Embed Size (px)
Citation preview
PORCINE VALVE FOLLOW-UP/Morris et al.
appeared to be related to the age of the donor. We believethat the methods of preparation, storage and insertion cangreatly influence the long term performance of the valves.
Aortic homografts continue to be our method of choicefor all patients undergoing aortic valve replacement. How-ever we feel that continued evaluation is required to definethe performance of these valves for longer periods of time.
References
1. Yacoub MH, Kittle F: Sterilization of valve homograft by antibiotic solu-tion. Circulation 41 (suppl Il): 11-29, 1970
2. Yacoub MH, Knight E, Towers MK: Aortic valve replacement using freshunstented homografts. Thoraxchirurgie 21: 451, 1973
3. Barratt-Boyes BG, Lowe JB, Cole DS, Kelly DT: Homograft replacementfor aortic valve disease. Thorax 20: 489, 1965
4. Ross DN, Yacoub MH: Homograft replacement of the aortic valve. Acritical review. Prog Cardiovasc Dis 40: 275, 1969
5. Gula G, Ahmed M, Thompson RH, Radley-Smith R, Yacoub MH: Com-bined homograft replacement of the aortic valve and aortic root withreimplantation of the coronary arteries. (abstr) Circulation 54 (suppi II):11-150, 1976
6. Berksen J, Cage RP: Calculation of survival rates for cancer. Proc StaffMeet Mayo Clin 25: 270, 1956
7. Anyanwu CH, Nassau E, Yacoub MH: Miliary tuberculosis followinghomograft valve replacement. Thorax 31: 101, 1976
8. Pacifico AD, Karp RB, Kirklin J: Homografts for the aortic valve. Cir-culation 45 (suppl II): 11-29, 1972
Hemodynamic Results of Aortic Valvular Replacementwith the Porcine Xenograft ValveDOUGLAS C. MORRIS, M.D., SPENCER B. KING, III, M.D.,
JOHN S. DOUGLAS, JR., M.D., CHARLES W. WICKLIFFE, M.D.,AND ELLIS L. JONES, M.D.
SUMMARY Twenty-three patients were evaluated by cardiaccatheterization two to 12 months following aortic valve replacementwith the porcine xenograft valve. These hemodynamic studies es-tablished a mean peak-to-peak systolic gradient across the prosthesisof 23 mm Hg with a range of 6-58 mm Hg. The mean effective orificearea was calculated to be 1.25 cm2. The effective orifice area in-
SINCE THE ERA of prosthetic cardiac valves was openedin 1952 with the implantation of the caged ball prosthesis inthe thoracic aorta by Hufnagel,' active investigation of newprosthetic models has continued because of dissatisfactionwith the hemodynamic characteristics, the durability, or thethrombogenicity of previously available prostheses. Amongthe prosthetic valves presently under clinical investigation isthe porcine xenograft aortic valve (fig. 1). This prosthesis isa composite tissue valve composed of porcine aortic leafletsmounted on a flexible stent and pretreated with a tanningagent (glutaraldehyde). The glutaraldehyde produces across-linkage between the collagen molecules and thus in-creases tissue strength. While the ease of implantation andthe very low thrombogenicity of this particular prosthesishave been substantiated by previous investigations,2 itslong-term durability remains unproven and its hemo-dynamic characteristics in the aortic position are untested.The present study defines the hemodynamic characteristicsof this prosthesis in the aortic position.
MethodsPatient Population
The study population consisted of 23 patients who hadaortic valve replacement with the porcine xenograft aortic
From the Cardiovascular Laboratory, Emory University Hospital andEmory University School of Medicine, Atlanta, Georgia.
Address for reprints: Douglas C. Morris, M.D., Crawford W. LongHospital of Emory University, 25 Prescott Street, Atlanta, Georgia 30308.
