Embed Size (px)
Citation preview
IDIOPATHIC PULMONARY FIBROSIS
CLINICAL FEATURES AND DIAGNOSIS OF IPF
CLINICAL FEATURES OF IPF
Clinical symptoms
Unexplained chronic exertional dyspnea Commonly presents with non-productive (dry) cough
usually refractory to anti-cough agents Gastroesophageal acid reflux is present in close to 90% Symptoms such as weight loss, fever, and arthralgias
are unusual in IPF and should prompt an investigation for secondary causes of pulmonary fibrosis
IPF should be considered in all adult patients with unexplained chronic exertional dyspnea, and commonly presents with cough, bibasilar inspiratory crackles, and finger clubbing
Am J Respir Crit Care Med 2011; 183:788–824.
Clinical signs
Chest auscultation: dry, end-inspiratory, “Velcro” rales are heard (> 80% of patients; most prevalent in the lung bases and extend toward the upper lung zones with disease progression)
Clubbing : 25–50% of patients Late phases of the disease: Cyanosis, cor pulmonale,
accentuated pulmonic second sound, right ventricular heave, peripheral edema and other classic signs of right heart failure
Am J Respir Crit Care Med 2011; 183:788–824.
Clinical features :Radiological
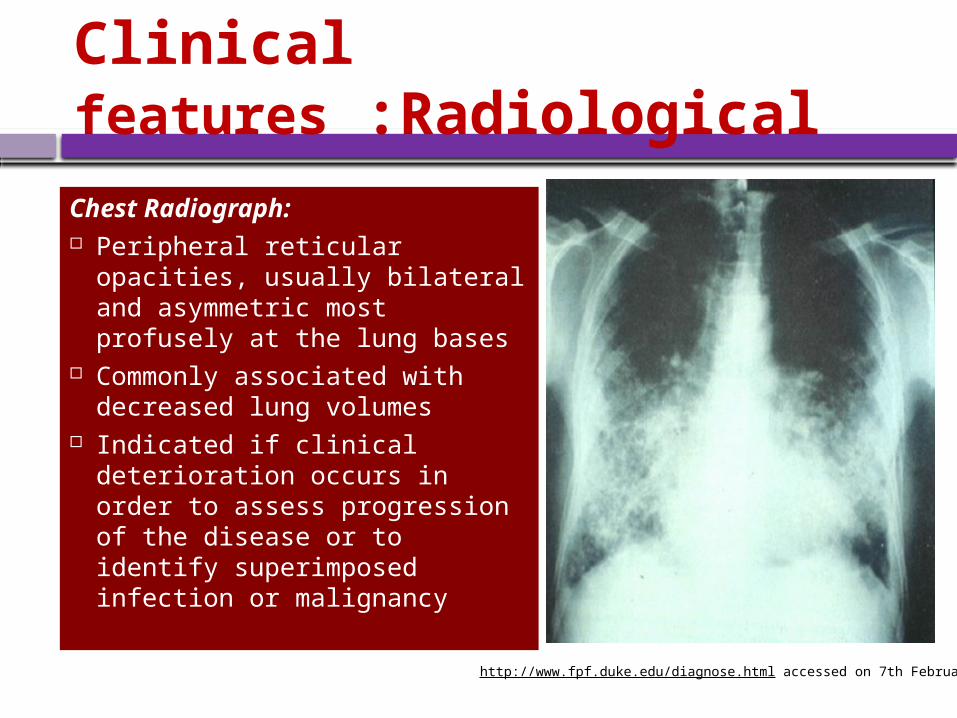
Chest Radiograph: Peripheral reticular opacities,
usually bilateral and asymmetric most profusely at the lung bases
