Embed Size (px)
Citation preview

1
STUDIO DEI BIOMARCATORI DELLA SINOVITE
Prof. Franco Cozzi
L’ IMPEGNO POLMONARE NELLA SCLEROSI SISTEMICA
DIAGNOSI E TERAPIA
U.O.C. di Reumatologia – Dipartimento di Medicina DI MEDAzienda Ospedaliera – Università di Padova
Impegno polmonarenella SSc
ILD
PAH
Causes and risk factors for death in systemic scler osis –A study from the EUSTAR data base
(Tyndall AJ, Bannert B, Cozzi F, et al. Ann Rheum Dis 2010; 69: 1809-15)

2
Subsets della sclerosi sistemica(Le Roy EC et al. J Rheumatol 1988; 15: 202-5)
skinthickness
2 5 10 20disease duration (years)
earlyintermediate late
LIMITED SSc
pulmonary hypert.
DIFFUSE SScearly
intermediate
late
lung, heart, GI, kidney
GI

3
Strieter RM, et al. J Clin Invest 2004; 114:165-8.
QUADRO CLINICO DELLA ILD
- dispnea da sforzo progressiva
- tosse stizzosa
- crepitii alle basi polmonari
- segni di scompenso congestizio
4
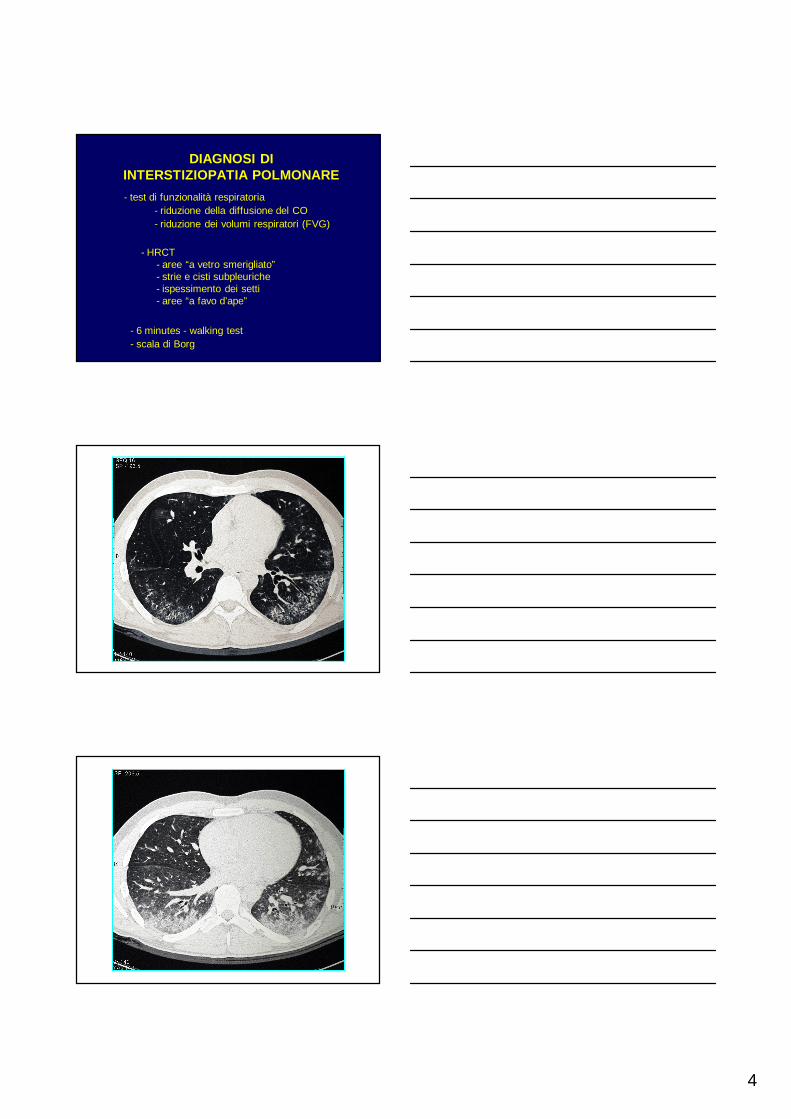
DIAGNOSI DI INTERSTIZIOPATIA POLMONARE
