Embed Size (px)
Citation preview

Alzheimer’s disease: Metals and the immune systemNEURODEGENERATION, Vol. 4, pp 107–111 (1995)
Hypothesis: is Alzheimer’s Disease a Metal-inducedImmune Disorder?
R.A. Armstrong,1 S.J. Winsper1 and J.A. Blair2
1Vision Sciences and 2Pharmaceutical and Biological Sciences, Aston University,Birmingham B4 7ET
A hypothesis that a metal-induced immune disorder may be involved in the pathogenesis of someforms of Alzheimer’s disease (AD) is presented. The classical complement pathway is activated inAD and T cells and reactive microglia appear in the brain. Studies of metal induced autoimmunityand the use of compounds containing aluminium as vaccine adjuvants suggest that metals canactivate complement and can be taken up by antigen presenting cells. The consequent immuneresponse could contribute to neuronal damage, β-amyloid deposition and cell death. The strengthsand weaknesses of this hypothesis are discussed and tests of some aspects are proposed.
Key words: Alzheimer’s disease, metals, aluminium, immune activation, majorhistocompatability locus antigens
107
THERE IS INCREASING evidence that a disorder of theimmune system is involved in the pathogenesis ofAlzheimer’s disease (AD) (Nandy, 1983; Rogers &Luber-Narod, 1988; McGeer et al., 1991). Complementproteins associated with the ‘classical’ pathway(McGeer et al., 1991), brain reactive antibodies (Nandy,1983), possibly immunoglobulins (Ishii & Haga, 1976;Eikelenboom & Stam, 1982), circulating immune com-plexes (CIC) in peripheral tissue and cerebral bloodvessels (Heinonen et al., 1993), helper/inducer andcytotoxic/suppressor T cells (McGeer et al., 1991) andabundant reactive microglia (McGeer et al., 1991) haveall been recorded in AD. Significant alterations in themajor histocompatibility locus (MHC) antigens havealso been demonstrated (Walford & Fortoul, 1983)suggesting either increased resistance or susceptibilityto an antigen in AD patients (Cohen et al., 1982;Henschke et al., 1978). These immune reactions couldbe a response to the pathological processes of AD.However, it is also possible that immune reactions toan environmental antigen could initiate such a patho-logical process. There is evidence that exposure tometals can induce an immune response in peripheral
tissues. First, mercury can induce antibodies againstrenal antigens and inhibit RT61 T-cells (Kosuda et al.,1993). Second, exposure to cobalt, aluminium (A1), tin,zirconium and beryllium has been associated withlung inflammatory disorders (Epstein et al., 1982, Kreisset al., 1993). Lymphocyte transformation, an increasein T cells and the development of a granulomatouspneumonitis are features of these disorders (Kreiss etal., 1993). Third, A1 phosphate and hydroxide are usedas vaccine adjuvants (Gupta et al., 1993), i.e. theyenhance the immune response to an antigen (Edelman,1980). Adjuvants containing A1 can activate comple-ment proteins (Ramanathan et al., 1979), prime helperT cells for IgE production (Kishimoto et al., 1973) andinduce antibody (Reiotella & Orasy, 1969). Since manymetals can be absorbed into the brain (Basun et al.,1991), it is possible that a metal-induced immuneactivation could occur in brain tissue and contribute tothe pathogenesis of AD. The objectives of this presentpaper are: (1) to propose a hypothesis describing howmetals could induce an immune response in AD; (2) toconsider its strengths and weaknesses and (3) to sug-gest studies to test aspects of the hypothesis.
Metals and an immune response
Of the metals that could be involved in an immuneresponse in AD, one possible candidate is A1. It oc-
Correspondence to: Dr R.A. ArmstrongReceived 11 March 1994; revised and accepted for publication 14
September 1994© 1995 Academic Press Limited1055-8330/95/010107 + 5 $08.00/0

R.A. Armstrong et al.
