Embed Size (px)
Citation preview

1627
Intracerebral microdialysis began more than twenty yearsago when Delgado sealed the end of Gaddum’s push-pullcannula with a semipermeable membrane, combined it witha multiple electrode, called it a "dialytrode", and stuck it in amonkey brain. 1,2 Subsequent use of intracerebral
microdialysis in rodents, cats, and non-human primates hascontributed to our understanding of the role of the cerebralmicroenvironment and of particular neurotransmitters instates of arousal, appetitive and addictive behaviours,movement disorders, epilepsy, cerebral ischaemia, andtraumatic injury of brain and spinal cord. Has this
technique an application in human neurosurgery and if so inwhich condition?The front runner has long seemed to be head injury, in
which a microdialysis probe might readily accompany apressure monitor and provide a guide to metabolic state.4The opportunity to test microdialysis acutely in man wasprovided by stereotaxic treatment in parkinsonism but itsclinical value in this context is not evident.5 Epilepsy hasnow come in ahead of the field thanks to the ingenuity anddetermination of During and Spencer at Yale. Their latestobservations (p 1607) are noteworthy in that, in addition tomaking a strong case for the clinical usefulness of cerebralmicrodialysis (by aiding identification of the site of seizureorigin), they show that the technique contributes to ourunderstanding of the pathophysiology of epilepsy.
In patients with refractory complex partial seizures
requiring depth electrode studies, During and Spencerimplanted microdialysis probes bilaterally along the
hippocampus. Their measurements of glutamate and
gamma-aminobutyric acid (GABA) concentrations inrelation to the electrographic onset of spontaneous seizuresshow an increase in glutamate concentration directly beforeseizure onset on the epileptogenic side. This result accordswith earlier preliminary findings in man6,7 and in laboratoryanimals.8 The non-epileptogenic hippocampus shows asmaller increase in glutamate concentration beginning afterseizure onset, and a simultaneous increase in GABAconcentration which is larger than that on the epileptogenicside.
Rises in extracellular neurotransmitter concentration mayindicate increased synaptic release but they may also dependon non-synaptic release or diminished or "reversed" uptake.Epileptologists have long speculated as to what governs thetransition from the interictal to the ictal state. The data of
During and Spencer provide the clearest evidence yet thatenhanced activation of glutamate receptors contributes tothe initiation of focal seizure activity. GABA may act todelay or limit the spread of seizure activity. Adenosinerelease probably has a role in terminating seizure activity.9 9This study does not contribute decisively to the debate
about excitotoxic cell death in epilepsy. From animalexperiments we know that activation of N-methyl-D-aspartate receptors contributes to cell death in hippocampalpyramidal neurons during lengthy limbic seizures. Thebrief seizures described by During and Spencer would not,however, be expected to give rise to nerve cell death.Observations of toxicity of glutamate in tissue culture are ofuncertain relevance in vivo.
During and Spencer’s study differs from earlier ones inwhich microdialysis was used in that it involved chronicmonitoring (up to 16 days) in conscious patients. Thus the
practical and ethical difficulties can be overcome. At presentmicrodialysis is only justifiable when there are compellingreasons for neurosurgical intervention and when theinclusion of the microdialysis probe does not add
appreciably to the risks.Intracerebral microdialysis has helped us to understand
the pathophysiology of ischaemia, central nervous systemtrauma, and epilepsy in laboratory animals and will haveincreasing application clinically. Many factors such as thetime and space available in intensive care units willdetermine how soon such discoveries can be translated intoroutine procedures for investigating and monitoringpatients.
B. S. Meldrum
1. Delgado JMR, DeFeudis FV, Roth RH, Ryugo DK, Mitruka BM.Dialytrode for long term intracerebral perfusion in awake monkeys.Arch Int Pharmacodyn 1972; 198: 9-21.
2. Delgado JMR, Lerma J, Martin del Rio R, Solis JM. Dialytrodetechnology and local profiles of aminoacids in the awake cat brain.J Neurochem 1984; 42: 1218-28.