Commonly associated with decreased lung volumes
Indicated if clinical deterioration occurs in order to assess progression of the disease or to identify superimposed infection or malignancy
http://www.fpf.duke.edu/diagnose.html accessed on 7th February 2012
Clinical features :Radiological HRCT Pattern: Essential component of the
diagnostic pathway in IPF
UIP pattern : Patchy, predominantly peripheral, sub-pleural, bibasal reticular abnormalities as well as architectural distortion and honeycombing, characteristically basal and peripheral in distribution, though often patchy
•Honeycombing is common, critical for making a definite diagnosis; diameters of usually 3–10 mm, but occasionally as large as 2.5 cm•Presence of coexistent pleural abnormalities (e.g., pleural plaques, calcifications, significant pleural effusion) suggests an alternative etiology •Mild mediastinal lymph node enlargement can be seen
The positive predictive value of a HRCT diagnosis of UIP is 90–100%
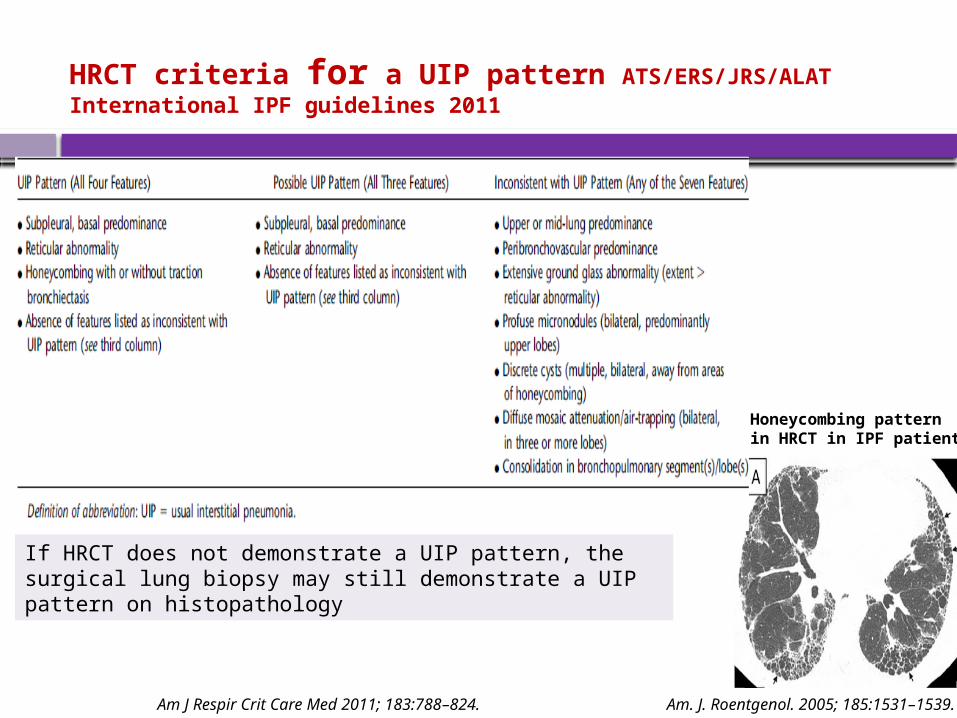
HRCT criteria for a UIP pattern ATS/ERS/JRS/ALAT International IPF guidelines 2011
Honeycombing pattern in HRCT in IPF patients
If HRCT does not demonstrate a UIP pattern, the surgical lung biopsy may still demonstrate a UIP pattern on histopathology
Am J Respir Crit Care Med 2011; 183:788–824. Am. J. Roentgenol. 2005; 185:1531–1539.