curs commonly in food and drinking water (Graves etal., 1990; Gregor, 1992; MAFF, 1993; Bowen et al.,1993), it can enter the brain and individual brain cells(Basun et al., 1991); Candy et al., 1992) and there isepidemiological (Martyn, 1992) and case control data(Graves et al., 1990; Neri and Hewitt, 1991) whichtogether suggest a possible link between A1 and AD.However, this line of evidence is extremely contro-versial and it is possible that other metals could beinvolved in AD. It has been established that metalions may induce: (1) antibodies against neuronal anti-gens (Kosuda et al., 1993), (2) complement factors(Ramanathan et al., 1979) or (3) a cellular immuneresponse (Sartvetnick & Fox, 1990). Sartvetnick andFox (1990) further suggest that the immune systemcan response to antigens expressed by the MHC path-way in non-immune cells. MHC-antigen complexeson the cell surface could then signal a T-cell response.For example, silver taken up into cells via transferrin(Tf) receptors results in the presence of CD41 T cells(McCoy et al., 1993). These are cells which recognizepeptide fragments taken up by macrophages and othercells. In addition, T-cell clones from patients withchronic beryllium disease are MHC class-II restrictedi.e. they only respond to beryllium when it is in asso-ciation with MHC class-II molecules on the surface ofantigen presenting cells (Richeldi et al., 1993). Hence,metals taken up into antigen presenting cells in thebrain could result in immune activation and death ofneurons.
The hypothesis
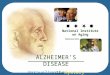
The essential features of the hypothesis are illustratedin Figure 1. An important aspect of the mechanism isthat metal ions like A1 enter brain cells and, in sus-ceptible individuals, are presented to the immunesystem via the MHC pathway.
First, entry into the cell could occur via Tf receptors(Roskams & Connor, 1990) although other methodsare possible. The density of Tf receptors is greatest inregions of high cortical pyramidal cell density, prob-ably reflecting the high use of iron by such cells (Pullenet al., 1990). However, it is probable that metals wouldalso enter other brain cells including microglia andcapillary endothelial cells. For example, A1 has beendetected inside membrane bound cytoplasmic inclu-sions within macrophages (Leininger et al., 1977), cellswhich share many of the same properties with brainmicroglia (Peress et al., 1993).
Second, we propose that metals are incorporatedinto the membranes of antigen presenting cells via theMHC pathway. This is unlikely to occur in neurons orastrocytes which do not express MHC antigens(McGeer et al., 1991) but could occur in microglia andcapillary endothelial cells which do express these an-tigens (McGeer et al., 1991). In support of this, signifi-cantly increased levels of MHC class II expressionhave been recorded in AD retinae principally due toinduced activity on endothelial cells (Liew et al., 1994).
Third, there is a cellular immune response result-ing in the production of CD41 T cells which mayinfiltrate the neuropil and cluster around antigen pre-senting cells.
Fourth, T cells release lymphokines e.g. interferon-gamma, which activate microglia (Weiss et al., 1993).
Fifth, activated microglia release free radicals in anoxidative attack which damages adjacent neurons.Activated microglia excrete large quantities of theunconjugated pterin neopterin, a marker of the cellu-
Figure 1. Hypothetical scheme of how a metal, e.g. Alu-minium (Al), could initiate the pathology of Alzheimer’sdisease by a metal-induced immune attack. Al-Tf 5 A1bound to transferrin; β/A4 5 β-amyloid peptide;CEC 5 Capillary endothelial cells; CMAC 5 Complementmembrane attack complex; CCC 5 Classical complementcascade; IFN-γ 5 Interferon-gamma; IL-1 5 Interleukin 1;MHC 5 Major histocompatibility complex; M 5 Microglia;A-M 5 Activated Microglia; N 5 Neuronal cell body;Ne 5 Neopterin; SP 5 Senile plaque.
108

Alzheimer’s disease: Metals and the immune system
lar immune response (Weiss et al., 1993; Armstrong etal., 1994). This immune attack could be exacerbatedby the presence of metal ions in pyramidal neuronswhich interfere with enzyme reactions. For example,A1 may interfere with cytoplasmic reactions whichemploy enzymes with Mg21 cofactors (Glick, 1990).Stimulation of the classical complement cascade cul-minating in the production of the ‘membrane attackcomplex’ (MAC) C5b-9 (Ramanathan et al., 1979) couldalso contribute to the immune response. It has re-cently been shown that in AD, neurons are attackedby MAC and attempt to resist the damage by internal-izing MAC fragments (Itagaki et al., 1994).
Sixth, these processes could increase the produc-tion of amyloid precursor protein (APP) and β-amyloid(β/A4) deposit due to loss of synaptic connectionsresulting from neuronal damage (Wallace et al., 1993).