3. Benveniste H, Huttemeier PC. Microdialysis: theory and application.Prog Neurobiol 1990; 35: 195-215.
4. Persson L, Hillered L. Chemical monitoring of neurosurgical intensivecare patients using intracerebral microdialysis. J Neurosurg 1992; 76:72-80.
5. Meyerson BA, Linderoth B, Karlsson H, Ungerstedt U. Microdialysis inthe human brain: extracellular measurements in the thalamus ofParkinsonian patients. Life Sci 1990; 46: 301-08.
6. Do KQ, Klancnik JM, Gahwiler B, Pershak H, Wieser H-G, Cuenod M.Release of excitatory amino adds: animal studies and epileptic focistudies in humans. In: Meldrum BS, Moroni F, Simon RP, Woods J,eds. Excitatory amino acids. New York: Raven, 1991: 677-86.
7. Carlson H, Ronne-Engstrom E, Ungerstedt U, Hillered L. Seizurerelated elevations of extracellular amino acids in human focal epilepsy.Neurosci Lett 1992; 140: 30-32.
8. Millan H, Chapman AG, Meldrum BS. Extracellular amino add levels inhippocampus during pilocarpine-induced seizures. Epilepsy Res 1993;14: 139-48.
9. During MJ, Spencer DD. Adenosine: a potential mediator of seizurearrest and postictal refractoriness. Ann Neurol 1992; 32: 618-24.
IMMUNOLOGY
Superantigens and infectious disease
The mechanism by which foreign antigens are presentedto T lymphocytes is central to the whole of immunology.The essentials are increasingly familiar to clinicians,particularly those who deal with diseases with an
immunological basis. Nevertheless, a brief resume of normalantigen presentation may be helpful. T cells recogniseconventional antigens not as whole proteins but as shortpeptide fragments derived from the protein by intracellularprocessing, and bound in a groove on the heavy chain of theclass I and class II molecules of the major histocompatibilitycomplex (MHC). Certain aminoacid residues at critical
points in the peptide sequence "anchor" the peptide in thegroove, and this interaction is moderately specific for each ofthe different allelic forms of MHC molecules. The endresult is that a complex of peptide and MHC molecule (andthe MHC molecule must be the same allelic form as that onthe T cell) is recognised by the T-cell receptor (TCR), withconsequent activation of the T cell and expression of itseffector functions. The TCR consists of ot and 0 chains, eachcomposed of variable (V) and joining (J) segments (with anadditional diversity [D] segment for the P chain); thesesegments are encoded by separate genes which undergoDNA rearrangement to give many different combinations.
EPILEPSY
Intracerebral microdialysis and seizure initiation

1628
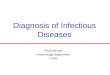
Mechanism of action of a conventional antigen and a
superantigen.
