Embed Size (px)
Citation preview

Hepatitis C plus HIV: How bad is it?

Hepatitis

Mortality in the Americas-PAHO
Sistema Regional de Mortalidad, 2015. Pan American Health Organization. http://www.paho.org

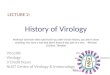
Estimated worldwide numbers of HIV/HCV co-infected individuals
Clausen LN et al. World J Gastroenterol 2014; 20:12132–12143.
HIV 33 million
HCV130–180 million
HIV/HCVco-
infection up to 10 million
Outbreaks in IDU & MSM

Global prevalence of HIV/HCV co-infection
Easterbrook P. International HIV/Viral Hepatitis Co-infection Satellite Meeting 2014. HCV, hepatitis C virus; IQR, inter-quartile ratio
2,500,000
2,000,000
1,500,000
1,000,000
500,000
0SouthEast Asia
Africa Eastern Europe
North America
Latin America
Western Pacific
Europe East Med
Burden of co-infection with HIV and HCV by region, 2013
Estimate Lower quartile Upper quartile
2.8 million(IQR: 1.6–5.9 million)

HCV :Natural History
10 to > 30 years

Progression of Liver Fibrosis Is Common in HIV Patients With HCV Coinfection1
• A prospective cohort study assessed the incidence of liver fibrosis progression in coinfected patients (N=282)
• On initial biopsy, 14% of patients had ≥ Metavir stage 2 fibrosis
• After a median follow-up 2.5 years:
1. Konerman MA et al. Hepatology. 2014;59:767–775.
Fibrosis progression
34%
Increase ≥2 Metavir stages
9%

FibrosisCirrhosis
LPS
HIV
HCV
• Direct effect on stellatecells
• Immune dysregulation• Cytokine alteration• Hepatocyte apoptosis
• Higher HBV and HCV chronicity rate
• Increased viral replication• Decreased HCV-specific
immune response
HAART
HCC
Adapted from Ingiliz P, Rockstroh JK, Current Opinion in HIV and AIDS 2015
HBV

Pathogenesis of HCV-related Liver Disease in HIV Patients With HCV Coinfection1
• HIV accelerates the progression of hepatic fibrosis via several T-cell independent mechanisms:
CCR4 = chemokine (C-C motif) receptor 5; CXCR4 = chemokine (C-X-C motif) receptor 4; NF-κB = nuclear factor kappa B; TGF-β1 = transforming growth factor beta 1; TLR-4 = toll-like receptor 4. 1. Sherman KE et al. Hepatology. 2014;59:307–317.
Upregulation of HCV replication - via signalling through CXCR4 and CCR5 co-receptors on hepatocytes1Enhanced fibrogenesis- via augmentation of HCV-related increases in TGF-β12NF-κB activation- via generation of reactive oxygen species3Independent induction of hepatocyte apoptosis4Microbial translocation in the gut- via TLR-4 on hepatocytes and stellate cells5
9

HIV/HCV co-infection burden: Accelerated disease progression and morbidity
• Prevalence, especially in some populations1–3
• Compared with HCV mono-infected patients, patients co-infected with HIV display: – viraemia (2–8-fold greater)1,4
• infectivity increases risk of transmission from mother to child (20% vs 6%) and risk of sexual transmission (3% vs <1%)1,5
– likelihood of spontaneously clearing HCV1,4
– hepatic fibrosis (2–5-fold greater), cirrhosis, decompensation, hepatocellular carcinoma and liver-related mortality1,5
1. World Health Organization. Protocol 6. Management of hepatitis C and HIV coinfection. WHO Regional Office for Europe 2007; 2. Wiessing L, et al. Euro Surveill 2011;16:pii:20031; 3. Taylor LE, et al. Clin Infect Dis 2012;55(S1):S33–42; 4. Sherman KE, et al. Gastroenterology 2005;128:313–27; 5. Vallet-Pichard A, Pol S. J Hepatol 2006;44(S1):S28–34.

