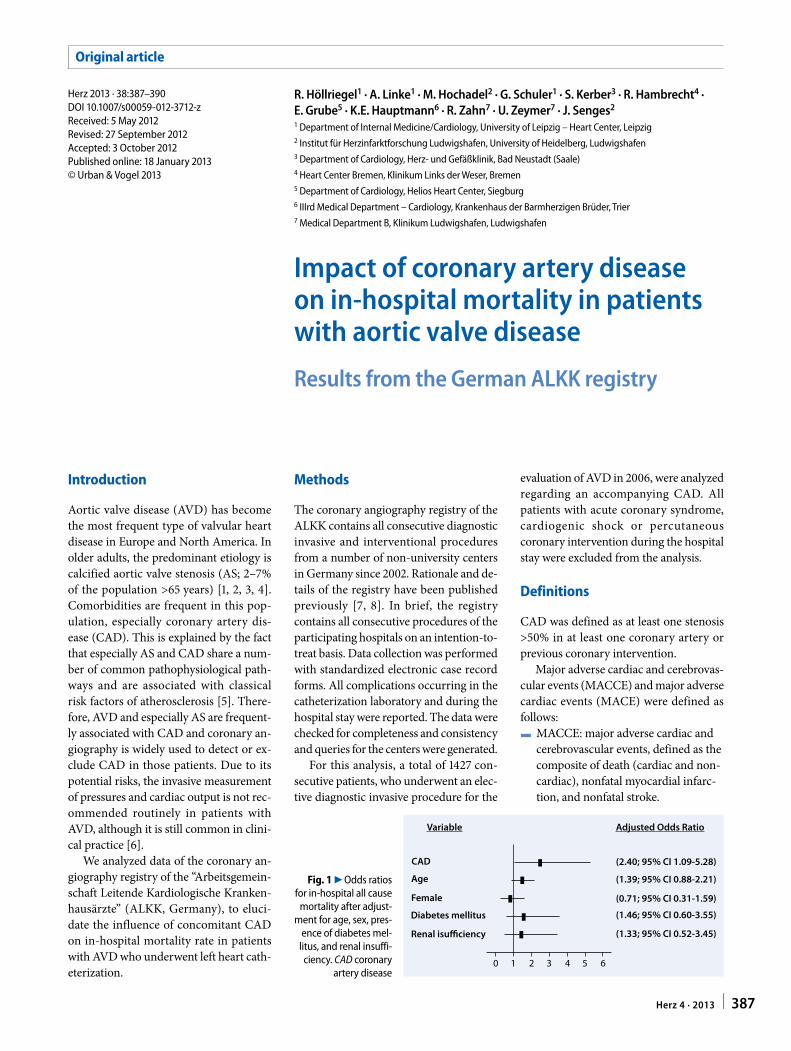
Variable Adjusted Odds Ratio
CAD
Age
Female
Diabetes mellitus
Renal isufficiency
0 1 2 3 4 5 6
(2.40; 95% CI 1.09-5.28)
(1.39; 95% CI 0.88-2.21)
(0.71; 95% CI 0.31-1.59)
(1.46; 95% CI 0.60-3.55)
(1.33; 95% CI 0.52-3.45)
Fig. 1 7 Odds ratios for in-hospital all cause
mortality after adjust-ment for age, sex, pres-
ence of diabetes mel-litus, and renal insuffi-ciency. CAD coronary
artery disease
387Herz 4 · 2013 |
FMACE: defined as a composite of death (cardiac and non-cardiac), non-fatal myocardial infarction.
Statistical analysis
Patient characteristics and outcomes are presented as absolute counts and percent-ages. The distribution of metric variables is described by medians. Binary variables were compared between subgroups by Pearson χ2 test and odds ratios with 95%
confidence intervals were computed. The Mann–Whitney test was used to compare the distribution of continuous variables. These statistics are based on the available cases.