The association of peptides with MHC alleles on the onehand, and the diversity of the TCR on the other, allows Tcells to recognise a huge number of antigens whilst
conferring extreme specificity on this recognition. All of thismeans that only a small fraction of all T cells will respond toany given antigen (see figure, top).However, in the past few years a class of antigens has
emerged that does not conform to this conventional pathwayof antigen presentation. These so-called superantigens havebeen named for their ability to activate simultaneously largenumbers of T cells.1 Superantigens do this by bypassing thenormal route of intracellular processing and binding directlyas intact proteins to class II MHC molecules at a site distinctfrom the peptide binding groove; they also bind to mostallelic forms of class II molecules rather than to restrictedalleles as do conventional peptide antigens. The
superantigen/MHC complex then reacts with the TCRthrough the V segment of the 0 chain (V(3), rather than withthe normal antigen-binding site on the TCR composed ofboth a and 0 chains. Furthermore, superantigens react withall T cells carrying a particular V (3 gene. Since there are 50different Vp genes in humans, a superantigen reacts withmore than 1 in 50 T cells whereas a conventional peptideantigen will react with 1 in 1()4 to 1 in 106 T cells (see figure,bottom).Two groups of proteins have been shown to act as
superantigens, one exogenous to the host and the othercarried endogenously in the host’s genome.2 The first groupare nearly all bacterial exotoxins.2,3 They include exotoxinsproduced by staphylococci-the toxins causing food
poisoning (enterotoxins A, B, C 1-3, D, and E), toxic shocksyndrome (TSST-1), and the scalded skin syndrome(exfoliating toxins A and B)—by group A streptococci (theirpyrogenic exotoxins A, B, C, and D), and by Clostridiumperfringens and Yersinia enterocolitica (their enterotoxins).Mycoplasma arthritidis also produces a superantigen.4 Thebacterial exotoxin superantigens are small proteins that bindto class I I molecules with high affinity and each stimulates Tcells through several different Vp segments. They areespecially strong T-cell mitogens and activate both CD4+ +
and CD8+ T cells (whereas conventional antigens presentedby class II MHC molecules activate only CD4+ T cells).The second class of superantigens has been clearly
defined only in the mouse. A group of antigens capable ofstimulating a strong mixed lymphocyte reaction between
mice of the same MHC haplotype was recognised some timeago, and these were termed minor lymphocyte stimulating(Mls) determinants. They also act by binding to class IIMHC molecules and stimulating large numbers of T cellsthrough their Vp elements. We now know that MIsdeterminants are proteins encoded by genes of mousemammary tumour viruses integrated and verticallytransmitted in the mouse genome5-in effect they areself-antigens, and as with any self-antigen encountered by Tcells during their maturation in the thymus, T cells that reactwith MIs determinants are clonally eliminated in their earlydevelopment with consequent "skewing" of the animal’s Vp z3T-cell repertoire. An interesting consequence of this processis that the mice are then resistant to infection with exogenousmammary tumour viruses.What are the clinical implications of all this? The different
ways in which superantigens activate T cells casts light on thepathogenesis of infectious disease.6 The ability of bacterialexotoxins to activate large numbers of T cells with
consequent release of cytokines could directly account fortheir pathogenic effects and the clinical syndromes theyproduce. For example, experimental staphylococcalenterotoxin shock depends on superantigen-induced releaseof tumour necrosis factor mediated via T cells.’ Widespreadactivation of T cells, with selective representation of
particular Vp elements, is also a feature of some
inflammatory joint diseases linked with infective agents8 andof Kawasaki disease,9 and superantigen effects could accountfor these associations. Intravenous immunoglobulin (IVIg)is reported to contain specific antibodies to exotoxin
superantigens; this feature might provide an explanation forthe therapeutic actions of IVIg in diseases in which
superantigens have been implicated in the aetiology.lONo human equivalent of the endogenous mouse retroviral
superantigens has yet been described. However, one
suggestion is that acquired human retroviruses (such asHIV) might act as superantigens, and that this propertycould contribute to the T-cell abnormalities they produce.Retrovirus integration and replication require activation anddivision of T cells, so the ability to stimulate T-cell divisionby a superantigen effect would be an advantage to T-cell-tropic retroviruses. Reports of selective depletion of acommon set ofVp elements in people with HIV infection,"and that HIV selectivity stimulates and replicates in CD4cells with particular V (3 elements in vitro,12 are compatiblewith (but not proof of) HIV encoding a superantigen.
Already it seems clear that superantigens are yet anotherexample of microbial pathogens evolving mechanisms to useand subvert the immune response; we shall hear more oftheir role in infective and autoimmune disease.
J. G. P. Sissons
1. Möller G, ed. Superantigens. Immunol Rev 1993; 131: 1-200.2. Marrack P, Winslow GM, Choi Y, et al. The bacterial and mouse
mammary tumour virus superantigens: two different families of
proteins with the same function. Immunol Rev 1993; 131: 79-92.3. Bowness P, Moss PAH, Tranter H, et al. Clostridium perfringens
enterotoxin is a superantigen reactive with human T cell receptors V&bgr;6.9 and V&bgr; 22. J Exp Med 1992; 176: 893-96.
