Embed Size (px)
Citation preview

Hereditary Nonpolyposis Colorectal Cancer (Lynch Syndromes I and 11)
11. Biomarker Studies
HENRY T. LYNCH. MD,' GUY S. SCHUELKE, PHD; WILLIAM J. KIMBERLING, PHD,? WILLIAM A. ALBANO, MD,* JANE F. LYNCH, BSN,' KAREN A. BISCONE, BSN,'
MARTIN L. LIPKIN, MD,§ ELEANOR E. DESCHNER, PHD.11 YVES B. MIKOL, P H D , ~ AVERY A. SANDBERG, MD,I ROBERT C. ELSTON, PHD,#
JOAN E. BAILEY-WILSON, PHD,# AND B. SHANNON DANES, MD, PHD'.
Nine families with the cancer family syndrome (CFS), or Lynch syndrome 11, and two with hereditary site-specific colonic cancer (HSSCC), or Lynch syndrome I, were investigated for the following potential biomarkers of genotype status: (1) in ritro tetraploidy of dermal fibroblast monolayer cultures; (2) tritiated thymidine uptake ('HdThd) labeling of colonic mucosa; (3) cytogenetics of peripheral blood mononuclear leukocytes; (4) quantitative serum immunoglobulin determinations; (5) methionine depen- dence in dermal fibroblasts in tissue culture; (6) segregation analysis; and (7) the study of gene linkage with respect to 25 landmark serum and blood group markers. Positive lod scores of 3.19 for linkage of the J k (Kidd blood group) with CFS were obtained. Both in vitro tetraploidy and 'HdThd uptake in the distal colonic mucosal crypt compartments were positively associated with cancer risk status in CFS and HSSCC kindreds. There was a high incidence of polymorphisms of centromeric heterochromatin, including complete inversion. These findings are of particular clinical and genetic significance because HNPCC lacks premonitory signs of cancer risk. If confirmed, they could conceivably enable definition of genotype as early as birth in members of HNPCC kindreds, thereby epabling psychologic preparation and intensive cancer education for improved compliance in surveillance/management programs. These studies also provide new clues about the chromosome(s) bearing the presumed cancer gene(s). For example, CFS gene(s) may possibly be located on chromosome 2, where J k is located. These biomarkers merit intensive study in additional HNPCC kindreds for a more complete assessment of their sensitivity and specificity. Additionally, essential aspects of previous reports involving biologic samples from these and/or similar subject kindreds are included to permit a comprehensive presentation of the combined findings of this consortium to date.
Cuncer 56:939-951, 1985.
HE HEREDITARY nonpolyposis colorectal cancer T (HNPCC) syndromes include the cancer family syndrome (CFS) and hereditary site-specific colon cancer (HSSCC), both of which lack premonitory signs for identification of gene camer status. It is therefore ex-
From the Departments of *Preventive Medicine/Public Health, +Department of Otolaryngology, #Department of Surgery, Creighton University School of Medicine and the Hereditary Cancer Institute, Omaha, Nebraska, the BLaboratory of Gastrointestinal Cancer Research, 11 Laboratory of Digestive Tract Carcinogenesis, Memorial Sloan-Ket- tering Cancer Center, New York, New York, the TDepartments of Medicine and Genetics, Roswell Park Memorial Institute, Buffalo, New York. the #Department of Biometry, Louisiana State University Medical Center, New Orleans, Louisiana, and the **Laboratory for Cell Biology, Department of Medicine, Cornell University Medical College, New York, New York.
Supported by NCI Grant #5 ROI-CA 27831-03 and 5 ROI-CA 28 198-05.
Accepted for publication September 4, 1984.
tremely important that biomarkers be investigated that might enable genotype camer identification before phe- notypic expression (clinical cancer).
This report describes biomarker findings that show variable association with the cancer-prone genotype in patients with HNPCC (Lynch syndromes I and 11). The following topics will be discussed: (1) in vitro tetraploidy of dermal fibroblast monolayer cultures'; (2) tritiated thymidine (3HdThd) labeling in flat colonic epithelium24; (3) cytogenetics of peripheral blood mononuclear leu- kocyte$; (4) quantitative serum immunoglobulin deter- mination$; ( 5 ) methionine dependence (MD) of dermal fibroblast monolayer cultures, which is a characteristic of transformed cell lines'; (6) segregation analyses; (7) study of gene linkage using 25 landmark serum and blood group markers'; and (8) a literature review of potential biomarker associations in these disorders.
939

940 CANCER August 15 1985 Vol. 56
Methods
Patients
Patient ascertainment and sampling on the clinical resource was performed as discussed in detail in the companion article (Part I). Because of practical con- straints, it was not always possible to perform all potential biomarker tests on all members of the kindreds investi- gated. Thus, a total of 597 patients were sampled for potential biomarkers. Investigated were a total of 326 from 1 1 kindreds for tetraploidy, 297 from 1 1 kindreds and 31 normal controls for 3HdThd uptake by colonic mucosa, 116 from 4 kindreds for serum immunoglobulin determinations, 44 from 4 kindreds for chromosomal analysis, and 21 from 4 kindreds for methionine depen- dency. Samples for all assays were assigned code numbers to assure that all studies were totally blind.
In Vitro Tetraploidy
Establishment of dermal jibroblast monolayer cultures: After carefully cleaning of the patient's skin with ethanol, a split-thickness biopsy specimen was taken from the axillary area of the arm with a sterile scalpel. Skin biopsy specimens from all 1 I families were obtained from each affected subject studied, first- and/or key second-degree relatives (from families of the affecteds), as well as from family members by marriage (considered not to be at risk for CFS or HSSCC).
Dermal fibroblast monolayer cultures were established from these split-thickness biopsy specimens by standard culture methods.' Cultures were grown in sterile plastic petri dishes (28 cm2 growth area) in Eagle's minimum essential medium (MEM) with 25% (volume) fetal bovine serum in an atmosphere of 5% C 0 2 in air. The pH of the medium was kept between 7.0 and 7.4 during the culture period. After 2 culture weeks, the initial explant culture was examined to determine that a zone of cellular migration surrounding the initial explant was present and then the culture was trypsinized to obtain a monolayer culture. The cells were grown in culture for 8 to 15 weeks (3-6 subcultures by trypsinization) before in vitro studies were done.
