Embed Size (px)
Citation preview

Hemorrhagic Ganglion of the TibialisAnterior Tendon: Report of an UnusualVariant
Nitza N. Rodriguez, DPM,1 and Neal M. Blitz, DPM, FACFAS2
While clinicians have encountered heme-laden ganglion cysts in the past, to our knowledge the conditionhas never been described in the literature as a distinct pathological entity, namely, the hemorrhagicganglion. Because hemorrhage may alter the appearance of an aspirate obtained from a ganglion cyst,and hemosiderin deposition within a ganglion cyst may alter the signal characteristics observed on amagnetic resonance image, such that both of these diagnostic methods may suggest the presence of asolid mass tumor rather than a ganglion cyst, it is important for clinicians and surgeons to be aware ofthe possibility of the presence of a hemorrhagic ganglion cyst. In this report, we present a case whereina hemorrhagic ganglion cyst of the tibialis anterior tendon was identified and excised. Level of ClinicalEvidence: 4 (The Journal of Foot & Ankle Surgery 47(6):571–575, 2008)
Key Words: aspirate, cyst, heme-laden, hemorrhagic ganglion, hemosiderin, magnetic resonance image,
tibialis anterior tendonGanglion cysts are gelatinous fluid filled, encapsulatedsoft tissue masses that typically occur adjacent to a joint ortendon (1). Their diagnosis is usually straightforward, andbased primarily on the history and clinical examination(2–4). The history often entails description of a lesion thatslowly evolved and enlarges with repetitive or strenuousmovement of the involved extremity, and palpation usuallydisplays a nodule that is deep to, and freely moveable under,the skin, and one that may be slowly fluctuant and rarelytender. Aspiration of the cyst characteristically reveals clearto straw-colored, viscous, gelatinous fluid, which is diag-nostic (5, 6). If the ganglion cyst is deep to the deep fascia,or if it has been present for a long period of time, it may bedifficult to determine the extent of the cyst, and its contentsmay be more firm and suggestive of a more ominous lesion.In such cases, aspiration may not yield enough fluid to be ofuse in making a clinical diagnosis, and magnetic resonanceimaging (MRI) may be indicated in such cases. The char-acteristic findings observed upon MRI of a ganglion cyst
Address correspondence to: Neal M. Blitz, DPM, FACFAS, Chief ofFoot Surgery, Department of Orthopaedic Surgery, Bronx-Lebanon Hos-pital Center, 1650 Selwyn Avenue 3H, Bronx, NY 10457. E-mail:[email protected].
1Podiatric Surgeon, Northern California Foot & Ankle Center, Califor-nia Pacific Medical Center, San Francisco, CA.
2Chief of Foot Surgery, Department of Orthopaedic Surgery, Bronx-Lebanon Hospital Center, Bronx, NY.
Financial Disclosure: None reported.Conflict of Interest: None reported.Copyright © 002 by the American College of Foot and Ankle Surgeons
1067-2516/08/4706-0014$34.00/0doi:10.1053/j.jfas.2008.08.012VOLUME 47
include a homogenous, bright signal on T2-weighted im-ages, indicative of the presence of a fluid-filled ganglioncyst (5). In the presence of substantial hemosiderin deposi-tion, however, the MRI characteristics will be altered suchthat the fluid will display low-to-intermediate intensity onT2-weighted images, a finding that could falsely suggest thepresence of a solid rather than fluid-filled mass. To the bestof our knowledge, this finding has not been described inrelation to a ganglion cyst, and for this reason we present thefollowing case in an effort to illustrate the diagnosis andmanagement of a hemorrhagic ganglion cyst associated withthe tendon of tibialis anterior in the foot.
