Embed Size (px)
Citation preview

Idiopathic Intracranial Hypertension –Investigation and Treatment
Dr CP WhiteConsultant Paediatric Neurologist
Abertawe Bro Morgannwg UHBJanuary 2011

Definition
“ a condition of increased intracranial pressure without clinical, laboratory or radiological evidence of intracranial pathology”.
� Unknown pathogenesis � Increased CSF secretion� Increased venous sinus pressure�Reduced CSF absorption
Updated Modified Dandy Criteria
1. If symptoms are present, they may only reflect those of generalised increased intracranial pressure or papilloedema.
2. If signs are present, they may only reflect those of generalised increased intracranial pressure or papilloedema.
3. Elevated opening pressure (in lateral decubitus position)
4. Normal CSF composition 5. Normal CT/MRI findings without evidence of
hydrocephalus, mass, structural or vascular lesion6. No other explanation for the raised intracranial
pressure

Current Controversies in IIH
�What (level of) pressure is high?�Which associations mean that IIH is no
longer idiopathic?�Should paediatric IIH only include
prepubertal children? (Rangwala and Lui 2007)

Controversies
�What (level of) pressure is high?�>20 cm H2O in the non-obese
�>25 cm H2O in the obese
�>25 cm H2O in all adults
�> 18cm H2O in < 8yr old children with papilloedema (Rangwala and Lui 2007)
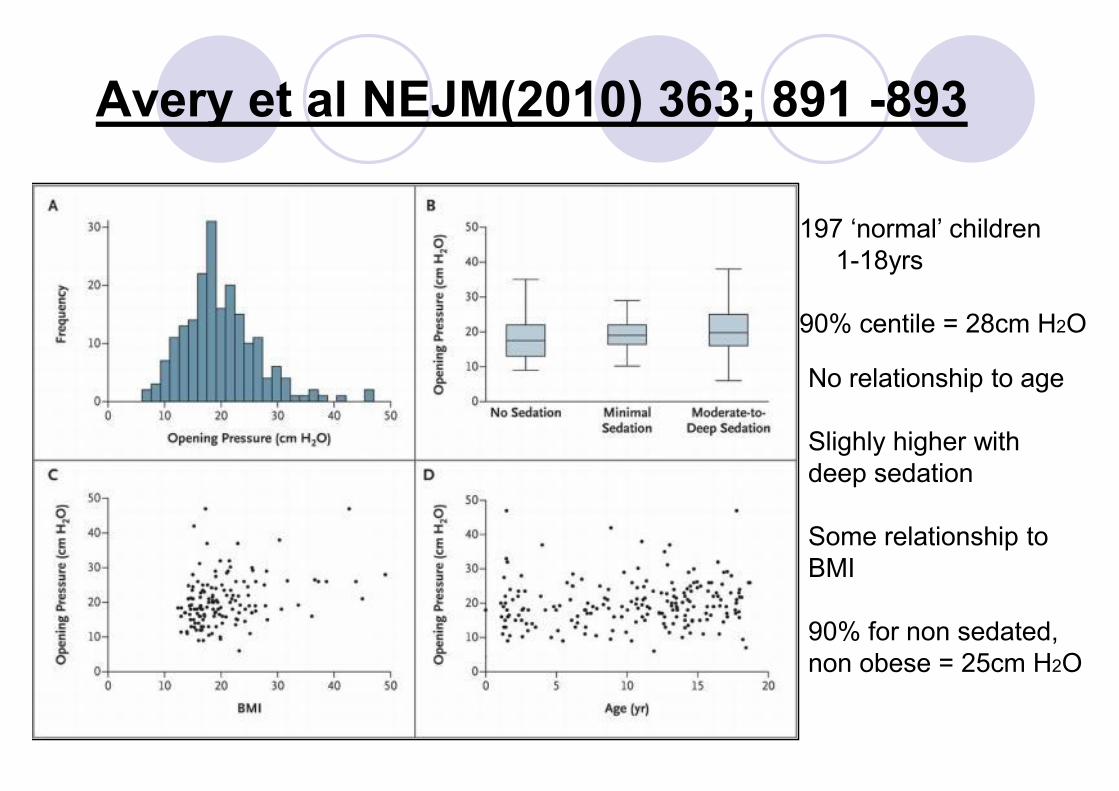
Avery et al NEJM(2010) 363; 891 -893
197 ‘normal’ children1-18yrs
90% centile = 28cm H2O
No relationship to age
Slighly higher with deep sedation
Some relationship to BMI
90% for non sedated, non obese = 25cm H2O

