Embed Size (px)
Citation preview

Epilepsy Research (2015) 109, 9—12
jo ur nal ho me p ag e: www.elsev ier .com/ locate /ep i lepsyres
SHORT COMMUNICATION
How long is long enough? The utility ofprolonged inpatient video EEG monitoring
Brian D. Moseleya,∗, Sandra Dewarb,1, Zulfi Haneefc,2,John M. Sternb,1
a Department of Neurology and Rehabilitation Medicine, University of Cincinnati, Cincinnati, OH, USAb Department of Neurology, David Geffen School of Medicine at UCLA, Los Angeles, CA, USAc Department of Neurology, Baylor College of Medicine, Houston, TX, USA
Received 19 September 2014; accepted 23 October 2014Available online 28 October 2014
KEYWORDSEpilepsy monitoring;Length of stay;Resource allocation;Epilepsy surgery;PNES
Summary Video EEG monitoring (VEM) is a valuable tool for the diagnosis of epileptic seizures(ES) and psychogenic nonepileptic seizures (PNES). We sought to determine the benefits ofprolonged length of stay (LOS). We retrospectively reviewed the records of patients admittedfor VEM. We analyzed LOS for ES and PNES patients to determine if there was reduced utility,as evidenced by a significantly higher inconclusive outcome, beyond a certain duration. Wecalculated receiver operating characteristic (ROC) curves to determine optimal cut off pointsfor LOS based on futility. Patients admitted with presumed PNES were significantly more likelyto have an inconclusive admission (31/150, 20.7%) versus all others (58/446, 13%, p = 0.033).There was no significant difference in the likelihood of having an inconclusive admission ifmonitoring was continued for any duration in patients with ES (area under curve, AUC, 0.46).For patients with PNES, a LOS ≥5 days was associated with an increased risk of the stay being
inconclusive (28% versus 12.5%, p = 0.026). Although the ROC curve suggested a cut off of 5.5days, it did not predict outcomes well (AUC 0.52, sensitivity 0.55, specificity 0.5). Based on ourdata, prolonging VEM appears useful for the proper classification and localization of ES.© 2014 Elsevier B.V. All rights reserved.∗ Corresponding author at: 260 Stetson Street, Suite 2300, Cincinnati,
E-mail addresses: [email protected] (B.D. Moseley), [email protected] (J.M. Stern).
1 Address: 710 Westwood Plaza, Suite 1250, Los Angeles, CA 90095, US2 Address: One Baylor Plaza, MS: NB302, Houston, TX 77030, USA. Tel.:
http://dx.doi.org/10.1016/j.eplepsyres.2014.10.0110920-1211/© 2014 Elsevier B.V. All rights reserved.
OH 45267-0525, USA. Tel.: +1 513 558 5440; fax: +1 513 558 [email protected] (S. Dewar), [email protected] (Z. Haneef),
A. Tel.: +1 3108255745; fax: +1 310 206 8461. +1 832 355 4044; fax: +1 713 798 0984.

10 B.D. Moseley et al.
F term( ientsp
I
Vtt(AbtiidoaTnrs
iacb(caiSt2
bccttmcerpsw
M
WpgpofLbsd
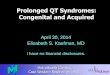
igure 1 Receiver operating characteristic curves used to deA) All patients, regardless of preadmission hypothesis. (B) Patsychogenic nonepileptic seizures.
ntroduction
ideo electroencephalographic (EEG) monitoring (VEM) ishe definitive tool for the evaluation of uncontrolled epilep-ic seizures (ES) and psychogenic nonepileptic seizuresPNES). Following passage of the Patient Protection andffordable Health Care Act, it is anticipated that larger num-ers of patients across the United States will have accesso this essential diagnostic tool. Although invaluable, VEMs not without shortcomings. Chief amongst these are thatt is resource intensive and that seizure occurrence is sel-om predictable. VEM requires a considerable investmentf patient and physician time, consumes hospital resources,nd is major cost to payers (Ghougassian et al., 2004).hese shortcomings must be balanced with the costs ofot performing VEM, including more frequent emergencyoom visits, lost time at work/school secondary to recurrenteizures, and ineffective prescription drug use.