Strengths and weaknesses of the hypothesis
The strengths of the present hypothesis are that itcould account of the following observations in AD:(1) the presence of immune activation in AD patients(McGeer et al., 1991; Heinonen et al., 1993; Armstronget al., 1994); (2) variations in MHC antigens in ADpatients (Walford & Fortoul, 1983); (3) the epidemio-logical evidence (Graves et al., 1990; Neri & Hewitt,1991; Martyn, 1992); (4) the production of excess APPand β/A4 deposits and (5) the association between b/A4 production and capillaries in the brain (Armstronget al., 1993). However, the hypothesis has a number ofweaknesses.
First, although there is evidence that metals enterbrain cells, the mechanism of entry into such cells hasnot been conclusively demonstrated. Although entryvia Tf receptors is possible (Roskams & Connor, 1990),other methods may also occur e.g. entry into glialcells could be via the haemopexin transport system.
Second, although a significant proportion of the A1which enters cells is found in the cytoplasm (Shi &Huang 1989; Dobson et al., 1993) it has not been dem-onstrated that A1 or any other metal can react withMHC proteins in human brain cells.
Third, there is no established link between varia-tions in MHC antigens in AD patients and suscepti-bility to metal-induced immunity.
Fourth, the hypothesis purposes that the immunereaction is a cause of the pathological ‘cascade’ in AD,i.e. it results in the production of β/A4. Against this,no association has been found between the presenceof A1 and β/A4 in chronic renal dialysis cases al-
though changes in tau protein did occur (Harringtonet al., 1994). However, we propose that such a linkwould only be seen in particular individuals whoseimmune system was susceptible to a particular metaland this may not be the case in such dialysis patients.In addition, the most obvious immune response ob-served in histological preparations is the presence ofmicroglia associated with mature β/A4 deposits inthe brain (Ohgami et al., 1991; Mann et al., 1992).Hence, an immune reaction could be a response to theproduction of APP or APP fragments in the brain.However, the later appearance of activated microgliadoes not preclude the possibility of an earlier im-mune response in which small numbers of T cells andmicroglia were present more locally in relation toglial or capillary endothelial cells. Diffuse β/A4 de-posits may not necessarily be associated with microgliaif the β/A4 is formed at synaptic terminals as a re-sponse to an immune attack on neuronal cells bodies.In addition, the earliest immune response could in-volve complement activation rather than a cellularimmune response.
Further studies
The most important question in relation to immunemechanisms in AD is whether an immune response isa cause or an effect of the pathological ‘cascade’ inAD. This could be studied in Down’s syndrome (DS)patients in whom the chronology of the pathologicalchanges in the brain has been well established (Mannet al., 1992) and in whom an immune response hasalso been detected (Hodgkins et al., 1993; Armstronget al., 1994). If a cellular immune response precedes β/A4 deposition in such patients then one would expectto see T cells infiltrating the neuropil close to bloodvessels and some activated microglia adjacent to neu-rons and capillary endothelial cells before the appear-ance of β/A4 deposits. In addition, markers of immuneactivation which include neopterin (Wachter, 1992;Weiss et al., 1993; Armstrong et al., 1994), tumournecrosis factor, complement factors, lymphokines andCIC (Heinonen et al., 1993) could be measured in theplasma of DS patients to determine at what age im-mune activation occurs relative to the appearance ofdiffuse β/A4 deposits. If immune markers like thesesuggest immune activation occurs after the appear-ance of β/A4, this would also argue against the hy-pothesis that a primary immune response initiates the‘pathological cascade’ in AD. The hypothesis wouldalso predict a relationship between immune markers
109

R.A. Armstrong et al.
and the concentration of metals in the body. Hence,the correlation between levels of immune markersand levels of metals bound to Tf or to low molecularweight species in the plasma (Hodgkins et al., 1993)could be studied. Studies of metal uptake intomicroglia and possible interactions between metals inthe cytoplasm and the MHC system should also bestudied. Epidemiological studies have not foundstrong correlations between A1 and AD and it is un-likely that further studies of this type would be usefulin testing the present hypothesis without taking intoaccount variations in MHC antigens in the popula-tion.
