Embed Size (px)
Citation preview

Original Research
Identifying Lesion Growth With MR Imaging inAcute Ischemic Stroke
Michael S. Bristow, MD,1* Brett W. Poulin, MD,2 Jessica E. Simon, FRCPC,3
Michael D. Hill, FRCPC,4–7 Jayme C. Kosior, BSc,7–9 Shelagh B. Coutts, FRCPC,4,7
Richard Frayne, PhD,1,4,7–9 J. Ross Mitchell, PhD,1,4,7–9 andAndrew M. Demchuk, FRCPC4,7
Purpose: To determine whether different MR diffusion- andperfusion-weighted imaging (DWI and PWI) parameters areimportant in distinguishing lesion growth from the acutelesion and from oligemia.
Materials and Methods: MR DWI and PWI were acquiredfrom thirteen patients. We defined three regions: (i) LESION- intersection of acute and final lesions, (ii) GROWTH -portion of final lesion not part of acute lesion, and (iii)OLIGEMIA - region of perfusion abnormality not part ofeither the acute or final lesions. We used logistic regressionmodeling to distinguish GROWTH from LESION and fromOLIGEMIA on a voxel-wise basis using DWI- and PWI-based parameters. Final models were selected based on theWald statistic and validated by cross-validation using themean (� standard deviation) area under the curve (AUC)from receiver operating characteristic analysis.
Results: The final model for differentiating GROWTH fromLESION included DWI, the apparent diffusion coefficient(ADC), cerebral blood flow (CBF) and tissue type (AUC �0.939 � 0.028). The final model for differentiatingGROWTH from OLIGEMIA included DWI, ADC, CBF, andtime-to-peak (AUC � 0.793 � 0.106).
Conclusion: Different MR parameters are important in dif-ferentiating lesion growth from acute lesion and from olige-mia in acute ischemic stroke.
Key Words: diffusion weighted MRI; perfusion weightedMRI; acute stroke; logistic regressionJ. Magn. Reson. Imaging 2008;28:837–846.© 2008 Wiley-Liss, Inc.
MR IMAGING can be used to predict tissue outcome inacute ischemic stroke (1). The clinical applications areimportant: MR imaging could better select patients forthrombolytic therapy (2) by targeting treatment at pa-tients that present with appreciable risk of lesiongrowth without recanalization and in whom the poten-tial risks of thrombolytic therapy are outweighed by thepotential benefits (3–6). MR imaging could also test theability of new therapies such as mechanical clot disrup-tion (7) or neuroprotectants (8,9) to alter predicted out-come.
It is recognized that diffusion-weighted imaging (DWI)can be used to identify cytotoxic edema and perfusion-weighted imaging (PWI) measures can indicate thedepth and extent of ischemia (3,6,10,11). Multivariable,voxel-wise predictions of tissue at risk of infarction onimages from human subjects have focused on differen-tiating final infarct from penumbra that is ultimatelysalvaged (1,12,13). Analyses of image-defined regions-of-interest (14–16) have assessed the different ischemiccompartments of the acute lesion, lesion growth, andoligemia separately, however, because these compart-ments reflect different stages in the spectrum of isch-emia and have different physiological characteristics(3,6,10,17,18). Differentiating lesion growth from boththe acute lesion and from oligemia is important forassisting decisions regarding clinical management be-cause it is the lesion growth that best corresponds to
1Department of Radiology, University of Calgary, Calgary, Alberta, Can-ada.2Department of Family Medicine, University of Calgary, Calgary, Al-berta, Canada.3Department of Palliative Care, University of Calgary, Calgary, Alberta,Canada.4Department of Clinical Neurosciences, University of Calgary, Calgary,Alberta, Canada.5Department of Community Health Sciences, University of Calgary,Calgary, Alberta, Canada.6Department of Medicine, University of Calgary, Calgary, Alberta, Can-ada.7Hotchkiss Brain Institute, Calgary, Alberta, Canada.8Department of Electrical and Computer Engineering, Schulich Schoolof Engineering, University of Calgary, Calgary, Alberta, Canada.9Seaman Family MR Research Centre, Foothills Medical Centre, Cal-gary Health Region, Calgary, Alberta, Canada.Contract grant sponsor: Alberta Foundation for Health Research; Con-tract grant sponsor: Alberta Heritage Foundation for Medical Research;Contract grant sponsor: Canada Foundation for Innovation; Contractgrant sponsor: Canadian Institutes of Health Research; Contract grantsponsor: Heart and Stroke Foundation of Canada; Contract grant spon-sor: Informatics Circle of Research Excellence; Contract grant sponsor:MS Society of Canada; Contract grant sponsor: Natural Sciences andEngineering Research Council of Canada.*Address reprint requests to: M.B., Diagnostic Imaging, Foothills Med-ical Centre, 1403-29 Street NW, Calgary, AB T2N 2T9, Canada. E-mail:[email protected] October 1, 2007; Accepted June 11, 2008.DOI 10.1002/jmri.21507Published online in Wiley InterScience (www.interscience.wiley.com).
JOURNAL OF MAGNETIC RESONANCE IMAGING 28:837–846 (2008)
© 2008 Wiley-Liss, Inc. 837

the threatened physiologic penumbra that is the pri-mary target of thrombolytic therapy (3,6,18). The nov-elty of this study as compared to previous similar workby Wu et al (1,12) and Rose et al (13) is the separationof the final infarct into the acute lesion and lesiongrowth as well as the testing of interactions in the mod-eling process.
The purpose of this study is to build two models todifferentiate (i) lesion growth from the acute lesion and(ii) lesion growth from oligemia using voxel-wise multi-variable logistic regression analysis of MR-derived DWIand PWI parameters. Our hypothesis is that differentoptimal models will differentiate lesion growth from theacute lesion and from oligemia. Given that gray andwhite matter (GM and WM) are susceptible to infarctionat different levels of diffusion and perfusion (19–21)and because WM is more resistant to ischemia than GM(22), we also investigate the role of tissue type whenmodeling tissue outcome. Because a relationship be-tween ADC and CBF has previously been reported onvoxel-wise analysis (23,24), the interaction betweenthese parameters is also assessed.