Cause or Association?� Obesity/rapid weight gain� Iron deficiency and other
anaemias� Lupus � Obstructive sleep apnoea � Renal impairment� Various infections � Malnutrition and re-
feeding� Menarche � Endocrine
�Thyroid disease�Adrenal disease�Parathyroid disease�Hypocalcaemia
� Prescription medications �Tetracyclines�Nitrofurantoin�Nalidixic acid�Oral contraceptives�Growth hormone�Vitamin A�Steroids�Desmopressin�Retinoic acid
Excludes IH associated with venous sinus thrombosis
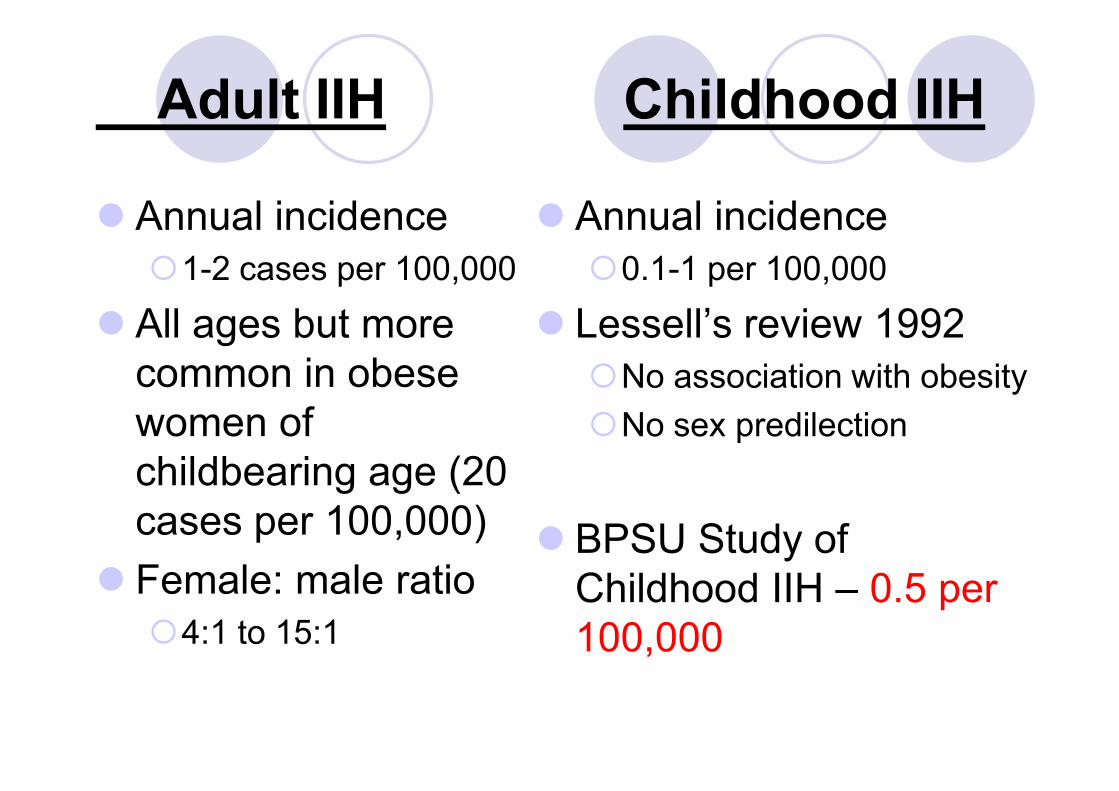
Adult IIH Childhood IIH
� Annual incidence �1-2 cases per 100,000
� All ages but more common in obese women of childbearing age (20 cases per 100,000)
� Female: male ratio �4:1 to 15:1
� Annual incidence �0.1-1 per 100,000
� Lessell’s review 1992�No association with obesity�No sex predilection
� BPSU Study of Childhood IIH – 0.5 per 100,000
BPSU Study of Childhood IIH
� Prospective national survey of newly diagnosed IIH cases aged 1-16 years.
� Via monthly notification to British Paediatric Surveillance Unit (BPSU) by all reporting paediatricians in the UK & Ireland.
� Surveillance period: � July 2007 to July 2009
� Aims to determine:� Contemporary national incidence of childhood IIH� Spectrum of clinical presentation� Incidence of clinical associations, especially obesity� Current clinical management� Clinical course of headache and visual outcome at 1 year

