Embed Size (px)
Citation preview

Hepatic Involvement in Hodgkin ’s Disease
Clues to Histologic Diagnosis
NGUYEN HUU DICH, MD, MAJ, MC,* ZACHARY D. GOODMAN, MD, LTC, MC, AND MICHAEL A. KLEIN, MD, LTC, MCt
The hepatic histopathology was studied in 125 patients with Hodgkin’s disease to determine whether there are any features other than Reed-Sternberg (RS) cells that might aid in the diagnosis of hepatic involvement by the neoplastic process. Liver biopsy specimens from 41 patients with Hodgkin’s disease in the liver were compared with biopsy specimens from 84 patients without hepatic involvement. Patients with hepatic involvement by Hodgkin’s disease are much more likely to have histologic evidence of portal infiltrates larger than 1 mm in diameter (78% versus l a ) , acute cholangitis (85% versus 4%), portal edema (90% versus 8%), and portal infiltrates with a predominance of atypical lymphocytes (78% versus 12%) than patients with Hodgkin’s disease who do not have hepatic involvement. When these features are observed alone or in combination in a liver biopsy specimen from a patient with proven or suspected Hodgkin’s disease, a diligent search for RS cells is indicated, with serial sections and repeat biopsy if necessary.
Cancer 64:212 1-21 26, 1989.
HE LIVER is one of the most common extranodal T sites to be routinely examined in Hodgkin’s disease, and because hepatic involvement indicates Stage IV dis- ease, it is a critical element in the therapeutic approach to the patient. However, the diagnosis of Hodgkin’s disease in a liver biopsy specimen may be difficult due to the small size of many biopsy specimens and the sparsity of diagnostic Reed-Sternberg (RS) cells or acceptable RS variants. Furthermore, liver biopsy specimens from pa- tients with Hodgkin’s disease frequently show a variety of nonspecific inflammatory changes that can cause con- fusion in the histologic diagnosis of hepatic involvement by the neoplastic process. Several publications have de- scribed these nonspecific changes, emphasizing the need to distinguish between these and hepatic Hodgkin’s dis-
From the Department of Pathology, Walter Reed Army Medical Cen- ter, and the Department of Hepatic Pathology, Armed Forces Institute of Pathology, Washington, DC.
* Current address: Department of Pathology, Brooke Army Medical Center, San Antonio, Texas.
t Current address: Boyce and Bynum Pathology Professional Service, Columbia, Missouri.
The authors thank Mr. Charles Brown and Ms. Robin-Anne Fems for assistance in the preparation of the photomicrographs.
Address for reprints: Zachary D. Goodman, MD, Department of He- patic Pathology. Armed Forces Institute of Pathology, Washington. DC 20306.
The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the Department of the Army or the Department of Defense.
Accepted for publication June 14, 1989.
ease.’-6 Patients who have Hodgkin’s disease in the liver also may have associated inflammatory changes. This study was undertaken to compare the inflammatory changes in patients with and without hepatic involvement to determine whether there are qualitative or quantitative differences that would suggest the presence of Hodgkin’s disease when acceptable RS cells are difficult or impossible to find.
Materials and Methods
Cases of Hodgkin’s disease in which liver biopsies had been performed were selected from the files of Walter Reed Army Medical Center (46 cases) and the Armed Forces Institute of Pathology (AFIP) (79 cases). The orig- inal diagnostic material was reviewed to confirm the di- agnosis of Hodgkin’s disease, and any questionable or equivocal cases were excluded. In five cases, the diagnosis had been made primarily on a liver biopsy specimen. In the remaining cases, the diagnosis had been made on one or more lymph nodes.
There were 308 liver biopsy specimens from 125 pa- tients available for review. These included 137 wedge and 143 needle biopsies performed as part of initial staging laparotomies and 28 biopsies (18 needle and 10 wedge) performed at other times during the patient’s course of treatment. One patient had five different biopsy specimens (obtained during a single procedure), 22 had four, 14 had three, 49 had two, and 39 had only one. The original
2121
2122 CANCER November I5 1989 Vol. 64
hematoxylin and eosin (H & E) stained sections were re- viewed in all cases, and Masson and periodic acid-Schiff (PAS) stains were reviewed when available. For hepatic involvement by Hodgkin’s disease, Lukes’ criteria for ex- tranodal manifestations were used.’ When the diagnosis of Hodgkin’s disease had been established in a lymph node, mononuclear vanants of RS cells in an appropriate background were sufficient to diagnose hepatic involve- ment. When liver tissue was the only material examined, as in five of our cases, classic multinucleated RS cells were required.