Case Report
A 59-year-old female complained of an enlarging masslocalized to the dorsal and anterior aspect of her right footand ankle. She first identified the mass approximately 2months prior to her clinical visit, and related that althoughit was not directly painful, it had enlarged to such a degreethat it was interfering with her shoes. The patient’s onlymedical problem was osteoporosis, for which she was tak-ing alendronate sodium by mouth. Physical exam demon-strated a 3-cm nonmovable nodule deep to the tibialis an-terior tendon, just distal to ankle. The mass was firm with noassociated pain or paresthesia upon palpation, and there wasno associated erythema or local increase in the overlyingskin temperature. The overlying skin was mobile with fullankle range of motion, and clinically not adherent to thesubcutaneous nodule. She displayed well-perfused feet with
symmetrical, intact sensation. Standard radiographs re-, NUMBER 6, NOVEMBER/DECEMBER 2008 571
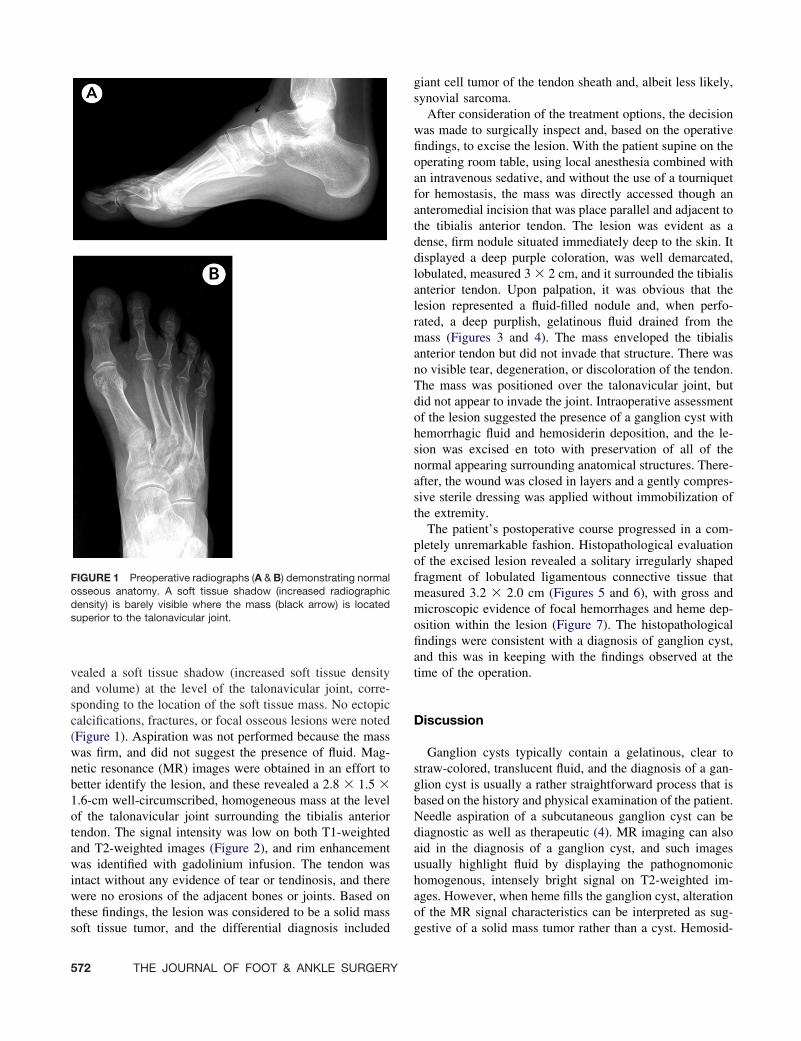
vealed a soft tissue shadow (increased soft tissue densityand volume) at the level of the talonavicular joint, corre-sponding to the location of the soft tissue mass. No ectopiccalcifications, fractures, or focal osseous lesions were noted(Figure 1). Aspiration was not performed because the masswas firm, and did not suggest the presence of fluid. Mag-netic resonance (MR) images were obtained in an effort tobetter identify the lesion, and these revealed a 2.8 � 1.5 �1.6-cm well-circumscribed, homogeneous mass at the levelof the talonavicular joint surrounding the tibialis anteriortendon. The signal intensity was low on both T1-weightedand T2-weighted images (Figure 2), and rim enhancementwas identified with gadolinium infusion. The tendon wasintact without any evidence of tear or tendinosis, and therewere no erosions of the adjacent bones or joints. Based onthese findings, the lesion was considered to be a solid mass
FIGURE 1 Preoperative radiographs (A & B) demonstrating normalosseous anatomy. A soft tissue shadow (increased radiographicdensity) is barely visible where the mass (black arrow) is locatedsuperior to the talonavicular joint.
soft tissue tumor, and the differential diagnosis included
572 THE JOURNAL OF FOOT & ANKLE SURGERY
giant cell tumor of the tendon sheath and, albeit less likely,synovial sarcoma.
