Embed Size (px)
Citation preview

British Journal of Surgery 1995, 82, 1086-1088
Hereditary breast cancer and linkage analysis to BRCAl A . G . M c K I N L E Y , S . E . H . R U S S E L L * , R . A . J . S P E N C E , W . O D L I N G - S M E E and N . C. N E V I N *
Departments of Surgery and 'Medical Genetics, Belfast City Hospital and Royal Victoria Hospital, The Queens University, Belfast, UK Correspondence to: Mr A. G . McKinley
In this study, over 1000 women with breast cancer were linkage analysis which confirmed that in 12 families breast contacted by questionnaire and 164 families with a strong cancer susceptibility could be traced to BRCAl. The study history of breast cancer were identified. Home visits to demonstrates the number of women at risk of breast obtain full pedigree details took place for 123 women, and cancer in the population, illustrates the complexity of members of 24 families gave venous blood samples. The genetic analysis for hereditary breast cancer and extracted DNA was typed by polymerase chain reaction demonstrates the problems of predictive analysis in amplification and the derived haplotypes submitted to clinical management.
A family history of breast cancer is recognized as one of the most important risk factors for the disease. In the majority of families this may represent a multifactorial combination of environmental risks and genetic input, but in some is the direct result of a dominant genetic influence. A number of epidemi~logical'-~ studies have suggested the presence of a rare autosomal dominant gene present in approximately 3 per 1000 individuals' which is responsible for a proportion of the familial clustering of breast cancer in the population.
A n association (lir~kage)~ between familial breast cancer and the region 12-23 on the long arm of chromosome 17 was established in 1990. This finding has been confirmed by a multinational consortium investigation of more than 200 breast cancer prone families, which suggested that approximately 45 per cent of families with at least three breast cancers and perhaps all families with multiple breast cancers in association with epithelial ovarian malignancy will trace susceptibility to this defective gene5. The region of chromosome 17 containing the gene has been the focus of intense interest, and although the area was narrowed considerably6,', it was not until recently that the exact location of this gene', known as BRCAl, was identified9.
Hereditary breast cancer is characterized by a number of features which differ from sporadic breast cancer. These include early onset of breast cancer'O, an excess of bilateral disease", an association with other malig- nancies12 (particularly ovarian and gastrointestinal cancers), and transmission of the disease through successive generations in an autosomal dominant patternI3.
This study on breast cancer prone families was prompted by developments in the molecular aspects of breast carcinogene~is~-~ and by the recognition that women from such families constitute a group at high risk of breast cancer (80 per cent lifetime risk for BRCAl gene carrier^)^.
Patients and methods Breast cancer prone families were identified from four main sources: (1) the Northern Ireland charity organization Action Cancer which provides cancer screening for women who refer
Paper accepted 9 December 1994
themselves; (2) high-risk women attending specialist breast clinics; (3) premenopausal women developing breast cancer in Northern Ireland in a 5-year period identified from pathology records; and (4) general practitioners in the province were circulated with details of the study and requested to refer any family felt to be at risk.
Women were contacted and asked to complete a family pedigree q~estionnaire'~ which requested details of breast cancer transmission through paternal or maternal lines, presence of bilateral disease and details of other malignancies in the family. Families in which at least three women had developed breast cancer were visited to obtain a complete pedigree and information regarding time and place of surgery for affected family members which allowed pathological verification of disease.
If the family appeared suitable for DNA analysis, i.e. they had a pedigree suggestive of hereditary breast cancer, and there was availability of affected family members, after discussion and consent, venous samples were taken and DNA obtained by guanidine extract i~n '~ as follows.
The red cells were lysed and the white cells separated by centrifugation at 2000r.p.m. for 10mins. A 14-ml aliquot of 6 mol/l guanidine chloride was added to the white cell pellet followed by 1.0 ml 7.5 M ammonium acetate, 1.0 ml 20 per cent N-lauryl sarcosine and 3 0 0 ~ 1 proteinase K 10mg/ml. The mixture was incubated at 55°C for 1 h. After cooling to room temperature, an equal volume of isopropanol was added. The DNA which appeared as strands in the isopropanol was spooled out, washed in 70 per cent ethanol and resuspended in 1.0ml Tris EDTA buffer solution at -20°C.