4. Cole BC. The immunobiology of Mycoplasma arthritidis and its
superantigen MAM. Curr Topics Microbiol Immunol 1991; 174:107-19.
5. Winslow GM, Scherer MT, Kappler JW, et al. Detection andbiochemical characterization of the mouse mammary tumor virus7 superantigen (Mls-18). Cell 1992; 71: 719-30.
6. Johnson HM, Russell JK, Pontzer CH. Superantigens inhuman disease.Sci Am 1992; 266: 92-101.
7. Miethke T, Wahl C, Heeg K, et al. T cell mediated lethal shock triggered

1629
in mice by the superantigen staphylococcal enterotoxin B: critical roleof tumour necrosis factor. J Exp Med 1992; 175: 91-98.
8. Paliard X, West SG, Lafferty JA, et al. Evidence for the effects of asuperantigen in rheumatoid arthritis. Science 1991; 253: 325-29.
9. Abe J, Kotzin BL, Jinjo K, et al. Selective expansion of T cells expressingT cell receptor variable regions V&bgr;2 and V&bgr;8 in Kawasaki disease. ProcNatl Acad Sci USA 1992; 89: 4066-70.
10. Takei S, Arora YK, Walker SM. Intravenous immunoglobulin containsspecific antibodies inhibitory to activation of T cells by staphylococcaltoxin superantigens. J Clin Invest 1993; 91: 602-07.
11. Imberti L, Sottini A, Bettinardi A, et al. Selective depletion in HIVinfection of T cells that bear specific T cell receptor V&bgr; sequences.Science 1991; 254: 860-62.
12. Laurence J, Hodtsev AS, Posnett DN. Superantigen implicated independence of HIV-1 replication in T cells on TCR V&bgr; expression.Nature 1992; 358: 255-59.
PERIOPERATIVE BLEEDING
Drugs for surgical blood loss
In 1988 a Lancet editorial inquired "Can drugs reducesurgical blood loss?". The answer is yes. The question nowis: "Which drug is best?". Ideally the agent should reducebleeding sufficiently to allow the patient to undergo surgerywithout the need for blood transfusion and should obviatethe risk of postoperative anaemia. Other requirements areapplicability to various procedures. The early promise ofdesmopressin in this role has faded and there is now little tosupport its routine use except in patients with uraemia. Theantiplatelet agents prostacyclin and dipyridamole are
likewise not routinely used because of their cardiovasculareffects and poor efficacy, respectively. Consequently, thechoice seems to lie between the lysine analogues, tranexamicacid and s-aminocaproic acid, and the serine proteaseinhibitors (SERPINs), aprotinin, nefamostat, and gabexate.Such agents have been used effectively in patientsundergoing dental, orthopaedic, hepatic, vascular, andneurosurgery procedures,1-3 but most of the data on the useof such drugs have accrued from cardiac surgery.6
After major surgery, either class of drug reduces
perioperative bleeding. However, if the primary endpointfor efficacy is the need for donor blood, differences becomeapparent. With the exception of aprotinin, none of theagents has been shown to influence the requirements forblood or blood-product transfusion consistently or
substantially, particularly in the high-risk categories ofsurgical, and especially cardiac surgical, patients. SERPINsalso suppress some potentially damaging inflammatorypathways. Plateletb and white cell activation2 are inhibited,as is the release of agents such as arachidonic acidmetabolites, specifically thromboxane6 and cytokines suchas interleukin-8/What about concerns over safety? In particular, are
blood-sparing agents associated with a higher mortality ormorbidity as a result of excess clot formation? The lysineanalogues are antifibrinolytics that inhibit certain plateletfunctions and have no effects on the coagulation process;they cannot initiate or accelerate clot formation but willdelay clot lysis. SERPINs are inhibitors of both plateletfunction and coagulation. They inhibit coagulation evenwhen there is a hypercoagulable state8 and reduce the
deposition of organ microemboli in cases of disseminatedintravascular coagulation associated with sepsis.9 Aprotininhas been used to reduce the incidence of deep-veinthrombosis following hip surgery. However, this inhibition
of coagulation has some drawbacks, and has led to
considerable difficulties in ensuring appropriate heparinadministration during cardiac surgery.