MATERIALS AND METHODS
Subjects
The subjects for this study were drawn from a largerprospective imaging study of patients with stroke ortransient ischemic attack. Subjects met the followinginclusion criteria: (i) baseline MR imaging within 6 h ofsymptom onset with DWI, PWI, and inversion recoveryspin-echo, echo-planar imaging (IRSEPI) sequences(19), (ii) occlusion of the internal carotid artery, M1 orM2 branch of the middle cerebral artery on acute MRangiography (MRA) (25) as assessed by a neuroradiolo-gist at the time of the scan, and (iii) follow-up imaging at25 days (�15 days) that included DWI and fluid-atten-uated inversion recovery (FLAIR) imaging. Thirteen pa-tients met these criteria and were included in thisstudy. The study had ethical approval of the local insti-tutional ethics review board and all patients or surro-gate provided informed consent for participation in thestudy. Demographic data collected included age, gen-der and time of symptom onset or time since last seenwell, which was used to calculate time from onset to MRimaging. The National Institute of Health Stroke Scale(NIHSS) score at presentation was determined. All pa-tients received standard clinical care as decided by thetreating physician. A subset of patients who met insti-tutional criteria received thrombolytic therapy as treat-ment for their stroke. However, for the purposes of thisstudy, recanalization status, which may or may nothave been the result of thrombolysis, was used as theoutcome by which patients were grouped.
Imaging
All imaging was performed on a 3 Tesla (T) MR scanner(Signa, General Electric Healthcare, Waukesha, WI).The sequences included: (i) DWI (TR � 7000 ms, TE �96.5 ms, b � 1000 s/mm2,) and T2-weighted imaging(T2, b � 0 s/mm2) from which apparent diffusion coef-ficient (ADC) maps were derived, (ii) dynamic suscepti-
bility contrast PWI (10, 12, or 19 slices were acquiredwith TR/TE/repetitions of 1750 ms/45 ms/51, 1850ms/45 ms/42, or 2250 ms/40 ms/26, respectively,and flip angle � 45°), (iii) pre- and postcontrast MRA(25), and (iv) an inversion recovery spin-echo EPI se-quence (IRSEPI, TR � 12,000 ms, TE � 17.4 ms andTI � 400 ms) that produces images with high GM, WMand cerebrospinal fluid (CSF) contrast (19,20). For thePWI and MRA, 20 mL of gadolinium-containing con-trast agent (Magnevist, Berlex, NJ) was injected intra-venously with a MR-compatible power-injector (Me-drad, Pittsburg, PA) at a rate of 5 mL/s (PWI) or 2 mL/s(MRA). At 24 h from symptom onset, PWI and MRA wererepeated using the same sequences as at baseline formost patients (11 of 13). All of the sequences, with theexception of the MRA, had reconstructed matrix dimen-sions of 256 � 256, a field of view of 320 mm, and a 5.0mm slice thickness with a gap of 2.0 mm. The precon-trast MRA consisted of a 2-slab time-of-flight sequence(TR � 24 ms, TE � 3.3 ms, flip angle � 15°) with matrixdimensions of 512 � 512 � 64 and volume dimensionsof 240 mm � 144 mm � 64 mm. The postcontrast MRAconsisted of a single-slab time-of-flight sequence (TR �33 ms, TE � 3.9 ms, flip angle � 35°) focused on theintracranial circulation with matrix dimensions of512 � 512 � 48 and volume dimensions of 240 mm �144 mm � 76.8 mm (25). Final follow-up imaging at 25days (�15 days) included DWI, PWI, MRA, and FLAIRimaging (TR � 9002 ms, TE � 161 ms, TI � 2250,NEX � 0.5). The FLAIR image volume had the samedimensions as the DWI with the only difference being a240 mm field of view.
Postprocessing
For each patient, all images were co-registered to thefirst PWI volume (26). An experienced operator selectedan arterial input function (AIF) from the contralateralmiddle cerebral artery (MCA) based on the peak ampli-tude and arrival time of the contrast bolus using Per-fTool (27). Time-to-peak (TTP) maps were generated byidentifying the time-to-peak tracer concentration foreach voxel relative to that of the contralateral MCA AIF.Cerebral blood flow (CBF), cerebral blood volume (CBV),and mean transit time (MTT) maps were generated us-ing PerfTool (27) implementing a previously describedperfusion quantification methodology (28). A neurora-diologist blind to clinical information other than symp-tom side assessed the initial and follow-up MRA todefine the degree of recanalization as none, minimal,partial, or complete and also assessed change in MTTdeficit based on MTT maps generated with the GeneralElectric MR scanner’s clinical workstation. Persistentocclusion at follow-up (24 h, if available) was defined asno, minimal or partial recanalization without resolutionof the MTT deficit. Recanalization was defined as com-plete or partial recanalization with resolution of theMTT deficit. Resolution of the MTT deficit was definedas complete absence of an MTT abnormality detected onthe follow-up PWI.
The PWI and IRSEPI images were manually outlinedto define a brain mask, which excluded areas with grossspatial distortion or signal loss due to susceptibility
838 Bristow et al.

artifacts. The largest extent of visible TTP abnormalitywith at least 4 s of delay compared with the contralat-eral side was identified for analysis. An acute DWI le-sion was segmented from baseline DWI and ADC datausing a multi-spectral cluster classification technique.This technique differentiates “normal” from “abnormal”tissue under the supervision and guidance of a trainedoperator and has been shown to improve the reliabilityof lesion volume measurement compared with hand-drawn segmentation (29,30). The final lesion was sim-ilarly identified using final follow-up FLAIR, DWI, andADC images. Three regions of interest were subse-quently identified. LESION was defined as voxels inboth the acute DWI and final lesions. We definedGROWTH as voxels that were not part of the acute DWIlesion, but became part of the final lesion. The region ofOLIGEMIA consisted of voxels in the TTP abnormalitythat were not part of either the acute DWI or final lesion.
Anisotropic diffusion filtering (31) was applied to theIRSEPI images to reduce noise and enhance edges. Tis-sue segmentation was performed on the filtered IRSEPIimages using a fully automatic 3-class k-means algo-rithm (32). The k-means algorithm is a well-establishedsegmentation technique that has been applied andevaluated in different contexts to segment GM, WM,and CSF on MR images with different contrast charac-teristics (33,34). This classification was used to assigneach voxel to GM, WM, or CSF. CSF was excluded fromfurther analysis. The image values were normalized totarget white matter values by multiplying the originalvalues by a normalization factor. This factor was deter-mined by dividing the target median WM value (DWI �900, ADC � 800 mm2/s � 10�6, CBF � 22.0 mL/100g/min, CBV � 3.0 mL/100g, MTT � 8.0 s, TTP � 7.0 s,T2 � 2000) by the median value of a patient’s normalWM voxels. The normal WM voxels included WM voxelswithin a patient’s brain mask but outside the acuteDWI lesion, the final lesion, and the region of perfusionabnormality. The target median WM values were deter-mined by a combination of our calculated values andvalues reported in the literature (35–38). These valuesapproximately preserve the theoretical relationshipsamongst the diffusion parameters (DWI � T2 � e�b �
ADC; b � 1000 s/mm2) and amongst the perfusion pa-rameters (MTT � CBV/CBF) according to the centralvolume theorem (10,11,28). Subsequently, voxels po-tentially contaminated with CSF or arteries, or affectedby errors in co-registration or tissue segmentation wereexcluded. This was done by excluding voxels with im-aging values outside the range expected of brain paren-chyma (DWI � 500, ADC � 1400 mm2/s � 10�6, CBF �100 mL/100g/min, CBV � 16.0 mL/100g, and T2 �3500).
