-
8/13/2019 Immobilization Extrication
1/75
IMMOBILIZATION
EXTRICATIONBy;
Nazri B. Aiwan @ Ismail
Kolej Pembantu Perubatan Ulu Kinta
-
8/13/2019 Immobilization Extrication
2/75
Introduction
To move casualty to hospital.
Early priority in the rescue effort.
Need appropriately planned.
To ensure safe and speedy transportation
while maintaining casualty comfort,
preventing further injury or damage &allowing full
monitoring to take place.
-
8/13/2019 Immobilization Extrication
3/75
-
8/13/2019 Immobilization Extrication
4/75
Basic Principles of Immobilization
1. To prevent further injury.
2. To provide pain relief.
3. To reduce blood loss.
4. To reduce the risk of fat emboli.
5. To facilitate extrication & rescue.
-
8/13/2019 Immobilization Extrication
5/75
-
8/13/2019 Immobilization Extrication
6/75
Basic Principles of Immobilization
3. To reduce blood loss
Traction splintage of long bone # ;
volume available for hematoma formation.
Restore muscle tensionclosed largevenous channels.
4. To reduce the risk of fat emboli
incidence marrow fat emboli enters venouscirculation.
-
8/13/2019 Immobilization Extrication
7/75
Basic Principles of Immobilization
5. To facilitate extrication & rescueImmobilization
Should be supported on either site of the #.
Immobilized the joints above & below theinjury.
The principles of equipments design;
simple
easy to uselightweight
Damage-proof
Easily cleaned following use.
-
8/13/2019 Immobilization Extrication
8/75
Basic Principles of Extrication
Entrapment
trapped casualty. Hospital staff alert for possible problems
a) Actual entrapment;
Victims are physically enclosed in avehicle or in area by the
structureimpinging on their body eg MVA, buildingcollapse.
b) Relative entrapment:
No actual physical entrapment present.
Unable to extricate because of ptconditions eg # femur.
-
8/13/2019 Immobilization Extrication
9/75
Preparation & Approach
Training & knowledge.
Equipment regularly checked & in
working order. Know the equipment & their potential.
Know own limitation.
-
8/13/2019 Immobilization Extrication
10/75
Pain Relief
Moving injured limbs or extrication
casualties may produce pain.
Tractionrelief pain Drugs for pain killer eg. entonox,
ketamine, titrated intravenous
analgesia and local block.
-
8/13/2019 Immobilization Extrication
11/75
Methods of Immobilization
a) Cervical Immobilization
Manual immobilization
i. Approach from behindii. Approach from in front
iii. Approach from the side.
Cervical collars
Injury above clavicle
Unconscious
Cervical spine #
-
8/13/2019 Immobilization Extrication
12/75
Cervical Collar
Types of collar
a) Stiffneck.
b) Necloc.
Optimal position for cervical
immobilization.
Slight degree of flexion
2 cm of occiput elevation
-
8/13/2019 Immobilization Extrication
13/75
Cervical Collar
Manual in-line stabilization Sizing the collar
Head in neutral position
Distance between an
imaginary line drawn across
the top of shoulder and a
parallel line running
backwards from the tip of
chin.
Front piece is applied
under the chin.
Fasten Velcro strap.
-
8/13/2019 Immobilization Extrication
14/75
-
8/13/2019 Immobilization Extrication
15/75
-
8/13/2019 Immobilization Extrication
16/75
Limb Immobilization
Simple methods
Arm slings jacket, tie or scarves
Manual methods
support injured hands
Triangular bandage
simple pre-hospital care for upper limb
injuries.used as a high arm sling, broad arm sling
or collar & cuff sling.
-
8/13/2019 Immobilization Extrication
17/75
-
8/13/2019 Immobilization Extrication
18/75
-
8/13/2019 Immobilization Extrication
19/75
-
8/13/2019 Immobilization Extrication
20/75
-
8/13/2019 Immobilization Extrication
21/75
Limb Immobilization
Frac straps
Fasten one leg to another or immobilize
an arm to the side of chest.
Neighbour strapping
Injured fingers bound to fingers on either
side or lower limb bound to other limb.