Occurrence of in vitro tetraploidy: For studies on tetraploidy in dermal fibroblast monolayer cultures, cells were trypsinized into suspension and approximately I O4 cells suspended in 5 ml medium, inoculated into sterile plastic petri dishes, and incubated in an atmosphere of 5% C 0 2 in air." Forty-eight hours later, when a burst of mitoses was observed, chromosome preparations were stained in aceto-orcein. The percent of tetraploidy was based on the number of metaphases showing tetraploidy divided by the total number scored blind on slides having at least 100 divisions per slide. For each line
established, the Occurrence of tetraploidy was determined after 2 and 4 months of continuous culture growth.
Sensitivity and specificity: Altered biologic properties have been considered to be in vitro expressions of cancer-prone gene(s) in dermal fibroblast monolayer cultures derived from individuals with a genotype for some autosomal dominant cancer syndromes.' In order to evaluate any such alteration as an in vitro gene expression, its discriminating capacity (sensitivity and specificity) must be evaluated. Such an evaluation was done for aberrant chromosome complement, increased in vitro tetraploidy, in the CFS and HSSCC families.
Tririared Thymidine Labeling of' Colonic Epithelial Cells
Details of methods for investigation of 'HdThd label- ing have been previously published." These studies detect DNA synthesis in cells at all levels of the colonic crypts, although normally S-phase cells only occur in the lower two thirds of the glands." Multiple analytical approaches were employed for evaluation of the 'HdThd findings. These included: comparison of labeling distri- butions between high- and low-risk populations, the classification of individuals based upon the 'HdThd labeling distributions, and the presence or absence of a shift of the major zone of DNA synthesis from the base (normal condition) to the middle and upper one third of crypts (abnormal condition). Abnormal distributions of labeled cells have been observed in colonic crypts of patients with colon cancer," familial polyposis coli patients.I3 and 1,2-dimethylhydrazine-treated mice.'4
Segregation A nalysis
All I 1 kindreds were used in the segregation analysis of in vitro tetraploidy. Of the 2762 individuals in these kindreds, 316 were measured for this trait. Data for segregation analysis of a shift of the major zone for 'HdThd uptake in colonic crypts and uptake in 1 1 crypt divisions were only available for a subset of these families (C- 197, C- 199, C- 1 15, JFLSO, C- 164, C- 196, C- 200, and C-OO 1, with 1 18 individuals measured for the shift of the major zone for 'HdThd uptake in colonic crypts; and families C- 197, C- 199, C- 1 15, C- 198, C- 196, C-200, and C-001, with 88 individuals measured for 'HdThd uptake in 1 1 crypt divisions).
The families were ascertained because of the presence of multiple cases of nonpolyposis colorectal cancer, each family having a proband (index case) identified. In an attempt to partially allow for the mode of ascertainment, all likelihoods in the segregation analysis were condi- tioned on the phenotypes of the index cases. However, in many instances, the tetraploidy and 'HdThd uptake values of the index cases were not measured, so that

No. 4 GENETICS, COLON CANCER, AND BIOMARKERS Lynch et a/. 94 1
I ( 1' 2 3
7 8
t l 14 1s
)t 9 10
4
f t 4 4 !. 20 21 22
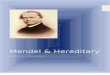
FIG. I . Normal (diploid) G-banded karyotype of a female family member (46, XX).
,e 5
1; 12
x x
this conditioning was not possible in some families. For each of the three traits, the segregation analyses, which are preliminary in nature, were performed on the trait converted into a dichotomy, using the general transmis- sion probability model, Is allowing for partial penetrance of each genotype; these penetrances were also allowed to be linear and quadratic exponential functions of age (but always being constrained to lie between 0 and 1). Three maximum likelihoods were calculated for each trait: ( 1 ) with the transmission probabilities constrained to be Mendelian; (2) with the transmission probabilities constrained to be equal: and (3) under the unrestricted model of arbitrary (but between 0 and 1) transmission probabilities. Each of the first two likelihoods was com- pared with the third likelihood to obtain an asymptotic chi-square test of significance.
Gene Linkage Gene marker determinations were performed on in-
formative members in the kindreds. The markers typed were ABO, Rh, MNS, Kell, Fy, Jk, Le, Se, Di (in only the one American Indian kindred), Gm, Km, Hapt, C3, Bf, Gc, Pi, Tnf, PGM,, ACP, EsD, AK, PGD, ADA,
GLO, and GPT. Linkage analysis was done using the LIPED linkage
Linkage analysis was done on colon/endometrium phenotype cancer. For cancer, indivi'duals were consid- ered affected if they were affected with colon and/or endometrial cancer. Genotypic probabilities of HNPCC for each unaffected individual in the pedigree were calculated assuming HNPCC to be a rare autosomal dominant gene with no sporadic cases and using a mean age of onset of 45 years with a standard deviation of I 1 years. A normal distribution for age of onset was as- sumed.
Cylogenet ics
Heparinized blood was shipped to Dr. Sandberg's laboratory from the various locations within less than 24 hours after sample procurement. The leukocytes were cultured with PHA (phytohemagglutinin) for 72 hours, harvested, and prepared for chromosome analysis by established methods.' G- (Fig. 1 ) and C-banding was performed on each specimen; 25 metaphases were ana- lyzed by C-banding and 15 metaphases by G-banding.

942 CANCER August I S 1985 Vol. 56
TABLE I . Occurrence of Increased In Virro Tetraploidy in Dermal Fibroblast Monolayer Cultures in Hereditary
- Nonpolyposis Colorectal Cancer Kindreds
Clinically atTected At risk Not at risk Increased in vifro Tetraploidyt Increased in v i m tetraploidy* Increased in vifro tetraploidyt
F _ _ _ - M F M F M
Family Age + - Age + - Age + - Age + - Age + - Age + -
C-OOI JFL5O c-I15 C-25 I C- I64 C- I96 C- 197 C-198 C- I99 c-200 c-220
53-79 2 1 64-85
41-73 24-54 2 1 38-55
44 58 62
51 I 66 52 I 57 28 1 40-52
3
4 3 1 1 1 1 I
3
15-68 10-43 15-72 14-62 10-77 22-39
34 27-69 21-66 18-33 16-48
2 15 2 4 2 4 7 6 5 6
5 I 4 2
3 6 1 7
15-72 11-72 20-52 15-4 I I 1-52 20-6 1 14-63 28-63
31 17-54 14-57
2 21 6 7 3 2 6 16 2 6 3 I I
5 2 5
I 2 10 4 2
24-69 31-70 55-73
2 13-62 59-73 23-65 26-64
71 57
29-67 32-5 1
10 3 3
6 5 3
1 3 3 I 1 5 2
26-65 37-60 37-53 22-50 30-60 26-64 32-57 30-54
29 49-73 20-57
I $ 13 5 2
4 5 4
2 2 2 3 I 8 3
Total 7 2 15 3 22 60 30 86 75 39 75 48
* Family members by mamage considered not at risk. t Increased in vitro tetraploidy in dermal fibroblast monolayer cultures
$ Family member by marriage with member of a colonic cancer- (+: present; -: absent).