Adjusted odds ratios for the effect of CAD and the basic risk factors age, sex, di-abetes, and renal insufficiency on in-hos-pital mortality were calculated by logistic regression. P values ≤0.05 were consid-ered significant. All p values are results of two-tailed tests. The statistical computa-
tions were performed with the SAS© sys-tem release 9.2 on a personal computer (SAS Institute, Inc., Cary, NC, USA).
Results
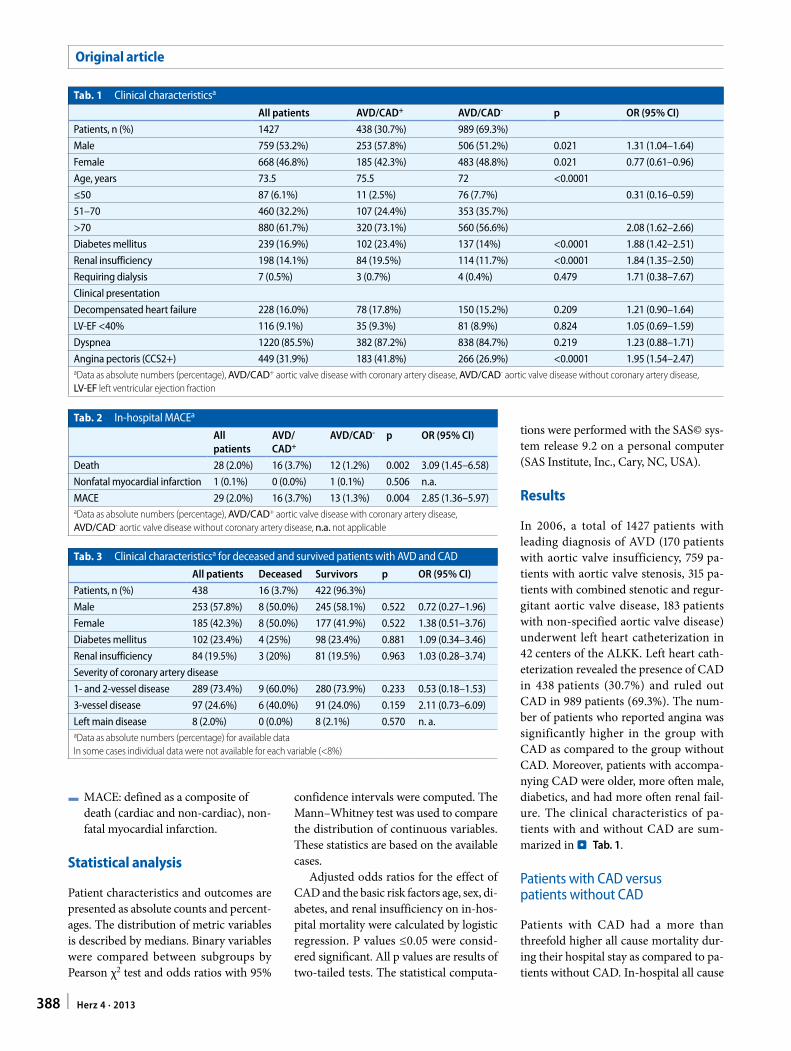
In 2006, a total of 1427 patients with leading diagnosis of AVD (170 patients with aortic valve insufficiency, 759 pa-tients with aortic valve stenosis, 315 pa-tients with combined stenotic and regur-gitant aortic valve disease, 183 patients with non-specified aortic valve disease) underwent left heart catheterization in 42 centers of the ALKK. Left heart cath-eterization revealed the presence of CAD in 438 patients (30.7%) and ruled out CAD in 989 patients (69.3%). The num-ber of patients who reported angina was significantly higher in the group with CAD as compared to the group without CAD. Moreover, patients with accompa-nying CAD were older, more often male, diabetics, and had more often renal fail-ure. The clinical characteristics of pa-tients with and without CAD are sum-marized in .Tab. 1.