Clinical features of IPF Pathological :Surgical lung biopsy
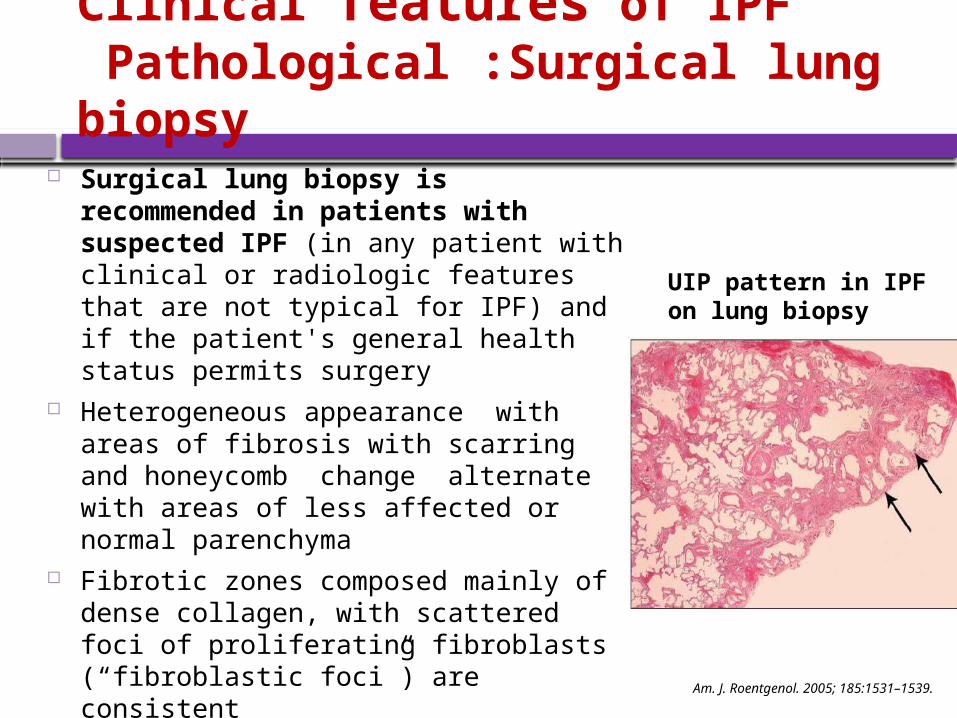
Surgical lung biopsy is recommended in patients with suspected IPF (in any patient with clinical or radiologic features that are not typical for IPF) and if the patient's general health status permits surgery
Heterogeneous appearance with areas of fibrosis with scarring and honeycomb change alternate with areas of less affected or normal parenchyma
Fibrotic zones composed mainly of dense collagen, with scattered foci of proliferating fibroblasts (“fibroblastic foci”) are consistent
Transbronchial biopsy approach is not recommended as the sensitivity, specificity , number and site from where they should be obtained are unknown
UIP pattern in IPF on lung biopsy
Am. J. Roentgenol. 2005; 185:1531–1539.
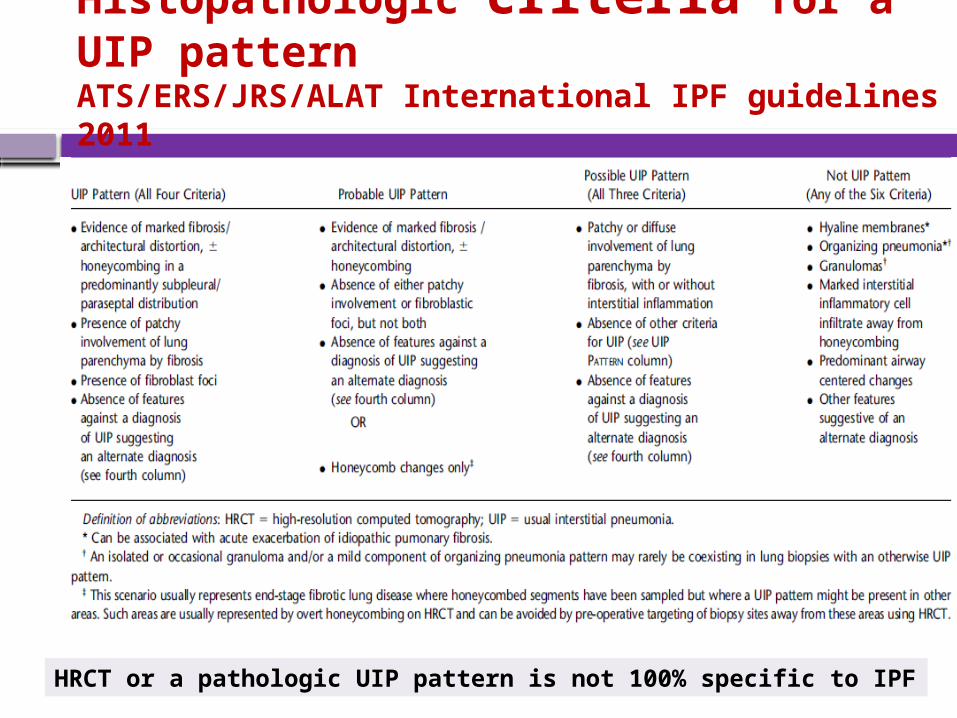
Histopathologic criteria for a UIP patternATS/ERS/JRS/ALAT International IPF guidelines 2011
HRCT or a pathologic UIP pattern is not 100% specific to IPF
Other tests : Pulmonary function tests
Patients with IPF typically reveal evidence of Restrictive impairment Reduced vital capacity [VC] and TLC) by body plethysmography Reduced lung volumes (FVC, TLC,FRC) Normal or increased FEV1 /FVC ratio Pressure–volume studies often yield a curve that is shifted
downward and to the right, consistent with stiff, non-compliant lungs Impaired gas exchange Decreased DLco, PaO2, Desaturation on exercise oximetry,
Increased A-a gradient