When abnormal clones consituting 1.2% of the cells were seen, 100 metaphases were then examined.
In each case, the karyotype of the individual, the number of chromosome abnormalities (gaps, breaks, fragments, and deletions), and the nature of the pericen- tromeric heterochromatin were established. Polymor- phism of the latter was presumed to exist when inversion (partial or complete) or abnormally large amounts of heterochromatin were present in chromosomes 1, 9, and/or 16, in which such heterochromatin is readily identified because of their large size.
Immunoglobulins
Serum immunoglobulins of the lgA, IgG, and IgM classes were quantitated with commercial radial immu- nodiffusion plates (Kallestad, Chaska, MN).I7
Phenotype for Methionine Dependence in Dermal Fibroblasts in Cultures
Dermal fibroblast cultures were established by standard techniques. Frozen stocks of cells were thawed, cultured, and determination of the phenotype for methionine dependence was camed out as previously de~cribed.~ Briefly, the cells were grown in an MEM culture medium containing either methionine or homocysteine and sup- plemented with folic acid and Vitamin B12. Represen- tative samples were counted every other day. Growth constants in the presence or absence of methionine were calculated during the exponential growth of the cells." By definition, the cells presented with the methionine dependence phenotype when the growth constants, in
prone kindred. 5 Of the 14 members by marriage with increased in vifro tetraploidy,
one (C-OOI) had colonic cancer. Family histories of !he other 13 will be ascertained.
the presence or absence of methionine, were significantly different from each other (paired t test).'
Results
In Vitro Tetraploidy
The data (Table 1 ) showed that increased in vitro tetraploidy was associated with HNPCC (suggestive of cancer gene[s]). All 1 1 families studied expressed in- creased in vitro tetraploidy.
Of the 27 cancer-affected individuals studied, 22 expressed increased in vitro tetraploidy, 5 did not, and 2 of the latter had only skin cancer. Based on this and previous research, it appeared that the Occurrence of skin cancer in two individuals (Table 1, Families C-00 1, C-200) was not due to the cancer-prone gene(s).
Sensitivity (percent of positive results in clinically affected patients) was evaluated (Table 2). As increased in v i m tetraploidy occurred in 22 of the 27 clinically affecteds studied, the sensitivity was 8 I .O%.
Of the 198 (82 male, 116 female) at-risk family members (with first- and seconddegree affected relatives), 22 male and 30 female members expressed in vilro tetraploidy (Table 1).
Eighty-seven of the 10 1 (46 male, 55 female) members by mamage in the HNPCC families studied and consid- ered not at risk for the colon-cancer-predisposing gene(s) did not express increased in vitro tetraploidy. One female member (with colonic cancer) expressed increased in vitro tetraploidy (Table 1). Specificity (percent of negative results in cases in which HNPCC is absent)

No. 4 GENETICS, COLON CANCER, AND BIOMARKERS Lynch el al. 943
TABLE 2. Sensitivity-Specificity of Increased In Vifro Tetraploidy for Clinical Colon Cancer
Family members studied
No. showing increased tetraploidy Total no. studied Sensitivity (96)
Clinically affected family members
Family members by marrianet
22 27 81*
No. showing no increased in vifro tetraploidy Total no. studied Specificity (%)
a7 l 0 l t 86*
* If 100 cancer family syndrome-affected subjects were studied, 19 would have been false-negatives. If 100 normal (not-at-risk) subjects were studied, 14 would have been false-positives.
t One family member by marriage had colonic cancer, not considered to be CFS (C-001). Family cancer history of the other 13 is being as- certained.
(Table 2) in family members by mamage (with no family history of cancer) was 86%.
Tritiated Thymidine Uptake Labeling
Comparative distribution of the upper-crypt labeled cell fiaction (&) for high-risk and low-risk groups: In previously reported, detailed work,'l.19*20 members of these families prone to HNPCC were compared to subjects at lower risk. Significant differences were found between groups of patients with HNPCC and subjects in cancer-free branches of their kindreds, when labeled cell distributions were compared by chi-square analyses over all of the crypt height compartments (P c 0.001). The data of these analyses also were informative because they indicated the direction in which the populations differed in labeled cell frequency versus crypt height compartment numbers." Further, distributions of the occupancy fractions of labeled cells in the upper 40% of crypt (bh), measured for members of each population (&), revealed a discriminant level that separated over 90% of low-risk subjects from a major fraction of those affected with either HNPCC or polyposis, and from nearly half of the at-risk progeny as expected for an
autosomal dominant trait. Thus, when the population fraction dp was plotted versus &,, displaying the fractile distribution of the &, data, a clear separation between the (&, &,,) distributions for patients with hereditary nonpolyposis colon cancer and subjects in the low-risk groups was found."
Thus, 4 h appears to be a more precise measure of risk than that previously used in discriminating individ- uals with genetic susceptibility to colon cancer, including at-risk progeny, from those at lower risk. Using the method for binary classification of individuals based on patterns of incorporation of 'HdThd-labeled cells, com- paring each individual with high- and low-risk reference population^,'^*^^ the sensitivity was found to be 92% and the specificity was 8896, as respectively assessed with 13 individuals known to be symptomatic for HNPCC, and 34 individuals from cancer-free branches of the families (Table 3). Further, application of the method to asymp- tomatic individuals in the kindreds believed to be at 50% risk revealed that they were largely bimodally distributed to nearly zero or full risk. Thus, current findings have suggested that this method of distinguishing among integer distributions of 'HdThd-labeled cells in biopsy specimens of colonic mucosa may also provide
TABLE 3. Group Findings for Symptomatic Familial Colon Cancer Subjects Versus Control Subjects in Cancer-Free Families Using the Methods of Lipkin and Associate~l~.'~
Parameters computed
Score Prognostic index Average versus (S, - 4) reference population Interpolated risk
FCC, FCC, Qd* Rst Binary categorization No. of ~
Population subjects S S 4 (+) (-) 2 (0.50) < FCCd FCCIQ
FCC, 13 (325) 12 1 0.95 0.09 12 1 30
(339) 0.02 4 FCCl 34 (386) (301) 4 30 0.89
Number of subjects positive or negative. t Average of R, values greater or equal to (2) or less than (<) 0.50. $ Number categorized as high risk. 0 Number categorized as low risk. FCC,: individuals affected with familial nonpolyposis colon cancer;
FCCI: individuals in cancer-free families of two or more generations; S,
and $: average scores of s and 1 groups; Q,: number of subjects in high risk (s) and low risk (I) groups having positive or negative prognostic index values; binary categorization: the same subjects automatically classified as high risk or low risk; R,: the average risk values of those subjects classified as high risk (R. 2 0.50) or low risk (R, < 0.50).