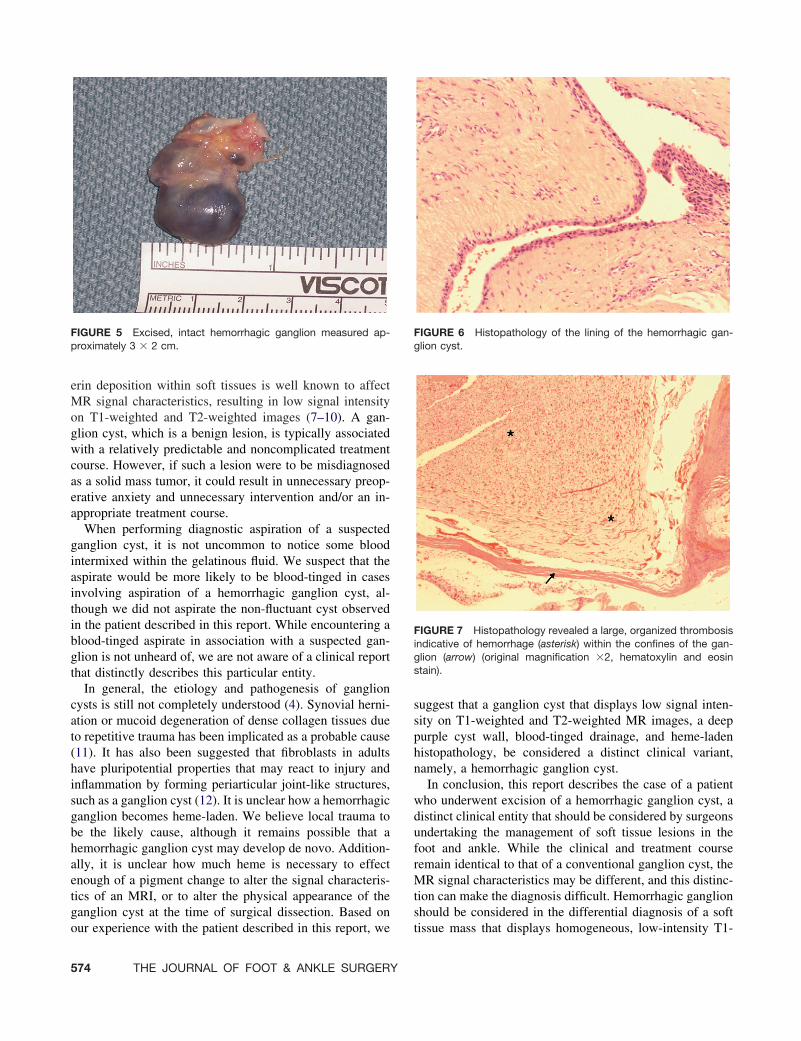
After consideration of the treatment options, the decisionwas made to surgically inspect and, based on the operativefindings, to excise the lesion. With the patient supine on theoperating room table, using local anesthesia combined withan intravenous sedative, and without the use of a tourniquetfor hemostasis, the mass was directly accessed though ananteromedial incision that was place parallel and adjacent tothe tibialis anterior tendon. The lesion was evident as adense, firm nodule situated immediately deep to the skin. Itdisplayed a deep purple coloration, was well demarcated,lobulated, measured 3 � 2 cm, and it surrounded the tibialisanterior tendon. Upon palpation, it was obvious that thelesion represented a fluid-filled nodule and, when perfo-rated, a deep purplish, gelatinous fluid drained from themass (Figures 3 and 4). The mass enveloped the tibialisanterior tendon but did not invade that structure. There wasno visible tear, degeneration, or discoloration of the tendon.The mass was positioned over the talonavicular joint, butdid not appear to invade the joint. Intraoperative assessmentof the lesion suggested the presence of a ganglion cyst withhemorrhagic fluid and hemosiderin deposition, and the le-sion was excised en toto with preservation of all of thenormal appearing surrounding anatomical structures. There-after, the wound was closed in layers and a gently compres-sive sterile dressing was applied without immobilization ofthe extremity.
The patient’s postoperative course progressed in a com-pletely unremarkable fashion. Histopathological evaluationof the excised lesion revealed a solitary irregularly shapedfragment of lobulated ligamentous connective tissue thatmeasured 3.2 � 2.0 cm (Figures 5 and 6), with gross andmicroscopic evidence of focal hemorrhages and heme dep-osition within the lesion (Figure 7). The histopathologicalfindings were consistent with a diagnosis of ganglion cyst,and this was in keeping with the findings observed at thetime of the operation.