Normal resting PFTs do not exclude IPF
Am J Respir Crit Care Med. 2000;161:646-664.Am J Respir Crit Care Med 2011; 183:788–824.
Other tests : Bronchoalveolar Lavage (BAL)
Most important use of BAL is in the exclusion of chronic hypersensitivity pneumonitis : prominent lymphocytosis (> 40%) is seen
In IPF patients, an increase in (levels >5%) neutrophils in 70–90% of patients, eosinophils in 40–60% of patients, and an additional increase in lymphocytes is noted in 10–20% of patients.
Utility of BAL in staging, or to monitor, IPF, is limited and, hence, is not routinely recommended
Am J Respir Crit Care Med 2011; 183:788–824.
Other tests : Serological Testing
Serologic evaluation should be performed even in the absence of signs or symptoms of connective tissue disease, and should include:
rheumatoid factor, anti-cyclic citrullinated peptide, and anti-nuclear antibody titer and pattern
Patients with a mildly positive antinuclear antibody titer and/or rheumatoid factor level without any other clinical features of connective tissue should be screened for signs and symptoms of connective tissues disease (e.g., arthritis, Raynaud’s phenomenon, skin changes, abnormal esophageal motility)
Am J Respir Crit Care Med 2011; 183:788–824.
APPROACH TO THE DIAGNOSIS OF IPF
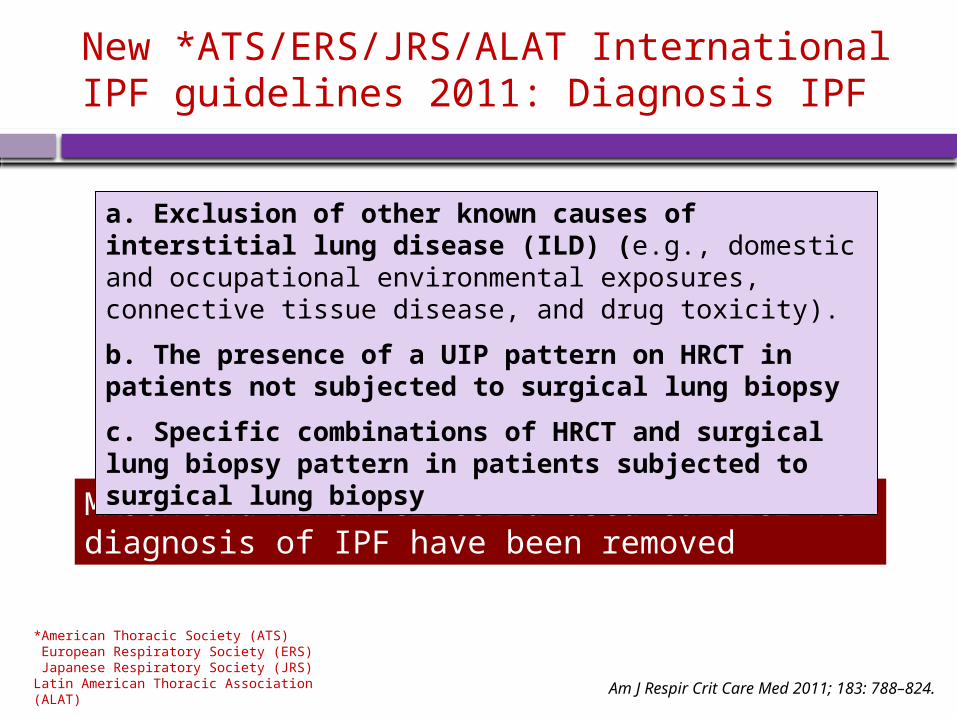
New *ATS/ERS/JRS/ALAT International IPF guidelines 2011: Diagnosis IPF
MAJOR and MINOR criteria used earlier for diagnosis of IPF have been removed
Am J Respir Crit Care Med 2011; 183: 788–824.