- test di funzionalità respiratoria- riduzione della diffusione del CO- riduzione dei volumi respiratori (FVG)
- 6 minutes - walking test- scala di Borg
- HRCT- aree “a vetro smerigliato”- strie e cisti subpleuriche- ispessimento dei setti- aree “a favo d’ape”
5
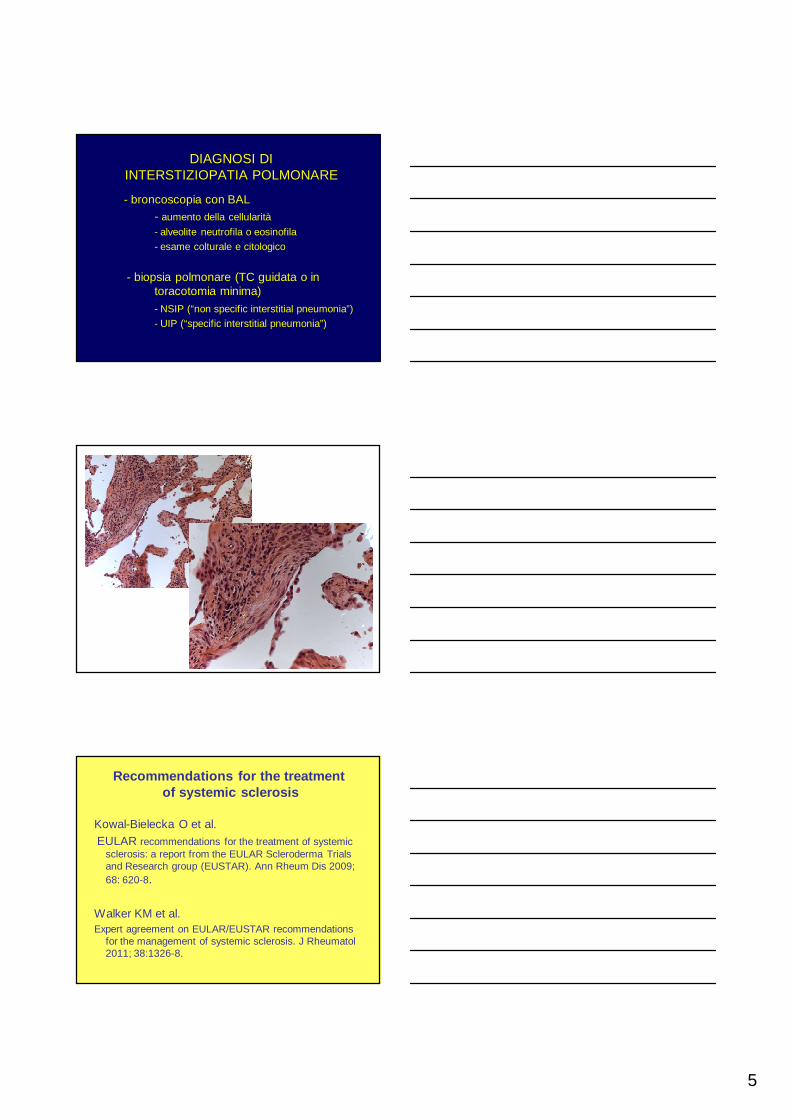
DIAGNOSI DI INTERSTIZIOPATIA POLMONARE
- broncoscopia con BAL - aumento della cellularità
- alveolite neutrofila o eosinofila- esame colturale e citologico
- biopsia polmonare (TC guidata o in toracotomia minima)
- NSIP (“non specific interstitial pneumonia”)- UIP (“specific interstitial pneumonia”)
Recommendations for the treatmentof systemic sclerosis
Kowal-Bielecka O et al.EULAR recommendations for the treatment of systemic
sclerosis: a report from the EULAR Scleroderma Trials and Research group (EUSTAR). Ann Rheum Dis 2009; 68: 620-8.
Walker KM et al.Expert agreement on EULAR/EUSTAR recommendations
for the management of systemic sclerosis. J Rheumatol 2011; 38:1326-8.