Analysis
The analysis was repeated for two groups of data. Thefirst dataset included the GROWTH and LESION regionvoxels from all patients (Growth versus Lesion). Thisdataset was used to determine how tissue destined forinfarction regardless of acute intervention might be dis-tinguished from the tissue potentially amenable toacute stroke therapy. The second dataset consisted of
the GROWTH and OLIGEMIA voxels only from thosepatients with persistent occlusion (Growth versus Oli-gemia). This dataset was used to distinguish tissuelikely to become infarct if acute recanalization is notachieved from tissue that is likely to remain viable re-gardless. Combining the two sets of analyses poten-tially allows for identification of the threatened penum-bra that is the target of acute stroke therapy. Allstatistical tests were two-tailed with P � 0.05 consid-ered significant. Commercial statistical software (Inter-cooled Stata 8.2, Stata Corporation, College Station,TX) was used for all statistical analyses. For DWI, TTPand T2, a one-factor analysis of variance test (ANOVA)was performed to test for differences between regions.For ADC, CBF, CBV, and MTT, two-factor ANOVA testswere performed to assess differences between regionsand between tissue types (GM and WM). ANOVA testingis robust to deviations from normality and equality ofvariance (39).
Logistic regression was used for the primary analysisand the primary outcome variable was the region(Growth versus Lesion, Growth versus Oligemia). Weused the cluster option of the logit function in Stata toaccount for independence of values across patients, butnot necessarily within patients. Univariable analysiswas performed for each imaging parameter on eachdataset of voxels pooled across patients. The Wald sta-tistic was used to test for significance of each parameterin the model. Area under the curve (AUC) on receiveroperating characteristic analysis was used to evaluatethe predictive ability of each parameter and standarderrors (SEs) of the AUC were calculated based on anonparametric method (40). Each parameter was as-sessed for linearity in the logit. Tests for correlation andco-linearity were also performed.
Multivariable analysis was carried out following theguidelines given by Hosmer and Lemeshow (41). Westarted with a full model that included all imaging pa-rameters deemed moderately important from the uni-variable analysis (Wald statistic P � 0.25). Parameterswere excluded iteratively from the model according tothe highest Wald statistic until all remaining covariateswere significant (P � 0.05). Changes in coefficients weremonitored for confounding. Once a model based onmain effects was obtained, two-way multiplicative in-teraction between ADC and CBF was evaluated as wereinteractions between tissue type and any of ADC, CBF,CBV, and MTT that were found to vary with tissue typeon ANOVA testing. Tissue type was coded in the Tissuevariable (GM � 0, WM � 1). The final model includedsignificant main effects and significant interactions.
Cross-validation was performed using a leave-one-patient-out approach (42,43). A model using the pa-rameters from the final model was trained on data fromall patients but one. The resulting model was thentested on data from the excluded patient. This wasrepeated for each patient in the dataset and the meanand standard deviation (SD) of the AUCs were calcu-lated. To evaluate the importance of using two separatemodels in differentiating GROWTH from LESION andfrom OLIGEMIA, each model was applied to the otherdataset. The resulting AUCs were compared with thoseresulting from the previous analysis to determine how
Identifying Stroke Lesion Growth With MR 839

well each model performed on the other dataset. Fi-nally, we applied the final models to imaging data togenerate probability maps that identify the acute le-sion, as well as predict tissue likely to be recruited intothe final infarct.
RESULTS
Demographic information is shown in Table 1 for the 13patients included in this study. Seven patients werefemale and the median (interquartile range) values ofthe clinical variables were as follows: age � 69 (58–78)
years old, NIHSS score at presentation � 6 (3–7), andtime from onset to MR imaging � 215 min (181–288min). Seven patients received thrombolytic therapy,three of whom recanalized. Of the six remaining pa-tients, one recanalized spontaneously. The mean val-ues of each imaging parameter are shown in Table 2 foreach region and tissue type. The first dataset (Growthversus Lesion, n � 13) included 7,964 voxels (87.1 mL)of GROWTH and 3973 voxels (43.5 mL) of LESION. Thesecond dataset (Growth versus Oligemia, n � 9) con-sisted of 6,378 voxels (69.8 mL) of GROWTH and45,015 voxels (492.4 mL) of OLIGEMIA. Significant dif-
Table 1Patient Demographic Data and Ischemic Compartment Volumes
Patientno.
Age(years)
Gender NIHSSTime to
MRI (h:m)Occluded
vesseltPA Recanalized
Compartment volumes (mL)
Lesion Growth Oligemia
1 78 F 13 3:35 R M1 Y N 5.93 36.00 49.252 73 M 3 2:33 R M2 & ICA N N 0.98 9.64 83.073 55 M 0 3:17 L M1 N N 0.30 4.20 57.434 48 F 6 4:59 R M2 N N 0.74 0.89 14.885 69 M 3 2:27 R MCA & ICA N N 1.13 3.60 123.546 75 F 3 5:55 L M2 Y N 0.80 4.34 57.157 58 M 2 5:56 R ICA N N 0.46 3.20 28.858 83 F 22 3:01 LM1 Y N 22.13 7.51 64.099 58 F 8 3:04 R ICA Y Na 0.07 0.38 14.0910 55 F 2 2:15 L M2 N Y 3.62 5.70 N/A11 80 M 6 3:51 R M2 Y Y 1.18 8.25 N/A12 68 F 6 4:11 L M2 Y Y 0.49 1.58 N/A13 79 M 7 4:48 R MCA Y Ya 5.63 1.83 N/A
aRecanalization was assessed using final follow-up magnetic resonance angiography (all others assessed at 24 hours).NIHSS � National Institutes of Health Stroke Scale score; MRI � magnetic resonance imaging; h � hours; m � minutes; tPA � intravenoustissue plasminogen activator; F � female; M � male; R � right; L � left; MCA � middle cerebral artery; M1 � M1 branch of MCA; M2 �M2 branch of MCA; ICA � internal carotid artery; Y � yes; N � no; N/A � not applicable.