Impact of HIV RNA, CD4, or Both on Liver Fibrosis Progression Rate
0
10
20
30
40
50
60
HIV RNA(copies/mL)
Est
imat
ed T
ime
From
HC
VIn
fect
ion
to C
irrh
osis
(yea
rs)
P=0.05 P=0.04
P=0.005 P=0.004 P=0.005
<400(n=141)
CD4(cells/mm3)
HIV RNA (copies/mL) +<500 CD4 cells/mm3
Brau N, et al. J Hepatol. 2006;44:47-55
49
400-99K(n=117)
>100k(n=16)
>350(n=124)
<350(n=150)
<400(n=100)
>400(n=88)
41
31
50
39
49
37
Time to cirrhosis estimated using liver fibrosis progressionrate based on Ishak Fibrosis units/year.

Impact of ART on Overall Liver Mortalityin HIV/HCV-Coinfected Patients
• Bonn cohort (1990-2002)– 285 HIV/HCV coinfected
patients• Liver-related mortality rates per
100 person-years– HAART: 0.45– ART: 0.69– No therapy: 1.70
• Predictors for liver-related mortality
– No HAART– Low CD4 cell count– Increasing age
Qurishi N, et al. Lancet. 2003:362:1708-1713.
0,2
0,4
0,6
0,8
1
Days
Overall Mortality
Cum
ulat
ive
Surv
ival
0 1000 2000 3000 4000 5000 6000
ART
HAART*
0,2
0,4
0,6
0,8
1
Days
Liver-Related Mortality
Cum
ulat
ive
Surv
ival
0 1000 2000 3000 4000 5000 6000
HAART*
No therapy
ART
No therapy
*P=0.018
*P<0.001

What is the optimal treatment strategy in HIV/HCV co-infected patients?
Treat HCV first?
Treat HIV first?
Treat HIV/HCV simultaneously?

0123456789
10
HIV Suppression Is Associated with Less Hepatic Necroinflammatory Activity
Mehta SH et al. Hepatology 2005
Activ
ity S
core
Viral LoadUndetectable
Viral LoadDetectable
**

Liver Toxicity due to HAART
• 14-20% of patients will develop elevated liver enzymes.• 2-10% of patients will need to interrupt HAART due to
severe liver injury.• Risk factors:• Viral hepatitis B or C• First regimen• Nevirapine• Full dose ritonavir• Female sex
J Infect Dis 2002; 186:23-31
Avoid mitochondrial toxicity

ARVs and Liver Disease
Slide credit: clinicaloptions.comDHHS Guidelines. January 2016. DTG/3TC/ABC [package insert]. 2016.
ART Drug Class Liver Toxicity
NRTI
Reported with most NRTIs Steatosis most common with ZDV, d4T, or ddI ddI: Prolonged exposure linked to noncirrhotic portal HTN, esophageal varices Flares: HIV/HBV-coinfected pts may develop severe hepatic flares when TDF, 3TC, and
FTC are withdrawn or when HBV resistance develops Dose adjust ABC
NNRTI
NVP > other NNRTIs NVP: Severe hepatotoxicity associated with skin rash or hypersensitivity. Risk greater for
women with pre-NVP CD4+ cell count > 250 cells/mm3 and men with pre-NVP CD4+ cell count > 400 cells/mm3. NVP in pts with hepatic insufficiency (CP B or C)
Use EFV with caution in liver disease
PI
All PIs: Drug-induced hepatitis and hepatic decompensation have been reported; greatest frequency with TPV/RTV
TPV/RTV contraindicated in CP B or C; DRV contraindicated in CP C Dose adjust ATV, FPV, IDV No boosting in CP B or C
INSTI DTG/3TC/ABC associated with severe acute exacerbations of hepatitis, which are
primarily described in HBV-coinfected pts DTG and EVG not recommended in CP C

Antiretroviral therapy reduces the rate of hepatic decompensation among HIV- and hepatitis C virus-coinfected veterans
Objective: To evaluate 10,090 HIV/HCV-co-infected
males from the Veterans Aging CohortStudy Virtual Cohort, who had notinitiated ART at entry, for incidenthepatic decompensation between1996 and 2010
Results: Initiation of ART significantly reduced the rate of hepatic decompensation
by 28–41% on average
Anderson JP, et al. Clin Infect Dis 2014; 58(5): 719–27.17