6
SSc - Interstitial lung disease (ILD)EULAR recommendations (2009)
In view of the results from two high-quality RCT and despite its known toxicity, cyclophosphamide should be considered for the treatment of SSc-ILD.
Tashkin DP et al. Cyclophosphamide versus placebo in sclerodermalung disease. N Engl J Med 2006; 354: 2655-66.
Hoyles RK et al. A multicenter, prospective, randomized, double-blind, placebo-controlled trial of corticosteroids and intravenouscyclophosphamide followed by oral azathioprine for thetreatment of pulmonary fibrosis in scleroderma. Arthritis Rheum2006; 54:3962-70.
Sullivan K et al. Progressive deteroration of patientswith scleroderma with pulmonary involvement: longterm outcomes from the Scleroderma Lung Study.Clin Exp Rheumatol 2014; 32:S17-18.
7
TERAPIA DELLA INTERSTIZIOPATIA POLMONARE - ALTRI FARMACI
MICOFENOLATO MOFETIL
RITUXIMAB
CORTICOSTEROIDI
Nithtyanova SI et al. Mycophenolate mofetil in diffuse
cutaneous systemic sclerosis -a retrospective analysis.
Rheumatology 2007; 46:442-5.
Le EN et al. Long-term experience of mycophenolate
mofetil for treatment of diffuse cutaneous systemic
sclerosis. Ann Rheum Dis 2011; 70:1104-7.
Mendoza FA et al. A prospective observational study of
mychophenolate mofetil treatment in progressive
diffuse systemic sclerosis of recent onset. J Rheumatol
2012; 39:1241-7.
Ann Rheum Dis 2014
8
• In patients with ILD FVC was stable after RTXtreatment (60,6±2,4 vs 61,3±4,1%; p=0,5), whilematched controls showed a decline in FVC atfollow-up � RTX prevent the further decline ofFVC.
• DLCO was significantly improved in patientstreated with RTX compared with baseline(41,1±2,8 vs 44,8±2,7%; p=0,03), but there wasno significative difference between RTX-treatedand matched-control patients.
Jordan S et al. 2014
Stem cell transplantation in SSc
Burt RK et al.Autologous non-myeloablative haemopoietic stem-cell
transplantation compared with pulse cyclophosphamideonce per month for systemic sclerosis (ASSIST): anopen-label, randomised phase 2 trial. Lancet 2011;378:498-506.
Van Laar JM et al.Autologous hematopoietic stem cell transplantation vs
intravenous pulse cyclophosphamide in diffusecutaneous systemic sclerosis: a randomized clinical trial.JAMA 2014; 311:2490-8.
9
“Findings of a series of 10 SSc patients with pulmonary arterial hypertension were reported at the University of Pittsburgh.
All patients had limited scleroderma and had either minimal or no pulmonary interstitial fibrosis”
Salerni R et al., Ann Intern Med 1977
PREVALENZA DELLA PAH NELLE CONNETTIVITI SISTEMICHE
Sclerosi sistemica 10 – 16%
Connettivite mista 5 – 15%
LES 3 – 5%Altre connettiviti < 1%
Denton CP et al., Rheum Dis Clin N Am 2003
10
QUADRO CLINICO DELLA PAH
- dispnea da sforzo- dolore toracico- sincope da sforzo
- segni di scompenso congestizio - aritmie- morte improvvisa
DIAGNOSI DI IPERTENSIONEARTERIOSA POLMONARE
- ecocardiogramma con doppler- stima della PAPs- dimensioni camere cardiache dx
- elettrocardiogramma
- test di funzionalità respiratoria- diffusione del CO (DLCO)
- cateterismo cardiaco- resistenze polmonari- pressione pre- e post-capillare- indice cardiaco- (test farmacologici di vasoreattività)
11
Pulmonary arterial hypertension (PAH)EULAR recommendations (2009)
Two high-quality RCT indicate that bosentan improves exercisecapacity, functional class and some haemodynamic measuresin PAH. Bosentan should be strongly considered to treatSSc-PAH.