Patients with CAD versus patients without CAD
Patients with CAD had a more than threefold higher all cause mortality dur-ing their hospital stay as compared to pa-tients without CAD. In-hospital all cause
Tab. 1 Clinical characteristicsa
All patients AVD/CAD+ AVD/CAD- p OR (95% CI)
Patients, n (%) 1427 438 (30.7%) 989 (69.3%)
Male 759 (53.2%) 253 (57.8%) 506 (51.2%) 0.021 1.31 (1.04–1.64)
Female 668 (46.8%) 185 (42.3%) 483 (48.8%) 0.021 0.77 (0.61–0.96)
Age, years 73.5 75.5 72 <0.0001
≤50 87 (6.1%) 11 (2.5%) 76 (7.7%) 0.31 (0.16–0.59)
51–70 460 (32.2%) 107 (24.4%) 353 (35.7%)
>70 880 (61.7%) 320 (73.1%) 560 (56.6%) 2.08 (1.62–2.66)
Diabetes mellitus 239 (16.9%) 102 (23.4%) 137 (14%) <0.0001 1.88 (1.42–2.51)
Renal insufficiency 198 (14.1%) 84 (19.5%) 114 (11.7%) <0.0001 1.84 (1.35–2.50)
Requiring dialysis 7 (0.5%) 3 (0.7%) 4 (0.4%) 0.479 1.71 (0.38–7.67)
Clinical presentation
Decompensated heart failure 228 (16.0%) 78 (17.8%) 150 (15.2%) 0.209 1.21 (0.90–1.64)
LV-EF <40% 116 (9.1%) 35 (9.3%) 81 (8.9%) 0.824 1.05 (0.69–1.59)
Dyspnea 1220 (85.5%) 382 (87.2%) 838 (84.7%) 0.219 1.23 (0.88–1.71)
Angina pectoris (CCS2+) 449 (31.9%) 183 (41.8%) 266 (26.9%) <0.0001 1.95 (1.54–2.47)aData as absolute numbers (percentage), AVD/CAD+ aortic valve disease with coronary artery disease, AVD/CAD- aortic valve disease without coronary artery disease, LV-EF left ventricular ejection fraction
Tab. 2 In-hospital MACEa
All patients
AVD/CAD+
AVD/CAD- p OR (95% CI)
Death 28 (2.0%) 16 (3.7%) 12 (1.2%) 0.002 3.09 (1.45–6.58)
Nonfatal myocardial infarction 1 (0.1%) 0 (0.0%) 1 (0.1%) 0.506 n.a.
MACE 29 (2.0%) 16 (3.7%) 13 (1.3%) 0.004 2.85 (1.36–5.97)aData as absolute numbers (percentage), AVD/CAD+ aortic valve disease with coronary artery disease, AVD/CAD- aortic valve disease without coronary artery disease, n.a. not applicable
Tab. 3 Clinical characteristicsa for deceased and survived patients with AVD and CAD
All patients Deceased Survivors p OR (95% CI)
Patients, n (%) 438 16 (3.7%) 422 (96.3%)
Male 253 (57.8%) 8 (50.0%) 245 (58.1%) 0.522 0.72 (0.27–1.96)
Female 185 (42.3%) 8 (50.0%) 177 (41.9%) 0.522 1.38 (0.51–3.76)
Diabetes mellitus 102 (23.4%) 4 (25%) 98 (23.4%) 0.881 1.09 (0.34–3.46)
Renal insufficiency 84 (19.5%) 3 (20%) 81 (19.5%) 0.963 1.03 (0.28–3.74)
Severity of coronary artery disease
1- and 2-vessel disease 289 (73.4%) 9 (60.0%) 280 (73.9%) 0.233 0.53 (0.18–1.53)
3-vessel disease 97 (24.6%) 6 (40.0%) 91 (24.0%) 0.159 2.11 (0.73–6.09)
Left main disease 8 (2.0%) 0 (0.0%) 8 (2.1%) 0.570 n. a.aData as absolute numbers (percentage) for available dataIn some cases individual data were not available for each variable (<8%)
388 | Herz 4 · 2013
Original article

mortality was 3.7% (16/438) in the group with CAD and 1.2% (12/989) in the group without CAD (p<0.01; OR 3.09, 95% CI 1.45–6.58). Even after adjustment for age, sex, presence of diabetes mellitus, and re-nal insufficiency, which were differently distributed in the two groups, in-hospi-tal all cause mortality remained signifi-cantly higher in the group with CAD (OR 2.40; 95% CI 1.09–5.28). Similarly, the in-hospital rates for MACE (p<0.01; OR 2.85, 95% CI 1.36–5.97) were significantly higher in patients with CAD (.Tab. 2). Due to the fact that no transient ischemic attacks or strokes were reported MACCE and MACE were equal in the groups. If patients with AVD were subdivided into aortic valve stenosis, aortic valve insuffi-ciency, combined aortic valve disease and the mortality in the different groups was analyzed based on the presence of CAD, the significance was lost.
