-
8/4/2019 Hematologic Studies
1/54
Hematologic Disorders
Jan Leynard Camposagrado, RN, USRN, MN
-
8/4/2019 Hematologic Studies
2/54
- Consist of blood, bone marrow and reticuloendothelial
system
- Blood is also considered an ORGAN
- Plasma is the fluid portion of theblood (55%)
Hematologic System
-
8/4/2019 Hematologic Studies
3/54
Blood
- Composed of: RBC, WBC and Platelets
- 45% of blood volume
- Carries oxygen, nutrients and wastes from system
- Also carries hormones and antibodies
-
8/4/2019 Hematologic Studies
4/54
Bone Marrow
- Site of hematopoiesis
- Marrow activity is limited topelvis, ribs, vertebrae and
sternumin adult
- Liver and spleen resume blood production in marrow
destruction
- Within the bone marrow are stem cells capable of
differentiation
myeloid lymphoid
-
8/4/2019 Hematologic Studies
5/54
Slide 002
-
8/4/2019 Hematologic Studies
6/54
-
8/4/2019 Hematologic Studies
7/54
Red Blood Cells
- Disk shape provides large surface for ABSORPTION andRELEASE of
oxygen molecules
- Primary function
- 120 days and removed by the reticuloendothelial cells
- Most of the iron is recycled to form new hemoglobin
- 5-day process of erythropoiesis
-
8/4/2019 Hematologic Studies
8/54
White Blood Cells
- Protect the body from invasion by bacteria and other foreign
entities
- Neutrophils arrive at the site within 1 hour of
inflammation
- Initiate phagocytosis but short-lived
- Monocytes follow and continue phagocytosis for longer
periods
- Macrophages are effective against fungi and viruses
-
8/4/2019 Hematologic Studies
9/54
Lymphocytes
- Releases lymphokines for enhanced phagocytic activity
T-Lymphocytes
- Responsible for delayed allergic reaction and foreign tissue
rejection
- Responsible for destruction of tumor cells
-
8/4/2019 Hematologic Studies
10/54
3 Main Groups of T-Lymphocytes
1. Killer T-cells- Sensitized and stimulated in the presence of
antigen- Destroy abnormal cells
2. Helper T-cells- Enhance activities of T-cells &
B-cells
- Reduced in patients with HIV
3. Suppressor T-cells- Have the effect of switching off the
immune system
- Controls too much T-cells
-
8/4/2019 Hematologic Studies
11/54
- Releases immunoglobulin or antibodies
B-Lymphocytes
- Function in hypersensitivity reactionEosinophils &
Basophils
- Eosinophils are impt in the phagocytosis of PARASITES
-
8/4/2019 Hematologic Studies
12/54
-
8/4/2019 Hematologic Studies
13/54
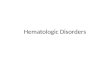
T cells on the right, platelet on the center and rbc at the
left
-
8/4/2019 Hematologic Studies
14/54
-
8/4/2019 Hematologic Studies
15/54
- For clotting mechanism- Circulate freely in an inactive state
in the endothelium- Normal life span of 7-10 days
Platelets
-
8/4/2019 Hematologic Studies
16/54
Test Normal Range Description
Red Blood Cells M: 4.7 6.1 x 106
F: 4.2 5.4 x 106
Hemoglobin M: 13.5 17.5 g/dL
F: 11.5 15.5 g/dL
Delivers oxygen through circulation to
body tissues and returns CO2 from
tissues to lungs
Hematocrit M: 40 52%
F: 36 48%
Indicates proportion of plasma and
RBCs
Platelets 150, 000 400, 000/mm3 20, 000/mm3 serious;
10, 000/mm3 life-threatening
Diagnostic Findings
-
8/4/2019 Hematologic Studies
17/54
Test Normal Range Description
White blood cells 5,000 10,000/mm3
Neutrophils 40 75% Indicates bacterial infection,
inflammation,
stress and steroids.