Table 2Means (Standard Deviations) of Each Region (All Voxels From Each Patient Combined)*
Lesiona Growtha OligemiabP (Growth vs. Lesiona) P (Growth vs. Oligemiab)
Region Tissue Interactionc Region Tissue Interactionc
DWI (SI) 1442 (233) 1108 (199) 903 (168) � 0.001 � 0.001ADC (mm2/s � 10�6) � 0.001 � 0.001 � 0.001 � 0.001 � 0.001 0.3739
GM 485 (139) 800 (197) 902 (207)WM 483 (114) 725 (146) 814 (161)
CBF (mL/100g/min) � 0.001 � 0.001 0.0191 � 0.001 � 0.001 � 0.001GM 13.2 (10.5) 20.9 (14.0) 35.0 (18.3)WM 9.9 (6.4) 16.6 (10.4) 25.1 (13.5)
CBV (mL/100g) � 0.001 � 0.001 � 0.001 � 0.001 � 0.001 � 0.001GM 2.5 (2.2) 4.1 (2.8) 5.9 (3.4)WM 2.1 (1.4) 3.1 (1.9) 4.2 (2.4)
MTT (s) 0.0105 � 0.001 � 0.001 � 0.001 0.6445 0.3209GM 11.1 (5.1) 11.8 (4.7) 10.1 (4.0)WM 12.2 (5.4) 12.0 (4.9) 10.1 (4.1)
TTP (s) 22.2 (17.6) 25.0 (18.7) 14.8 (10.4) � 0.001 � 0.001T2 (SI) 2275 (433) 2276 (443) 2110 (478) 0.9711 � 0.001Volume (mL) 43.5 87.1 492.4Voxels 3973 7964 45015
*Means shown for GM and WM separately for ADC, CBF, CBV and MTT.aNumber of patients � 13 in Growth vs. Lesion analysis.b number of patients � 9 in Growth vs. Oligemia analysis.c Two-way multiplicative interaction between Region and Tissue.DWI � diffusion-weighted imaging; ADC � apparent diffusion coefficient; CBF � cerebral blood flow; CBV � cerebral blood volume; MTT �mean transit time; TTP � time-to-peak; T2 � T2-weighted imaging; SI � signal intensity; GM � gray matter; WM � white matter; P � P valuefrom analysis of variance.
840 Bristow et al.

ferences were found between regions for all parametersexcept T2 between GROWTH and LESION. Differenceswere also found between GM and WM for ADC, CBF,CBV and MTT except for MTT in the Growth versusOligemia dataset. The mean values presented in Table 2are slightly different than the expected median valuesdue to a skew distribution. For example, the medianvalue of WM in the region of OLIGEMIA was 22.4 mL/100 g per min as compared to the mean value of 25.1mL/100 g per min. The former value more closely re-sembles the median value of normal white matter, nor-malized to 22.0 mL/100 g per min.
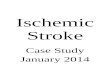
The results of the logistic regression analysis areshown in Figure 1. In the Growth versus Lesion univa-riable analysis, ADC was the best predictor of outcome(AUC � 0.911; P � 0.001), followed by DWI (AUC �0.863; P � 0.001), CBF (AUC � 0.710; P � 0.001), andCBV (AUC � 0.686; P � 0.003). MTT, TTP, and T2 werenot statistically significant predictors. In the Growthversus Oligemia univariable analysis, DWI was the bestpredictor (AUC � 0.785; P � 0.001), followed by CBF(AUC � 0.743, P � 0.001), TTP (AUC � 0.739; P �0.001), CBV (AUC � 0.657; P � 0.001), ADC (AUC �0.655; P � 0.001), MTT (AUC � 0.638; P � 0.003), andT2 (AUC � 0.614; P � 0.001). Each parameter had anappropriate linear relationship with the logit of the out-come variable. CBF and CBV were highly correlated(Pearson’s r � 0.83 for Growth versus Lesion, r � 0.81for Growth versus Oligemia). In favor of model simplic-ity and because CBF achieved a higher AUC in both
datasets, CBF was used in the multivariable analysisand CBV was excluded. There was some correlationbetween DWI and ADC in the Growth versus Lesiondataset (Peason’s r � �0.61) but as this was less than�0.8, we did not expect it to cause problems in model-building and so both parameters were included (44).The remaining correlation coefficients were � �0.5. Alltests for co-linearity were negative in the model-build-ing process.
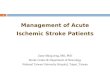
For the Growth versus Lesion multivariable analysis,the final model included DWI, ADC, CBF, tissue type,interaction between ADC and CBF, and interaction be-tween CBF and tissue type. This model provided anAUC of 0.936 (SE � 0.002) on the pooled dataset. Figure2 shows the probabilities of acute infarction for GM andWM plotted at certain levels of CBF for a range of ADC.This graph shows that, given a certain level of ADC,voxels at a lower level of CBF are at a higher risk ofbeing part of the acute lesion. This relationship is moreevident in WM than GM. In addition, it shows that GMis at higher risk than WM at the same level of CBF. Forthe Growth versus Oligemia multivariable analysis, thefinal model included DWI, ADC, CBF, TTP and interac-tion between ADC and CBF. Again, given a certain levelof ADC, voxels at a lower level of CBF are at a higher riskof being part of lesion growth than oligemia. This modelprovided an AUC of 0.831 (SE � 0.003) on the pooleddataset. The final model coefficients are given in Table3. Our hypothesis that the models are different wasconfirmed because the models contain different param-
Figure 2. Interaction among ADC, CBF, and tissue type. At agiven value of ADC, the probability of acute infarction dependson the level of CBF with lower CBF representing higher prob-ability. The probability of acute infarction at a certain level ofCBF depends on the tissue type. GM is at higher risk than WMat the same level of CBF. The increase in probability of acuteinfarction attributed to a decrease in CBF is more evident inWM than in GM. For example, a decrease in CBF from 25 to 15mL/100g per min at an ADC of 500 � 10�6 mm2/s increasesthe probability of acute infarction in GM from 54% to 58%. InWM, on the other hand, a similar decrease in CBF increasesthe probability of acute infarction from 35% to 47%. Theseprobabilities were calculated from the Growth versus Lesionmodel with DWI � 1200. ADC, apparent diffusion coefficient;CBF, cerebral blood flow; GM, gray matter; WM, white matter;DWI, diffusion-weighted imaging.
Figure 1. AUC results of univariable and multivariable mod-els. In the Growth versus Lesion univariable analysis, ADCwas the best predictor of outcome according to the AUC fol-lowed by DWI, CBF and CBV. MTT, TTP, and T2 were notstatistically significant predictors. In the Growth versus Olige-mia univariable analysis, DWI was the best predictor followedby CBF, TTP, CBV, ADC, MTT, and T2.The multivariable finalmodels are more accurate than any single parameter alone(Final; Growth versus Lesion AUC � 0.936, Growth versusOligemia AUC � 0.831) and are validated by cross-validation(XVal; Growth versus Lesion AUC � 0.939, Growth versusOligemia AUC � 0.793). AUC, area under the curve (receiveroperating characteristic analysis); DWI, diffusion-weightedimaging; ADC, apparent diffusion coefficient; CBF, cerebralblood flow; CBV, cerebral blood volume; MTT, mean transittime; TTP, time-to-peak; T2, T2-weighted imaging.