Received March 28, 1977; revision accepted June 21, 1977.
creased with increasing valve size from 0.99 cm2 for the 19 mmprosthesis to 1.44 cm2 for the 25 mm prosthesis. While in general thehemodynamics of the porcine xenograft valve are comparable to otheravailable prostheses, the exceedingly small orifice areas (0.99 cm2and 1.03 cm2) calculated for the 19 mm and 21 mm prostheses rendertheir use inadvisable.
valve at Emory University Hospital between July 1974 andJuly 1975. The patients were selected from the total group ofpatients receiving the porcine xenograft valve only on thebasis of their willingness to participate in this study.
In 14 of these 23 patients valve replacement was per-formed for amelioration of calcific aortic stenosis; threepatients had a mixed valve lesion with thickened, calcific, yetincompetent, leaflets; and only six patients had predominantaortic regurgitation. The valvular calcification extended intothe anulus in five of the patients. Two of these patients, inaddition, had a heavy bar of calcium extend from the anulusinto the anterior leaflet of the mitral valve. Debridement ofthe calcium was successful in every case and in no instancedid residual calcium hinder prosthesis implantation.
Nineteen patients were asymptomatic and in functionalclass I at the time of the postoperative hemodynamic evalua-tion. Three patients were in functional class II and one wasin functional class III. The average age of the patients withaortic stenosis was 58 years, while the patients with aorticregurgitation and mixed valve lesions averaged 38 years and42 years, respectively.
Hemodynamic Evaluation
These twenty-three patients were evaluated by left andright cardiac catheterization two to 12 months after valvereplacement in order to establish the effective orifice area ofthe prosthesis and to determine the degree of regurgitantflow across the prosthesis during diastole.
841
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from
VOL 56, No 5, NOVEMBER 1977
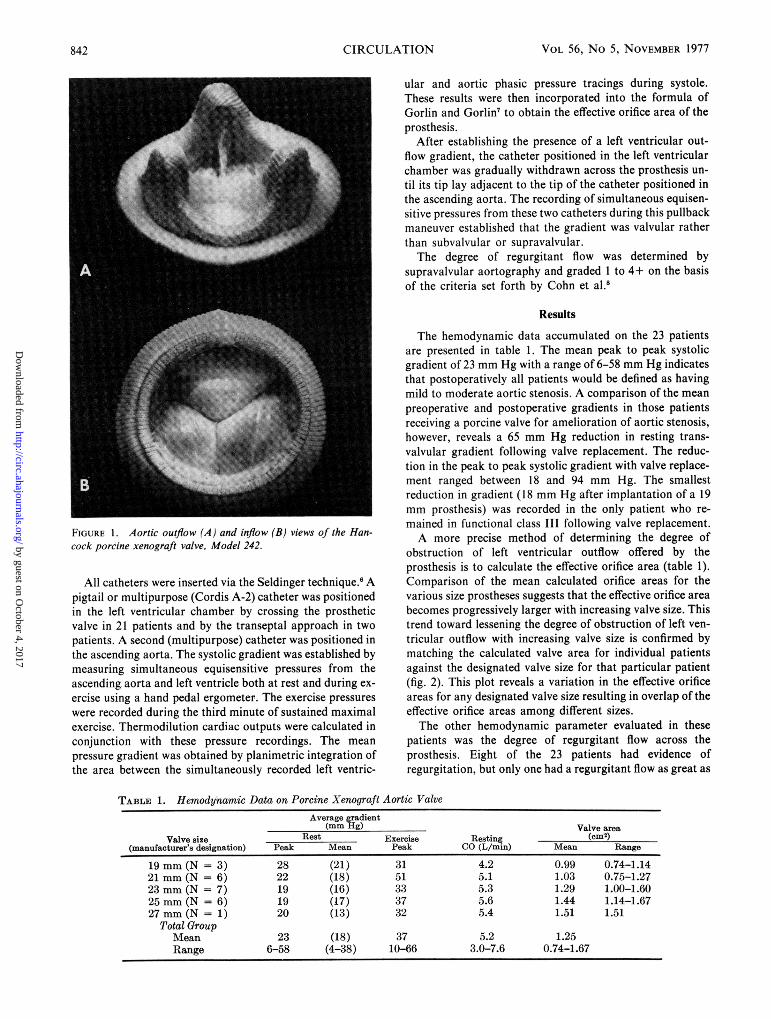
FIGURE Aortic outflow (A) and inflow (B) views of the Han-cock porcine xenograft valve, Model 242.