a. Exclusion of other known causes of interstitial lung disease (ILD) (e.g., domestic and occupational environmental exposures, connective tissue disease, and drug toxicity).
b. The presence of a UIP pattern on HRCT in patients not subjected to surgical lung biopsy
c. Specific combinations of HRCT and surgical lung biopsy pattern in patients subjected to surgical lung biopsy
*American Thoracic Society (ATS) European Respiratory Society (ERS) Japanese Respiratory Society (JRS)Latin American Thoracic Association (ALAT)
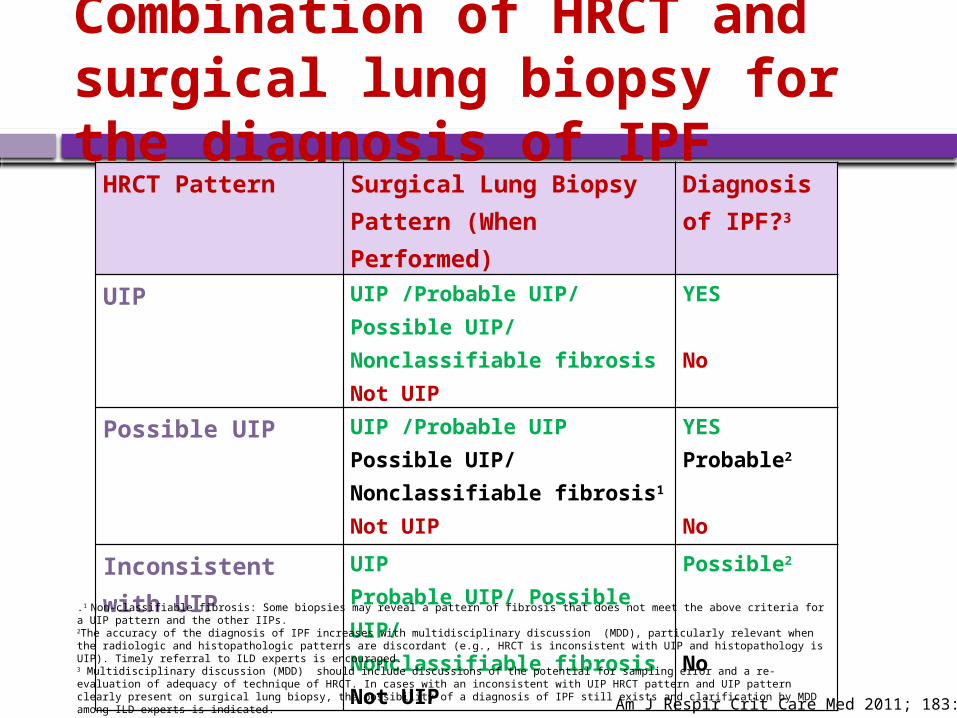
Combination of HRCT and surgical lung biopsy for the diagnosis of IPF
HRCT Pattern Surgical Lung Biopsy Pattern (When Performed)
Diagnosis of IPF?3
UIP UIP /Probable UIP/ Possible UIP/ Nonclassifiable fibrosisNot UIP
YES
No
Possible UIP UIP /Probable UIPPossible UIP/ Nonclassifiable fibrosis1
Not UIP
YESProbable2
No
Inconsistent with UIP
UIP Probable UIP/ Possible UIP/Nonclassifiable fibrosisNot UIP
Possible2
No
Am J Respir Crit Care Med 2011; 183: 788–824
.1 Non-classifiable fibrosis: Some biopsies may reveal a pattern of fibrosis that does not meet the above criteria for a UIP pattern and the other IIPs.2The accuracy of the diagnosis of IPF increases with multidisciplinary discussion (MDD), particularly relevant when the radiologic and histopathologic patterns are discordant (e.g., HRCT is inconsistent with UIP and histopathology is UIP). Timely referral to ILD experts is encouraged.3 Multidisciplinary discussion (MDD) should include discussions of the potential for sampling error and a re-evaluation of adequacy of technique of HRCT. In cases with an inconsistent with UIP HRCT pattern and UIP pattern clearly present on surgical lung biopsy, the possibility of a diagnosis of IPF still exists and clarification by MDD among ILD experts is indicated.