References
Armstrong RA (1993) The spatial patterns of β/A4 deposit subtypesand blood vessels in Alzheimer’s disease cases with pronouncedcongophilic angiopathy. Neurosci Res Commun 12:183–191
Armstrong RA, Cattell RJ, Jones SA, Winsper S, Blair JA (1994)Elevated urinary neopterin suggests immune activation inAlzheimer’s disease and Down’s syndrome. Neurosci ResCommun 14:63–69
Basun H, Forssell LG, Wellerberg L, Winblad B (1994) Metals andtrace elements in plasma and cerebrospinal fluid in normalageing and Alzheimer’s disease. J Neural Transm (P–D Sect)4:231–258
Bowen DJ, Gunn AM, Lacey RF, Itzhaki RF (1993) Aluminium indrinking water and Alzheimer’s disease-final report. Report FR0376, Foundation of Water Research
Candy JM, McArthur FK, Oakley AE, Taylor GA, Chen CPL,Mountfort SA, Thompson JE, Chalker PR, Bishop HE, BeyreutherK, Perry G, Ward MK, Martyn CN, Edwardson JA (1992) Alu-minium accumulation in relation to senile plaque andneurofibrillary tangle formation in the brains of patients withrenal failure. J Neurol Sci 107:210–218
Cohen D, Eisdorfer C, Walford R (1982) Histocompatibility anti-gens (HLA) and patterns of cognitive loss in dementia of theAlzheimer type. Neurobiol Aging 2:277–280
Dobson CB, Templer J, Day JP, Itzhaki RF (1993) Aluminium andAlzheimer’s disease: sites of aluminium-binding in humanneuroblastoma cells. Biochem Soc Trans 21:P32
Edelman R (1980) Vaccine adjuvants. Rev Inf Dis 2:370–383Eikelenboom P, Stam FC (1982) Immunoglobulin and complement
factors in senile plaques. Acta Neuropathol 57:239–242Epstein PE, Dauber JH, Rossman MD, Daniele RP (1982)
Bronchoalveolar lavage in a patient with chronic berylliosis:evidence for hypersensitivity pneumonitis. Ann Int Med 57:213–216
Glick JL (1990) Dementias: the role of magnesium deficiency and ahypothesis concerning the pathogenesis of Alzheimer’s disease.Med Hypoth 31:211–225
Graves AB, White E, Koepsell TD, Reitler BV, van Belle G, LarsonEB (1990) The association between aluminium containing prod-ucts and Alzheimer’s disease. J. Clin Epidemiol 43:35–44
Gregor JL (1992) Dietary and other sources of aluminium uptake.In: Aluminium in Biology and Medicine. Ciba Foundation Symp169:26–49. John Wiley, New York
Gupta RK, Relyveld EH, Lindblad EB, Bizzini B, Ben-Efraim S,Gupta KG (1993) Adjuvants — a balance between toxicity andadjuvanticity. Vaccine 11:293–306
Harrington CR, Wischik CM, McArthur FK, Taylor GA, EdwardsonJA, Candy JM (1994) Alzheimer’s disease-like changes in tauprotein processing: association with aluminium accumulationin brains of renal dialysis patients. Lancet 343:993–997
Heinonen O, Syrjanen S, Soininen H, Talasmenii S, Kaski M,Mantyjarvi R, Syrjanen K, Riekkinen P (1993) Circulating im-mune complexes in sera from patients with Alzheimer’s dis-ease, multi-infarct dementia and Down’s syndrome. NeurosciLett 149:67–70
Henschke PJ, Bell DA, Cape RDT (1978) Alzheimer’s disease andHLA: Tissue Antigens 12:132–135
Hodgkins PS, Prasher V, Farrar G, Armstrong RA, Sturman S,Corbett J, Blair JA (1993) Reduced transferrin binding in Down’ssyndrome: a route to senile plaque formation and dementia.NeuroReport 5:21–24
Ishii T, Haga S (1976) Immuno-electron microscopic localisation ofimmunoglobulins in amyloid fibrils of senile plaques. ActaNeuropathol 20:372–378
Itagaki S, Akiyama H, Saito H, McGeer PL (1994) Ultrastructurallocalisation of complement membrane attack complex (MAC)-like immunoreactivity in brains of patients with Alzheimer’sdisease. Brain Res 645:78–84
Kishimoto T, Ishizaka K (1973) Regulation of antibody response invitro VI. Carrier-specific helper cells for IgG and IgF antibodyresponses. J Immunol 111:720–732
Kosuda LL, Greiner DL, Bigazzi PE (1993) Mercury-induced renalautoimmunity: changes in RT61 T-lymphocytes of susceptibleand resistant rats. Environ Health Perspect 101:178–185
Kreiss K, Wasserman S, Mroz MM, Newman LS (1993) Berylliumdisease screening in the ceramic industry.