HCV Disease Progression Remains Faster in Coinfected Patients, Despite Effective ART
ART, antiretroviral therapy; HCV, hepatitis C virus; HIV, human immunodeficiency virus.
1. Adapted from: Lo Re 3rd V, et al. Ann Intern Med 2014;160:369–79.
If HIV RNA <1000 copies/mL: +65% excess riskIf HIV RNA >1000 copies/mL: +82% excess risk
If CD4 < 200/mm2: +203% excess riskIf CD4 > 200/mm2: 56–63% excess risk
Time to hepatic decomposition (years)
HCV-monoinfected patientsAntiretroviral-treatment patients coinfected withHIV/HCV: HIV RNA level < 1000 copies/mLAntiretroviral-treatment patients coinfected withHIV/HCV: HIV RNA level ≤ 1000 copies/mL
0.1
0.2
0.0
0.0760.0690.048
0 1 2 3 4 5 6 7 8 9 10
Cum
ulat
ive
inci
denc
e
0.081
0.0690.048
0 1 2 3 4 5 6 7 8 9 10
HCV-monoinfected patientsAntiretroviral-treatment patients coinfected withHIV/HCV: CD4 count < 0.200 x 109 cells/LAntiretroviral-treatment patients coinfected withHIV/HCV: CD4 count ≥ 109 cells/L
Cum
ulat
ive
inci
denc
eTime to hepatic decomposition (years)
0.1
0.2
0.0
18

100%
?
19911989
FDA approves RBV to combine with IFN
FDA approves IFN as the first therapy
Discovery of HCV
New Era of HCV Therapy

NS3 inhibitor2
• Inhibits activity of NS3 protease
• Prevents processing of HCV proteins required for replication
NS5B inhibitor(s)2
• Inhibits NS5B RNA replicase
• Prevents replication of viral genome
NS5A inhibitor2
• Inhibits activity of NS5A, a multifunctional protein
• Prevents viral replication
HCV life cycle
HCV virion
New HCV virion
PEG-IFN lambda3
• Type III pegylatedinterferon
• Expression of receptor is more limited than Alfa, should lead to improved tolerability and safety
1. Manns MP, et al. Nat Rev Drug Discov 2007;6:991–1000. 2. Rice C. Top Antivir Med 2011;19(3):117–20. 3. Donnelly R, et al. Trends Immunol 2011;32(9):443–50. 4. Gallay P, Lin K. Drug Des Devel Ther 2013;7:105-15.
Endocytosis
SR-B1
CD81
Cytoplasm
Liver cell
ER
Maturation
Nucleus
Uncoating
RNA replication
Virionassembly
Golgi
Adapted from reference 1
ER Lumen Adapted from reference 2
Cytoplasm
NS4A NS4B
Cyclophilin Ainhibitor4
• Inhibition of cyclophilin A reduces HCV replication
-previr
-asvir
-buvir

Benefits of SVR
↓ Chirrosis↓ Descompensation
↓ HCC↓ Transplant
↓ MortalityNeoplasiasDiabetes
CVDRenal
NeurocognitiveQoL improvement
Cure!
Clinical improvement[1,2]
1. Smith-Palmer J, et al. BMC Infect Dis. 2015;15:19.2. Negro F, et al. Gastroenterology. 2015;149:1345-1360.3. George SL, et al. Hepatology. 2009;49:729-738.
Hepatic Extrahepatic
Reduced Transmission [1]

22

EASL & AASLD SnapshotSV
R24
(%)
0
10
20
30
40
50
60
70
80
90
100
100%

Current therapies
Protease (NS3/4a) NS5a (assembly complex) NS5b (RNA-polymerase)
Telaprevir
Boceprevir
Simeprevir
Paritaprevir
Grazoprevir
Sofosbuvir
Sofosbuvir
Dasabuvir*
Sofosbuvir
Daclatasvir
Ledipasvir
Ombitasvir
Elbasvir
Velpatasvir
* non-nucleoside RNA polymerase inhibitor