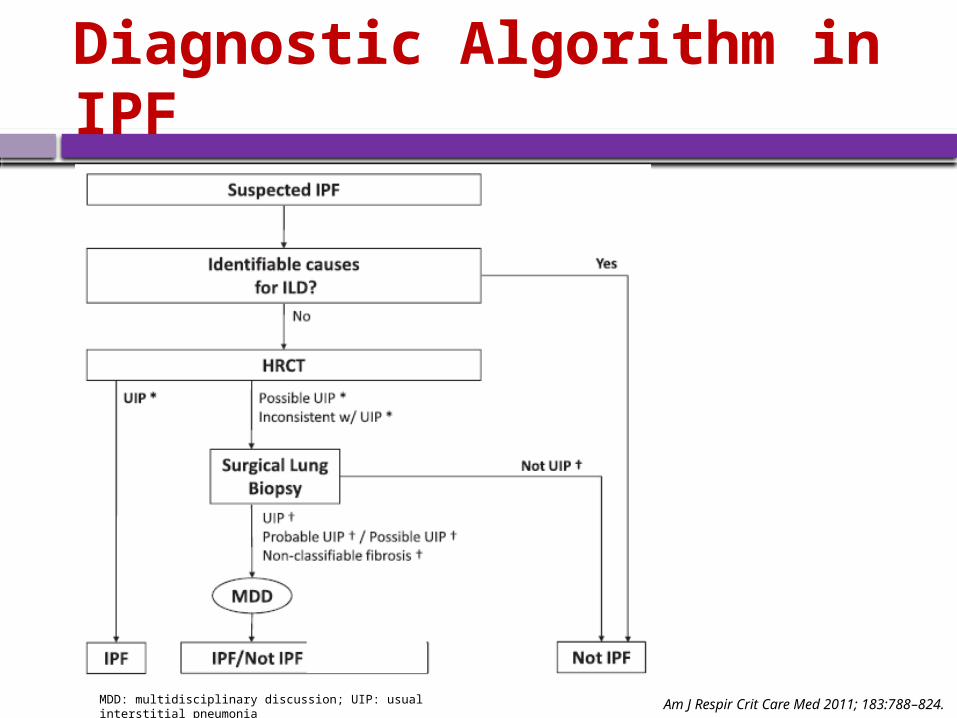
Diagnostic Algorithm in IPF
MDD: multidisciplinary discussion; UIP: usual interstitial pneumonia Am J Respir Crit Care Med 2011; 183:788–824.
Differential Diagnosis
Other idiopathic interstitial pneumonias (NSIP, DIP, RBILD, COP, AIP)
Connective tissue diseases ( scleroderma, rheumatoid arthritis, polymyositis/ dermatomyositis)
Identifying previous exposures (asbestos, silicon, birds, metal, and wood dusts, etc)- asbestosis, hypersensitivity pneumonitis
Sarcoidosis
Am J Respir Crit Care Med. 2000;161:646-664.
THE END





