Each liver biopsy specimen was examined for the pres- ence of lymphoreticular infiltrates that were defined as either nonspecific infiltrates or malignant infiltrates. A nonspecific infiltrate was an aggregate of 20 or more in- flammatory cells, predominantly lymphocytes, that also invariably contained other cells such as histiocytes, plasma
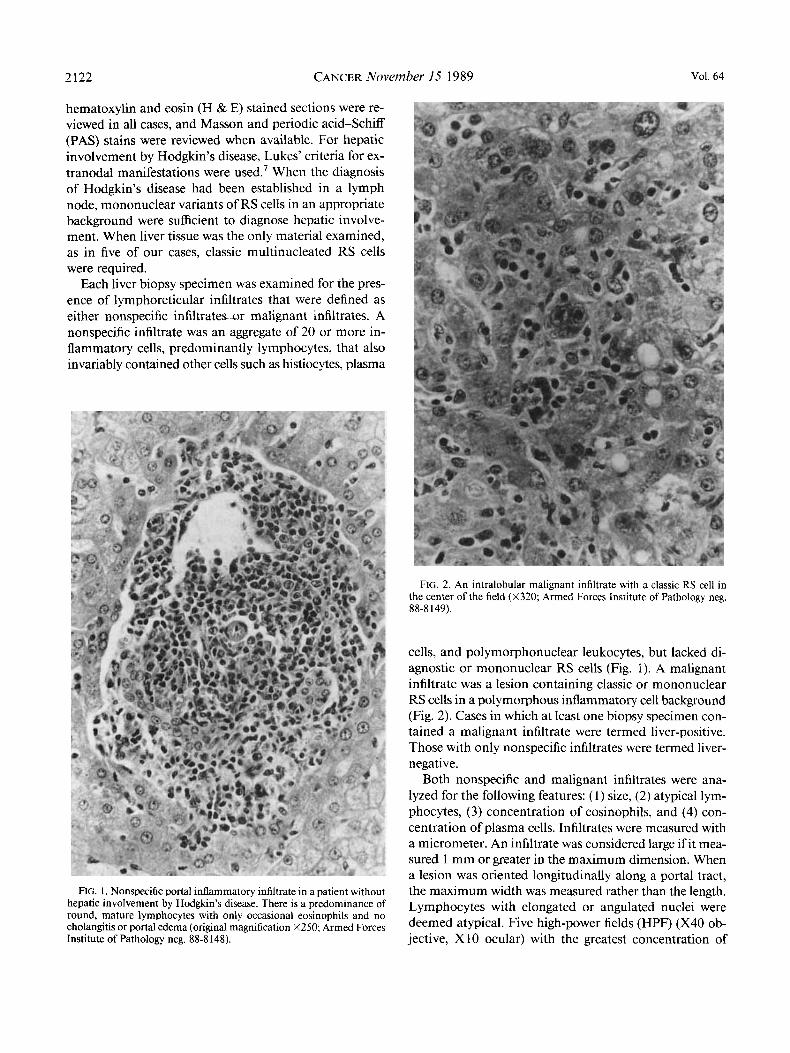
FIG. 2. An intralobular malignant infiltrate with a classic RS cell in the center of the field (X320 Armed Forces Institute of Pathology neg. 88-8 149).
cells, and polymorphonuclear leukocytes, but lacked di- agnostic or mononuclear RS cells (Fig. 1). A malignant infiltrate was a lesion containing classic or mononuclear RS cells in a polymorphous inflammatory cell background (Fig. 2). Cases in which at least one biopsy specimen con- tained a malignant infiltrate were termed liver-positive. Those with only nonspecific infiltrates were termed liver- negative.
Both nonspecific and malignant infiltrates were ana- lyzed for the following features: (1) size, (2) atypical lym- phocytes, (3) concentration of eosinophils, and (4) con- centration of plasma cells. Infiltrates were measured with a micrometer. An infiltrate was considered large if it mea- sured l mm or greater in the maximum dimension. When a lesion was oriented longitudinally along a portal tract,
FIG. 1. Nonspecific portal inflammatory infiltrate in a patient without the maximum width was measured rather than the length. hepatic involvement by Hodglun’s disease. There is a predominance of Lymphocytes with elongated or angulated nuclei were round, mature lymphocytes with only occasional eosinophils and no cholangitis or portal edema (original magnification X250; Armed Forces deemed Five high-power (HPF) (x40 Ob- Institute of Pathology neg. 88-8 148). jective, X 10 ocular) with the greatest concentration of

No. 10 HEPATIC INVOLVEMENT IN HODGKIN’S DISEASE - Dich ct ul. 2123
atypical lymphocytes were examined; a predominance of atypical lymphocytes was considered to be present when the number of atypical cells exceeded 5070 of the total number of lymphocytes. The degree of atypia was mild in all cases, with irregular nuclear contours but without indentation of the nuclear membrane (Fig. 3). Any case with a predominance of markedly atypical lymphocytes was excluded, as this finding invariably raised doubt about the diagnosis. The concentration of eosinophils was de- termined by the mean number of eosinophils counted in the five HPF with the greatest concentration. Eosinophilia was considered to be present when the number exceeded 30/HPF. The concentration of plasma cells was considered high when there were ten or more plasma cells per HPF in the five fields with the greatest number.