944 CANCER Augusr 15 1985 Vol. 56
TABLE 4. Results of Linkage Analysis of Hereditary Nonpolyposis Colorectal Cancer With a Set of Markers
Recombination fractions
Marker 0.0 0.05 0.10 0.20 0.30 0.40
ABO Rh M NS Kell FY Jk Pi Le set ACP ESD GLO GPT =Mi AK PGD Gm Hapt Gc Pi Bf
-4.550 -7.162
-1.513 -2.813
-3.995 -3.547 - 1.027
-a,
-a,
-a 0.334
-3.573 -5.909 -0.489 -0.3 I5
-2.419 -2.255 -4.530 -1.431 - 1.245
0.332
- I .434 -2.69 I -3.108 -0.967 -0.795
-1.189 - I .768 -0.779 -1.500
-1.915 -2.535 -0.41 5 -0.275
- 1.308 -0.545 - 1.366 -0.446 -0.275
1.779
0.277
0.270
-0.688 - 1.490 - 1.862 -0.697 -0.424
I .63 I -0.994 -1.129 -0.560 -0.531
- 1.276 -1.421 -0.319 -0.237 0.153
-0.849 -0. I62 -0.844 -0.136 -0.089
0.226
-0.236 -0.48 I -0.742 -0.37 1 -0.180 1.067
-0.292 -0.489 -0.250 -0.115 0.141
-0.583 -0.535 -0. I55 -0.155 0.1 15
-0.377 0.076
-0.360 0.044
-0.0 1 1
-0.063 -0.1 14 -0.260 -0.175 -0.107 0.590
-0.101 -0.107 -0.084 -0.004 0.080
-0.237 -0.162 -0.035 -0.086 0.045
-0.149 0.089
-0. I38 0.039
-0.004
-0.009 0.003
-0.005 -0.06 1 -0.058 0.198
-0.014 -0.044 -0.0 I4 0.002 0.035
-0.070 -0.0 I8 -0.001 -0.035 0.007
-0.04 I 0.039
-0.036 0.009 O.Oo0
a useful basis for identifying individuals with a gene for HNPCC by separating their labeling patterns from those of low-risk subjects.
Segregation Analysis of 'HdThd Uptake Within Colonic Crypts and In Vitro Dermal Fibroblast Tetraploidy
Posilivily or negativity of a shifi of the major zone of 'HdThd uptake: Under the unrestricted transmission probability model, it was found that the linear effect of age on the penetrances was significant (chi-square = 15.71, 1 df), but the quadratic effect was not. Allowing
TABLE 5. Linkage Analysis: Hereditary Nonpolyposis Colorectal Cancer Versus Jk
Recombination fraction
Family 0.0 0.05 0.10 0.20 0.30 0.40
c-I15 -0.085 -0.068 -0.053 -0.029 -0.013 -0.003 C- 198. -0.097 -0.067 -0.043 -0.012 0.003 0.001 JFL5O -0.002 0.0 0.002 0.003 0.003 0.001 c-164 0.145 0.116 0.089 0.047 0.019 0.004 C-25 I* --a, -0.853 -0.451 -0.198 -0.071 -0.017 C- I96 0.351 0.304 0.250 0.141 0.048 0.004 c-200 1.400 1.240 1.077 0.747 0.426 0.151 CM) I 1.208 0.935 0.654 0.312 0.154 0.058 c-220 0.304 0.249 0.197 0.1 10 0.045 0.022 CFS & HSSCC -a 1.778 1.631 1.067 0.592 0.204 CFS alonet 3.187 2.663 2.125 1.277 0.666 0.221
Families lacking endometrial cancer and pmumed lo represent HSSCC. t Total lod score of CFS alone: without families C-198. C-251. CFS cancer family syndrome; HSSCC: hereditary site-specific colonic cancer.
for this effect of age, it was now found that there is no significant departure from Mendelian autosomal domi- nant transmission (chi-square = 0.33, 2 df), but there is significant departure from the hypothesis of no intergen- erational transmission (i.e., equal transmission proba- bilities, chi-square = 8.81, 2 df). The penetrance of the dominant genotype was estimated to be unity; that of the recessive genotype was estimated to be 0.03 at birth and increasing by a factor of I .028 for each year of age.
'HdThd uptake in 1 1 colonic crypt divisions: For 'HdThd uptake in 1 1 colonic crypt divisions also, it was found that the linear effect of age on the penetrances was significant (chi-square = 19.974, I df), but the qua- dratic effect was not. Allowing for this effect of age, it was now found that there is a significant departure from Mendelian autosomal dominant transmission (chi- square = 7.77, 1 df). However, the estimates of the genotypic frequencies and the penetrance of the domi- nant genotype under the Mendelian hypothesis were quite similar to those obtained for the shift of the major zone of 'HdThd uptake.
In Vitro Telraploidy: As before, it was also found for in vitro tetraploidy that the linear effect of age on the penetrances was significant (chi-square = 47.83, 1 df), but the quadratic effect was not. Allowing for this effect of age, it was found that there is no significant departure from Mendelian autosomal dominant transmission (chi- square = 4.8, 2 df), but there was significant departure from the hypothesis of no intergenerational transmission (chi-square = 8.42, 1 df). The penetrance of the dominant genotype was estimated to be 0.44 at birth and increasing by a factor of I .006 for each year of age. The penetrance of the recessive genotype was estimated to be 0; i.e., there were no sporadic cases.
Linkage
The linkage analysis results are shown in Tables 4 and 5. For HNPCC versus the standard set of markers, only one result is noteworthy. A maximum lod score of + I .88 was observed for all HNPCC kindreds taken together with the Kidd (Jk) blood group. A breakdown of these results per family is shown in Table 5. Only one family (C-25 I ) gave a decidedly negative score. This family and Family C- 198 both did not have any members affected with endometrial cancer, and may have repre- sented HSSCC. Therefore, there was a legitimate basis for excluding these families from the analysis. When kindreds C-198 and C-25 I were removed, the lod score was 3.19 at recombination fraction 8 = 0.0. Although significant, these results must be veiwed cautiously be- cause of the fact that two families were excluded from the summation of lod scores.