AVD with CAD: deceased versus survivors
In a subgroup analysis of patients in the AVD with CAD group, no differenc-es were detectable between patients who died (n=16) and patients who survived (n=422) regarding age, sex, presence of diabetes mellitus, or renal insufficien-cy (.Tab. 3). If subdivided into patients with 1- and 2-vessel disease versus 3-vessel disease, a trend to higher in-hospital mor-tality for more severe CAD was determin-able (3.1% versus 6.2%, p=0.33). Patients who died during the hospital stay tended to have a higher CCS class at admission, although this was not significant (CCS III 80.0% versus 40.1%, p=0.07).
Procedure
No difference was detectable regarding the amount of contrast agent used and fluoroscopy time for patients with CAD versus without CAD (contrast agent vol-ume: 120 ml versus 110 ml, p=0.16; flu-oroscopy time: 6.1 min versus 5.2 min, p=0.11). Moreover, the subgroup analysis of patients in the group with CAD regard-ing both above mentioned parameters re-vealed no differences between survivors and deceased (contrast agent volume:
Abstract · Zusammenfassung
Herz 2013 · 38:387–390 DOI 10.1007/s00059-012-3712-z© Urban & Vogel 2013
R. Höllriegel · A. Linke · M. Hochadel · G. Schuler · S. Kerber · R. Hambrecht · E. Grube · K.E. Hauptmann · R. Zahn · U. Zeymer · J. Senges
Impact of coronary artery disease on in-hospital mortality in patients with aortic valve disease. Results from the German ALKK registry
AbstractObjective. Although aortic valve disease (AVD) is frequently associated with coronary artery disease (CAD), little is known about the impact of significant coronary artery disease on mortality after diagnostic cardiac cathe-terization in patients with AVD.Methods. We analyzed data of the coro-nary angiography registry of the “Arbeitsge-meinschaft Leitende Kardiologische Kranken-hausärzte” (ALKK) in Germany. The primary endpoint was in-hospital mortality.Results. A total of 1427 consecutive pa-tients with AVD (438 patients with CAD ver-sus 989 patients without CAD) underwent di-agnostic catheterization in 2006 in 42 hospi-tals. All cause in-hospital mortality was more than threefold higher in patients with CAD (16/438; 3.7%) as compared to patients with-out CAD (12/989; 1.2%; p<0.01; OR 3.09, 95% CI 1.45–6.58). Even after adjustment for age, sex, presence of diabetes mellitus and
renal insufficiency, in-hospital all cause mor-tality remained statistically significant differ-ent between the two groups (OR 2.4; 95% CI 1.09–5.28; p<0.01). Several factors, such as transient ischemic attack/stroke, volume of contrast agent, and left heart catheter-associ-ated complications could not be identified as possible causes for the increase in mortality.Conclusion. This analysis in patients with the leading diagnosis of AVD shows a signifi-cantly higher in-hospital mortality after diag-nostic cardiac catheterization in case of an ac-companying CAD. However, further studies are necessary to identify the driving force for the increase in mortality.