The average length of stay (LOS) in an epilepsy monitor-ng unit (EMU) has previously been reported as 3—4 days fordults, with shorter durations of 1.2—1.5 days reported forhildren (Nordli, 2006). The duration has been reported toe longer for ES patients undergoing a presurgical workupmean 3.5 days) versus PNES patients admitted for spelllassification (2.4 or less days) (Lobello et al., 2006; Alvingnd Beniczky, 2009; Woollacott et al., 2010). However, it
s not uncommon for VEM durations to go beyond 3 days.ome have even reported that it is not rare for such moni-oring to continue beyond one week (Friedman and Hirsch,009). Some EMU stays are extended beyond those durationspsth
ine optimal cut off points for length of stay based on futility. with presumed epileptic seizures. (C) Patients with presumed
ecause a sufficient number of seizures/spells have not beenaptured to make a definitive diagnosis. Although there isonsensus on the need to capture all habitual seizure/spellypes to make a conclusive diagnosis (Shafer et al., 2012),here is no consensus on the maximum required duration ofonitoring to achieve that goal. Given the changing health-
are landscape and need to use resources wisely (Lakhant al., 2013), this question is likely to become increasinglyelevant. Accordingly, we sought to determine the utility ofrolonged LOS in patients with presumed ES and PNES. Wepecifically questioned whether there was a time point athich continued VEM was rendered diagnostically futile.
ethods
e retrospectively reviewed the medical records of allatients admitted to the adult EMU at the Ronald Rea-an UCLA Medical Center between 1/2004 and 12/2008. Allatients underwent scalp VEM for classification/localizationf medication resistant seizures/spells. Data abstractedrom the medical records included reason for admission,OS, and discharge diagnosis. The reason for admission wasased on the admitting epileptologist’s diagnostic impres-ion from the initial outpatient evaluation. A dischargeiagnosis of inconclusive was assigned when none of a
atient’s habitual seizures/spells occurred during the admis-ion. Patients who did not experience the full repertoire ofheir habitual spells/seizures prior to discharge (i.e. onlyad some of their habitual spells/seizures or atypical spells)
11
Chan
ces
of
inco
nclu
sive
adm
issi
ons
in
pati
ents
wit
h
prol
onge
d
EMU
stay
s.
All p
atie
nts
(n
=
596)
Pati
ents
wit
h pr
esum
ed
ES
(n
=
333)
Pati
ents
wit
h
pres
umed
PNES
(n
=
150)
ersu
s
≤3
days
68/4
89
(13.
9%)
vers
us
21/1
07
(25.
2%),
p
=
0.14
25/3
03
(8.3
%)
vers
us
4/30
(13.
3%),
p
=
0.31
24/1
04
(23.
1%)
vers
us
7/46
(15.
2%),
p
=
0.38
ersu
s
≤4
days
62/4
28
(14.
5%)
vers
us
27/1
68
(16.
1%),
p
=
0.61
23/2
83
(8.1
%)
vers
us
6/50
(12%
),
p
=
0.41
22/7
8
(28.
2%)
vers
us
9/72
(12.
5%),
p
=
0.02
6*er
sus
≤5
days
55/3
72
(14.
8%)
vers
us
34/2
24
(15.
2%),
p
=
0.91
20/2
49
(8%)
vers
us
9/84
(10.
7%),
p
=
0.5
19/6
5
(29.
2%)
vers
us
12/8
5
(14.
1%),
p
=
0.02
7*er
sus
≤6
days
41/2
96
(13.
9%)
vers
us
48/3
00
(16%
),
p
=
0.49
16/2
04
(7.8
%)
vers
us
13/1
29
(10.
1%),
p
=
0.55
11/4
3
(25.
6%)
vers
us
20/1
07
(18.
7%),
p
=
0.38
ersu
s
≤7
days
33/2
31
(14.
3%)
vers
us
56/3
65
(15.
3%),
p
= 0.
8112
/166
(7.2
%)
vers
us
17/1
67
(10.
2%),
p
=
0.44
10/3
2
(31.
3%)
vers
us
21/1
18
(17.
8%),
p
=
0.14
ersu
s
≤
8
days
26/1
79
(14.
5%)
vers
us
63/4
17
(15.
1%),
p =
0.9
11/1
28
(8.6
%)
vers
us
18/2
05
(8.8
%),
p
=
18/
27
(29.
6%)
vers
us
23/1
23
(18.
7%),
p
=
0.2
vers
us
≤9
days
22/1
45
(15.
2%)
vers
us
67/4
51
(14.
9%),
p =
0.89
9/10
4
(8.7
%)
vers
us
20/2
29
(8.7
%),
p
=
1
7/21
(33.
3%)
vers
us
24/1
29
(18.
6%),
p
=
0.15
,
epile
psy
mon
itor
ing
unit
;
ES,
epile
ptic
seiz
ures
;
LOS,
leng
th
of
stay
;
PNES
,
psyc
hoge
nic
none
pile
ptic
seiz
ures
.