Discussion
Ganglion cysts typically contain a gelatinous, clear tostraw-colored, translucent fluid, and the diagnosis of a gan-glion cyst is usually a rather straightforward process that isbased on the history and physical examination of the patient.Needle aspiration of a subcutaneous ganglion cyst can bediagnostic as well as therapeutic (4). MR imaging can alsoaid in the diagnosis of a ganglion cyst, and such imagesusually highlight fluid by displaying the pathognomonichomogenous, intensely bright signal on T2-weighted im-ages. However, when heme fills the ganglion cyst, alterationof the MR signal characteristics can be interpreted as sug-
gestive of a solid mass tumor rather than a cyst. Hemosid-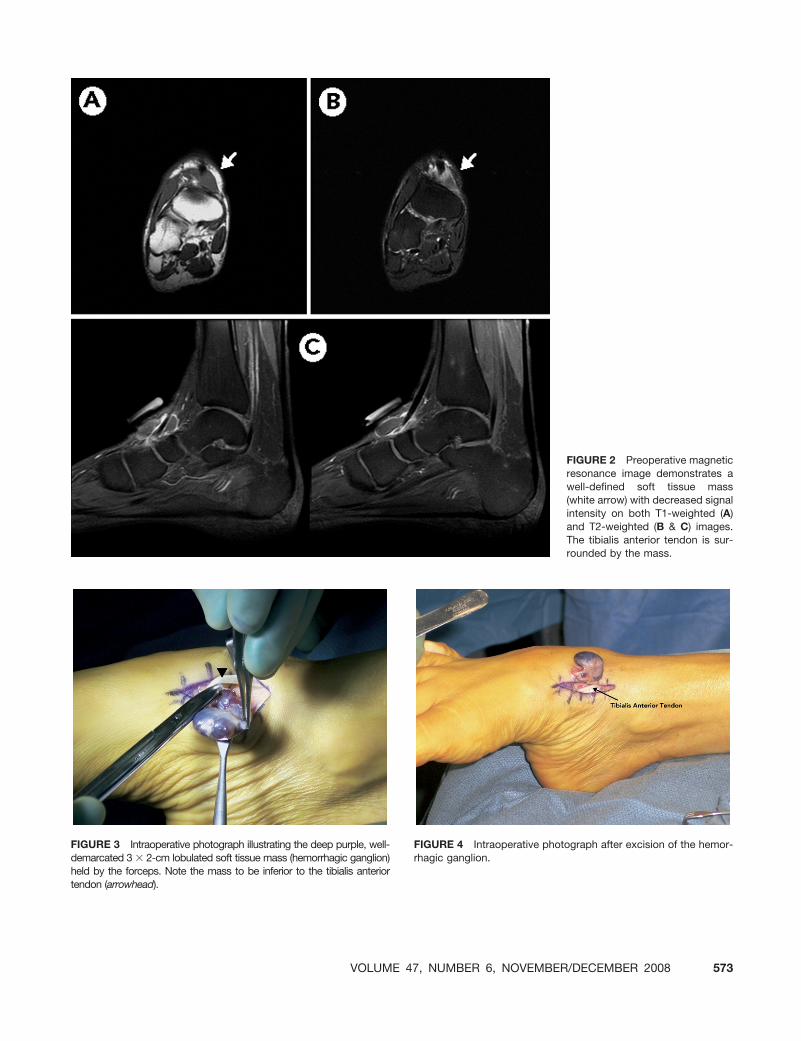
FIGURE 2 Preoperative magneticresonance image demonstrates awell-defined soft tissue mass(white arrow) with decreased signalintensity on both T1-weighted (A)and T2-weighted (B & C) images.The tibialis anterior tendon is sur-
rounded by the mass.rhagic ganglion.
FIGURE 3 Intraoperative photograph illustrating the deep purple, well-demarcated 3 � 2-cm lobulated soft tissue mass (hemorrhagic ganglion) held by the forceps. Note the mass to be inferior to the tibialis anteriortendon (arrowhead).VOLUME 47
FIGURE 4 Intraoperative photograph after excision of the hemor-
, NUMBER 6, NOVEMBER/DECEMBER 2008 573
erin deposition within soft tissues is well known to affectMR signal characteristics, resulting in low signal intensityon T1-weighted and T2-weighted images (7–10). A gan-glion cyst, which is a benign lesion, is typically associatedwith a relatively predictable and noncomplicated treatmentcourse. However, if such a lesion were to be misdiagnosedas a solid mass tumor, it could result in unnecessary preop-erative anxiety and unnecessary intervention and/or an in-appropriate treatment course.
When performing diagnostic aspiration of a suspectedganglion cyst, it is not uncommon to notice some bloodintermixed within the gelatinous fluid. We suspect that theaspirate would be more likely to be blood-tinged in casesinvolving aspiration of a hemorrhagic ganglion cyst, al-though we did not aspirate the non-fluctuant cyst observedin the patient described in this report. While encountering ablood-tinged aspirate in association with a suspected gan-glion is not unheard of, we are not aware of a clinical reportthat distinctly describes this particular entity.
