Embed Size (px)
Citation preview

Hereditary Long Q-T Syndrome Presenting as Epilepsy: Electroencephalography Laboratory Diagnosis Sidney M. Gospe, Jr, MD, PhD,"t and Michael Choy, MDt
Patients with hereditary Q-T interval prolongation can present with seizures, syncope, and sudden death. In 2 siblings with autosomal dominant familial long Q-T syndrome, electroencephalographic examinations per- formed 6 and 2 years before diagnosis included electro- cardiographic tracings documenting the cardiac abnor- mality. A timely diagnosis of this condition may have prevented the death of 1 of these patients. Measurement of the corrected Q-T interval on electrocardiographic tracings obtained in the electroencephalography labora- tory should be considered in selected patients.
Gospe SM Jr, Choy M. Hereditary long Q-T syndrome presenting as epilepsy:
electroencephalography laboratory diagnosis. Ann Neurol 1989;25:514-516
Two familial syndromes characterized by episodes of syncope, ventricular tachyarrhythmias, sudden death, and prolongation of the Q-T interval o n the electrocar- diogram (EKG) have been described {l-31. Both of these conditions can present with seizures due to car- diac tachyarrhythmias, and diagnosis is often delayed until an EKG is obtained E4-101. T h e underlying car- diac abnormality can be recorded in the electroenceph- alography (EEG) laboratory via routine monitoring of an EKG lead. To emphasize the importance of analyz- ing the E K G lead for this possible abnormality, we present the cases of 2 siblings with autosomal domi- nant long Q-T syndrome (Romano-Ward syndrome) in whom EEG studies performed several years before diagnosis documented the prolonged Q-T interval.
Case Reports Patient 1 A 15Y4-year-old girl had a several-year history of seizures that were precipitated by excitement or exertion. The epi-
From the Departments of "Neurology and PPediatrics, School of Medicine, University of California, Davis, Davis, CA. Received Aug 2, 1988, and in revised form Oct 21. Accepted for publication Oct 21, 1988. Address correspondence to Dr Gospe, Department of Neurology, University of California, Davis Medical Center, 231 5 Stockton Blvd, Sacramento, CA 95817.
sodes were preceded by a visceral aura and consisted of gen- eralized tonic-clonic motor activity followed by postictal lethargy. She was treated for a period of time with phenobar- bital, but she continued to have 1 to 2 episodes yearly.
On the day of hospital admission the girl was attending a movie when she noticed a boy from her school. She became anxious, told her friends that she was going to have a seizure, and spit out the candy she was eating. A 1-minute general- ized tonic-clonic seizure occurred, followed by unrespon- siveness and absent respirations and pulse. The Heimlich maneuver was administered, and cardiopulmonary resuscita- tion was initiated and continued for 45 minutes. Ventricular fibrillation was documented and normal sinus rhythm was established with cardioversion. The arterial blood gas evalua- tion revealed carbon dioxide tension of 59, oxygen tension of 15, oxygen saturation of 12%, and p H of 7.06. On exami- nation, the patient had no spontaneous motor activity and no responses to stimuli; the pupils were slightly reactive, but the remainder of her brainstem reflexes were absent. Cardio- vascular examination was normal. A subarachnoid bolt was placed and the patient received aggressive treatment for in- creased intracranial pressure. After the patient's history and the family history were reviewed, a 12-lead EKG was ob- tained that documented a prolonged corrected Q-T interval (Q-Tc) of 0.57 seconds (normal < 0.44 seconds). The pa- tient's condition did not respond to therapy, and she expired on the eighth hospital day.
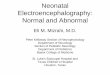
Review of old records revealed that 6 years previously the patient had a normal computed tomography scan of the head and a normal EEG. An EKG tracing was present on a portion of the EEG and showed a Q-Tc of 0.53 seconds (Fig 1).
Patient 2 The brother of Patient 1, aged 12 years 5 months, began having fainting spells at 8 years of age. These occurred ap- proximately once yearly and were precipitated by hyperven- tilation, heavy exercise, or nervousness. He denied palpa- tions but did note diffuse paresthesias at the onset of these events. On two occasions, the patient experienced these epi- sodes while swimming and needed to be rescued. Clinical seizures had not been documented. An EEG obtained at 10 years 10 months of age was unremarkable except for bursts of generalized spike and polyspike and slow-wave complexes during photic stimulation at 14 Hz. The patient refused to hyperventilate during the study. A routine 12 lead EKG obtained at the time of his sister's diagnosis showed a Q-Tc of 0.53 seconds. An electrocardiographic monitor had been present on his previous EEG examination and documented a Q-Tc of 0.52 seconds (Fig 2). The patient is now being treated with nadolol, and he has had no recurrence of syn- copal episodes.