Identifying Stroke Lesion Growth With MR 841

eters despite being created by the same model-buildingprocess and parameter selection criteria. The sensitiv-ities, specificities, and positive and negative predictivevalues are given in Table 4 for selected probabilitythresholds.
The results of cross-validation are shown in Table 5for each patient. Cross-validation of the Growth versusLesion model parameters on all 13 patients resulted ina mean AUC of 0.939 (SD � 0.028), indicating thismodel is internally robust in discriminating betweenthese two compartments. Cross-validation of theGrowth versus Oligemia model parameters on the ninepatients with persistent occlusion resulted in a meanAUC of 0.793 (SD � 0.106), indicating that this model issimilarly valid. When the final model resulting from theGrowth versus Oligemia analysis was applied to theGrowth versus Lesion pooled dataset, the AUC was
0.816 (SE � 0.004), considerably lower compared withthe AUC of 0.936 obtained by the custom-fit model.When the model resulting from the Growth versus Le-sion analysis was applied to the Growth versus Olige-mia pooled dataset, the AUC was 0.700 (SE � 0.004),again considerably lower than the 0.831 obtained bythe custom-fit model. The differences in AUC obtainedby each of the models when applied to the other datasetfurther supports our hypothesis that different modelsare required for distinguishing GROWTH from LESIONand from OLIGEMIA.
Figures 3 and 4 show the results of applying theGrowth versus Lesion and Growth versus Oligemiamodels to MR imaging data from two patients. In Figure3, a case of persistent occlusion, the tissue predicted tobecome part of the final lesion (G) is similar to the finallesion shown on the follow-up FLAIR (E). The difference
Table 3Multivariable Analysis Results: Final Logistic Regression Models
Final Model Parameter Coefficient P95% Confidence interval
AUC (SE)Lower Upper
Growth vs. Lesion 0.936 (0.002)DWI 0.00448 0.001 0.00183 0.00714ADC �0.01323 �0.001 �0.01518 �0.01129CBF �0.08786 �0.001 �0.12344 �0.05228
Tissue 0.05714 0.850 �0.53516 0.64943ADC � CBF 0.00015 �0.001 0.00010 0.00020
CBF � Tissue �0.03316 0.001 �0.05215 �0.01416Constant 1.76204 0.268 �1.35441 4.87848
Growth vs. Oligemia 0.831 (0.003)DWI 0.00508 �0.001 0.00388 0.00628ADC �0.00093 0.117 �0.00209 0.00023CBF �0.06179 0.005 �0.10504 �0.01853TTP 0.03665 �0.001 0.02316 0.05014
ADC � CBF 0.00004 0.036 0.00000 0.00007Constant �6.24988 �0.001 �7.58436 �4.91539
DWI � diffusion-weighted imaging; ADC � apparent diffusion coefficient; CBF � cerebral blood flow; TTP � time-to-peak; P � P value ofWald statistic; AUC � area under the curve (receiver operating characteristic analysis); SE � standard error.
Table 4Predictive Performance of Models at Different Probability Thresholds Using Receiver Operating Characteristic Analysis*
Final Model Probability % Sensitivity % Specificity % PPV % NPV
Growth vs. Lesion0.90 38.7 (1538 of 3973) 99.3 (7909 of 7964) 96.5 (1538 of 1593) 76.5 (7909 of 10344)0.85 46.4 (1843 of 3973) 98.7 (7857 of 7964) 94.5 (1843 of 1950) 78.7 (7857 of 9987)0.75 58.4 (2319 of 3973) 96.9 (7719 of 7964) 90.4 (2319 of 2564) 82.4 (7719 of 9373)0.50 76.4 (3036 of 3973) 91.4 (7282 of 7964) 81.7 (3036 of 3718) 88.6 (7282 of 8219)0.25 90.0 (3574 of 3973) 81.2 (6466 of 7964) 70.5 (3574 of 5072) 94.2 (6466 of 6865)0.15 94.9 (3772 of 3973) 72.6 (5780 of 7964) 63.3 (3772 of 5956) 96.6 (5780 of 5981)0.10 96.9 (3850 of 3973) 64.6 (5146 of 7964) 57.7 (3850 of 6668) 97.7 (5146 of 5269)
Growth vs.Oligemia
0.90 5.2 (334 of 6378) 99.8 (44942 of 45015) 82.1 (334 of 407) 88.1 (44942 of 50986)0.85 8.1 (519 of 6378) 99.8 (44904 of 45015) 82.4 (519 of 630) 88.5 (44904 of 50763)0.75 13.1 (833 of 6378) 99.6 (44814 of 45015) 80.6 (833 of 1034) 89.0 (44814 of 50359)0.50 27.6 (1758 of 6378) 98.5 (44341 of 45015) 72.3 (1758 of 2432) 90.6 (44341 of 48961)0.25 52.5 (3348 of 6378) 92.8 (41782 of 45015) 50.9 (3348 of 6581) 93.2 (41782 of 44812)0.15 67.7 (4315 of 6378) 82.9 (37326 of 45015) 35.9 (4315 of 12004) 94.8 (37326 of 39389)0.10 77.8 (4960 of 6378) 71.3 (32107 of 45015) 27.8 (4960 of 17868) 95.8 (32107 of 33525)
*The probability represents the probability of a voxel being part of the acute lesion (Growth vs. Lesion model and dataset) or of lesion growth(Growth vs. Oligemia model and dataset) according to the logistic regression model.PPV � positive predictive value; NPV � negative predictive value.
842 Bristow et al.

between the predicted acute (F) and final (G) lesionsrepresents tissue potentially amenable to acute stroketherapy. Figure 4 demonstrates a case with recanaliza-tion. In this case the final lesion apparent on the fol-low-up FLAIR is similar to both the predicted acute (F)and final (G) lesions.
DISCUSSION
This study found that different DWI and PWI parame-ters, and consequently different models, optimally dis-tinguish lesion growth from the acute lesion comparedwith those that distinguish lesion growth from oligemia.This is important because it suggests that, in identify-ing tissue that may be salvaged with acute stroke ther-apy with voxel-based predictive models, different imag-ing parameters and methods should be used todistinguish the target of therapy from each of the phys-iologically distinct acute lesion and region of oligemia.