Where possible, archival tissue was obtained for family members who had died and DNA extractedI6 as follows. Xylene (1 ml) was added to the sample and a soft pellet obtained by microfugation at 13000r.p.m. for 5 min. The xylene was removed, 1 ml of 100 per cent ethanol added and the pellet broken down by shaking. A further microfugation at 13000 r.p.m. separated the ethanol which was poured off and the sample left to air-dry. Digestion was achieved by adding 75 pl of a mixture containing 0.5 mgiml proteinase K and 0.5 per cent Tween-20 (Sigma Chemicals, Poole, UK) and incubating overnight at 37°C. The sample was heated in a boiling water bath for 10min and the supernatant containing the extracted DNA was removed.
DNA typing was performed with six microsatellite DNA markers situated on the long arm of chromosome 17 which flank the region containing the BRCAl gene. The polymerase chain reaction (PCR) was used to ampllfy the DNA sequence delineated by each microsatellite marker".
A radioactive isotope (y"P-adenosine 5'-triphosphate) was included in the reaction mixture to label the DNA fragments. The alleles were separated according to size by acrylamide gel electrophoresis and autoradiography.
1086 0 1995 Blackwell Science Ltd
B R E A S T C A N C E R A N D BRCAZ 1087
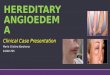
From the autoradiograph the allelic bands were read and numbered for each individual typed at that marker and a haplotype derived for each family member across the BRCAl region of chromosome 17.
The likelihood method of linkage analysisIx was used to calculate the probability that a family was linked to BRCAl by analysis of the haplotypes. This value was given as a logarithmic ratio, allowing combination of the results for different families as a lod scoreIK. A computer program analysed the haplotypes by the Linkage program produced by Ott'". A lod score'' of +3 equates to odds of 1000 to 1 in favour of linkage and a score of -2 excludes linkage by odds of 100 to 1. Individual family lod scores were used in combination with epidemiological data to estimate the lifetime risk of breast cancer for unaffected women in families with linkage2" to BRCAl.
Results From a total of 1033 women contacted, 164 families in which at least three women had developed breast cancer were identified. Home visits took place for 123 families (Table 1 ) and, of the remaining 41 families, 27 were reluctant to take any further part in the study, nine did not provide a telephone number and failed to respond to a posted request to arrange a home visit, and various family circumstances prevented five other visits. For four families the death of a family member from breast cancer meant that the family was too distressed to discuss details of the pedigree and one family moved to another part of the UK before a visit could be arranged.
Additional characteristics of hereditary disease noted in the families are shown in Table 2.
DNA was obtained from venous blood samples for affected and at-risk individuals from 24 families. For 10 families DNA from affected family members was obtained from archival tissue. In total, 260 DNA samples were extracted, 237 from venous blood samples and 23 from archival tissue specimens. For the majority of families DNA was obtained from three or more affected women, but for some, DNA from only two women with breast cancer was available. DNA from 77 affected women and from 183 at-risk women was utilized.
In an attempt to exclude families who did not show linkage to BRCAl, haplotype analysis was performed for
Table 1 Number of affected women per family
No. of affected women in family
No. of families identified
63 31 12 12 2 1 2
Table 2 Additional features of hereditary disease noted in the families
Feature of hereditary disease No. of families
Bilateral breast cancer 38 Ovarian cancer 22 Gastrointestinal cancer 27
affected family members. Clearly, if affected family members did not share a haplotype across the region containing BRCAl their disease could not be attributed to this gene. Seven families were excluded from further investigation in this manner.
For the remaining 17 families, the maximum lod scores obtained at each of the six microsatellite DNA markers are shown in Table 3. The individual family lod scores for family 5 are shown in Table 3.
Five families had a negative lod score for the markers and so are unlikely to be linked to BRCAl, and the maximum lod scores obtained when these five families are excluded from analysis are shown (Table 3). The combined maximum lod score for the residual 12 families at marker 42D6 is 5.46, which corresponds to odds of almost 400000 to 1 in favour of these families being linked to BRCAl.
Estimation of lifetime risk for breast cancer The calculations necessary for estimation of risk of breast cancer over a woman's lifetime of more than 80 years are dependent on a combination of epidemiological data and calculations based on individual family lod scores'O. Using family 5, which shows the highest individual lod scores, an unaffected woman from this family who shares an identical haplotype with affected women in the family across the BRCAl region of chromosome 17 has an estimated lifetime risk of developing breast cancer of approximately 80 per cent. However, for a woman from this family who does not share the BRCAl haplotype, the lifetime breast cancer risk is approximately 12 per cent, which is similar to that of the normal population2'.