The different linkage results found for the CFS and HSSCC kindreds suggested that in these two hereditary

No. 4 GENETICS, COLON CANCER, AND B~OMARKERS - Lynch ez al. 945
TABLE 6. Chromosome and Heterochromatin Polymorphism Studies in Colon Cancer Families
Family identification
C- 164 370-437 c-200
c-220 545-567 C-25 I 449-540 Control
No. of subjects No. of subjects with studied chromosome changes
24 3
7 4
22 5
16 7
19 2
(12.5%)
(57.1%)
(22.7%)
(43.8%)
( 10.5%)
No. of subjects with heterochromatin
10 (4 I .7%)
4 (57.1%)
I 1
7 (43.8%)
4 (2 I . I % )
(50%)
Chromosome No.
1 9 16
8 (33.3%)
0 (0%)
3 (42.8%)
2 (12.5%)
0 (0%)
7 (29.2%)
4 (57.1%)
6 (85.7%)
4
4 (2 1 . 1 % )
(25%)
0 (0%)
2 (28.6%)
3 (47.8%)
1 (6.2%)
0 (W)
syndromes different genetic mechanisms were operating. Segregation analysis, using the clinical disease as the phenotype, was therefore performed on these two groups of kindreds, both separately and together.
In each case, it was found that a dominant Mendelian hypothesis fit the data, and there was significant departure from the hypothesis of no intergenerational transmission. Finally, it was found that there was no significant heterogeneity between the estimates obtained for the two groups, regardless of the assumed hypothesis (P > 0.5). Thus, this segregation analysis failed to give any evidence of a different genetic mechanism in the two groups, CFS and HSSCC.
Cytogenet ics
Table 6 shows: (1 ) a much higher level of heterochro- matin polymorphism in the affected families when com- pared with a control family that was characterized by a low incidence of cancer (percent of known family mem- bers versus percent of affected members in test families); and (2) this polymorphism was observed with more than one chromosome in the affected families, a phenomenon not observed in the control family. Thus, the hetero- chromatin polymorphism was observed in the control family only on chromosome 9. In the HNPCC kindreds, although chromosome 9 was involved in all four of the families studied, polymorphisms of chromosomes 1 and/ or 16 were also common.
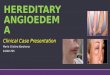
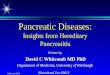
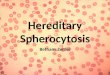
Table 7 shows chromosome changes (breaks, gaps, dicentrics, and translocations). Translocations were ob- served only in the affected families. In one family, a translocation between chromosomes 13 and 22 (Figs. 2 and 3) was seen in two female members and one male member. This resulted in a chromosome count of 45. Heterochromatin polymorphism was not seen in these three subjects. In a second family, an interesting poly- morphism of chromosome 9 (Figs. 4-6) resulted in an abnormal chromosome whose origin could only be identified with C-banding. Only male family members were observed to have this polymorphism.
Immunoglobulins Three CFS kindreds were investigated for quantitative
serum immunoglobulin levels. In a single kindred (Fam- ily C- 1 15), 6 of 23 bloodline relatives were shown to be below the bottom end of the normal range of 85 mg/dl for IgA. By the binomial proportion test by normal approximation, with correction for continuity, the P value was exceedingly close to zero. No other immu- noglobulin abnormalities were found in the other kindreds evaluated.
Met hion ine dependence: Met h ion i ne dependence was investigated in 2 1 dermal fibroblast cultures derived from biopsy specimens from members of four families affected with HNPCC. Results are presented in Table 8. The phenotype for methionine dependence is indepen- dent of the age or sex of the individuals, aging of the dermal fibroblasts, and conditions able to alter gene expression.’ A high degree of correlation with other markers (95%) was observed for the methioninedepen- dence phenotype.
Discussion A major goal of biomolecular research in cancer
genetics is to identify those factors that are the direct
TABLE 7. Chromosomal Abnormalities and Heterochromatin Polymorphism in a Control Family Compared With Four
Hereditary Nonpolyposis Colorectal Cancer Families
Control Colon families* familiest
Range of chromosome
Mean of chromosome
Range of heterochromatin
Mean of heterochromatin
abnormalities 10.5% 12.5%-57.0%
abnormalities 10.5% 34.0%
polymorphism
polymorphism 21.1% 48.2%
21.1% 41.7%-57.1%
In the control family, only chromosome 9 was involved in poly- morphism.
t In colon families, although chromosome 9 was involved in all four of the families studied, polymorphism of chromosome 1 and/or 16 was also observed.

946 CANCER August 15 1985 Vol. 56
9 10
9 9
16
a @
21
4 5
XI 22 x x
FIG. 2. G-banded karyotype of a female family member containing 45 chromosomes due to a translocation of one chromosome 22 to the short arm of a chromosome 13 (arrow). The karyotype is 45, XX, -22, t( 13;22).
result of the cancer-prone genotype through the use of in v i m and/or in vivo studies2' ldentification of these factors may then lead to a better understanding of the etiologic chain of events from putative-cancer-predis- posing genotype to cancer phenotype.2' This objective includes a search for those factors that are directly related either to the deleterious gene or to the presence of other modulating genes, which may lead to variation in cancer-prone genotype expression (phenotype). Studies by Becher el suggest a specific chromosomal change in at least a subgroup of large bowel cancers. Additionally, investigations by Sakaguchi and associates24 suggest that the oncogene for colon cancer resides on chromosome 12. Tables 9 and 1025-36 provide literature examples of other biologic phenomena that might be associated with the HNPCC-predisposing genotype(s).
In Vitro Tetruploidy
Studies3' have shown increased in vitru tetraploidy in dermal fibroblast monolayer cultures from patients with
some heritable colon cancer syndromes (Tables 1 and 2). A similar study by Delhanty and colleagues38 studying I7 familial polyposis coli (FPC) patients showed that increased in v i m tetraploidy was one feature of cultured cells from such patients. Another feature was the number of cytogenetically abnormal clones, a fraction of which reached 80% to 100% in those derived from early- passage cultures. From these two studies, it could be concluded that these chromosomal alterations were the in vitro expressions of a cancer-prone gene@) associated with hereditary colon cancer. It is also noteworthy that increased in vitro tetraploidy (TETR) was strongly as- sociated with HNPCC, appearing therefore as a marker for both CFS and HSSCC.