In distinguishing lesion growth from the acute lesion,ADC was found to be the best predictor of outcome.This agrees with the findings of Kidwell et al (3) thatADC was the most important predictive variable inmodeling irreversible infarction despite recanalization.Furthermore, ADC interacts with CBF, which meansthat at a given level of ADC, the probability of acuteinfarction depends on the level of CBF. This interactionhas not been reported in studies of tissue outcomemodeling in acute ischemic stroke. However, previousstudies have observed that ADC decreases graduallywith a decrease in CBF until a certain critical thresholdis reached below which ADC decreases more abruptlywith CBF (23,24). Because MR imaging of the strokepatient occurs at a single snapshot in time during adynamic process, this interaction between ADC andCBF is important to consider in predicting tissue out-come. Furthermore, it explains the difficulties encoun-tered when using ADC or CBF thresholds in isolationfor predicting tissue fate and helps explain the reversalof ADC lesions with acute thrombolytic therapy (14–
16,45,46). In addition, we found significant interactionbetween CBF and tissue type. At a given level of lowCBF, GM is at higher risk of being part of the acutelesion than WM confirming that GM is more vulnerableto ischemia than WM (19–22).
In distinguishing lesion growth from oligemia in thesetting of persistent occlusion, ADC is not as helpful asit is in identifying the acute lesion but still interactswith CBF. TTP is an important predictor of tissue out-come and, interestingly, DWI remains useful, perhapsdue to conservative segmentation of the acute lesion.Distinguishing lesion growth from oligemia is a moredifficult task, as indicated by the lower AUC, and likelyreflects the time-varying nature of diffusion and perfu-sion thresholds and errors in MR perfusion quantifica-tion. Our results indicate that in distinguishing lesiongrowth from the acute lesion and from oligemia onpooled data, a relatively accurate determination (AUC �0.8) of tissue outcome can still be achieved with only afew MR imaging parameters and the approach is reli-able across patients. It should be noted that a goodaverage AUC is not the same as good discriminationamong compartments on a patient-by-patient basis,however. The threshold that optimally discriminatesone compartment from another, as represented by theoptimal point on a receiver operating characteristiccurve for example, may vary from patient to patient,making it difficult to prospectively predict tissue out-come.
Wu et al (1) found that in building a generalized linearmodel to distinguish final infarct from noninfarct ipsi-lateral tissue with normalized imaging parameters,DWI, ADC, CBF, CBV, MTT, T2, and the time of thepeak of the residue function were all significant param-eters. In building our models, we assumed indepen-dence of values across patients, but not within patients,resulting in a more conservative selection of model co-variates. Their study reported an AUC of 0.90 � 0.05 fora model developed on 11 patients who did not receivethrombolytic therapy, which is consistent with the
Table 5Results of Cross-Validation*
Patient no.Growth vs. Lesion Growth vs. Oligemia
AUC (SE) Training voxels AUC (SE) Training voxels
1 0.902 (0.006) 8104 0.773 (0.005) 557202 0.962 (0.008) 10966 0.654 (0.011) 550383 0.955 (0.012) 11526 0.725 (0.011) 578794 0.894 (0.026) 11788 0.765 (0.025) 620735 0.969 (0.008) 11505 0.903 (0.005) 518906 0.892 (0.020) 11467 0.780 (0.012) 578927 0.968 (0.009) 11602 0.680 (0.017) 605838 0.938 (0.005) 9227 0.897 (0.006) 569679 0.957 (0.031) 11896 0.963 (0.010) 6219110 0.929 (0.008) 11085 N/A N/A11 0.959 (0.010) 11075 N/A N/A12 0.951 (0.015) 11748 N/A N/A13 0.935 (0.010) 11255 N/A N/AMean (SD) 0.939 (0.028)a 0.793 (0.106)a
*AUCs shown for each patient are the results of applying a model that was trained on voxels from all other patients.aSD given in parentheses instead of SE.AUC � area under the curve (receiver operating characteristic analysis); SE � standard error of single AUC; SD � standard deviationcalculated across patients; N/A � not applicable.
Identifying Stroke Lesion Growth With MR 843

AUCs obtained in our two models. Another study byRose et al (13) that used absolute and relative measuresof DWI, CBF, CBV, and MTT to train a parametric clas-sifier to distinguish final infarct from salvaged tissue in
nontreated patients found that CBF was useful andCBV was of dubious value. Their model obtained amean sensitivity of 74%, a mean specificity of 97%, amean positive predictive value of 68%, and a mean
Figure 3. Application of logistic regression models to MR imaging from Patient 1 who experienced persistent occlusion. A–D: Thetop row shows the acute DWI (A), ADC (B), CBF (C), and TTP (D) images (brain masked). E–H: The bottom row shows the finalfollow-up FLAIR (E), the probability maps generated by the Growth versus Lesion (F) and Growth versus Oligemia (G) modelsoverlaid on the FLAIR, and the region of perfusion abnormality selected for analysis (H). Probability values range between 0 and1, where 0 (dark) is at low risk of infarction and 1 (bright) is at high risk. The logistic regression models generate probability mapsthat highlight the tissue destined for infarction regardless of acute intervention (F) and the tissue likely to become infarct if acuterecanalization is not achieved (G). The difference between these two represents tissue potentially amenable to acute stroketherapy. DWI, diffusion-weighted imaging; ADC, apparent diffusion coefficient; CBF, cerebral blood flow; TTP, time-to-peak;FLAIR, fluid attenuated inversion recovery.
Figure 4. Application of logistic regression models to MR imaging from Patient 10 who experienced spontaneous recanalization. A–D:The top row shows the acute DWI (A), ADC (B), CBF (C), and TTP (D) images (brain masked). E–H: The bottom row shows the finalfollow-up FLAIR (E), the probability maps generated by the Growth versus Lesion (F) and Growth versus Oligemia (G) models overlaidon the FLAIR, and the region of perfusion abnormality selected for analysis (H). Probability values range between 0 and 1, where 0(dark) is at low risk of infarction and 1 (bright) is at high risk. The logistic regression models generate probability maps that highlightthe tissue destined for infarction regardless of acute intervention (F) and the tissue likely to become infarct if acute recanalization isnot achieved (G). The difference between these two represents tissue potentially amenable to acute stroke therapy. In this case, thereis not much difference between the predicted acute (F) and final (G) lesions suggesting that any potential benefit of thrombolytictherapy probably would not have outweighed the potential risk. DWI, diffusion-weighted imaging; ADC, apparent diffusion coefficient;CBF, cerebral blood flow; TTP, time-to-peak; FLAIR, fluid attenuated inversion recovery.
844 Bristow et al.

negative predictive value of 98% on a training dataset of10 patients imaged within 13 h of stroke onset whowere not treated with thrombolytic therapy. These stud-ies did not separate lesion growth from the acute lesionin distinguishing the final lesion from salvaged tissue.