-
8/13/2019 Immobilization Extrication
22/75
-
8/13/2019 Immobilization Extrication
23/75
Limb Immobilization
Inflatable splint
clear plastic, double walled tubes.
little contribution to # Mx.
use in Rx of soft tissue injury.
inflate by blowing only.
often crack & perish or tend to leak.
vulnerable to damage from sharp objects.
-
8/13/2019 Immobilization Extrication
24/75
-
8/13/2019 Immobilization Extrication
25/75
-
8/13/2019 Immobilization Extrication
26/75
-
8/13/2019 Immobilization Extrication
27/75
Limb Immobilization
Box splint (Loxley splint)Consists of three long padded pieces
of
board joined to form an open oblong
together with a foot support at one end.
Vacuum splint
Bag of polystyrene bead enclosed in
tough plastic.
provide rigid support to the body & verycomfortable.
Used to immobilize the limbs, the cervical
spine & other spinal injuries.
-
8/13/2019 Immobilization Extrication
28/75
Limb Immobilization
Vacuum splintVacuum splints conform to the exact shape of
the
injury site.
Providing excellent support without applying
unnecessary circumferential pressure.Eliminates the potential
for compartment
syndrome, unnecessary pressure sores, or
impairing circulation to the injured area.
Sensory function remains intact, yet the injuredarea is
immobilized properly to prevent further
injury and reduce pain.
-
8/13/2019 Immobilization Extrication
29/75
-
8/13/2019 Immobilization Extrication
30/75
Traction Splint
Hare traction splint.Indications
closed & open # femoral shaft.
closed & open # of the shaft of thetibia & fibula.
# around the knee (avoid traction)
Contraindications
dislocation of hip.
# dislocation of the knee
Ankle injuries.
-
8/13/2019 Immobilization Extrication
31/75
-
8/13/2019 Immobilization Extrication
32/75
Limb Immobilization
Functionsimmobilized # in a reduced position.
pain.
prevent further neurovascular damage.
severity shock
fat embolism.
Complication
damage neurovascular supply to the leg.
pressure sores pt with sensory loss.
limited space in ambulance.
-
8/13/2019 Immobilization Extrication
33/75
Application
Correct application requires 2 people.
Applied after extrication.
Method
1. Give appropriate analgesia.
2. Control external hemorrhage.
3. Remove footwear & assess MSC.
4. Select appropriate ankle hitch & adjust splint
length against normal leg. Open all straps &
placed correctly.
-
8/13/2019 Immobilization Extrication
34/75
Application
5. The hitch is placed under the ankle & thestraps are then
tightly folded across the frontof the ankle.
6. Manual traction is started with one hand. Theleg is supported
whilst the splint is put onposition. Role pt away from the splint
thenslide the splint under the pt. The top paddedring must fit
under the ischial tuberosity. Thept is then rolled back onto the
splint. Manualtraction must be maintained throughout
thisprocedure.
-
8/13/2019 Immobilization Extrication
35/75
Application
7. The top strap is then done up avoiding the
external genitalia.
8. The traction hook is then put through the D
rings & traction taken up, ensuring themanual traction is
not released before the
traction is tightened. Traction is applied until
the limb is comfortable. Repeat MCS
assessment.
9. Raised the footstand & velcro straps are
positioned & tightened.
-
8/13/2019 Immobilization Extrication
36/75
-
8/13/2019 Immobilization Extrication
37/75
-
8/13/2019 Immobilization Extrication
38/75
-
8/13/2019 Immobilization Extrication
39/75
-
8/13/2019 Immobilization Extrication
40/75
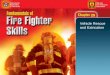
Pneumatic Antishock Garment (PASG)
Military Anti Shock Trousers (MAST)
An inflatable garments that surrounds the
leg & abdomen.
Indications
Hypovolaemic shock.
splinting of pelvic & lower limb #.
-
8/13/2019 Immobilization Extrication
41/75
Pneumatic Antishock Garment (PASG)
Contraindications
a) Absolute
Cardiac failure.
Pulmonary edema.Significant blunt chest injury.
ruptured diaphragm
advanced pregnancy.b) Relative
significant head injury.
uncontrolled bleeding above garment
-
8/13/2019 Immobilization Extrication
42/75
Pneumatic Antishock Garment (PASG)
Complications
Extreme hypotension.