The liver biopsy specimens also were examined for the presence of the following features: ( 1 ) cholangitis, (2) por- tal edema, ( 3 ) atrophy of liver cell plates, (4) acidophilic bodies, ( 5 ) Kupffer cell hypertrophy, and (6) cholestasis. Acute inflammation in or around the interlobular bile ducts associated with injury of the ductal epithelium was considered cholangitis (Figs. 3 and 4). The biliary epithelial
FIG. 4. Portal area adjacent to a malignant infiltrate. Two bile ducts are infiltrated by neutrophils (acute cholangitis). There is marked portal edema and a predominance of atypical lymphocytes (X250; Armed Forces Institute of Pathology neg. 88-8 15 I ).
cells might be stratified, enlarged, vacuolated, flattened, or swollen. On occasion they were detached from the basement membrane. Cell borders were often blurred, and mitotic figures were sometimes present, Portal edema was seen as loose portal connective tissue with separation of the collagen bundles (Figs. 3, 4, and 5 ) . Narrowing of the cell plates between sinusoids was considered atrophy of liver cell plates. Acidophilic bodies were seen as remnants of necrotic liver cells and Kupffer cell hypertrophy was seen as enlargement of the sinusoidal macrophages. Bile pigment in hepatocytes, canaliculi, cholangioles, or bile ducts was considered cholestasis.
Associations between variables were tested for inde- pendence using Fisher’s exact test.
Results
Hodgkin’s disease was present in biopsy specimens from 41 (3370) of the 125 patients. These included nine of 46
FIG. 3. Portal area with a malignant infiltrate. Although no RS cells are present in this field, there is a predominance of atypical lymphocytes (X480; Armed Forces Institute of Pathology neg. 88-8 150).

2124 CANCER November 15 1989 Vol. 64
FIG. 5. Portal area adjacent to a malignant infiltrate. There is mild portal edema recognized as separation of the portal collagen bundles. The edema fluid has a pale blue appearance with a Masson trichrome stain (X 140; Armed Forces Institute of Pathology neg. 88-8152).
cases from Walter Reed Hospital and 32 of 79 cases from the AFIP, reflecting the nature of consultation material submitted to the AFIP. Nonspecific inflammatory infil- trates were present in 1 12 (90%) of the cases; 41 (100%)
TABLE I . Distribution of Hepatic Infiltrates in 125 Patients With Hodgkin’s Disease (Liver-Positive Cases [n = 411 Compared With Liver-Negative Cases In = 841)
~ ~~
Portal Intralobular Portal & only only intralobular None Total
~~~
Malignant infiltrates 22 3 16 0 41 Nonspecific infiltrates
in liver positive cases 8 0 33 0 41
Nonspecific infiltrates in liver negative cases 30 5 36 13 84
of the positive and 71 (85%) of the negative cases. In 13 cases no infiltrates, neoplastic or nonspecific, were found.
Both malignant and nonspecific infiltrates were seen more frequently in portal areas than in the hepatic pa- renchyma (Table l). A significant number of biopsy spec- imens contained both portal and intralobular infiltrates. The distribution did not, however, seem to differ between liver-positive and liver-negative cases.
Overall, the distribution of lesions was patchy. The size, shape, and cellular components vaned from field to field, portal tract to portal tract, and even from one area to another within the same portal tract. Virtually normal portal tracts were frequently seen adjacent to malignant lesions. Twenty liver-positive patients had more than one biopsy performed during the same staging procedure. Only five of the 20 cases demonstrated malignancy in all spec- imens, whereas 15 (75%) had both positive and negative biopsy specimens, thus demonstrating the value of mul- tiple biopsy specimens.