The finding of increased in vitro tetraploidy in 10 of the 14 individuals who were positive for increased in vitro tetraploidy, but were not at increased genetic risk for cancer, is enigmatic (Table 1). Ten of these 14 individuals were from a Navajo Indian kindred (Family C-25 1). Our determination of significance of this putative biomarker has been based exclusively upon a white

No. 4 GENETICS, COLON CANCER, AND BIOMARKERS * Lynch et a/ . 947
i rr li' 2 3
7 8 9 10
11 14 15
t ? 20
rb 16
&a
21
FIG. 3. G-banded karyotype of a male family member containing 45 chromosomes due to a translocation of one chromosome 22 to the short arm of a chromosome 13 (arrow). The karyotype is 45, XY, -22. t( I13;22).
population3' and, therefore, may not apply to Indian populations. h vitro tetraploidy among Navajo Indians who are not at increased risk for colon cancer must be performed in order to determine significance.
'HdThd Labeling Studies
Studies of cell proliferation have aided our under- standing of the neoplastic transformation of colonic epithelial cells in hereditary conditions that predispose to ~ance r .~ -~ . ' '-19.20 For example, an abnormal pattern of incorporation of 3HdThd into DNA of colonic epi- thelial cells has been observed in FPC wherein increased numbers of epithelial cells in the upper portion of the colonic crypts continue to incorporate 'HdThd into DNA. These abnormally proliferative upper crypt epi- thelial cells tend to accumulate near the lumenal surface of the colonic mucosa and give rise to adenomasW
New analytical methods have now been developed through current work and have enabled these measure- ments to be carried out with increased precision. These
new methods have facilitated analysis of the height distribution patterns of 3HdThd-labeled epithelial cells in colonic crypts of high- and low-risk population groups, permitting application to study differences that develop in subjects with hereditary predisposition to colon cancer and in other subgroups in the general population. Several of the are of particular interest and have improved the sensitivity and specificity with which sub- jects at high risk for colon cancer could be differentiated from those at low risk (e.g., Table 3). Moreover, studies are currently in progress to determine if biopsy specimens obtained from the cecal area might be more sensitive than rectal biopsy specimens in detecting camers of genes predisposing to cancer in the proximal colon.
Segregation Analysis
It was not possible to allow completely for the mode of ascertainment of the pedigrees. However, both in vitro tetraploidy and a shift of the major zone for 'HdThd uptake in colonic crypts appeared to fit a model

948 CANCER August I5 1985 Vol. 56
,. 9'
r f 8 i r
3
8
15
!? 4 18
4 5
9 10 11 12
1. #.
21 2 2
dt X Y
FIG. 4. G-banded karyotype of a male member of a family showing heteromorphism of a chromosome 9 (arrows). The other chromosomes appear normal.
of dominant Mendelian transmission, the penetrance illcreasing with age. The lack of fit of 'HdThd uptake in 1 1 colonic crypt divisions to a genetic model may or may not be significant. The statistical tests used rely on asymptotic properties that may or may not hold for 88 individuals distributed in six pedigrees. In any case, further data need to be collected on all three traits and analyzed as quantitative variables rather than as simple dichotomous variables before any definite conclusions regarding the mode of inheritance can be reached. It will also be of interest to analyze jointly, in a multivariate analysis, the three variables: shift of the major zone for 'HdThd uptake in colonic crypts, 3HdThd uptake in 1 1 colonic crypt divisions, and in v i m tetraploidy.
Linkage Anal-vsis
These current linkage analyses show a possible linkage between CFS and Jk. These observations must be inter- preted cautiously, since two families presumed to be HSSCC families were removed from the final calculation, leading to a significant increase in the lod score (3.19) for the CFS kindreds.
Immiinohiologic Findings
One kindred had an abnormally high number of individuals with low serum IgA levels. High priority should be given to elucidating mechanisms behind the multiple immune abnormalities noted in such kindreds (Tables 9 and lo), as these observations may provide clues to the extent of genetic heterogeneity. tumor susceptibility, and survival advantage4' within the HNPCC syndromes and their relation to other cancer susceptibility syndromes.
Chromosornul Studies
Chromosomal abnormalities have an association with neoplasia, as clearly evidenced in such disorders as the chromosome breakage syndromes. Although we do not claim that the findings described in these families have comparable significance, it is nevertheless difficult to ignore the possibility that they may be contributing to susceptibility to neoplasia. In particular, we wonder about the effects of translocations (10.5% control versus 34% in affected kindreds). The cancer-affected families

No. 4 GENETICS, COLON CANCER, AND BIOMARKERS - Lynch et d. 949
3
(Q 8
?'
15
rl 18
I .
21
rI7 l i 9 10
* * . . 22
4
* t Im
11
I ! 5
:; 12
X V
Fie. 5 . G-banded karyotype of another male member of a family showing heteromorphism of a chromosome 9 (arrows). The other chromosomes appear normal.
have a higher incidence of heterochromatin polymor- phisms, but their interpretation remains elusive and will depend upon proper control data. Nevertheless, the possibility remains that these changes, regardless of whether they occur in the affected or nonaffected indi- viduals from these families, may interact with other genetic and/or cytogenetic events, and thereby may have more etiologic significance than is currently appreciated.
Methionine Dependence
Methionine dependence is expressed as a reduced growth of cells in a methionine-deficient culture medium. It is a characteristic of tumor and transformed cell lines42 and is also observed in dermal fibroblasts of patients with Gardner's syndrome and familial colon cancer.' The current data extend the validity of previous observations' and suggest an association between abnor- mal methyl metabolism in human cells and neoplasia.
Conclusions
The above-mentioned biomarkers require extensive evaluation in both CFS and HSSCC kindreds before
FIG. 6. C-banded chromoWmes 9 of parents and two sons with heteromorphism of a chromosome 9. Thus, in each male one chro- mosome 9 (on the right) shows an inordinately large amount of (C- banded) heterochromatin, with the two sons inheriting the anomaly from the father. The two Xchromosomes of the mother appear normal.