Discussion In this study a large number of families prone to breast cancer were identified through a variety of sources, the majority through the Action Cancer screening charity organization, suggesting that many women are aware of the risk associated with a positive family history. Of these, 27 families were reluctant to discuss their family pedigree and nine did not respond to a request for a home visit. Many women will not want to know that they have inherited a genetic predisposition to breast cancer, and denial is a common reaction to the serious threat of breast cancer".
There are other reasons for unwillingness to discuss genetics and breast cancer risk, which may include concern for life events such as relationships, marriage and parenthood, career potential and even life or health insurancez3. For some women the knowledge of risk of
Table 3 Maximum lod scores obtained for the six DNA markers
DNA marker 1* 27 3*
D17S250 (mfdl.5) - 2.39 - 0.09 - 0.26 Thral - 0.15 - 0.50 + 0.86 D17S579 (mfd188) + 1.81 + 0.03 + 1.08 D17S588 (4206) + 3.12 + 0.86 + 5.46 NMEl (NM23) + 1.35 + 0.50 + 2.38 D17S587 (46E6) - 0.90 - 0.37 - 2.01
*Maximum lod scores at 8 = 0.05 for all families; ?maximum lod scores at 8=0.05 for family 5; *maximum lod scores at 8=0.05 for all families excluding five families without linkage to BRCAl
0 1995 Blackwell Science Ltd, British Journal of Surgery 1995,82, 1086-1088
1088 A. G . M c K I N L E Y , S . E . H. R U S S E L L , R . A . J . S P E N C E , W . O D L I N G - S M E E and N. C . N E V I N
breast cancer may be harmful, and predictive testing should not be offered to any woman without adequate counselling, psychological assessment and fully informed consentz2.
The criterion used to identify families with hereditary breast cancer in most studies is three or more affected women in a far nil^^-^. A total of 63 families was identified from the survey on this basis, while the other 60 families contained more affected individuals. Breast cancer is common in Northern Ireland, the incidence being 142 per 100 000 population2' and, although some families with three affected members did show evidence of linkage, a number of these families may represent chance sporadic clustering of the disease.
In the families identified there were 38 in which at least one woman had developed bilateral disease. This illustrates the penetrance of hereditary breast cancer genes and it has been estimated that the risk of developing a second breast cancer in a woman with a pedigree of breast cancer is almost 50 per cent over 20 years". It is suggested that a young woman from a family with breast cancer who develops breast cancer should be advised to undergo mastectomy rather than breast- conserving surgeryz3, and, to reduce the risk of breast cancer further, should consider bilateral mastectomy with r econ~ t ruc t ion~~ .
In addition to a history of breast cancer, there were 22 families in which at least one ovarian malignancy had developed and 27 in which at least one individual had gastrointestinal cancer. In similar studies such genetic h e t e r ~ g e n e i v - ~ has been a prominent feature and suggests that if families having breast cancer are considered for surveillance some may require screening for other malignancies.
From the original 123 families identified only 24 were suitable for DNA typing. The primary reason for this reduction in numbers was unavailability of DNA from affected women, as many of these women had died as a result of their disease.
From the 24 families, seven were excluded from further study as haplotype analysis showed that they could not be linked to BRCAl, and lod scores from linkage analysis excluded another five families as unlinked. This finding confirms previously published finding^^-^ that approximately 50 per cent of hereditary breast cancer families are not linked to BRCAl.
The risk estimation calculations included in this study illustrate the difficulty in attempting to include linkage data in clinical management. Only families with large lod scores will give risk estimations of sufficient accuracy to allow their incorporation into clinical management, and in this study only two families were suitablez0.
Genetic linkage analysis is of benefit in identifying which families are linked to BRCAl so that mutation analysis can be offered to unaffected women, allowing unequivocal identification of BRCAl carriers". At present only a very small number of women can be identified as non-BRCAl carriers at no increased risk of breast cancer.