Lymphocytes 20 50% Increased after bacterial and viral
infection
Monocytes 1 10% Increased in acute and chronic infection,
and inflammation
Eosinophils 0
6% Increased in allergic states, parasites andmetastatic
tumors
Basophils 0 2% Increase is very rare
-
8/4/2019 Hematologic Studies
18/54
Anemia- Hemoglobin concentration is lower than normal
- Lower RBC than normallower amount of oxygen delivered
Three Broad Etiologic Categories:1. Loss of RBCdue to
bleeding
2. Decreased production of RBC
3. Increased destruction of RBC
- Deficiency in co-factors- Lack of erythropoietin
- Overactive RES
- Abnormal RBC
-
8/4/2019 Hematologic Studies
19/54
Classifications of Anemia
1. Hypoproliferative - marrow cannot produce adequately- due to
medications
- lack of co-factors
II. Hemolytic Anemia - premature destruction of RBC
-
8/4/2019 Hematologic Studies
20/54
Nursing Diagnosis
1. Activity Intolerance r/t weakness, fatigue & general
malaise
2. Imbalanced Nutrition, less than body requirement r/t
inadequate intake
of essential nutrients
3. Ineffective tissue perfusion r/t inadequate blood volume
-
8/4/2019 Hematologic Studies
21/54
Hypoproliferative Anemia
A. Iron Deficiency Anemia- Inadequate intake of Iron resulting
to low manufacture ofhgb
- Most common anemia
- Most common cause in male adult & post menopausal women is
bleeding
- Most common cause in pre-menopausal women is menstruation
- Alcoholism causes GIT blood loss
-
8/4/2019 Hematologic Studies
22/54
Assessment1. Pallor
2. Weakness and fatigue
3. Irritability
Diagnostic FindingBone Marrow Aspiration
- Most definitive
- Low ferritin level
- Seldom used
-
8/4/2019 Hematologic Studies
23/54
Medical Management
1. Iron Preparation
- Ferrous sulfate, Ferrous gluconate6 month therapy
2. Iron Dextran
- IM for poor iron absorption
- ANST before giving the full dose
-
8/4/2019 Hematologic Studies
24/54
Nursing Interventions
1. Give iron supplements between meals
2. Given with vit. C or multivitamins or fruit juice
3. Dont give iron with milk or antacid
4. Use a straw in liquid iron forms
5. Instruct pt. of S/E: constipation, black stool, foul
aftertaste
6. Instruct high iron foods: Liver, bread and cereals, dark
green leafy,meat, raisins, egg yolk, beans
-
8/4/2019 Hematologic Studies
25/54
B. Aplastic Anemia- Rare disease where there is decrease or
damage to marrow stem cellsFAT
- Significant neutropenia + thrombocytopenia are also seen
Causes:
1. Idiopathic2. Exposure to myelotoxic agents, autoimmune
disorder
- benzene, gold compounds,chloramphenicol, arsenic,
sulfonamides
-
8/4/2019 Hematologic Studies
26/54
Diagnostic FindingBone Marrow Aspiration- Most definitive
- Demonstrates conversion of red bone marrow to fatty red bone
marrow
Assessment1. Pancytopenia
2. Petechiae, purpura, bleeding, pallor, weakness, tachycardia,
fatigue
3. Infections are common
-
8/4/2019 Hematologic Studies
27/54
Medical Management1. Bone Marrow Transplantation
- Treatment of choice if a suitable donor exists
2. Immunosuppressive Therapy- Presumed that pts lymphocytes
destroy the stem cell
- Antithymocyte & cyclosporine
3. Supportive Therapy
- Transfusion of RBC and platelets
- Discontinue any offending agents
-
8/4/2019 Hematologic Studies
28/54
Nursing Interventions
1. Administer immunosuppressive medications
2. Administer blood transfusion as prescribed
3. Advise pt to obtain Medic-Alert bracelet
4. Assess carefully for signs of infection and bleeding
-
8/4/2019 Hematologic Studies
29/54
Hemolytic Anemia
A. Sickle Cell Anemia- RBCs have a shortened lifespan
- RBC = decreased available O2 hypoxia
- Hemoglobin (hemoglobin A) is partly or completely replaced by
an abnormalsickle hemoglobin (hemoglobin S)
- Happens when there is decreased O2 tension
-
8/4/2019 Hematologic Studies
30/54
-
8/4/2019 Hematologic Studies
31/54
Spleen Primary site of sickling infarctionand phagocytosis by
macrophage
infection
Lungs Infarctionpulmonary HPN Pulmonary infiltrate Chest pain,
dyspnea,
CNS Infarction CVA Weakness
Kidneys Sicklingdamage to renal medulla Hematuria,
renalfailure
Dehydration
Bone Increased erythroid production
(compensation)
Widening of medullary
spaces
Bone pain
Skin Infarction Skin ulcer Pain , decrease healing
Eye Infarction Scarring andhemorrhage
Decreased vision;blindness
Manifestations
-
8/4/2019 Hematologic Studies
32/54
Sickle Cell Crisis
1. Vasoocclusive Crisis- Most common
- Stasis of blood with clumping of the cells in the
microcirculation,ischemia and infarctionnecrosis
- s/sx: fever, pain and tissue engorgement
2. Splenic Sequestration
- Life threatening caused by pooling of blood in the spleen
(autosplenectomy)
- Liver and Lungs are involved in adults
- s/sx: profound anemia, hypovolemia and shock
-
8/4/2019 Hematologic Studies
33/54
3. Aplastic Crisis
- Causes production of RBC to shut down for about 10 days
andlevel falls rapidly & marrow cannot compensate
- Results from infection with the human parvovirus
- s/sx: anemia and pallor
-
8/4/2019 Hematologic Studies
34/54
Medical Management1. Hydroxyurea
- Chemotherapeutic agent used to decrease permanent formation of
sickle cells
- S/E: a. Chronic suppression of WBC b. Potential development of
malignancy
3. Transfusion Therapy
- Long term RBC transfusion- Risks include: a. Iron Overload
b. Infection and thrombosis from the sitec. Hepatitis and HIVd.