Changing DemographyDistribution of age and sex
0123456789
101112
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Age in years
No.
of I
IH c
ases
M F
BPSU Study of Childhood IIH - Jul 2007 to Dec 2008 88 children – 66% girls
3-9y: N = 18 (9M:9F) vs 10-16y: N = 70 (21M:49F (70%F))Median age at diagnosis: 12 years in both female and male

Changing DemographyDistribution of age groups, gender and obesity
0
5
10
15
20
25
30
35
40
45
No. of
IIH ca
ses
Non-obese 3 5 5 12
Obese 4 1 13 28
3-9 years Males
3-9 years Females
10-16 years Males
10-16 years Females
BPSU Study of Childhood IIH - Jul 2007 to Dec 2008Obese (BMI ≥ 98th centile): 46/71 (65%)
Age 3-9y: 5/13 (38%, 4M:1F) Age 10-16y: 41/58 (71%, 13M:28F)
UK incidence of childhood obesity -13.7% (2003)

Presenting Symptoms
� Common�Headache - 86%�Nausea/vomiting�Transient Visual
obscurations�Blurred vision�Diplopia�Photophobia�?visual loss
� Less Common�Pulsatile tinnitus�Neck stiffness�Back/shoulder pain� Irritability�Lethargy� Increasing head size�Asymptomatic
Presenting Signs
�Papilloedema – 89%�VIth nerve palsy – 9 - 48%� IVth nerve palsy - rare� IIIrd nerve palsy - rare�Visual deficit – 25% (up to 91%)

Early Investigations� Neuroimaging
�MRI preferable �MRV
� Lumbar puncture �diagnostic�therapeutic
� FBC� ESR� U+Es� Bone profile � TFTs

Neuroimaging
� Excluding other causes of RICP
� Non specific abnormalities

(Partially) empty sella
� Adults with IIH�70-94%
� Lim et al 2010 �26% of children (cf 5%
of normals)

Flattening of the posterior globe
� Adults with IIH - 80%
� Lim et al 2010 �61% of children (cf 40%
of normals)

Prominence of CSF signal in peri-optic sheath
� Adults with IIH - 45%
� Lim et al 2010 �65% of children (cf 35%
of normals)

Tortuosity of the optic disc sheath
� Adults with IIH - 40%
� Lim et al 2010 �30% of children (cf 5%
of normals)

MR Venography

©2004AAN Enterprises, Inc. 2
Lateral venous sinus stenoses

Lumbar puncture
� Diagnostic�Pressure�Normal composition
� Therapeutic
� Practicalities�Ambience�Position
� Anaesthesia�Agent�1kPa increase in end –
tidal pCO2 increases CSF pressure by 3.5-12cm H2O

Goals of Management
�Relief of symptoms�Preservation of vision
�Not to keep the pressure down
�Concept of the “normal” pressure for person
Management
�Multidisciplinary�Correct initial diagnosis�Of underlying predisposition� ‘Therapeutic’ lumbar puncture�Medical therapy �Surgical intervention
Treatment
�Underlying predispositions�Weight loss�Drug withdrawal�Management of associated conditions�Could this be enough?
�Therapeutic Lumbar puncture�CSF removal to lower closing pressure to 15cm water�10-20% resolve after initial LP (BPSU -12%)
First Line Medical Treatment
� Wait 48hrs after LP
� Acetazolamide - strong carbonic anhydrase inhibitor- inhibits CSF production- mild diuretic
� Children �25mg/kg/day �Twice daily�Increase by 25mg/kg/day�Maximum - 100mg/kg/day or 2g
� Adolescents�Start at 1g/day� Increase by
250mg/day�Maximum 4g/day