Current All-Oral Regimens for HCV Infection
Regimen Component Classes Approved Genotypes
Grazoprevir/elbasvir Protease inhibitor + NS5A inhibitor 1, 4
Ombitasvir/paritaprevir/ritonavir Protease inhibitor + NS5A inhibitor 4
Ombitasvir/paritaprevir/ritonavir + dasabuvir
Protease inhibitor + NS5A inhibitor +
polymerase inhibitor1
Sofosbuvir + daclatasvir Nucleotide polymerase inhibitor + NS5A inhibitor 1, 3
Sofosbuvir/ledipasvir Nucleotide polymerase inhibitor + NS5A inhibitor 1, 4, 5, 6
Simeprevir + sofosbuvir Nucleotide polymerase inhibitor + protease inhibitor 1
Sofosbuvir/velpatasvir Nucleotide polymerase inhibitor + NS5A inhibitor 1, 2, 3, 4, 5, 6
References in slidenotes.

Slide credit: clinicaloptions.com
AASLD Guidance: HCV/HIV Coinfection
All pts with HCV should be treated– Pts with cirrhosis among highest priority for treatment– HCV/HIV coinfection among high priority for treatment
Even in this era of potent HIV antiretrovirals, pts with HCV/HIV coinfection are at greater risk for rapidly progressive fibrosis and cirrhosis
“HIV ARV therapy is not a substitute for HCV treatment”
AASLD/IDSA. HCV guidance. July 2016.

Summary of DDIs Between HCV and HIV Therapies
SMV + SOF[1] LDV/SOF[1] DCV +
SOF[1]OBV/PTV/RTV
+ DSV[1] EBR/GZR[1] SOF/VEL[1]
ATV + RTV Χ ≈ ≈ √ Χ ≈
DRV + RTV Χ ≈ √ ≈[5] Χ ≈
Tipranavir + RTV Χ Χ Χ Χ Χ Χ
EFV or ETR Χ √ ≈ Χ Χ Χ
RPV √ √ √ Χ √ √
DTG or RAL √ √ √ √ √ √
EVG + COBI Χ ≈ √ Χ Χ ≈
3TC/ABC √ √ √[4] √ √ √
TAF √[2] √[3] √* √* √[2] √
TDF √ ≈ √ √ √ ≈
Slide credit: clinicaloptions.com
1. AASLD/IDSA HCV Guidance. July 2016. 2. NY/NJ AETC. 2016. 3. Custodio J, et al. IDWeek 2015. Abstract 727. 4. Liverpool Drug Interactions Group. 5. Wyles D, et
al. CROI 2016. Abstract 574.
No clinically significant interaction expected
Potential interaction may require adjustment to dosage, timing of administration, or monitoring
Do not coadminister*No data.

Recommendations for LDV/SOF Use in HCV/HIV Coinfection
Slide credit: clinicaloptions.comAASLD/IDSA. HCV guidance. July 2016.
LDV/SOF Can be used with most ARVs Avoid use with TDF in pts with CrCl < 60 mL/min Avoid use with TDF + RTV or COBI (pending more data) For pts receiving RTV- or COBI-containing ART, TAF may be
an alternative to TDF during LDV/SOF therapy SOF-based regimens should NOT be used with TPV For combinations anticipated to increase TFV levels,
perform baseline and ongoing monitoring for nephrotoxicity

Recommendations for DCV + SOF Use in HCV/HIV Coinfection
Dose adjustment needed for DCV when used with ATV/RTV, EFV, or ETR, but DCV + SOF not coformulated, allowing adjustment of DCV dose
Slide credit: clinicaloptions.comAASLD/IDSA. HCV guidance. July 2016.
DCV + SOF Decrease DCV dose to 30 mg daily with RTV-boosted ATV
Increase DCV dose to 90 mg daily with EFV or ETR
SOF-based regimens should NOT be used with TPV