One high-quality RCT indicates that sildenafil improvesexercise capacity, functional class and some haemodynamicmeasures in PAH. Sildenafil may be considered to treat SSc-PAH.
One high-quality RCT indicates that continuous intravenousepoprostenol improves exercise capacity, functional class andsome haemodynamic measures in PAH. Intravenousepoprostenol should be considered for treatment of patientswith severe SSc-PAH.
TERAPIA DELLA PAH Altri farmaci
Ambrisentan per os
Tadalafil per os
Iloprost inalatorio
Treprostinil sc e inalatorio
TERAPIE DI ASSOCIAZIONE
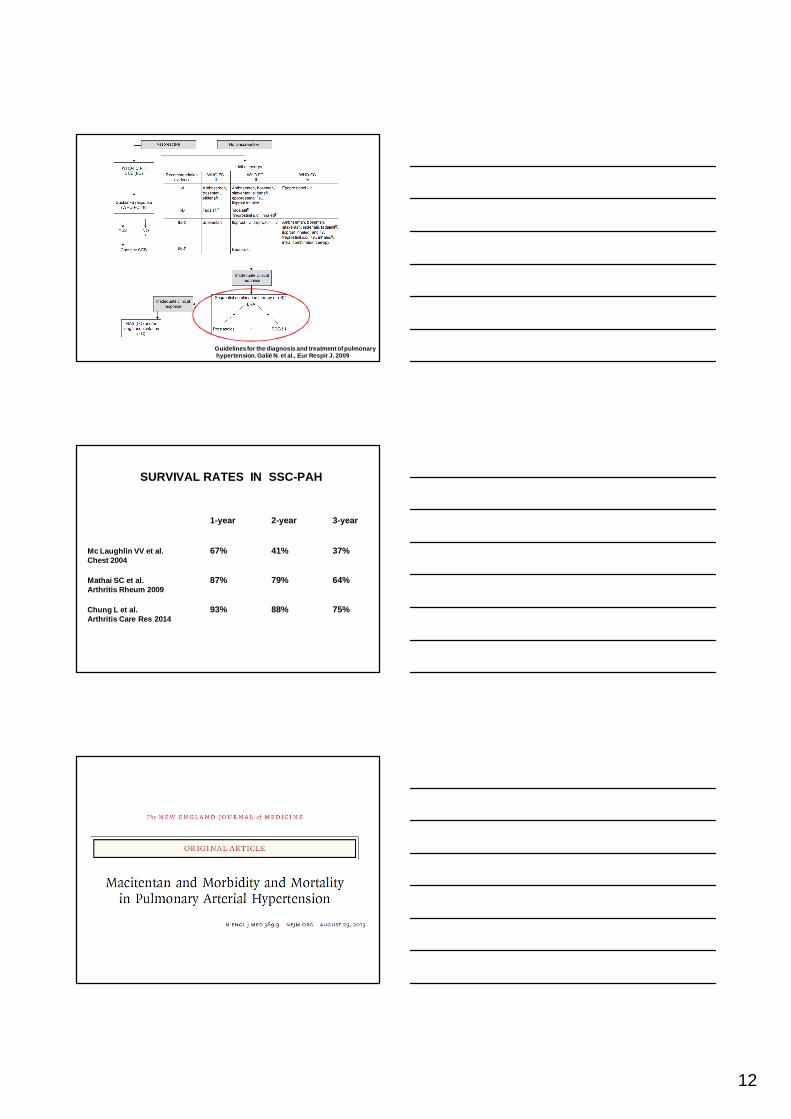
12
Guidelines for the diagnosis and treatment of pulmo naryhypertension. Galiè N. et al., Eur Respir J. 2009
SURVIVAL RATES IN SSC-PAH
1-year 2-year 3-year
Mc Laughlin VV et al. 67% 41% 37%Chest 2004
Mathai SC et al. 87% 79% 64%Arthritis Rheum 2009
Chung L et al. 93% 88% 75%Arthritis Care Res 2014
13
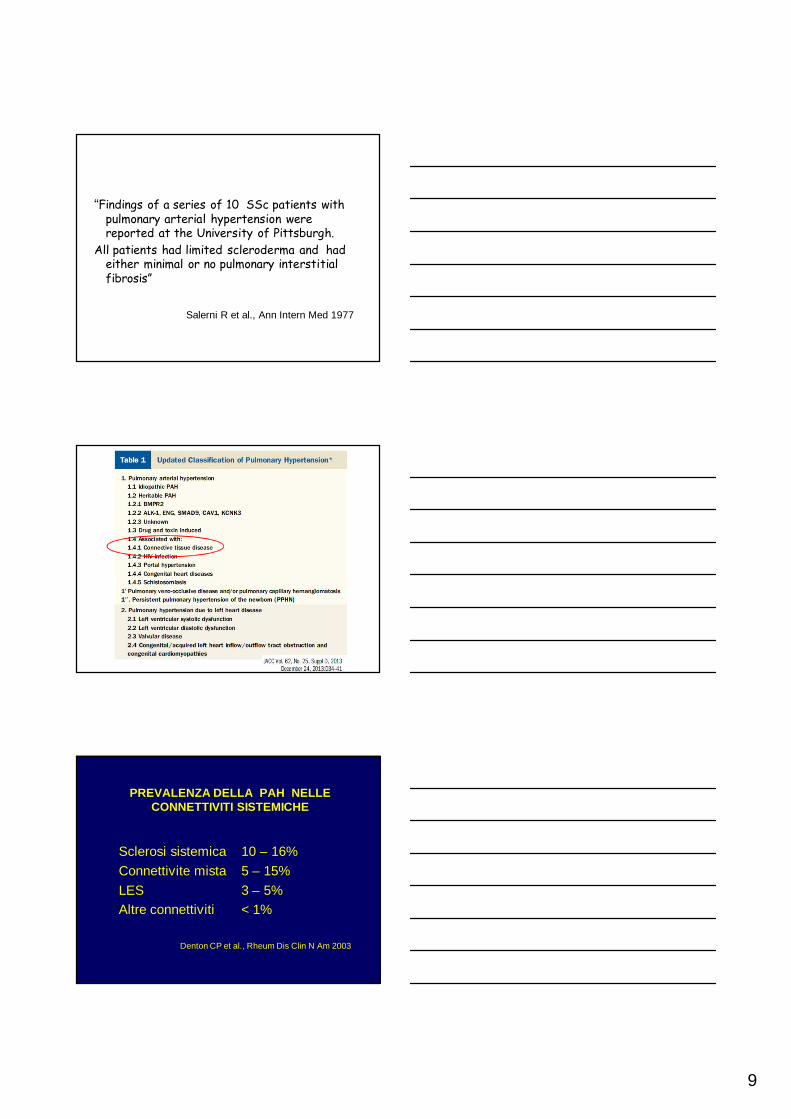
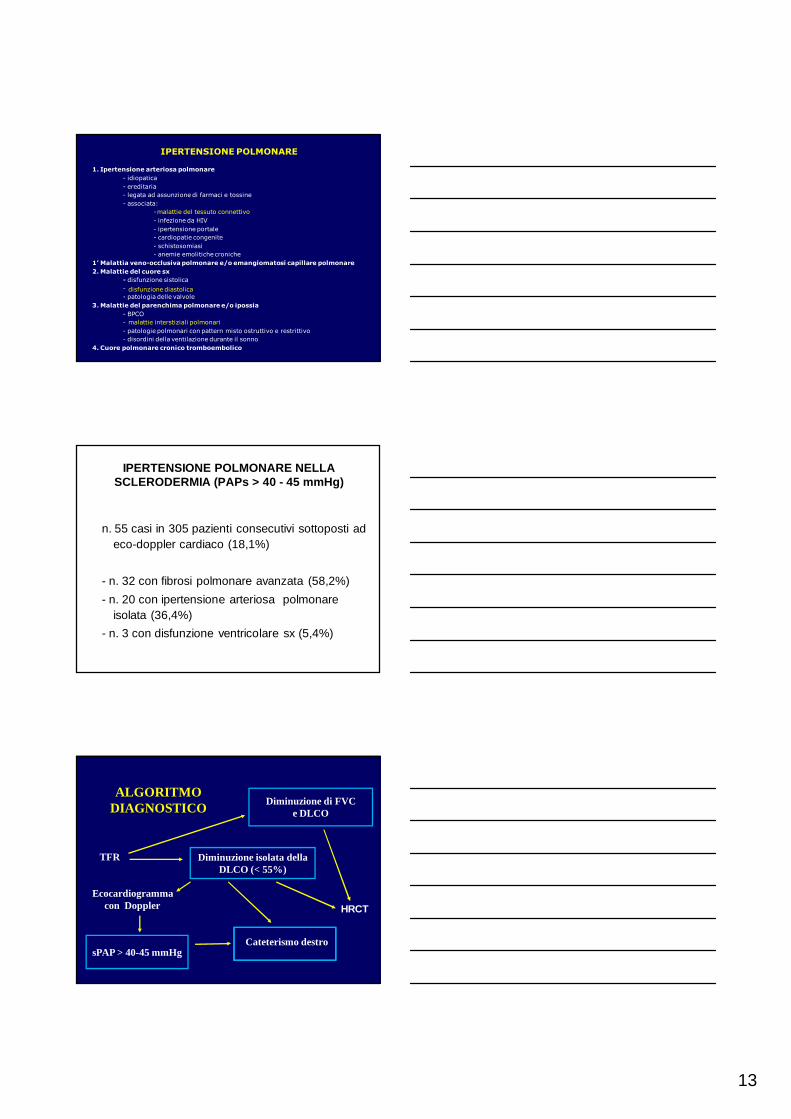