Other Family Members The father and 4 other children in this family have now been diagnosed with this condition. All of these family members have been asymptomatic and all are now being treated.
Discussion In the familial syndromes of Q-T interval prolonga- tion, syncopal attacks and convulsive seizures are sec-
514 Copyright 0 1989 by the American Neurological Association

Q - T o.53=0.53sec C = m
Fig 1. Routine electroencephalogram with electrocardiographic tracing performed on Patient 1 at age 8 years 4 months. Patient had been receiving phenobarbital at time of examination. Electro- cardiographic tracing demonstrates corrected QT interval (Q-T,)
of 0.53 seconds (normal < 0.44 seconds). (Horizontal calibration = 1 sec; vertical calibration = 100 pV {electroencephalogram}, 4.2 mV {electrocardiogram}.)
Fig 2. Routine electroencephalogram with electrocardiographic tracing pegomzed on Patient 2 at age 10 years 10 months. Pa- tient was not receiving medication. Electrocardiographic tracing demonstrates corrected QT interval (Q-T,) of 0.52 seconds (nor-
ondary to cerebral ischemia resulting from ventricular tachyarrhythmias. The Romano-Ward syndrome is as- sociated with autosomal dominant inheritance El, 2), whereas the Jervell-Lange-Nielsen syndrome is an autosomal recessive condition in which congenital deafness also occurs [ 3 } . These conditions usually pre- sent in childhood or adolescence with recurrent syn- cope or convulsive syncope, frequently induced by exercise or excitement. A family history of similar episodes or of sudden death is common. The survival rate in untreated patients is 25%, and lifelong therapy with beta-adrenergic blocking agents is now the pre- ferred method of treating these disorders [l 1). Recog- nition of these syndromes is vital in affected families to prevent severe neurological morbidity and sudden death. In our 2 patients, the diagnosis of a prolonged Q-Tc could have been made many years earlier by analyzing the EKG tracings that were recorded in the EEG laboratory.
Monitoring the EKG during EEG examination is routinely performed in many laboratories by placing electrodes on both arms or shoulders (which simulates
ma/< 0.44 seconds). (Horizontal calibration = 1 sec; vertical calibration = 100 FV {electroencephalogram}, 4.2 mV {electro- cardiogram}.)
EKG lead I). Examining both electrophysiological measures together aids in distinguishing EKG and pulse artifacts in the EEG. Simultaneous recordings of the EKG and EEG have proved useful in charac- terizing other forms of syncope, and a number of car- diac rhythm disturbances can be detected on a single EKG lead recorded with the EEG Cl2, 13). Follow-up 12-lead electrocardiography and rhythm strip and car- diology consultation are indicated whenever a previ- ously undiagnosed cardiac dysrhythmia is uncovered.
Since the Q-T interval varies with heart rate, this measurement needs to be appropriately corrected (Q-Tc). This is accomplished by dividing the measured Q-T interval by the square root of the corresponding cycle length (R-R interval). Using this method, the normal Q-Tc should be shorter than 0.44 seconds [14}. If a prolonged Q-Tc is discovered, other causes of prolongation such as electrolyte disturbances, rheu- matic carditis, myocarditis, severe liver disease, myo- cardial infarction, and certain drug effects must be con- sidered [S, 11, 14). In patients with prolonged Q-T interval, variation in interval length can be seen, and
Brief Communication: Gospe and Choy: Diagnosis of Long Q-T Syndrome 515

several beats should therefore be examined in each lead. Since the Q-Tc can vary in different EKG leads, a normal Q-Tc measured on a single EKG lead as part of an EEG examination does not rule out Q-Tc prolon- gation.
Bricker and colleagues 18, 151 emphasized that “Q- T interval prolongation is more subtle than striking on the [EKG] and must be looked for specifically.” Evalu- ation of the EKG data contained in the EEG examina- tions of our 2 patients would have led to an earlier diagnosis of the Romano-Ward syndrome. We suggest that electroencephalographers should be aware of the syndromes of hereditary Q-T interval prolongation and that the Q-Tc should be calculated in young pa- tients with syncope, seizures precipitated by exercise and excitement, or a family history of similar episodes and sudden death. Twelve-lead EKG evaluation of pa- tients with this history is always indicated.
The authors wish to thank Dr A. J. Gabor for reviewing the manu- script, and Ms J. Redmond and Ms J. Davey for editorial assistance.