950 CANCER August 15 1985 Vol. 56
TABLE 8. Incidence of the Methionine Dependence Phenotype in Members of Cancer Family Syndrome Families
TABLE 9. Immunologic Findings in Some Members of Nonmlyposis Colon Cancer-Prone Kindreds
~ ~ ~~ ~
Patient Other phenotype not sample associated with
no. Phenotype Medical history clinical diagnosis
13 16 26 30
460 463 170 149 I10 I14 120 I30 I74 I76 I79 485 490 I I6 113 115 526
MD MD MD MD MD MD 0 MD 0 0 0 0 0 0 0 0 0 MD MD MD MD
Colon cancer Colon cancer Colon cancer Colon cancer Colon cancer Colon cancer Colon cancer At risk* Low risk? Low risk Low risk Low risk Low risk Low risk Low risk Low risk Low risk Low risk Low risk Low risk Low risk
Authors Immunologic findings
Creagan and Fraumeni2’
Law et a/.26
L R P NT
Berlinger and Good”
Katano er ~ 1 . ~ ~
HRP HRP HRP, IT HRP, IT
At risk of developing colon cancer, but died of breast cancer. t Includes spouse and members of isolated clusters free of colon cancer. MD. methioninedependence phenotype; 0: absence of the methi-
oninedependence phenotype; LRP low-risk profile of thymidine in- corporation in colonic crypts; NT: normal in vitro tetraploidy; HRP: high-risk profile of thymidine incorporation in colonic crypts; IT: in- creased in virro tetraploidy.
their utility can be assessed for purposes of both identi- fying gene carriers and showing these to be distinct genetic entities, as was suggested in the clinical data (Part I), by differing mean ages of cancer onset. Contin- ued investigations of cellular, biochemical, and/or be- havioral anomalies in such kindreds could help to elucidate the mechanism(s) responsible for cellular con- version from a normal to a malignant phenotype(s).
The biomarker findings provide a major advance in the comprehension of HNPCC. Heretofore, classification as “affected“ versus “nonaffected” has been dependent upon the expression or lack of expression of the syn- drome cancer phenotype, which is complicated by the age-dependent penetrance. If these biomarkers continue to display high sensitivity and specificity in the testing of additional HNPCC kindreds, we would then have a capability of very early genotype prediction, thereby indicating who will versus who will not manifest the phenotype (syndrome cancer).
Psychologic preparation of patients destined to develop cancer of specific anatomic sites could be effected so that compliance with particular surveillance/management programs might become maximal. We would have an unparalleled opportunity to test a variety of possible intervention programs among individuals from HNPCC pedigrees who would be at very high risk of developing
Lynch er a/.29
Sivak et a/.”
Lynch er ul.”
Arthur el a/.”
1. Lymphocytopenia 2. Decreased IgA and IgG 3. Decreased lymphoproliferative
4. Antiparietal antibodies 5 . Elevated EBV antibody titers 1. Depressed mitogen and mixed
lymphocyte culture responses in about one half of the family members
responses
2. Low percentage of T-lymphocytes 3. Depressed delayed type hypersensitivity
Identified monocytes suppressing mixed lymphocyte culture responses in some CFS family members
I . Depressed mitogen responses 2. Probable association with HLA A9-
Bw35 haplotype Possible association with HLA A2-BIZ
haplotype Suggest linkage with histocompatibility
antigens Elevated CEA levels segregated in high-
risk family members and spouses of high-risk CFS kindred members
lmmune parameters normal: suggest use of CEA levels in subject surveillance
to skin tests
EBV: Epstein-Ban virus; CFS: cancer family syndrome; CEA: car- cinoembryonic antigen.
cancer in their lifetimes. One could then more accurately evaluate genetic and environmental interactions in car- cinogenesis. This is important when considering the enormous heterogeneity of host as well as environmental factors that influence cancer expression in the general population. I t may be possible to determine what factors. delay or prevent the expression of the cancer gene(s). An awareness of such protective factors might lay the foundation for better methods of cancer prevention in the general population.
TABLE 10. Possible Nonimmunologic Biomarkers in Hereditary Nonpolyposis Colorectal Cancer
Authors Biologic finding
Lynch er 01.”
Lipkin el a/.”
Lynch el d2’
Features of Tom’s syndrome in small subset of CFS
Abnormal tritiated thymidine labeling of colonic
I . Possible genetic linkage with Jk blood group in the CFS
2. Possible linkage with increased frequency of in vitro skin fibroblast tetraploidy
Decreased conversion of cholesterol to its degradation products in some patients
Reduced DNA repair synthesis in patients genetically predisposed to colorectal cancer
patients
crypts
Lipkin er ~ 1 . ’ ~
Per0 er a/.”
Macrae er Brachydactyly (one family)
CFS: cancer family syndrome.

No. 4 GENETICS, COLON CANCER, AND BIOMARKERS - Lynch el a/. 95 1
In conclusion, this work provides a format for further investigations into the significant problem of genetically determined colon cancer. Specifically, these investigations should include as many potentially informative biologic parameters as possible per sampling to: ( 1 ) assess con- cordance of putative biomarkers within kindreds; (2) assess differences in genotype and/or environmental influences between the various colon-cancer-prone kindreds; and (3) obtain maximal information before patient participation may begin to decrease with addi- tional samplings. As reliable genotype markers are elu- cidated, it should theoretically become possible to ac- curately determine both the contribution of genetically determined cancer to the total colon cancer burden and the incidence of colon-cancer-predisposing genotypes in the human population.
REFERENCES
I . Danes BS, Bulow S, Svendsen LB. Hereditary colon cancer syndromes: An in v i m study. Clin Genet 1980 18: 128--136.
2. Lipkin M. Phase I and Phase 2 proliferative lesions of colonic epithelial cells in disease leading to colonic cancer. Cancer 1974; 34:
3. Deschner EE. Early proliferative changes in gastrointestinal neo- plasia. Am J Gastroenterol 1982; 77:207-2 1 I .
4. Lipkin M, Deschner E, Blattner W, Fraumeni JF, Lynch HT. Tritiated thymidine incorporation into colonic epithelial cells of subjects in colon cancer-prone families (Abstr). Proceedings of AACR/ASCO Annual Meeting, May 26-27, 1980.
5. Sandberg AA. The Chromosomes in Human Cancer and Leu- kemia. New York-Amsterdam: Elsevier, 1980; 748.
6. Hughes NR. Serum concentrations of $3, yA. and r M immu- noglobulins in patients with carcinoma, melanoma, and sarcoma. J Null Cancer Inst 1971; 46:1015-1027.
7. Mikol YB, Lipkin M. Methionine dependence in skin fibroblasts of humans affected with familial colon cancer or Gardner syndrome. J Natl Cancer Inst 1984; 72: 19-22.
8. On J. Estimation of the recombination fraction in human pedigrees: Efficient computation of the likelihood for human linkage studies. Am J Hum Genet 1974; 26588-597.