All catheters were inserted via the Seldinger technique.6 Apigtail or multipurpose (Cordis A-2) catheter was positionedin the left ventricular chamber by crossing the prostheticvalve in 21 patients and by the transeptal approach in twopatients. A second (multipurpose) catheter was positioned inthe ascending aorta. The systolic gradient was established bymeasuring simultaneous equisensitive pressures from theascending aorta and left ventricle both at rest and during ex-
ercise using a hand pedal ergometer. The exercise pressures
were recorded during the third minute of sustained maximalexercise. Thermodilution cardiac outputs were calculated inconjunction with these pressure recordings. The mean
pressure gradient was obtained by planimetric integration ofthe area between the simultaneously recorded left ventric-
ular and aortic phasic pressure tracings during systole.These results were then incorporated into the formula ofGorlin and Gorlin7 to obtain the effective orifice area of theprosthesis.
After establishing the presence of a left ventricular out-flow gradient, the catheter positioned in the left ventricularchamber was gradually withdrawn across the prosthesis un-
til its tip lay adjacent to the tip of the catheter positioned inthe ascending aorta. The recording of simultaneous equisen-sitive pressures from these two catheters during this pullbackmaneuver established that the gradient was valvular ratherthan subvalvular or supravalvular.The degree of regurgitant flow was determined by
supravalvular aortography and graded I to 4+ on the basisof the criteria set forth by Cohn et al.8
Results
The hemodynamic data accumulated on the 23 patientsare presented in table 1. The mean peak to peak systolicgradient of 23 mm Hg with a range of 6-58 mm Hg indicatesthat postoperatively all patients would be defined as havingmild to moderate aortic stenosis. A comparison of the meanpreoperative and postoperative gradients in those patientsreceiving a porcine valve for amelioration of aortic stenosis,however, reveals a 65 mm Hg reduction in resting trans-valvular gradient following valve replacement. The reduc-tion in the peak to peak systolic gradient with valve replace-
ment ranged between 18 and 94 mm Hg. The smallestreduction in gradient (18 mm Hg after implantation of a 19mm prosthesis) was recorded in the only patient who re-
mained in functional class III following valve replacement.A more precise method of determining the degree of
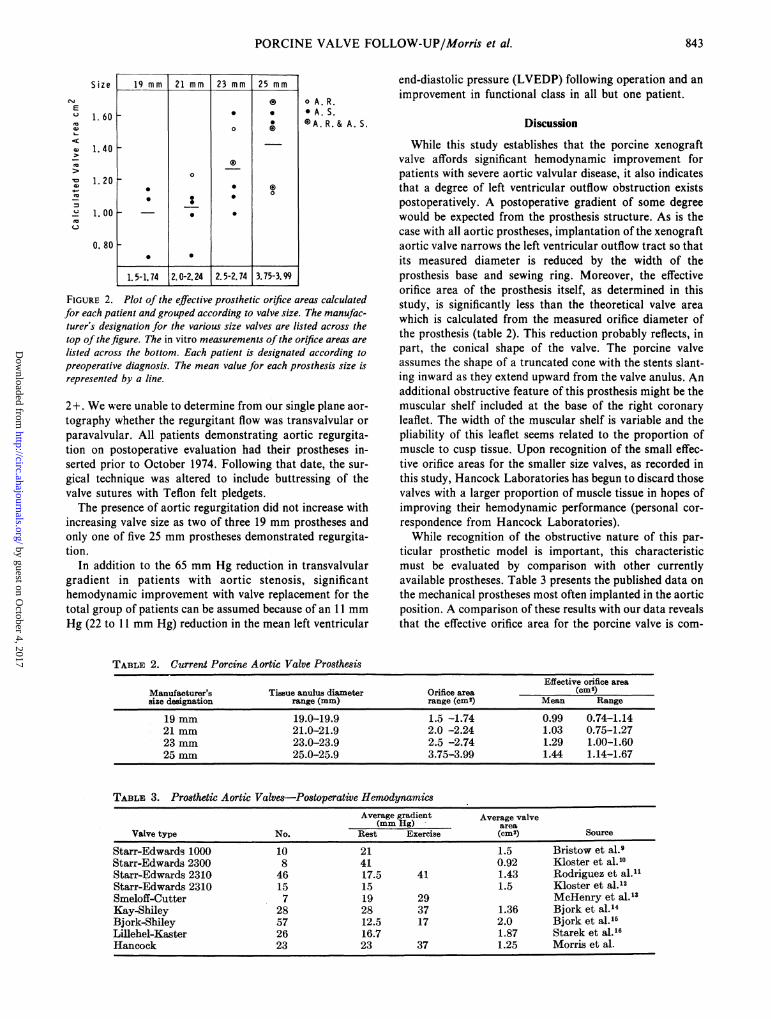
obstruction of left ventricular outflow offered by theprosthesis is to calculate the effective orifice area (table 1).Comparison of the mean calculated orifice areas for thevarious size prostheses suggests that the effective orifice area