KeywordsAortic valve disease · Coronary artery disease · Diagnostics · Cardiac catheterization · Survival
Einfluss einer koronaren Herzkrankheit auf die intrahospitale Mortalität bei Patienten mit Aortenvitium. Resultate des ALKK-Registers
ZusammenfassungHintergrund. Aortenklappenvitien sind häu-fig mit einer koronaren Herzkrankheit (KHK) vergesellschaftet. Der Einfluss einer beglei-tenden KHK auf die intrahospitale Mortalität nach einer diagnostischen Herzkatheter-untersuchung bei Patienten mit einem füh-renden Aortenklappenvitium ist bisher un-bekannt.Methoden. Die Analyse erfolgte mit den Daten des Linksherzkatheterregisters der deutschen „Arbeitsgemeinschaft Leitende Kardiologische Krankenhausärzte“ (ALKK). Als primärer Endpunkt der Analyse wurde die in-trahospitale Mortaliät gewählt.Ergebnisse. Bei insgesamt 1427 konseku-tiven Patienten mit der Hauptdiagnose eines Aortenklappenvitiums (438 Patienten mit begleitender KHK versus 989 Patienten ohne KHK) wurde im Jahr 2006 in 42 Zentren eine diagnostische Herzkatheteruntersuchung durchgeführt. Patienten mit begleitender KHK hatten im Vergleich zu Patienten ohne KHK eine 3-fach höhere intrahospitale Mor-talität [3,7% (16/438) versus 1,2% (12/989);
p<0,01; OR: 3,09; 95%-KI: 1,45–6,58)]. Auch nach Adjustierung für Einflussfaktoren wie Alter, Geschlecht, Diabetes mellitus und Nie-reninsuffizienz blieb die intrahospitale Mor-talität statistisch signifikant verschieden zwischen den beiden Gruppen (OR: 2,4; 95%-KI: 1,09–5,28; p<0,01). Katheterassoziierte Komplikationen bzw. die verwendete Kon-trastmittelmenge konnten als Ursachen für den Unterschied ausgeschlossen werden.Schlussfolgerung. Patienten mit der Haupt-diagnose eines Aortenklappenvitiums ha-ben nach Durchführung einer diagnosti-schen Herzkatheteruntersuchung im Fall ei-ner begleitenden KHK eine signifikant höhere intrahospitale Mortalität. Zur Klärung der genauen Ursachen sind weitere Studien not-wendig, damit diese dann im klinischen All-tag berücksichtigt werden können.
SchlüsselwörterAortenklappenvitium · Koronare Herzkrankheit · Diagnostik · Herzkatheteruntersuchung · Überleben
389Herz 4 · 2013 |

115 ml versus 129 ml, p=0.77; fluorosco-py time: 7.1 min versus 6.0 min, p=0.78).
Discussion
AVD and especially AS is frequently asso-ciated with CAD and coronary angiogra-phy is commonly performed in those pa-tients. However, according to our data pa-tients with the leading diagnosis of AVD and accompanying CAD have significant-ly higher in-hospital all cause mortality af-ter left heart catheterization. Similarly to a report of Bermudez et al. [9], in our analy-sis the presence or absence of angina pec-toris did not predict the presence of CAD. More than 50% of patients with CAD did not report such symptoms, which implies that CAD also exists in a significant num-ber of asymptomatic patients with severe AVD. Therefore, the routine use of left heart catheterization is indicated and rec-ommended in patients >40 years and in younger patients with significant risk fac-tors for CAD since the presence of CAD effects the complexity of surgical inter-vention [10].
What might be the reason for the higher mortality in the AVD with CAD group? Unfortunately, no data are avail-able about causes of death. Just one death in the group without CAD was reported as a left heart catheter-associated compli-cation. No difference was detectable re-garding the amount of contrast agent in patients with CAD versus without CAD. Moreover, in-hospital MACCE was equal to in-hospital MACE. Therefore, transient ischemic attacks or strokes, contrast agent volume, and left heart catheter-associated complications do not seem to be relevant in this regard.
Most patients with severe AVD and es-pecially AS are characterized by concomi-tant increased oxygen requirement by the hypertrophic myocardium in the presence of diminished oxygen delivery second-ary to reduced coronary flow reserve and decreased diastolic perfusion pressure. These pathophysiological circumstanc-es may lead to a relative subendocardial ischemia. One could speculate that appli-cation of contrast agents in patients with AVD and accompanying CAD might lead to an aggravation of pre-existing myocar-dial ischemia. This notion is supported by
our data according to severity of CAD in dead and alive patients of the AVD with CAD group. Even if not statistically signif-icant, there was a strong trend for a high-er severity of CAD in dead patients. How-ever, this was not statistically significant most likely due to the small number of pa-tients in this subgroup.