9. Danes BS, Beam AG. Cystic fibrosis of the pancreas: A study in cell culture. J Exp Med 1969; 129:775-793.
10. Danes BS. Occurrence of in vitro tetraploidy in the heritable colon cancer syndromes. Cancer 198 I ; 48: 1 596- I60 I .
I I . Lipkin M, Blattner WE, Fraumeni JF. Lynch HT, Deschner E, Winawer S. Tritiated thymidine (&,, A) labeling distribution as a marker for hereditary predisposition to colon cancer. Cancer Res 1983;
12. Maskens AP, Deschner EE. Tritiated thymidine incorporation into epithelial cells of normal appearing colorectal mucosa of cancer patients. J Nut1 Cancer Inst 1977: 58:1221-1224.
13. Deschner EE, Lipkin M. Proliferative patterns in colonic mucosa in familial polyposis. Cancer 1975; 35:413-418.
14. Deschner EE, Maskens AP. Significance of the labeling index and labeling distribution as kinetic parameters in colorectal mucosa of cancer patients and DMH treated animals. Cancer 1982; 501 136- 1141.
15. Elston RC, Stewart J. A general model for the genetic analysis of pedigree data. Hum Hered 1971; 21523-542.
16. Morton NE. Sequential tests for the detection of linkage. Am J Hum Genet 1955; 7:277-318.
17. Rowe DS, Anderson SG, Skegg J. Standardization of quantitative measurements of human immunoglobulins G, A, and M. In: Merler E, ed. Immunoglobulins. Washington, DC: National Academy of Sciences, 1970; 361.
878-888.
43: 1899- 1904.
18. Poirier LA, Wilson MJ. The elevated requirement for methionine by transformed rat liver epithelial cells in vilro. Ann N Y Acad Sci
19. Lipkin M. Method for binary classification of individuals with familial polyposis based on patterns of incorporation of tritiated thymidine into colonic epithelial cells as a marker for hereditary predisposition to colon cancer. Cell Tissue Kine: 1984; 17:209-222.
20. Lipkin M, Blattner W, Gardner G et a/. Classification and risk assessment of individuals with FPC, Gardner syndrome, and familial nonpolyposis colon cancer from ’HdThd-labeling patterns in colonic epithelial cells. Cancer Res 1984; 44:420 1-4207.
21. Lynch HT, Danes BS, Lipkin M et a/. Biomarkers and the cancer family syndrome (CFS) (Abstr). Proceedings of ASCO Annual Meeting, May 22-24, 1983.
22. Mulvihill JJ, Miller RW, Fraumeni JF, eds. Genetics of Human Cancer. New York: Raven Press, 1977; 519.
23. Becher R, Gibas 2, Sandberg AA. Involvement of chromosomes 7 and I2 in large bowel cancer: Trisomy 7 and 12q-. Cancer Genet Cyiogenet 1983; 9:329-332.
24. Sakaguchi AY. Naylor SL. Shows TB, Toole JJ, McCoy M, Weinberg RA. Human c-fi-ras2 proto-oncogene on chromosome 12. Science 1983; 2 19: 108 I - 1083.
25. Creagan ET, Fraumeni JF. Familial gastric cancer and immu- nologic abnormalities. Cancer 1973; 32: 1325-1331.
26. Law IP. Hollinshead AC, Whang-Peng J et a/. Familial occur- rences of colon and uterine carcinoma and of lymphoproliferative malignancies: 11. Chromosomal and immunologic abnormalities. Cancer
27. Berlinger NT, Good RA. Suppressor cells in healthy relatives of patients with hereditary colon cancer. Cancer 1980 45: 1 112-1 116.
28. Katano M, Fujiwara H, Toyoda K, Torisu M. Immunogenetic studies of familial large bowel cancer. Gann 1980; 71583-588.
29. Lynch HT. Thomas RJ, Terasaki PI et a/. HLA in cancer family “N.” Cancer 1975; 36:1315-1320.
30. Sivak MV, Sivak DS, Braun WA, Sullivan BH. A linkage study of HLA and inherited adenocarcinoma of the colon. Cancer 1981; 48:
3 I . Lynch HT, Guirgis HA, Hams RE et a/. Familial clustering of plasma carcinoembryonic antigen (CEA) in the cancer family syndrome. Scand J Immunol 1978; (Suppl) 8:465-470.
32. Arthur DC, Robison LL, Woods WG, Krivit W, Nesbit ME. Hereditary adenocarcinoma of the colon in childhood: association with the cancer family syndrome. (Submitted for publication).
33. Lynch HT, Lynch PM, Pester J, Fusaro RM. The cancer family syndrome: Rare cutaneous phenotypic linkage of Torre’s syndrome. Arch Intern Med 1981; 141:607-611.
34. Lipkin M, Reddy BS, Weisburger J, Schechter L. Nondegradation of fecal cholesterol in subjects at high risk for cancer of the large intestine. J Clin Invest 1981; 67:304-307.
35. Per0 RW, Miller DG, Lipkin M et a/. Reduced capacity for DNA repair synthesis in patients with or genetically predisposed to colorectal cancer. J Nail Cancer Inst 1983; 70867-875.
36. Macrae FA, Roberts-Thomson IC, McRussell D, St. John DJB. Familial colorectal cancer and hereditary brachydactyly. Br Med J
37. Danes BS. Increased in vitro tetraploidy: Tissue specificity within heritable colorectal cancer syndromes with polyposis coli. Cancer 1978;
38. Delhanty JDA, Davis MB, Wood J. Chromosome instability in lymphocytes, fibroblasts, and colon epithelial-like cells from patients with familial polyposis coli. Cancer Genet Cytogenet 1983; 8:27-50.
39. Danes BS, Lynch HT. Increased in vitro tetraploidy in dermal monolayer cultures derived from normals. Cancer Genet Cytogenet
40. Lynch HT. Albano WA, Danes BS, Lynch J, Lynch PM. Precursor conditions and monitoring of high risk colon cancer patients. In: Stroehlein JR, Romsdahl MM, eds. Gastrointestinal Cancer. New York: Raven Press, 1981; 297-325.
41. Albano WA, Recabaren JA, Lynch HT el a/. Natural history of hereditary cancer of the breast and colon. Cancer 1982; 50360-363.
42. Hoffman RM. Methionine dependence in cancer cells: A review. In Vitro 1982; 18:421-428.
1980 349283-293.
1977; 39:1229-1236.
76-8 1.
I98 I ; 282: 143 1-1432.
41 :2330-2334.
1983; 8:81-87.