becomes progressively larger with increasing valve size. Thistrend toward lessening the degree of obstruction of left ven-
tricular outflow with increasing valve size is confirmed bymatching the calculated valve area for individual patientsagainst the designated valve size for that particular patient(fig. 2). This plot reveals a variation in the effective orificeareas for any designated valve size resulting in overlap of theeffective orifice areas among different sizes.The other hemodynamic parameter evaluated in these
patients was the degree of regurgitant flow across theprosthesis. Eight of the 23 patients had evidence ofregurgitation, but only one had a regurgitant flow as great as
TABLE 1. Hemodynamic Data on Porcine Xenograft Aortic ValveAverage gradient
(mm Hg) Valve areaValve size Rest Exercise Resting (cm2)
(manufacturer's designation) Peak Mean Peak CO (L/min) Mean Range
19 mm (N = 3) 28 (21) 31 4.2 0.99 0.74-1.1421 mm (N = 6) 22 (18) 51 5.1 1.03 0.75-1.2723 mm (N = 7) 19 (16) 33 5.3 1.29 1.00-1.6025 mm (N = 6) 19 (17) 37 5.6 1.44 1.14-1.6727 mm (N - 1) 20 (13) 32 5.4 1.51 1.51
Total GroupMean 23 (18) 37 5.2 1.25Range 6-58 (4-38) 10-66 3.0-7.6 0.74-1.67
842 CIRCULATION
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from
PORCINE VALVE FOLLOW-UP/Morris et al.
E
.-
Size
1. 60
1.40
1. 20
1. 00
0. 80
19 mm 21 mm 23 mm 25 mm
0* 0
o 0
1517 2022 2527 37-.0
0
1. 5-1.74 2.0-2.24 2. 5-2.74 3.75-3.99
o A. R.* A. S.0A. R. & A. S.
FIGURE 2. Plot of the effective prosthetic orifice areas calculatedfor each patient and grouped according to valve size. The manufac-turer's designation for the various size valves are listed across thetop of thefigure. The in vitro measurements of the orifice areas are
listed across the bottom. Each patient is designated according topreoperative diagnosis. The mean value for each prosthesis size is
represented by a line.
2 +. We were unable to determine from our single plane aor-
tography whether the regurgitant flow was transvalvular or
paravalvular. All patients demonstrating aortic regurgita-tion on postoperative evaluation had their prostheses in-serted prior to October 1974. Following that date, the sur-
gical technique was altered to include buttressing of thevalve sutures with Teflon felt pledgets.The presence of aortic regurgitation did not increase with
increasing valve size as two of three 19 mm prostheses andonly one of five 25 mm prostheses demonstrated regurgita-tion.
In addition to the 65 mm Hg reduction in transvalvulargradient in patients with aortic stenosis, significanthemodynamic improvement with valve replacement for thetotal group of patients can be assumed because of an 11 mm
Hg (22 to 11 mm Hg) reduction in the mean left ventricular
end-diastolic pressure (LVEDP) following operation and an
improvement in functional class in all but one patient.