Recommendations for OBV/PTV/RTV + DSV Usein HCV/HIV Coinfection
Phase II study of OBV/PTV/RTV + DSV + RBV in HCV/HIV coinfection included pts with ATV- or RAL-based ART only[1]
Slide credit: clinicaloptions.com1. Sulkowski MS, et al. JAMA. 2015;313:1223-1231. 2. AASLD/IDSA. HCV guidance. July 2016.
OBV/PTV/RTV + DSV[2]
ARVs without substantial interactions: 3TC, ATV, DTG, ENF, FTC, RAL, and TDF
Should NOT be used with DRV, EFV, RTV-boosted LPV, RTV-boosted TPV, ETR, NVP, COBI, or RPV
If using with other RTV-boosted HIV PI, RTV dose may need to be adjusted (or held) during OBV/PTV/RTV + DSV coadministration; HIV PI should be administered at the same time as the fixed-dose HCV combination
Should NOT be used in HCV/HIV-coinfected individuals who are not on ART

Recommendations for SOF/VEL Use in HCV/HIV Coinfection
Slide credit: clinicaloptions.comAASLD/IDSA. HCV guidance. July 2016.
SOF/VEL Can be used with most ARVs, but should NOT be used with EFV,
ETR, or NVP Avoid use with TDF in pts with CrCl < 60 mL/min In pts with CrCl > 60 mL/min, coadministration of VEL and TDF
with RTV or COBI did not lead to renal toxicity in 56 pts; renal monitoring is recommended
For pts receiving RTV- or COBI-containing ART, TAF may be an alternative to TDF during SOF/VEL therapy
SOF-based regimens should NOT be used with TPV For combinations anticipated to increase TFV levels, perform
baseline and ongoing monitoring for nephrotoxicity

96 95 97 96 94
0
20
40
60
80
100
SVR1
2 (%
)
nN
321335
179185
142150
258268
6367
LDV/SOF(N=335)
0 12Study Weeks
Ledipasvir/sofosbuvir for 12 Weeks in Patients Coinfected with HCV and HIV-1: ION-4
Efficacy Results:GT1 and 4 with HIV/HCV co-infectionStudy Design:
GT1 and 4 with HIV/HCV co-infection*
Cooper C, et al; 8th IAS, Vancouver, Canada, July 19-22, 2015; Abst. TUAB0202 and Naggie S, N Engl J Med 2015.

ALLY-2: DCV+SOF in HIV/HCV Coinfection
0
20
40
60
80
100
SVR1
2, %
𝟖𝟖𝟖𝟖𝟖𝟖𝟖𝟖
𝟒𝟒𝟖𝟖𝟒𝟒𝟒𝟒
𝟖𝟖𝟑𝟑𝟒𝟒𝟑𝟑
12-WeekNaive
12-WeekExperienced
𝟗𝟗𝟖𝟖𝟑𝟑𝟖𝟖𝟑𝟑
𝟖𝟖𝟖𝟖𝟓𝟓𝟖𝟖
𝟓𝟓𝟑𝟑𝟓𝟓𝟓𝟓
8-WeekNaive
GT 1
PrimaryEndpoint
0
20
40
60
80
100
𝟗𝟗𝟖𝟖𝟑𝟑𝟖𝟖𝟑𝟑
𝟓𝟓𝟑𝟑𝟓𝟓𝟓𝟓
𝟖𝟖𝟖𝟖𝟓𝟓𝟖𝟖
All Patients
96 98 76 97 98 76
12-WeekNaive
12-WeekExperienced
8-WeekNaive
Wyles D, et al. 50th EASL; Vienna, Austria; April 22-26, 2015. Abst. LP01 and Wyles D, et al. N Engl J Med 2015.