Our results indicate that, especially given the inter-action between ADC and CBF, the acute lesion is bestidentified with a multi-parametric approach. By refin-ing the diffusion-perfusion mismatch approach to pen-umbra identification, a multi-parametric, voxel-basedapproach could be used prospectively to first identifythe acute lesion and then distinguish probable lesiongrowth from oligemia using separate models of MR im-aging-based parameters (3). This approach is illus-trated in Figures 3 and 4 where the mismatch betweenthe model-identified, acute lesion, highlighted in theprobability map F, and the final lesion, highlighted in G,would identify tissue that may benefit from acute stroketherapy. In Figure 3, there is an appreciable region oftissue that may have benefited from recanalization. InFigure 4 on the other hand, there is not much differencebetween the model-identified acute lesion and the pre-dicted final lesion suggesting that any potential benefitof thrombolytic therapy probably would not have out-weighed the potential risk. This type of approach ispotentially feasible in the clinical setting. Advance-ments in image co-registration computing methodshave reduced the most time-consuming step in imageprocessing from a couple of minutes to a few seconds.The IRSEPI sequence only takes several extra secondsto acquire and the filtering and tissue segmentationtake only a few seconds to perform. The calculation ofperfusion parameters takes approximately 30 s of pro-cessing time once the images are loaded and an AIF isselected (27). It takes only seconds to apply the modelsto the postprocessed data to generate probability maps,although this would first require normalization to targetwhite matter values. The challenge would be to stream-line these steps in a comprehensive software package toallow for user-friendly and efficient processing. Withsuch a tool and a trained operator, it should be possibleto generate probability maps in less than 5 min on adesktop computer to support stroke management deci-sions for individual patients in the acute setting.
This study was limited by the small number of pa-tients and by the relatively small strokes that thesepatients experienced. This reflects the difficulty ofquickly recruiting, consenting and imaging patientswith severe strokes for research studies. It is possiblethat patients with large infarcts may have dominatedthe training process causing the models to be biased.Errors in co-registration and in lesion and tissue seg-mentation may have resulted in voxels being assignedto the wrong ischemic tissue compartment or tissuetype. These errors, along with partial volume effects,may have had a large impact on patients with smallacute lesion and growth volumes. Quantification of MRperfusion parameters is still hampered by multiplesources of error. As a result, MR perfusion maps arecommonly scaled or normalized according to a normalWM reference region to allow for between-subject per-fusion comparisons (1,21). Deviations in the underlyingassumption that normal WM has low variability in the
human population may have introduced bias that re-duced true differences among patients. Another limita-tion was that the patients in this study were assessed atdifferent times since stroke onset even though ADC andCBF thresholds for infarction are time-dependent(6,24). Including patient-based clinical variables suchas time-from-onset, thrombolytic administration, age,gender, serum glucose, blood pressure, and tempera-ture (6,11,47) would be appropriate in studies withlarger patient numbers. Despite these drawbacks, themodels still performed well on cross-validation. Thesemodels need to be further validated, however, on inde-pendent data. As well, further work could evaluate theselection of optimal thresholds for individual patientsand the applicability of common thresholds across pa-tients for prospective tissue outcome prediction.
In differentiating GROWTH from LESION, we in-cluded patients with persistent occlusion as well aspatients who recanalized. Because early restorationof blood flow is a critical event in determining tissuefate, it is likely that separate models would be moresuitable for these two patient populations. Limited bythe number of patients and small infarct sizes in thisstudy, we attempted to partially account for this byexcluding from our analysis the region of reversiblediffusion abnormality (DWI lesion acutely, but notpart of the final lesion), which may occur with recan-alization (3,46). Having excluded this region, our im-aging-based definition of the acute lesion does notchange, regardless of recanalization. We believe thatearly recanalization is more likely to alter the bound-ary between lesion growth and oligemia and for thisreason we only considered patients with persistentocclusion in differentiating GROWTH from OLIGE-MIA. Recanalization is not expected to alter the out-come of either the acute, core infarct or the region ofbenign oligemia. It may well affect, however, the crit-ical boundary that separates the penumbra that isrecruited into the final infarct from that which issalvaged (3,6). It is the identification of probable le-sion growth, or threatened penumbra, that is mostcritical for future stroke treatment trials.
In conclusion, this study has determined that theoptimal MR imaging parameters and predictive modelthat distinguish lesion growth from the acute lesion aredifferent compared with those that optimally distin-guish lesion growth from oligemia. Distinction amongthe different ischemic regions is important for identify-ing the target of acute stroke treatment, the threatenedpenumbra (3,18). In this study, normalized DWI, ADC,CBF, TTP, and tissue type were the most importantparameters in modeling the different ischemic compart-ments and these parameters provide relatively accurateand reliable discrimination among the acute lesion, le-sion growth, and oligemia.
ACKNOWLEDGMENT
The authors thank Dr. James N. Scott for assessing theMTT deficits derived from the PWI as well as the MRA.
Identifying Stroke Lesion Growth With MR 845

REFERENCES
1. Wu O, Christensen S, Hjort N, et al. Characterizing physiologicalheterogeneity of infarction risk in acute human ischaemic strokeusing MRI. Brain 2006;129:2384–2393.
2. Tissue plasminogen activator for acute ischemic stroke. The Na-tional Institute of Neurological Disorders and Stroke rt-PA StrokeStudy Group. N Engl J Med 1995;333:1581–1587.
3. Kidwell CS, Alger JR, Saver JL. Beyond mismatch: evolving para-digms in imaging the ischemic penumbra with multimodal mag-netic resonance imaging. Stroke 2003;34:2729–2735.
4. Rowley HA. Extending the time window for thrombolysis: evidencefrom acute stroke trials. Neuroimaging Clin N Am 2005;15:575–587, x.
5. Sims J, Schwamm LH. The evolving role of acute stroke imaging inintravenous thrombolytic therapy: patient selection and outcomesassessment. Neuroimaging Clin N Am 2005;15:421–440, xii.
6. Muir KW, Buchan A, von Kummer R, Rother J, Baron JC. Imagingof acute stroke. Lancet Neurol 2006;5:755–768.
7. Gobin YP, Starkman S, Duckwiler GR, et al. MERCI 1: a phase 1study of mechanical embolus removal in cerebral ischemia. Stroke2004;35:2848–2854.
8. Davalos A, Castillo J, Alvarez-Sabin J, et al. Oral citicoline in acuteischemic stroke: an individual patient data pooling analysis of clin-ical trials. Stroke 2002;33:2850–2857.
9. Singhal AB, Benner T, Roccatagliata L, et al. A pilot study of nor-mobaric oxygen therapy in acute ischemic stroke. Stroke 2005;36:797–802.
10. Baird AE, Warach S. Magnetic resonance imaging of acute stroke.J Cereb Blood Flow Metab 1998;18:583–609.
11. Lauzon ML, Sevick RJ, Demchuk AM, Frayne R. Stroke imaging at3.0 T. Neuroimaging Clin N Am 2006;16:343–366.
12. Wu O, Koroshetz WJ, Ostergaard L, et al. Predicting tissue outcomein acute human cerebral ischemia using combined diffusion- andperfusion-weighted MR imaging. Stroke 2001;32:933–942.