Discussion
While this study establishes that the porcine xenograftvalve affords significant hemodynamic improvement forpatients with severe aortic valvular disease, it also indicatesthat a degree of left ventricular outflow obstruction existspostoperatively. A postoperative gradient of some degreewould be expected from the prosthesis structure. As is thecase with all aortic prostheses, implantation of the xenograftaortic valve narrows the left ventricular outflow tract so thatits measured diameter is reduced by the width of theprosthesis base and sewing ring. Moreover, the effectiveorifice area of the prosthesis itself, as determined in thisstudy, is significantly less than the theoretical valve area
which is calculated from the measured orifice diameter ofthe prosthesis (table 2). This reduction probably reflects, inpart, the conical shape of the valve. The porcine valveassumes the shape of a truncated cone with the stents slant-ing inward as they extend upward from the valve anulus. Anadditional obstructive feature of this prosthesis might be themuscular shelf included at the base of the right coronary
leaflet. The width of the muscular shelf is variable and thepliability of this leaflet seems related to the proportion ofmuscle to cusp tissue. Upon recognition of the small effec-tive orifice areas for the smaller size valves, as recorded inthis study, Hancock Laboratories has begun to discard thosevalves with a larger proportion of muscle tissue in hopes ofimproving their hemodynamic performance (personal cor-
respondence from Hancock Laboratories).While recognition of the obstructive nature of this par-
ticular prosthetic model is important, this characteristicmust be evaluated by comparison with other currentlyavailable prostheses. Table 3 presents the published data on
the mechanical prostheses most often implanted in the aorticposition. A comparison of these results with our data revealsthat the effective orifice area for the porcine valve is com-
TABLE 2. Current Porcine Aortic Valve ProsthesisEffective orifice area
Manufacturer's Tissue anulus diameter Orifice area (cm2)size designation range (mm) range (cm2) Mean Range
19 mm 19.0-19.9 1.5 -1.74 0.99 0.74-1.1421 mm 21.0-21.9 2.0 -2.24 1.03 0.75-1.2723 mm 23.0-23.9 2.5 -2.74 1.29 1.00-1.6025 mm 25.0-25.9 3.75-3.99 1.44 1.14-1.67
TABLE 3. Prosthetic Aortic Valves-Postoperative HemodynamicsAverage gradient Average valve
(mm Hg) areaValve type No. Rest Exercise (cm2) Source
Starr-Edwards 1000 10 21 1.5 Bristow et al.9Starr-Edwards 2300 8 41 0.92 Kloster et al.10Starr-Edwards 2310 46 17.5 41 1.43 Rodriguez et al.11Starr-Edwards 2310 15 15 1.5 Kloster et al.'2Smeloff-Cutter 7 19 29 McHenry et al.-3Kay-Shiley 28 28 37 1.36 Bjork et al.14Bjork-Shiley 57 12.5 17 2.0 Bjork et al.-1Lillehel-Kaster 26 16.7 1.87 Starek et al.16Hancock 23 23 37 1.25 Morris et al.