IPERTENSIONE POLMONARE
1. Ipertensione arteriosa polmonare
- idiopatica
- ereditaria
- legata ad assunzione di farmaci e tossine
- associata:
-
- infezione da HIV
- ipertensione portale
- cardiopatie congenite
- schistosomiasi
- anemie emolitiche croniche
1’ Malattia veno-occlusiva polmonare e/o emangiomatosi capillare polmonare
2. Malattie del cuore sx
- disfunzione sistolica
-
- patologia delle valvole
3. Malattie del parenchima polmonare e/o ipossia
- BPCO
-
- patologie polmonari con pattern misto ostruttivo e restrittivo
- disordini della ventilazione durante il sonno
4. Cuore polmonare cronico tromboembolico
malattie del tessuto connettivo
malattie interstiziali polmonari
disfunzione diastolica
IPERTENSIONE POLMONARE NELLA SCLERODERMIA (PAPs > 40 - 45 mmHg)
n. 55 casi in 305 pazienti consecutivi sottoposti ad eco-doppler cardiaco (18,1%)
- n. 32 con fibrosi polmonare avanzata (58,2%)
- n. 20 con ipertensione arteriosa polmonare isolata (36,4%)
- n. 3 con disfunzione ventricolare sx (5,4%)
ALGORITMODIAGNOSTICO
TFR
Ecocardiogramma con Doppler
Cateterismo destro
Diminuzione di FVCe DLCO
Diminuzione isolata della DLCO (< 55%)
sPAP > 40-45 mmHg
HRCT

14
TAKE HOME MESSAGE
• Nella sclerodermia il sintomo dispnea è moltofrequente, ma può essere dovuto a complicanzepolmonari diverse.
• Per diagnosticarle, i pazienti vanno sottopostiperiodicamente nel follow-up ai test difunzionalità respiratoria e all’ ecocardiogramma.
• La conferma diagnostica viene per la PAH dalcateterismo cardiaco, per la ILD dalla TCpolmonare ad alta risoluzione.
TAKE HOME MESSAGE
• La terapia della PAH nella sclerodermia ha fatto notevoli progressi negli ultimi anni grazie ai nuovi farmaci specifici.
• I risultati sono comunque inferiori a quelli ottenuti con gli stessi farmaci nella PAH idiopatica.
• La terapia della ILD nella sclerodermia con farmaci immunosoppressori rimane ancora poco soddisfacente e risulta efficace solo se intrapresa nella fase precoce alveolitica.





