13. Rose SE, Chalk JB, Griffin MP, et al. MRI based diffusion andperfusion predictive model to estimate stroke evolution. Magn Re-son Imaging 2001;19:1043–1053.
14. Rohl L, Ostergaard L, Simonsen CZ, et al. Viability thresholds ofischemic penumbra of hyperacute stroke defined by perfusion-weighted MRI and apparent diffusion coefficient. Stroke 2001;32:1140–1146.
15. Grandin CB, Duprez TP, Smith AM, et al. Which MR-derived per-fusion parameters are the best predictors of infarct growth in hy-peracute stroke? Comparative study between relative and quanti-tative measurements. Radiology 2002;223:361–370.
16. Schaefer PW, Ozsunar Y, He J, et al. Assessing tissue viability withMR diffusion and perfusion imaging. AJNR Am J Neuroradiol 2003;24:436–443.
17. Markus HS. Cerebral perfusion and stroke. J Neurol NeurosurgPsychiatry 2004;75:353–361.
18. Gonzalez RG. Imaging-guided acute ischemic stroke therapy: from“time is brain” to “physiology is brain”. AJNR Am J Neuroradiol2006;27:728–735.
19. Simon JE, Bristow MS, Lu H, et al. A novel method to deriveseparate gray and white matter cerebral blood flow measures fromMR imaging of acute ischemic stroke patients. J Cereb Blood FlowMetab 2005;25:1236–1243.
20. Bristow MS, Simon JE, Brown RA, et al. MR perfusion and diffusionin acute ischemic stroke: human gray and white matter have dif-ferent thresholds for infarction. J Cereb Blood Flow Metab 2005;25:1280–1287.
21. Arakawa S, Wright PM, Koga M, et al. Ischemic thresholds for grayand white matter: a diffusion and perfusion magnetic resonancestudy. Stroke 2006;37:1211–1216.
22. Falcao AL, Reutens DC, Markus R, et al. The resistance to ischemiaof white and gray matter after stroke. Ann Neurol 2004;56:695–701.
23. Lin W, Lee JM, Lee YZ, Vo KD, Pilgram T, Hsu CY. Temporalrelationship between apparent diffusion coefficient and absolute
measurements of cerebral blood flow in acute stroke patients.Stroke 2003;34:64–70.
24. Guadagno JV, Jones PS, Fryer TD, et al. Local relationships be-tween restricted water diffusion and oxygen consumption in theischemic human brain. Stroke 2006;37:1741–1748.
25. Yang JJ, Hill MD, Morrish WF, et al. Comparison of pre- andpostcontrast 3D time-of-flight MR angiography for the evaluation ofdistal intracranial branch occlusions in acute ischemic stroke.AJNR Am J Neuroradiol 2002;23:557–567.
26. Jenkinson M, Smith S. A global optimisation method for robustaffine registration of brain images. Med Image Anal 2001;5:143–156.
27. Kosior JC, Frayne R. PerfTool: a software platform for investigatingbolus-tracking perfusion imaging quantification strategies. J MagnReson Imaging 2007;25:653–659.
28. Ostergaard L, Weisskoff RM, Chesler DA, Gyldensted C, Rosen BR.High resolution measurement of cerebral blood flow using intra-vascular tracer bolus passages. Part I. Mathematical approach andstatistical analysis. Magn Reson Med 1996;36:715–725.
29. Mitchell JR, Karlik SJ, Lee DH, Fenster A. Computer-assisted iden-tification and quantification of multiple sclerosis lesions in MRimaging volumes in the brain. J Magn Reson Imaging 1994;4:197–208.
30. Mitchell JR, Tomanek A, Simon JE, et al. Reliable computer as-sisted measurement of stroke lesion volumes. Stroke 2002;33:363(abstract).
31. Black MJ, Sapiro G, Marimont DH, Heeger D. Robust anisotropicdiffusion. IEEE Trans Image Proc 1998;7:421–432.
32. Hartigan J, Wong M. Algorithm AS136: a k-means clustering algo-rithm. Appl Stat 1979;28:100–108.
33. Cardenas VA, Ezekiel F, Di Sclafani V, Gomberg B, Fein G. Reli-ability of tissue volumes and their spatial distribution forsegmented magnetic resonance images. Psychiatry Res 2001;106:193–205.
34. Leigh R, Ostuni J, Pham D, et al. Estimating cerebral atrophy inmultiple sclerosis patients from various MR pulse sequences. MultScler 2002;8:420–429.
35. Burdette JH, Durden DD, Elster AD, Yen YF. High b-value diffu-sion-weighted MRI of normal brain. J Comput Assist Tomogr 2001;25:515–519.
36. Helenius J, Soinne L, Perkio J, et al. Diffusion-weighted MR imag-ing in normal human brains in various age groups. AJNR Am JNeuroradiol 2002;23:194–199.
37. Vonken EJ, van Osch MJ, Bakker CJ, Viergever MA. Measurementof cerebral perfusion with dual-echo multi-slice quantitative dy-namic susceptibility contrast MRI. J Magn Reson Imaging 1999;10:109–117.
38. Helenius J, Perkio J, Soinne L, et al. Cerebral hemodynamics in ahealthy population measured by dynamic susceptibility contrastMR imaging. Acta Radiol 2003;44:538–546.
39. Miller RG. Beyond ANOVA: basics of applied statistics. New York:Chapman and Hall; 1997.
40. Delong ER, Delong DM, Clarke-Pearson DL. Comparing the areasunder two or more correlated receiver operating curves: a non-parametric approach. Biometrics 1988;44:837–845.
41. Hosmer DW, Lemeshow S. Applied logistic regression. New York:John Wiley and Sons, Inc.; 2000. 373 p.
42. Hastie T, Tibshirani R, Friedman JH. The elements of statisticallearning. New York: Springer; 2001.
43. Alpaydin E. Introduction to machine learning. Cambridge, MA: TheMIT Press; 2004.
44. Katz MH. Multivariable analysis: a practical guide for clinicians.Cambridge, UK: Cambridge University Press; 2006. 203 p.
45. Warach S. Measurement of the ischemic penumbra with MRI: it’sabout time. Stroke 2003;34:2533–2534.
46. Kidwell CS, Saver JL, Mattiello J, et al. Thrombolytic reversal ofacute human cerebral ischemic injury shown by diffusion/perfu-sion magnetic resonance imaging. Ann Neurol 2000;47:462–469.
47. Warach S. Tissue viability thresholds in acute stroke: the 4-factormodel. Stroke 2001;32:2460–2461.
846 Bristow et al.