Limitations of the study
As a retrospective, observational study, there are limitations inherent to such an analysis. We registered only in-hospital events and did not collect data after dis-charge. However, most events occur dur-ing or early after left heart catheterization, when patients are usually still in the hos-pital. We could not evaluate the influence of an invasive measurement of pressures and cardiac output regarding AVD in ad-dition to coronary angiography. There-fore, the unknown number of patients in whom the aortic valve was passed retro-gradely could have had an influence on the results. However, no transient isch-emic attacks or strokes were reported and death was only indicated as complication in 8.3% in the group without CAD ver-sus 0% in the group with CAD. We cannot exclude underreporting of complications, since no formal audit was performed.
Conclusion
Patients with AVD and especially AS fre-quently have an accompanying relevant CAD. Therefore, left heart catheteriza-tion is necessary in those patients in par-ticular due to its surgical implication. Re-garding to our data, patients with AVD and CAD have a significant 2.4-fold high-er in-hospital all cause mortality after diagnostic cardiac catheterization. For this reason, both the informed consent discussion and the commonly used in-formed consent sheet must have a state-ment added concerning higher mortali-ty in patients with AVD and CAD under-going diagnostic catheterization. Further studies are necessary to elucidate the un-derlying causes.
Corresponding address
R. HöllriegelDepartment of Internal Medicine/Cardiology, University of Leipzig – Heart CenterStruempellstr. 39, 04289 [email protected]
Conflict of interest. On behalf of all authors, the cor-responding author states that there are no conflicts of interest.
Reference
1. Stewart BF, Siscovick D, Lind BK et al (1997) Clini-cal factors associated with calcific aortic valve dis-ease. Cardiovascular Health Study. J Am Coll Cardi-ol 29:630–634
2. Otto CM, Lind BK, Kitzman DW et al (1999) Asso-ciation of aortic-valve sclerosis with cardiovascu-lar mortality and morbidity in the elderly. N Engl J Med 341:142–147
3. Soler-Soler J, Galve E (2000) Worldwide perspec-tive of valve disease. Heart 83:721–725
4. Iung B, Baron G, Butchart EG et al (2003) A pro-spective survey of patients with valvular heart dis-ease in Europe: the Euro Heart Survey on valvular heart disease. Eur Heart J 24:1231–1243
5. Rajamannan NM, Gersh B, Bonow RO (2003) Cal-cific aortic stenosis: from bench to the bedside—emerging clinical and cellular concepts. Heart 89:801–805
6. Vahanian A, Baumgartner H, Bax J et al (2007) Guidelines on the management of valvular heart disease: the task force on the management of val-vular heart disease of the European society of car-diology. Eur Heart J 28:230–268
7. Vogt A, Bonzel T, Harmjanz D, Leitner ER von et al (1997) PTCA registry of German community hos-pitals. Arbeitsgemeinschaft Leitender Kardiolo-gischer Krankenhausarzte (ALKK) Study Group. Eur Heart J 18:1110–1114
8. Zeymer U, Zahn R, Hochadel M et al (2005) Indi-cations and complications of invasive diagnostic procedures and percutaneous coronary interven-tions in the year 2003. Results of the quality con-trol registry of the Arbeitsgemeinschaft Leitende Kardiologische Krankenhausarzte (ALKK). Z Kardiol 94:392–398
9. Bermudez GA, Abdelnur R, Midell A, DeMeester T (1983) Coronary artery disease in aortic stenosis: importance of coronary arteriography and surgical implications. Angiology 34:591–596
10. Bhakhri K, Teoh K, Yap J (2012) Preoperative inves-tigations in adult cardiac surgery patients. Surgery 30:9–12
390 | Herz 4 · 2013
Original article

