In large studies there is no evidence of increased mortalitywhen either class of agent was used, but what aboutmorbidity? Thrombosis of cerebral vessels is a reportedcomplication when tranexamic acid is given over severaldays,3 but not when use is restricted to the period of cardiacsurgery. Nonetheless, stroke was observed only in patientsin the treatment group in the studies from Philadelphia.4The rate of stroke in high-risk cardiac surgery patientsreceiving aprotinin therapy is lower than would be
anticipated.6 Concerns have also been expressed about thepossibility of graft occlusions and increased myocardialischaemia, especially in patients undergoing myocardialrevascularisation. With both lysine analogues and aprotinin,more postoperative myocardial infarctions have been
reported in treated patients5,10 although the increase is notstatistically significant.The effect of lysine analogues on graft patency has not
been formally investigated. In low-risk patients there is noeffect of aprotinin on graft patency; in high-risk patientsthere have been reports suggesting graft occlusion in
patients receiving the drug. In one study,lO necropsy wasundertaken in about half of the patients who died, andshowed graft occlusion only in patients given aprotinin. Asurprising observation is that the thrombosed grafts wereconfined to the patients who received a low dose ofaprotinin; graft occlusions were not seen in patients allocatedto receive a high dose or placebo.
There are several outstanding issues. We need moreinformation about which agent and dose is appropriate forall these compounds, and we also need to know more abouttheir efficacy in reducing the need for donor blood and theirsafety profile in high-risk procedures. Lysine analogues costless than SERPINs. With both classes of compounds thechallenge is to show that the risk of administration is verylow, and certainly less than that of blood products.
David Royston
1. Mallett SV, Cox D, Burroughs AK, Rolles K. Aprotinin and reduction ofblood loss and transfusion requirements in orthotopic liver
transplantation. Lancet 1990; 336: 886-87.2. Lord RA, Roath OS, Thompson JF, Chant ADB, Francis JL. Effect of
aprotinin on neutrophil function after major vascular surgery. Br JSurg 1992; 79: 517-21.
3. Wijdicks EFM, Hasan D, Lindsay KW, et al. Short term tranexamic acidtreatment in aneurysmal subarachnoid hemorrhage. Stroke 1989; 20:1674-79.
4. Horrow JC, van Riper DF, Strong MD. The hemostatic effects oftranexamic add and desmopressin during cardiac surgery. Circulation1991; 84: 2063-69.
5. Øvrun E, Holen EA, Abdelmoor M, Øystese R, Ringdal ML.Tranexamic acid (Cyclokapron) is not necessary to reduce blood lossafter coronary artery bypass operations. J Thorac Cardiovasc Surg1993; 105: 78-83.
6. Royston D. High dose aprotinin: a review of the first five years’experience. J Thorac Cardiovasc Anaesth 1992; 6: 76-100.
7. Whitten CW, Latson TW, Allison PM, et al. Does aprotinin inhibitcardiopulmonary bypass induced inflammation? Anesthesiology 1992;77: A266 (abstr).
8. Herschlein HJ, Steichele DF. Die Hemmung der Hyperkoagulabilitätdes Blutes. Med Welt 1964; 24: 1314-17.
9. Kojima M, Shimamura K, Mori N, Oka K, Nakazawa M. A histologicalstudy on micro thrombi in autopsy cases of DIC. Bibl Haematol 1983;49: 95-106.
0. Cosgrove DM, Heric B, Lytle BW, et al. Aprotinin therapy for
reoperative myocardial revascularization: a placebo-controlled study.Ann Thorac Surg 1992; 54: 1031-38.