843
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from
CIRCULATION VOL 56, No 5, NOVEMBER 1977
TABLE 4. Effective Orifice Area
Anulus Effective orifice area (cm2)diameter Bjork'7 Lillehei'6
of prosthesis Shiley Kaster Hancock
21 mm 1.30 - .25 1.30 i .23 1.03 - .1923 mm 1.70 - .49 1.40 - .24 1.29 - .2625 mm 2.2 - .5 1.90 o .31 1.42 - .23
parable to these other prostheses with the possible exceptionof the tilting disc models. The discrepancy between the effec-tive orifice areas of the tilting disc models and the porcinevalve assumes the most clinical significance in the small sizeprostheses (table 4). The extremely small effective orificeareas calculated for the 19 mm and 21 mm Hancock valvescoupled with the significantly larger areas for similar sizeBjork valves influences us in favor of the latter prosthesiswhen smaller sizes are required. The progressive increase ineffective orifice area in relation to valve size is not predict-ably found in the central occluder valves.12
Another feature common to the ball valve prosthesis is a
mean systolic gradient greater than the peak systolicgradient. This unusual relationship reflects the fact that thepressure gradient is present primarily in early systolepresumably secondary to poppet inertia.'2 A similar pressure
relationship was noted in 6 of our 23 patients.These gradients across the Hancock porcine valve were
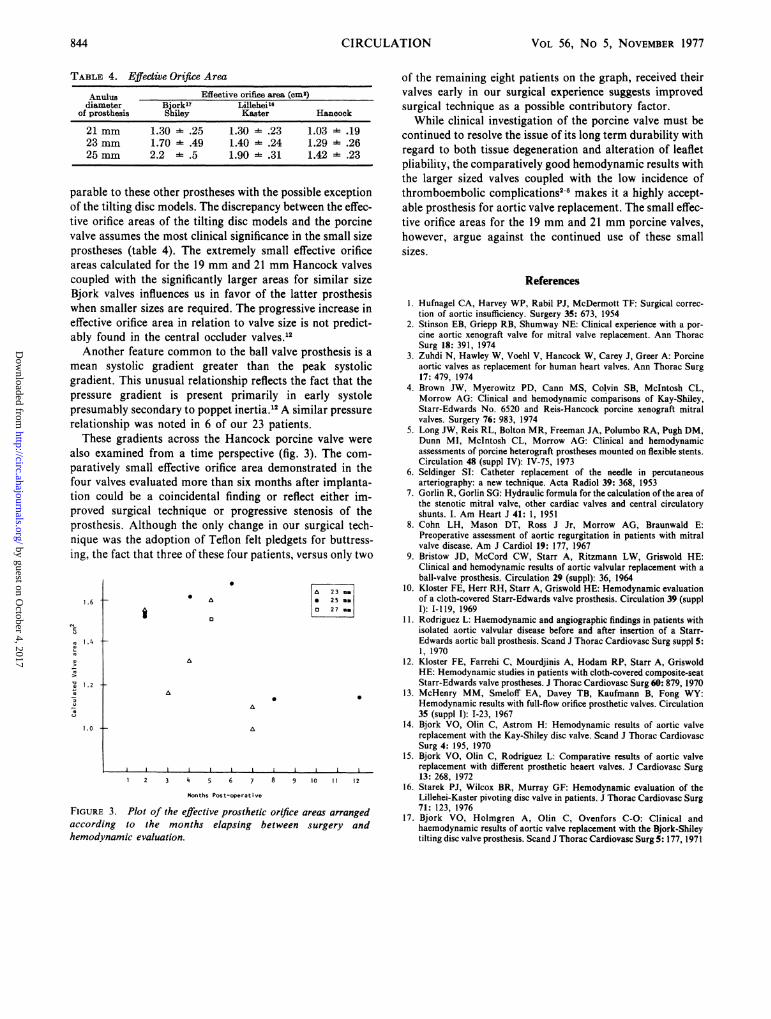
also examined from a time perspective (fig. 3). The com-
paratively small effective orifice area demonstrated in thefour valves evaluated more than six months after implanta-tion could be a coincidental finding or reflect either im-proved surgical technique or progressive stenosis of theprosthesis. Although the only change in our surgical tech-nique was the adoption of Teflon felt pledgets for buttress-ing, the fact that three of these four patients, versus only two
1.6 t * A
A an
an
mm
1.4 --
1.2
A
0
1.0 4-
J I L l l I
1 2 3 4 5 6 7 8 9 10 11 12
Months Post-operative
FIGURE 3. Plot of the effective prosthetic orifice areas arrangedaccording to the months elapsing between surgery and
hemodynamic evaluation.
of the remaining eight patients on the graph, received theirvalves early in our surgical experience suggests improvedsurgical technique as a possible contributory factor.
While clinical investigation of the porcine valve must becontinued to resolve the issue of its long term durability withregard to both tissue degeneration and alteration of leafletpliability, the comparatively good hemodynamic results withthe larger sized valves coupled with the low incidence ofthromboembolic complications2-5 makes it a highly accept-able prosthesis for aortic valve replacement. The small effec-tive orifice areas for the 19 mm and 21 mm porcine valves,however, argue against the continued use of these smallsizes.