Utility of prolonged inpatient video EEG monitoring
were also given an inconclusive diagnosis. For patients hav-ing more than one admission during the study period, onlythe first admission was analyzed.
We systematically analyzed LOS to discover significantdifferences in the rates of inconclusive admissions for staysexceeding specific limits. We utilized chi-square analysis(Fisher’s Exact Test, 2 sided), with p-values <0.05 consideredstatistically significant. We subsequently calculated receiveroperating characteristic (ROC) curves to determine poten-tial cut off points for LOS based on futility. All data entry andstatistical analysis were performed using IBM SPSS StatisticsVersion 19 (IBM, Armonk, NY, U.S.A.).
The protocol was approved by the UCLA InstitutionalReview Board (IRB).
Results
Five hundred ninety six patients were admitted for VEMduring the study period. The majority of patients (333,55.9%) were admitted for an epilepsy surgery evaluationwith presumed ES. The remaining patients were admittedfor differential diagnosis of presumed PNES (150, 25.2%) orspells of presumed other, nonepileptic etiology (113, 19%).At discharge, only 89/596 admissions (14.9%) were inconclu-sive. However, patients admitted for differential diagnosisof presumed PNES were significantly more likely to havean inconclusive admission (31/150, 20.7%) compared to allothers (58/446, 13%, p = 0.03).
When examining all patients together, there was no sig-nificant difference in the likelihood of having an inconclusiveadmission if monitoring was continued for any duration. Thecutoffs analyzed were for progressive LOSs between 4 and10 days (Table 1). The ROC curve calculated for all patientsindicated LOS did not predict futility (area under curve 0.48,standard error 0.034, asymptotic sig. 0.6, Fig. 1). The samewas true when analysis was limited to patients admittedwith presumed ES (Table 1). The ROC curve calculated for ESpatients indicated a similar inability of LOS to predict futil-ity (area under curve 0.46, standard error 0.059, asymptoticsig. 0.46, Fig. 1). For patients admitted with presumed PNES,a LOS ≥5 days was associated with an increased possibilityof the stay being inconclusive (p = 0.026). This continued tobe significant when LOSs ≥6 days were examined (p = 0.027).However, it was no longer significant when LOSs ranging from≥7 days to ≥10 days were examined (Table 1). Although theROC curve suggested a possible cut off of 5.5 days (sensi-tivity 0.55, specificity 0.5), it did not predict outcomes well(area under curve 0.52, standard error 0.066, asymptoticsig. 0.767, Fig. 1).
Discussion
Our results support the effectiveness and high efficacyof VEM. At our institution, over 85% of admissions werediagnostic, with less than 15% being inconclusive. Suchdata compares favorably to inconclusive rates of 15—38%reported in previous studies (Ghougassian et al., 2004;
Benbadis et al., 2004; Noe and Drazkowski, 2009). The valueof such monitoring is apparent when considering the poten-tial consequences of misdiagnosis. At epilepsy centers, it isestimated that up to 30% of PNES patients who have not hadTabl
e
1
LOS
≥4
days
v≥5
days
v≥6
days
v≥7
days
v≥8
days
v≥9
days
v≥1
0
days
Keys
:
EMU

1
VScalm(ib
pdcppiiwpsr$qmdntr
egwdTwwtcwaoeaWlls
A
Tp
R
A
B
B
B
B
F
G
L
L
N
N
N
R
S
Behav. 25, 449—456.Woollacott, I.O., Scott, C., Fish, D.R., Smith, S.M., Walker, M.C.,
2010. When do psychogenic nonepileptic seizures occur on avideo/EEG telemetry unit? Epilepsy Behav. 17, 228—235.
2
EM are erroneously diagnosed with ES (Benbadis, 2007).uch errors have the potential to expose patients to theonsequences and costs of unnecessary and non-therapeuticntiseizure drugs and emergency department visits. Theonger this misdiagnosis persists, the harder it may be to ulti-ately treat PNES once the correct diagnosis is established
Bodde et al., 2009). Support for VEM is justified consider-ng that the annual cost of misdiagnosis is estimated to beetween $650 million and $4 billion (Nowack, 1997).
The literature has previously been sparse on data sup-orting prolonged stays (Friedman and Hirsch, 2009). Ourata strongly suggests that prolonging VEM for the properlassification and localization of ES is appropriate. When ESatients whose hospitalizations lasted ≥5 days were com-ared to those with LOSs ≤4 days, no significant differencesn the rates of inconclusive admissions could be found. VEMs an integral test for patients with drug resistant epilepsyho are being considered for resective epilepsy surgery, androlonged VEM is justifiable on the basis of utility. Canadiantudies have shown such monitoring and resulting surgeryesult in an incremental cost-effectiveness ratio of $25,020-69,451 Canadian dollars ($24,019—$66,673 US dollars) peruality-adjusted life years (QALYs) (Bowen et al., 2012). Itay be more cost effective to keep such patients the extraays required to record additional seizures than to termi-ate EMU stays earlier and readmit at a later date. If the lat-er is done, it is possible such patients will only end up beingeadmitted for an overall longer duration and total cost.