The histologic features of the infiltrates were compared between the liver-positive cases and the liver-negative cases (Table 2). There were statistically significant differences between the two groups in all variables examined except for plasma cells. Most significantly, there were large dif- ferences between positive and negative cases in the fre- quency of large infiltrates (78% versus l%), cholangitis (85% versus 4%), portal edema (90% versus 8%), and a predominance of atypical lymphocytes (78% versus 12%). More importantly, when the analysis was limited to in- filtrates that lacked diagnostic RS cells or RS variants, there were still highly significant differences in these vari- ables (Table 3). That is, when no RS cells could be found, it was still possible to suspect the presence of Hodgkin’s disease when there were large infiltrates (especially with
TABLE 2. Frequency of Histologic Features i n Liver Biopsy Specimens From Patients With Hodgkin’s Disease
Liver-positive Liver-negative (n = 41) (n = 84) Pvalue
Large infiltrates 32 (78%) 1(1%) Acute cholangitis 35 (85%) 3 (4%) Portal edema 37 (90%) 7 (8%) Infiltrates with atypical
lymphocytes 32 (78%) 10 (12%) Eosinophils (30/HPF) 12 (29%) 1 ( 1 % ) Plasma cells (lO/HPF) I(2%) 1 (1%) Atrophy liver cell
Kupffer cell plates 15 (37%) 10 (12%)
hypertrophy 40 (98%) 45 (54%) Acidophilic bodies 1 1 (27%) 2 (2%) Cholestasis 4 (10%) 0
H P F high-power fields; NS: not significant.
<o.oo 1 <0.001 <0.001
<o.oo 1 <0.001
NS
<0.001
<0.001 <0.001 <0.02

No. 10 HEPATIC INVOLVEMENT IN HODGKIN’S DISEASE - Dich et al. 2125
TABLE 3. Morphologic Features of Nonspecific Infiltrates (Lacking RS Cells and RS Variants) in Liver-Positive Cases
Compared With Liver-Negative Cases
Liver-positive Liver-negative (n = 41) (n = 84) Pvalue
Large infiltrates 22 (54%) l ( I % ) t0.00 1 Acute cholangitis 28 (68%) 3 (4%) <0.001 Portal edema 35 (85%) 7 (8%) <o.oo 1 Infiltrates with atypical
lymphocytes 28 (68%) 10 (12%) <0.001 Eosinophils (3O/HPF) 5 (12%) 1(l%) <0.02 Plasma cells (IO/HPR 1(2%) 1(1%) NS
RS: Reed-Stemberg; HPF: high-power fields; NS: not significant.
atypical lymphocytes), portal edema, and acute cholan- gitis.
Although acute cholangitis was a frequent finding in the liver-positive group, this was typically patchy in dis- tribution, similar to the distribution of the Hodgkin’s dis- ease. Cholestasis and other histologic features of mechan- ical biliary obstruction were infrequent findings. Other histologic features were found to differ between the pos- itive and negative groups (Table 2), but were less useful than those discussed above in distinguishing individual cases. Livers with Hodgkin’s disease were significantly more likely to have atrophy of the liver cell plates (37% versus 12%), Kupffer cell hypertrophy (98% versus 54%), and acidophilic bodies (27% versus 2%), but the predictive value of these was low. Numerous eosinophils were found in 29% of the positive cases, but in only one liver-negative case. Eosinophils also were numerous in 12% (five cases) of nonspecific infiltrates in otherwise positive cases, and so while often unhelpful, this feature was sometimes useful in separating the groups. Other histologic abnormalities were infrequent or did not differ significantly between the groups. Sarcoid-like noncaseating granulomas were only found in one positive case and in none of the negative cases.
Discussion
The diagnosis of hepatic involvement by Hodgkin’s disease is frequently made difficult by the uneven and patchy distribution of lesions, and by the nature of the lesions themselves. Hodgkh’s disease consists of a mixture of cell types, most of which are benign inflammatory and mesenchymal cells. Malignant cells, particularly those that are diagnostic of Hodgkin’s disease, are relatively few, and furthermore, malignant lesions may be outnumbered by associated benign inflammatory infiltrates. Because the presence of Hodgkin’s disease in the liver may change the clinical stage and alter therapy, it would be helpful to
know whether there are any morphologic clues that could increase the diagnostic yield or suggest the need for ad- ditional sections or repeat biopsy. The current study was undertaken to investigate that possibility.
Nonspecific benign hepatic inflammatory lesions have been well-documented in Hodgkin’s disease. Chronic portal inflammati~n,’-~ focal parenchymal n e c r ~ s i s , ~ ’ ~ sarcoid-like g ran~ lomas ,~ -~ and parenchymal lymphoid aggregates6 have all been described, and the need to rec- ognize these as nonneoplastic has become widely estab- lished. Patients with Hodgkin’s disease also can have other pathologic changes in the liver in the absence of neoplasm. Sinusoidal dilatation has been reported to be a frequent finding,* and severe intrahepatic cholestasis, although rare, is well-do~umented.~~’~
Surprisingly little has been written about hepatic changes associated with the presence of Hodgkin’s disease in the liver. Several authors have mentioned the propen- sity of Hodgkin’s disease to involve portal areas. 1-3,7,1 ’ Cavalli ef al.” pointed out that the tumor may involve small bile ducts, causing a destructive cholangitis and he- patic changes related to this. All have agreed that the di- agnosis of Hodgkin’s disease should not be made without RS cells or acceptable RS variants.