Ischaemic compartment syndrome,
tissue damage & metabolic acidosis.Respiratory
embarrassment.
Exacerbation of;
Cardiac /thoracic vascular bleedingpulmonary edema
Congestive cardiac failure
-
8/13/2019 Immobilization Extrication
43/75
-
8/13/2019 Immobilization Extrication
44/75
-
8/13/2019 Immobilization Extrication
45/75
-
8/13/2019 Immobilization Extrication
46/75
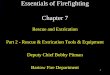
Extrication Devices
Kendrick extrication device (KED)
Russell extrication device (RED)
Provide support & stabilization to the
upper spine.Replaced short wooden board.
Flexible & can be positioned between the
casualty and the seat.
-
8/13/2019 Immobilization Extrication
47/75
Kendrick Extrication Device
-
8/13/2019 Immobilization Extrication
48/75
-
8/13/2019 Immobilization Extrication
49/75
-
8/13/2019 Immobilization Extrication
50/75
-
8/13/2019 Immobilization Extrication
51/75
-
8/13/2019 Immobilization Extrication
52/75
Long Spinal Board Immobilization
At least 3 rescuers ( preferably four)
Perform log roll.
Manually stabilize pts head & neck.
Apply rigid cervical collar.
Assess pulse, movement & circulation in all four
extremities.
Position the pthis arm straight down by his
side.
-
8/13/2019 Immobilization Extrication
53/75
Long Spinal Board Immobilization
Position the rescuersat the signal of the
rescuer at the head, the two at the side should
reach to the far side of pt.
1strescuer -Shoulder & hip.2ndrescuer - Thigh & lower
leg.
On signal, simultaneously roll the pt on to his
sidemove as a unit.
Position the spinal board under the pt.
-
8/13/2019 Immobilization Extrication
54/75
LONG SPINAL BOARD
-
8/13/2019 Immobilization Extrication
55/75
Log Roll
-
8/13/2019 Immobilization Extrication
56/75
Log Roll
-
8/13/2019 Immobilization Extrication
57/75
-
8/13/2019 Immobilization Extrication
58/75
-
8/13/2019 Immobilization Extrication
59/75
-
8/13/2019 Immobilization Extrication
60/75
-
8/13/2019 Immobilization Extrication
61/75
-
8/13/2019 Immobilization Extrication
62/75
-
8/13/2019 Immobilization Extrication
63/75
Pelvic Splint
The human pelvis comprises three pelvic bones which
combine to form a strong anatomic ring. Major trauma - injuries
may include pelvic fractures &
disrupt the integrity and stability of the pelvic ring.
lead to significant pelvic bleeding in the victim since
thearteries and major veins passing through the pelvic area
may easily be pinched, torn, or lacerated by thefractured
bones.
Pelvic bleeding is the major cause of death.
Immediate and important concern in early treatment ofthe victim
is stabilization of the pelvis, which reduces
bleeding, improves the comfort of the victim, andincreases the
victim's chances of survival.
The temporary measure most often undertaken tostabilize the
pelvis involves the use of a splint.
-
8/13/2019 Immobilization Extrication
64/75
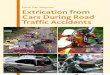
Noninvasive Pelvic Immobilization
Royal Hospital London Pelvic Splint
-
8/13/2019 Immobilization Extrication
65/75
Noninvasive Pelvic Immobilization
Dallas Pelvic Binder
-
8/13/2019 Immobilization Extrication
66/75
Invasive Pelvic Immobilization
Pelvic Clamp
-
8/13/2019 Immobilization Extrication
67/75
-
8/13/2019 Immobilization Extrication
68/75
Extrication Devices
Stretchers
Provide means of lifting pt onto a trolley
or trolley cot.
-
8/13/2019 Immobilization Extrication
69/75
-
8/13/2019 Immobilization Extrication
70/75
-
8/13/2019 Immobilization Extrication
71/75
-
8/13/2019 Immobilization Extrication
72/75
-
8/13/2019 Immobilization Extrication
73/75
Removing a Helmet
-
8/13/2019 Immobilization Extrication
74/75
Removing a Helmet
-
8/13/2019 Immobilization Extrication
75/75