Leininger JR, Farrell RL, Johnson GR (1977) Acute lung lesions dueto zirconium and aluminium compounds in hamsters. ArchPathol Lab Med 101:543–549
Liew SCK, Penfold PL, Provis JM, Madigan MC, Billson FA (1994)Modulation of MHC class II expression in the absence oflymphocytic infiltrates in Alzheimer’s retinae. J Neuropath expNeurol 53:150–157
MAFF (1993) Aluminium in food. 39th report, London, HMSOMann DMA, Younis N, Jones D, Stoddart RW (1992) The time
course of the pathological events in Down’s syndrome withparticular reference to the involvement of microglial cells anddeposits of β/A4. Neurodegen 1:201–205
Martyn CN (1992) The epidemiology of Alzheimer’s disease inrelation to aluminium. Ciba Foundation Symp 169:69–79
McCoy KL, Noone M, Inman JK, Stutzman R (1993) Exogenousantigens internalized through transferrin receptors activateCD41 T cells. J Immunol 150:1691–1704
McGeer PL, McGeer EG, Kawamata T, Yamada T, Akiyama H(1991) Reactions of the immune system in chronic degenerativeneurological diseases. Can J Neurol Sci 18:376–379
Nandy K (1983) Immunologic factors. In: Reisberg B (ed).Alzheimer’s disease. The standard reference. Macmillan, Lon-don and New York, pp.135–138
Neri LC, Hewitt D (1991) Aluminium, Alzheimer’s disease anddrinking water. Lancet 338:390
Ohgami T, Kitamoto T, Shin RW, Kaneko Y, Ogomori K, Tateishi J(1991) Increased senile plaques without microglia in Alzheimer’sdisease. Acta Neuropathol 81:242–247
Peress NS, Fleit HB, Perillo E, Kuljis R, Pezzullo C (1993) Identifica-tion of Fc R1, 11 and 111 on normal human brain ramifiedmicroglia and on microglia in senile plaques in Alzheimer’sdisease. J Neuroimmunol 48:71–80
Pullen RGL, Candy JM, Morris CM, Taylor G, Keith AB, EdwardsonJA (1990) Gallium 67 as a potential marker for aluminium trans-port in the rat brain: implications for Alzheimer’s disease. JNeurochem 55, 251–259
Ramanathan VD, Badenoch-Jones P, Turk JL (1979) Complementactivation by aluminium and zirconium compounds. Immunol37:881–888
110

Alzheimer’s disease: Metals and the immune system
Reiotella R, Orasy Z (1969) Reagenic antibody production in differ-ent mouse strains. Immunol 17:45–54
Richeldi L, Sorrentino R, Saltini C (1993) HLA-DPB1 glutamate 69:A genetic marker of beryllium disease. Science 262:242–244
Rogers J, Luber-Narod J (1988) Immune actions in nervous system:brief review with special emphasis on Alzheimer’s disease.Drug Dev Res 15:227–235
Roskams AJ, Connor JR (1990) Aluminium access to the brain: arole for transferrin and its receptor. Proc Natl Acad Sci USA87:9024–9027
Sarvetnick N, Fox HS (1990) Interferon-gamma and the sexualdimorphism of auto-immunity. Mol Biol Med 7: 323–331
Shi B, Huang A (1989) Aluminium uptake by neuroblastoma cells. JNeurochem 28:3911–3915
Wachter H, Fuchs S, Hausen A, Reibnegger G, Weiss G, Werner
ER, Werner-Felmayer G (1992) Neopterin: Biochemistry,Methods, Clinical Application. Walter de Gruyter, Berlin andNew York
Walford RL, Fortoul T (1983) Histocompatibility locus antigens inAlzheimer’s disease. In: Reisberg B (ed). Alzheimer’s disease.The standard reference, Macmillan, London and New York,pp.166–169
Wallace W, Ahlers ST, Gotlib J, Bragin V, Sugar J, Gluck R, Shea PA,Davis KL, Haroutunian V (1993) Amyloid precursor protein inthe cerebral cortex is rapidly and persistently induced by loss ofsubcortical innervation. Proc Natl Acad Sci USA 90:8712–8716
Weiss G, Fuchs D, Hausen A, Reibnegger G, Werner ER, Werner-Felmayer G, Semenitz E, Dierich MP, Wachter H (1993)Neopterin modulates toxicity mediated by reactive oxygen andchloride species. FEBS 321:89–92
111