Acetazolamide
�Bicarbonate therapy � if symptomatic�1-2mmol/kg/day
�Monitoring�Electrolytes - ?frequency�renal ultrasound after 6m
�Wean after 2 months headache free�Efficacy – 47- 67%
Second Line Treatment
�Topiramate� Weak carbonic anhydrase inhibitor�1.5-3mg/kg/day, max. 200mg/day�Increase by 25mg/kg/week
�Weight loss�Treatment of chronic headache syndromes
�Adult studies only
Other Medical Treatment� Furosemide
�Depletion of total body extracellualr fluid �Weak carbonic anhydrase inhibitor
� Dose�1-2mg/kg/day �Max. 2mg/kg tds�Side effects�Monitoring
�Electrolytes - ?frequency�Additional potassium
� Second line or adjuvant?� ‘Success’ rates?

Other Medical Treatment� Steroids
� ?mechanism of action
� Dose � Prednisolone 2mg/kg/day for 2 weeks � wean over 2 weeks� Beware rapid withdrawal and weight gain
� Second line or adjuvant?� No studies of efficacy� Use limited by side effects� Steroids

Other Medical Treatment
�Serial LPs�Other diuretics �Zonisamide�Octretide
Fulminant IIH
� Definition�Acute onset of symptoms and
signs of IIH (<4wks)�Rapid visual loss�Normal imaging
� Rare� ?commoner in secondary cases� Invariably obese women� Mean opening pressure=54.1cm� Monitor vision daily� 50% persisting visual loss
� Treatment�Acetazolamide�Repeat LPs�Steroids
� IV methylprednisolone
�Surgery�ONSF�Shunt proceedure
Headache management
� Reduction of raised pressure
� Symptomatic headache relief�Conventional analgesics
� 68% adults have other headaches�Migraine�Tension headache �Analgesia overuse� Low pressure headache�Often recognised as different from high pressure headache

Surgical Treatment
� Indications�Severe visual loss at
onset�Progressive visual loss
despite therapy�Refractory symptoms
� Frequency�5-20%�BPSU Study
�5% LP Shunt�1 ONSF

Surgical Treatment
�CSF Diversion procedures�Lumboperitoneal shunting (LPS)�Ventriculoperitoneal shunting (VPS)
�Optic Nerve Sheath Fenestration (ONSF)
�Dural Venous Sinus Stenting
Surgical treatment
� LPS�Requires more
revisions (RR 2.5)� Increased risk of
obstruction (RR 3.5)�Low pressure headache
(difficult to treat may be avoided by programmable shunt)
�No need for craniotomy
� VPS�Requires less revision�Lower risk of
obstruction�Low pressure headache
controlled by programmable shunt
�Requires craniotomy
Surgical treatment
� LPS� Infection�CSF leak�Abdominal pain�Radicular pain� Iatrogenic chiari
malformation�Treatment failure (30-
50%)
� VPS� Infection�Abdominal pain�Risk of stroke,
haemorrhage, infection etc
�Treatment failure (up to 30%)
Optic nerve sheath fenestration
�Variably available�Limited duration�Protects vision�Relieves headache in 2/3

Outcome
� Remission in 1wk to 6m� ?worse in pubertal
children than others� ?related to degree of
papilloedema� Worse in those without
headache� Recurrence rate
� 6-22%�Early and late
� Permanent loss of acuity – 0-10%
� Permanent loss of visual fields <17%

Long Term Follow up and Monitoring
�No consensus/guidelines
�What to monitor and how?�Headache �Visual acuity and fields�Optic nerve assessment

Follow up/ Monitoring
� If normal visual acuity and responding to treatment� Initial frequency of follow up will depend on visual
parameters and symptoms�3/12 follow up neurology/ophthalmology when stable�How long to follow up?
� If no response �Weekly monitoring neurology/ophthalmology�Plan for sudden deterioration in vision

Summary
� Correct diagnosis�Confirm papilloedema �Correct LP technique�Exclude venous sinus thrombosis
� Good imaging� Good communication
�Agree local protocol for follow up� Beware loss of acuity +/field loss� Symptoms may not be a good guide