References 1 Iselius L, Slack J, Littler M, Morton WE. Genetic
epidemiology of breast cancer in Britain. Ann Hum Genet
1991; 55: 151-9. 2 Claus EB, Risch NJ, Thompson WD. Genetic analysis of
breast cancer in the cancer and steroid hormone study. A m J Hum Genet 1991; 48: 232-4.
3 Houlston RS, McCarter E, Parbhoo S, Scurr JH, Slack J. Family history and risk of breast cancer. J Med Genet 1992; 29: 154-7.
4 Hall JM, Lee MK, Newman B et al. Linkage of early-onset familial breast cancer to chromosome 17q21. Science 1990;
5 Easton DF, Bishop DT, Ford D, Crockford GP. Genetic linkage analysis in familial breast and ovarian cancer: results from 214 families. The Breast Cancer Linkage Consortium. Am J f f u m Genet 1993; 52: 678-701.
6 Porter DE, Cohen BB, Wallace MR, Carothers A, Steel CM. Linkage mapping in familial breast cancer: improved localisation of a susceptibility locus on chromosome 17q12- 21. Int J Cancer 1993; 53: 188-98.
7 Bowcock AM, Anderson LA, Friedman LS et al. THRAl and D17S183 flank an interval of <4cM for the breast/ovarian cancer gene (BRCAI) on chromosome 17q21. A m J Hum Genet 1993; 52: 718-22.
8 Black DM, Solomon E. The search for the familial breast/ ovarian cancer gene. Trends Gen 1993; 9: 22-6.
9 Miki Y, Swenson J, Shattuck-Eidens D et al. A strong candidate for the breast and ovarian cancer susceptibility gene BRCAI. Science 1994; 266: 66-71.
10 Claus EB, Risch NJ, Thompson WD. Age at onset as an indicator of familial risk of breast cancer. Am J Epidemiol
11 Lynch HT, Harris RE, Organ CH Jr, Lynch JF. Management of familial breast cancer 2. Case reports, pedigrees, genetic counseling, and team concept. Arch Surg 1978; 113: 1061-7.
12 Lynch HT, Harris RE, Guirgis HA, Maloney K, Carmodey LL, Lynch JF. Familial association of breast/ovarian carcinoma. Cancer 1978; 41: 1543-9.
13 Lynch HT, Fain PR, Golgar D, Albano WA, Mailliard JA, McKenna P. Familial breast cancer and its recognition in an oncology clinic. Cancer 1981; 47: 2730-9.
14 Cole J, Conneally PM, Hodes ME, Merritt AD. Genetic family history questionnaire. J Med Genet 1978; 15: 10-18.
15 Jeanpierre M. A rapid method for the purification of DNA from blood. Nucleic Acids Res 1987; 15: 9611.
16 Shibata D, Martin WJ, Arnheim N. Analysis of DNA sequences in forty-year-old paraffin-embedded thin-tissue sections: a bridge between molecular biology and classical histology. Cancer Res 1988; 48: 4564-6.
17 Desforges JF. The polymerase chain reaction. A new method of using molecular genetics for medical diagnosis. N Engf J Med 1990; 322: 178-83.
18 Ott J. Analysis of Human Genetic Linkage. London: The Johns Hopkins University Press, 1985.
19 Lanthrop GM, Lalouel JM, Julier C, Ott J. Strategies for
250: 1684-9.
1990; 131: 961-72.
multilock linkage analysis in humans. Proc Natl A&d Sci (USA) 1984: 81: 3443-6.
20 Porter DE, Steel CM, Cohen BB et al. Genetic linkage analysis applied to unaffected women from families with breast cancer can discriminate high- from low-risk individuals. Br J Surg 1993; 80: 1381-5.
21 Northern Ireland Cancer Registration, Registrar Generals Report, Statistics and Research Bulletin. Belfast: Department of Health and Social Services, 1988-1990.
22 Birch JM, Easton D, Ponder B, Spurr N, Lane D, Craft A, Hopwood P. Management of women with a family history of breast cancer. Unpublished data from the Breast Cancer Family Study Group.
23 Evans DGR, Fentiman IS, McPherson K, Asbury D, Ponder BAJ, Howell A. Familial breast cancer. BMJ 1994; 308:
24 Leis HP Jr. Selective, elective, prophylactic contralateral 183-7.
mastectomy. Cancer 1971; 28: 956-61.
0 1995 Blackwell Science Ltd, British Journal of Surgery 1995. 82, 1086-1088