References
5 16
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
Romano C, Gemme G, Pongigloine R. Aritmie cardiache rare dell’eta pediatrica. Clin Pediatr 1963;45:656-683 Ward OC. New familial cardiac syndrome in children. J Irish Med Assoc 1964;54:103-106 Jervell A, Lange-Nielsen F. Congenital deaf-mutism: functional heart disease with prolongation of the Q-T interval, and sudden death. Am Heart J 1957;54:59-68 van Bruggen HW, Sebus J, van Heyst ANP. Convulsive syn- cope resulting from arrhythmia in a case of congenital deafness with ECG abnormalities. Am Heart J 1969;78:81-86 Singer PA, Crampton RS, Bass NH. Familial Q-T prolongation syndrome. Arch Neurol 1974;31:64-66 Selby PJ, Driver MV. An unusual cause of apparent epilepsy: ECG and EEG findings in a case of Jervell Lange-Nielsen syn- drome. J Neurol Neurosurg Psychiatry 1977;40:1102-1108 Ballardie FW, Murphy RP, Davis J. Epilepsy: a presentation of the Romano-Ward syndrome. Br Med J 1983;287:896-897 Bricker JT, Garson A, Gillette PC. A family history of seizures associated with sudden cardiac deaths. Am J Dis Child 1984;
Horn CA, Beekman RH, Dick M, Lacina SJ. The congenital long QT syndrome. Am J Dis Child 1986;140:659-661 Sundaram MBM, McMeekin JD, Gulamhusein S. Cardiac tachyarrhythmias in hereditary long QT syndromes presenting as a seizure disorder. Can J Neurol Sci 1986;13:262-263 Schwartz PJ. The idiopathic long QT syndrome. Ann Intern Med 1983;99:561-562 Jordan JE, Grice ST, White DH. The usefulness of routine electrocardiographic monitoring in the EEG laboratory. Clin Electroencephalogr 1978;9:69-79 Gerson IM, Gorbly C, Amorosco M. Renewed importance of electrocardiographic monitoring during routine and special elec- troencephalographic studies. Clin Electroencephalogr 1977;8:
Moss A. Prolonged Q-T interval syndromes. JAMA 1986;256:
Garson A. The electrocardiogram in infants and children: a sys- tematic approach. Philadelphia: Lea and Febiger, 1983
138~866-868
36-46
2985-2987
The Effect of Carbamazepine on Cerebral Glucose Metabolism William H. Theodore, MD, Edward Bromfield, MD, and Linda Onorati, BA
We used positron emission tomography with I8F-2- deoxy-Dglucose to study the effect of carbamazepine on local cerebral metabolic rate for glucose (ICMRGlc) in 9 patients with complex partial seizures. Twenty re- gions of interest were evaluated. Seven control patients had serial scans without a drug change. Metabolic rates were significantly ( p < 0.05) lower in patients on car- bamazepine in 6 of 20 regions of interest (3 left cerebral hemisphere, 3 right). Mean ICMRGlc was 7.4 f 2.0 mg/ mid100 in patients on carbamazepine and 8.8 f 2.5 in patients off carbamazepine ( p < O.oooO5; cutoff level for 180 comparisons: 0.00027). The mean ( f SEM) differ- ence in ICMRGlc between scans was 12 = 2%. No sig- nificant changes in lCMRGlc on serial scans were de- tected in any of the 20 regions for the control group. The mean (-t SEM) variation for control regions of in- terest was 1 f 1%. This study showed that car- bamazepine depresses cerebral glucose metabolism as much as phenytoin does, but much less than phenobar- bital does. The difference in effect on lCMRGlc may be related to drug mechanisms of action, as well as to ef- fects on memory, learning, mood, and behavior.
Theodore WH, Bromfield E, Onorati L. The effect of carbamazepine on cerebral glucose metabolism.
Ann Neurol 1989;25:516-520
Antiepileptic drugs may have profound effects on ce- rebral function. Cognitive impairment has been attrib- uted to the use of phenobarbital (PB), benzodiaze- pines, and to a lesser degree, phenytoin (PHT); data on the latter are less convincing, and some investiga- tors have not found PHT to cause significant adverse neuropsychological effects Cl-S}. Differences between drugs in effect on cognitive function are paralleled by differences in effect on local cerebral metabolic rate for glucose (ICMRGlc). In previous studies, we showed that PB reduces lCMRGlc by a mean of 3796,
From the Clinical Epilepsy Section, National Institutes of Health, Bethesda, MD. Received Sep 9, 1988, and in revised form Nov 4. Accepted for publication Nov 7, 1988. Address correspondence to Dr Theodore, National Institutes of Health, Clinical Epilepsy Section, Building 10, Room 5N-248, Bethesda, MD 20892.

![WONOEP appraisal: Imaging biomarkers in epilepsy...recent advances in identifying the irritative zone (e.g., scalp and intracranial electroencephalography–functional MRI [EEG-fMRI])](https://img.dokumen.tips/doc/110x75/6055314f35bedc66711e5aef/wonoep-appraisal-imaging-biomarkers-in-epilepsy-recent-advances-in-identifying.jpg)