We discovered that prolonged LOS may be of greater ben-fit to patients with presumed ES versus PNES. Our data sug-est there may be a dichotomy of patients with PNES: someho have typical spells soon after admission and others whoo not have their typical spells, even with prolonged VEM.his is consistent with the observation that many patientsith PNES have a shorter time to first seizure versus patientsith ES (Rose et al., 2003; Alving and Beniczky, 2009). Given
he need to use healthcare resources wisely and efficiently,are providers should consider the utility of prolonging VEMhen seizures/spells have not occurred. There is consider-ble challenge in managing an EMU, with the expectationf achieving safe and successful outcomes in patients withpisodic and unpredictable medical conditions. To managen elective service successfully, LOS needs to be controlled.hen faced with dwindling EMU resources, recognizing the
ikely diagnosis may prove useful. Although decisions willikely need to be individualized, our results suggest at leastome weight be given to the presumed etiology.
cknowledgements
he authors have no acknowledgements. No outside/thirdarty funding was utilized for this study.
B.D. Moseley et al.
eferences
lving, J., Beniczky, S., 2009. Diagnostic usefulness and durationof the inpatient long-term video-EEG monitoring: findings inpatients extensively investigated before the monitoring. Seizure18, 470—473.
enbadis, S.R., 2007. Errors in EEGs and the misdiagnosis ofepilepsy: importance, causes, consequences, and proposedremedies. Epilepsy Behav. 11, 257—262.
enbadis, S.R., O’Neill, E., Tatum, W.O., Heriaud, L., 2004. Out-come of prolonged video-EEG monitoring at a typical referralepilepsy center. Epilepsia 45, 1150—1153.
odde, N.M., Brooks, J.L., Baker, G.A., Boon, P.A., Hendrik-sen, J.G., Mulder, O.G., Aldenkamp, A.P., 2009. Psychogenicnon-epileptic seizures — definition, etiology, treatment andprognostic issues: a critical review. Seizure 18, 543—553.
owen, J.M., Snead, O.C., Chandra, K., Blackhouse, G., Goeree, R.,2012. Epilepsy care in ontario: an economic analysis of increasingaccess to epilepsy surgery. Ont. Health Technol. Assess. Ser. 12,1—41.
riedman, D.E., Hirsch, L.J., 2009. How long does it take to makean accurate diagnosis in an epilepsy monitoring unit. J. Clin.Neurophysiol. 26, 213—217.
hougassian, D.F., d’Souza, W., Cook, M.J., O’Brien, T.J., 2004.Evaluating the utility of inpatient video-EEG monitoring. Epilep-sia 45, 928—932.
akhan, S.E., Ebied, A.M., Tepper, D., Nguyen, T., 2013. The historyof reimbursements in neurology. Front. Neurol. 4, 171.
obello, K., Morgenlander, J.C., Radtke, R.A., Bushnell, C.D., 2006.Video/EEG monitoring in the evaluation of paroxysmal behav-ioral events: duration, effectiveness, and limitations. EpilepsyBehav. 8, 261—266.
oe, K.H., Drazkowski, J.F., 2009. Safety of long-term video-electroencephalographic monitoring for evaluation of epilepsy.Mayo Clin. Proc. 84, 495—500.
ordli Jr., D.R., 2006. Usefulness of video-EEG monitoring. Epilepsia47 (suppl. 1), 26—30.
owack, W.J., 1997. Epilepsy: a costly misdiagnosis. Clin. Elec-troencephalogr. 28, 225—228.
ose, A.B., McCabe, P.H., Gilliam, F.G., Smith, B.J., Boggs, J.G.,Ficker, D.M., Moore, J.L., Passaro, E.A., Bazil, C.W., Consortiumfor Research in Epilepsy, 2003. Occurrence of seizure clustersand status epilepticus during inpatient video-EEG monitoring.Neurology 60, 975—978.
hafer, P.O., Buelow, J.M., Noe, K., Shinnar, R., Dewar, S., Levi-sohn, P.M., Dean, P., Ficker, D., Pugh, M.J., Barkley, G.L., 2012.A consensus-based approach to patient safety in epilepsy moni-toring units: recommendations for preferred practices. Epilepsy