In the current study, we found that four histologic fea- tures can be helpful in predicting hepatic involvement in patients with Hodgkin’s disease. These are large infiltrates, acute cholangitis, portal edema, and infiltrates with a pre- dominance of atypical lymphocytes. Although we are not prepared to advocate that these features replace RS cells as diagnostic of Hodgkin’s disease, their presence, singly or in combination, does imply that diagnostic RS cells may be present nearby, and thus suggests the need for serial sectioning or repeat biopsy. In such cases, the biopsy specimen should not be regarded as negative or nonspe- cific, but merely as nondiagnostic. Also, we do not rec- ommend that the absence of these histologic features be used to exclude Hodgkin’s disease with confidence, but that the decision to pursue further diagnostic study be made on the basis of the total clinical situation.
In the differential diagnosis of hepatic Hodgkin’s dis- ease, nonneoplastic disorders cause more problems than other neoplasms. Acute cholangitis with portal edema may be caused by mechanical biliary obstruction of any cause.13 Its presence in cases of Hodgkin’s disease is prob- ably due to the propensity of the tumor to infiltrate the portal tracts, causing a localized obstruction. It is advis- able, therefore, to consider the possibility of obstruction when other clinical and histologic features do not support a diagnosis of hepatic Hodgkin’s disease. Similarly, a lymphoid infiltrate in the absence of the other features could be due to chronic active hepatitis rather than Hodg- kin’s disease.

2126 CANCER November 15 1989 Vol. 64
In summary, we have found that the presence of Hodg- kin’s disease in the liver frequently produces histologic changes that can be helpful in suggesting the diagnosis in the appropriate clinical setting. A careful search for these features may help in evaluating individual patients and in recommending further diagnostic studies.
REFERENCES
I . Bagley CM Jr, Roth JA, Thomas LB, DeVita VT. Liver biopsy in Hodgkin’s disease: Clinicopathologic correlations in 127 patients. Ann Intern Med 1972; 76219-225.
2. Abt AB, Kirschner RH, Belliveau RE et al. Hepatic pathology as- sociated with Hodgkin’s disease. Cancer 1974; 33: 1564-1 57 1.
3. Skovsgaard T, Brinkmeyer LM, Vesterager L, Thiede T, Nissen NI. The liver in Hodgkin’s disease: 11. Histopathologic findings. Eur .I Clin Oncol 1982; 18:429-435.
4. Kadin ME, Donaldson SS, Dorfman RF. Isolated granulomas in Hodgkin’s disease. N Engl JMed 1970; 283:859-861
5. Sacks EL, Donaldson SS, Gordon J, Dorfman RF. Epithelioid
granulomas associated with Hodgkin’s disease: Clinical correlations in 55 previously untreated patients. Cancer 1978; 41562-567.
6. Leslie KO, Colby TV. Hepatic parenchymal lymphoid aggregates in Hodgkin’s disease. Hum Path01 1984; 15308-809.
7. Lukes RJ. Criteria for involvement of lymph node, bone marrow, spleen, and liver in Hodgkin’s disease. Cancer Res 197 I ; 31:1755-1767.
8. Bruguera M, Caballero T, Cameras E, Aymerich M, Rodes J, Roz- man C. Hepatic sinusoidal dilatation in Hodgkin’s disease. Liver 1987; 7:76-80.
9. Piken EP, Abraham CE, Hepner GW. Investigation of a patient with Hodgkin’s disease and cholestasis. Gastroenterology 1979; 77: 145- 147.
10. Birrer MJ, Young RC. Differential diagnosis of jaundice in lym- phoma patients. Semin Liver Dis 1987; 1:269-277.
1 I . Jaffe ES. Malignant lymphomas: Pathology of hepatic involve- ment. Semin Liver Dis 1987; 7:257-268.
12. Cavalli G, Casali AM, Lambertini F, Busachi C. Changes in the small biliary passages in the hepatic localization of Hodgkin’s disease. Virchows Arch [A] 1979; 384:295-306.
13. MacSween RNM. Mechanical duct obstruction. In: Peters RL, Craig JR, eds. Liver Pathology. New York: Churchill Livingstone, 1986; 161-176.





