References
1. Hufnagel CA, Harvey WP, Rabil PJ, McDermott TF: Surgical correc-tion of aortic insufficiency. Surgery 35: 673, 1954
2. Stinson EB, Griepp RB, Shumway NE: Clinical experience with a por-cine aortic xenograft valve for mitral valve replacement. Ann ThoracSurg 18: 391, 1974
3. Zuhdi N, Hawley W, Voehl V, Hancock W, Carey J, Greer A: Porcineaortic valves as replacement for human heart valves. Ann Thorac Surg17: 479, 1974
4. Brown JW, Myerowitz PD, Cann MS, Colvin SB, McIntosh CL,Morrow AG: Clinical and hemodynamic comparisons of Kay-Shiley,Starr-Edwards No. 6520 and Reis-Hancock porcine xenograft mitralvalves. Surgery 76: 983, 1974
5. Long JW, Reis RL, Bolton MR, Freeman JA, Polumbo RA, Pugh DM,Dunn MI, McIntosh CL, Morrow AG: Clinical and hemodynamicassessments of porcine heterograft prostheses mounted on flexible stents.Circulation 48 (suppl IV): IV-75, 1973
6. Seldinger SI: Catheter replacement of the needle in percutaneousarteriography: a new technique. Acta Radiol 39: 368, 1953
7. Gorlin R, Gorlin SG: Hydraulic formula for the calculation of the area ofthe stenotic mitral valve, other cardiac valves and central circulatoryshunts. I. Am Heart J 41: 1, 1951
8. Cohn LH, Mason DT, Ross J Jr, Morrow AG, Braunwald E:Preoperative assessment of aortic regurgitation in patients with mitralvalve disease. Am J Cardiol 19: 177, 1967
9. Bristow JD, McCord CW, Starr A, Ritzmann LW, Griswold HE:Clinical and hemodynamic results of aortic valvular replacement with aball-valve prosthesis. Circulation 29 (suppl): 36, 1964
10. Kloster FE, Herr RH, Starr A, Griswold HE: Hemodynamic evaluationof a cloth-covered Starr-Edwards valve prosthesis. Circulation 39 (supplI): I-119, 1969
11. Rodriguez L: Haemodynamic and angiographic findings in patients withisolated aortic valvular disease before and after insertion of a Starr-Edwards aortic ball prosthesis. Scand J Thorac Cardiovasc Surg suppl 5:1, 1970
12. Kloster FE, Farrehi C, Mourdjinis A, Hodam RP, Starr A, GriswoldHE: Hemodynamic studies in patients with cloth-covered composite-seatStarr-Edwards valve prostheses. J Thorac Cardiovasc Surg 60: 879, 1970
13. McHenry MM, Smeloff EA, Davey TB, Kaufmann B, Fong WY:Hemodynamic results with full-flow orifice prosthetic valves. Circulation35 (suppl I): 1-23, 1967
14. Bjork VO, Olin C, Astrom H: Hemodynamic results of aortic valvereplacement with the Kay-Shiley disc valve. Scand J Thorac CardiovascSurg 4: 195, 1970
15. Bjork VO, Olin C, Rodriguez L: Comparative results of aortic valvereplacement with different prosthetic heaert valves. J Cardiovasc Surg13: 268, 1972
16. Starek PJ, Wilcox BR, Murray GF: Hemodynamic evaluation of theLillehei-Kaster pivoting disc valve in patients. J Thorac Cardiovasc Surg71: 123, 1976
17. Bjork VO, Holmgren A, Olin C, Ovenfors C-O: Clinical andhaemodynamic results of aortic valve replacement with the Bjork-Shileytilting disc valve prosthesis. Scand J Thorac Cardiovasc Surg 5: 177, 1971
844
UE
m
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

D C Morris, S B King, J S Douglas, Jr, C W Wickliffe and E L JonesHemodynamic results of aortic valvular replacement with the porcine xenograft valve.
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1977 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.56.5.841
1977;56:841-844Circulation.
http://circ.ahajournals.org/content/56/5/841the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from





