In general, the etiology and pathogenesis of ganglioncysts is still not completely understood (4). Synovial herni-ation or mucoid degeneration of dense collagen tissues dueto repetitive trauma has been implicated as a probable cause(11). It has also been suggested that fibroblasts in adultshave pluripotential properties that may react to injury andinflammation by forming periarticular joint-like structures,such as a ganglion cyst (12). It is unclear how a hemorrhagicganglion becomes heme-laden. We believe local trauma tobe the likely cause, although it remains possible that ahemorrhagic ganglion cyst may develop de novo. Addition-ally, it is unclear how much heme is necessary to effectenough of a pigment change to alter the signal characteris-tics of an MRI, or to alter the physical appearance of theganglion cyst at the time of surgical dissection. Based on
FIGURE 5 Excised, intact hemorrhagic ganglion measured ap-proximately 3 � 2 cm.
our experience with the patient described in this report, we
574 THE JOURNAL OF FOOT & ANKLE SURGERY
suggest that a ganglion cyst that displays low signal inten-sity on T1-weighted and T2-weighted MR images, a deeppurple cyst wall, blood-tinged drainage, and heme-ladenhistopathology, be considered a distinct clinical variant,namely, a hemorrhagic ganglion cyst.
In conclusion, this report describes the case of a patientwho underwent excision of a hemorrhagic ganglion cyst, adistinct clinical entity that should be considered by surgeonsundertaking the management of soft tissue lesions in thefoot and ankle. While the clinical and treatment courseremain identical to that of a conventional ganglion cyst, theMR signal characteristics may be different, and this distinc-tion can make the diagnosis difficult. Hemorrhagic ganglionshould be considered in the differential diagnosis of a soft
FIGURE 6 Histopathology of the lining of the hemorrhagic gan-glion cyst.
FIGURE 7 Histopathology revealed a large, organized thrombosisindicative of hemorrhage (asterisk) within the confines of the gan-glion (arrow) (original magnification �2, hematoxylin and eosinstain).
tissue mass that displays homogeneous, low-intensity T1-

weighted and T2-weighted MR images, especially when theresults of a diagnostic aspiration of the lesion fail to yieldenough fluid for analysis, display hemorrhagic fluid, or if anaspiration has not been undertaken.
References
1. Inaparthy PK, Ravikumar KJ. Intratendinous ganglion of peroneustertius—A case report. Foot Ankle Surg 12:221–222, 2006.
2. Rozbruch SR, Chang V, Bohne WH, Deland JT. Ganglion cysts of thelower extremity an analysis of 54 cases and review of the literature.Orthopedics 21:141–148, 1998.
3. Pontius J, Good J, Maxian S. Ganglions of the foot and ankle. Aretrospective analysis of 63 procedures. J Am Podiatr Assoc 89:163–168, 1999.
4. Schram AJ, Kirschenbaum SE. Presentation of a unique ganglioniccyst. J Foot Surg 27:530–532, 1988.
5. Esteban JM, Oertel YC, Mendoza M, Knoll SM. Fine needle aspiration
in the treatment of ganglion cysts. South Med J 79:691–693, 1986.VOLUME 47
6. Nield DV, Evans DM. Aspiration of ganglia. J Hand Surg (Br) 11(2):264, 1986.
7. Mahallati H, Wallace CJ, Hunter KM, Bilbao JM, Clark AW. MRimaging of a hemorrhagic and granulomatous cyst of the ligamentumflavum with pathologic correlation. Am J Neuroradiol 20:1166–1168,1999.
8. Eustace S, Harrison M, Srinivasen U, Stack J. Magnetic resonanceimaging in pigmented villonodular synovitis. Can Assoc Radiol J45:283–286, 1994.
9. Cotten A, Flipo RM, Chastanet P, Desvigne-Noulet MC, Du-quesnoy B, Delcambre B. Pigmented villonodular synovitis of thehip: review of radiographic features in 58 patients. Skeletal Radiol24:1– 6, 1995.
10. Hughes TH, Sartoris DJ, Schweitzer ME, Resnick DL. Pigmentedvillonodular synovitis: MRI characteristics. Skeletal Radiol 24:7–12,1995.
11. Kannus P, Jozsa L. Histopathological changes preceding spontaneousrupture of a tendon. J Bone Joint Surg Am 73:1507–1525, 1991.
12. Adn M, Hamlat A, Morandi X, Guegan Y. Intraneural ganglion cyst of
the tibial nerve. Acta Neurochir (Wien) 148(8):885–889, 2006., NUMBER 6, NOVEMBER/DECEMBER 2008 575





