Rockstroh JK, et al. Lancet HIV. 2015;2:e319-e327
0
1008060
20
C-EDGE Coinfection: Grazoprevir/Elbasvir
for 12 Wks in HIV/HCV Coinfection
SVR
12 (%
)
139/
144
42/44
27/28
All Pts GT1a GT1b
GT4
96.3 96.5 95.5 96.4
210/218
Discontinued* 1 0 1 0
Relapse 5 4 0 1
Reinfection 2 1 1 0
*Unrelated to virologic failure.
n/N =
40
Slide credit: clinicaloptions.com
• N = 218 HCV treatment-naive pts; 66% genotype 1a HCV, 60% had HCV RNA > 800,000 IU/mL, 16% cirrhotic
– New NS3, NS5A RAVs detected at failure in 4 of 5 pts who relapsed• No pt discontinued for AEs and no serious treatment-related AEs

ASTRAL-5: Sofosbuvir/Velpatasvir for 12 Wks in HIV/HCV Coinfection
Slide credit: clinicaloptions.com
• N = 106 pts; HCV treatment experienced: 29%, compensated cirrhosis: 18%, BL NS5A RAVs: 12%
– Of 2 relapses, 1 treatment experienced, neither with cirrhosis or BL NS5A RAVS• No significant effect on CrCl regardless of TDF use with or without boosted ARV
Wyles D, et al. EASL 2016. Abstract PS104.
n/N =
100
80
60
40
20
0
SVR
12 (%
)
All Pts 1a 1b 2 3 4 No Yes No YesGenotype Cirrhosis Tx
Experienced
95 95 92 100 92 100 94 100 93 97
99/ 104
62/65
11/12
11/11
11/12
4/4
80/85
71/75
28/29
19/19n/N =

Wyles, AASLD 2014 #1939 and Sulkowski M, et al. JAMA 2015
HIV-HCV Coinfection study: TURQUOISE-I: 3 DAAs + RBV

The ideal DAA..
Pangenotypic Efficacy Short duration regimens No ribavirin required Efficacious in patients failing DAAs Active in genotype 3Without drug interactions No limitations in renal insufficiency Affordable cost
3

Hepatitis C Is an INFECTIOUS Virus: Treatment as Prevention
Slide credit: clinicaloptions.com
1. Terrault NA, et al. Hepatology. 2013;57:881-899. 2. Thomas SL, et al. Int J Epidemiol. 1998;27:108-117. 3. Larsen C, et al. PLoS One. 2011;6:1-9. 4. Shepard CW, et al. Lancet Infect Dis. 2005;5:558-567.
Infection in monogamous heterosexual couples is rare[1]
Risk of transmission from mother to child is low[2]
Sex between men who are HIV-positive increases the risk of contracting HCV[3]
People who inject drugs account for the majority of new cases of HCV in developed countries[4]

Treatment Can Prevent Onward Transmission
• Observed and modeled HCV chronic prevalence among PWID in Melbourne, Australia
Martin NK, et al. Hepatology. 2013;58:1598-1609. Slide credit: clinicaloptions.com
HCV
Chro
nic P
reva
lenc
e Am
ong
PWID
(%)
Yr
DataNo scale-up from baseline (3/1000 PWID annually)Scale-up to 10/1000 PWID annuallyScale-up to 20/1000 PWID annuallyScale-up to 40/1000 PWID annuallyScale-up to 80/1000 PWID annually
100
80
60
40
20
02007 2012 2017 2022 20272002
90
70
50
30
10


Global Call for HCV Elimination
• Vision: “A world where viral hepatitis transmission is stopped and everyone has access to safe, affordable, and effective treatment and care”– 2020 target: 3 million HCV infections treated
• Feasible by scaling up 6 key interventions to high coverage:– Hepatitis B vaccination (including birth dose)
– Safe injection practices and safe blood
– Harm reduction for injecting drug users
– Safer sex (including condom promotion)
– Hepatitis B treatment
– Hepatitis C cure
Slide credit: clinicaloptions.comWHO. Towards the elimination of hepatitis B and C by 2030. Draft WHO Global Hepatitis Strategy, 2016-2021.
2030 Targets90% Diagnosed
80% Treated
65% Reduced Mortality

Chronic hepatitis C and HIV: Conclusions
• HIV infected individuals with HCV coinfection remain at higher risk for fibrosis progression and hepatic decompensation
• Therefore HCV therapy is prioritized in most guidelines in this patient group
• The short- and mid-term effects of ART on the progression of HCV-related liver disease largely outweigh the potential risks for long-term toxicity
• Consider drug interactions• HCV therapy as a case of TasP?• Safe and even better options are just around the corner