Significant financial cost
2. Arginine
- Enhances nitric oxidepotent vasodilator to decrease pulmonary
pressure
-
8/4/2019 Hematologic Studies
35/54
3. Supportive Therapy
PAINsignificant issue
a. Lasting hours to days
b. Adequate hydration is important
c. O2 may also be required
d. Pain medication may be given (aspirin, nsaids, morphine)
e. Physiotherapy can also be used (heat, massage)f. Cognitive
and behavioral intervention (distraction, relaxation)
-
8/4/2019 Hematologic Studies
36/54
Nursing Interventions
1. Managing pain
- Make use of pain scale
- Relaxation and breathing exercises
2. Preventing and Managing Infection
- Monitor s/sx of infection
3. Minimizing deficient knowledge
- inform: Keep warm
Maintain hydration
Avoid stressful events
-
8/4/2019 Hematologic Studies
37/54
B. G-6-PD- Glucose-6-Phospate Dehydrogenase Deficiency- G-6-PD
produces an enzyme w/in the erythrocyte for membrane stability-
Hemolysis only results when erythrocytes are stressed
- Commonly affected: African-American, Greek, Italian, Asian and
Jewish
- X-linked defects- Medications causing hemolysis:
1. Anti-malarial2. Bactrim/Septra3. Aspirin
5. HydroDIURIL6. OHA7. Chloramphenicol4. Vit. K
-
8/4/2019 Hematologic Studies
38/54
Assessment1. Asymptomatic most of the time2. Pallor, jaundice
and hemoglobinuria
3. Hemolysis is often mild and self limiting
Diagnostic Test1. Screening Test (NB Screening)
2. Quantitative Assay of G-6-PD
-
8/4/2019 Hematologic Studies
39/54
Medical Management1. Stop the offending medications
2. Transfusion if severe hemolysis occurs (Mediterranean
Type)
Nursing Management1. Pt is educated and given a list of
medications to avoid
2. Medic-Alert
-
8/4/2019 Hematologic Studies
40/54
Polycythemia Vera- Uncontrolled mechanisms of the myeloid stem
cellsresulting to hypercellular bone marrow activity.
- erythrocyte, leukocyte and platelet counts are elevated
Manifestations:
a. Increase blood volume - headache, dizziness, tinnitus,
fatigue, paresthesiaand blurred vision.
b. Increase blood viscosity - angina, claudication, dyspnea,
thrombophlebitis
c. Increase BP
d. Generalized pruritus
e. Splenomegaly
-
8/4/2019 Hematologic Studies
41/54
Diagnostic Test1. Elevated erythrocyte count
2. Increased leukocyte and platelet
3. Elevated hematocrit (60%)
Complications1. Thromboses
- MI- CVA
2. Bleeding - Very large platelets but dysfunctional
-
8/4/2019 Hematologic Studies
42/54
Medical Management1. Phlebotomy - to diminish blood
viscosity
2. Anagrelide (Agrylin)inhibits platelet aggregation
3. Interferon Alpha-2b (Intron-A)for pruritus- anti-histamines
are not effective
4. Chemotherapeutic Agents (Hydroxyurea)
- Suppress bone marrow but increases risk for leukemia
- Lowers incidence of thrombolytic complications than
phlebotomy
-
8/4/2019 Hematologic Studies
43/54
Nursing ManagementNurses role is primarily an EDUCATOR
1. Avoid smoking, obesity, poorly controlled hypertension
2. Avoid tight or restrictive clothing (stockings)3. Avoid
crossing legs
4. Avoid aspirin
5. Minimize alcohol intake (GI bleeding)
6. Avoid Iron Preparations
7. Bathe in tepid or cool water or sodium bicarbonate
-
8/4/2019 Hematologic Studies
44/54
Hemophilia
Hemophilia A
- Deficient or defective factor VIII
Hemophilia B- Deficient or defective factor IX
- Both hemophilias are inherited as X-linked traits
- Females are carriers and are asymptomatic
-
8/4/2019 Hematologic Studies
45/54
Manifestations
1. Joint bleeding (hemarthrosis)75% of all bleeding
- knees, elbows, ankles, hips, wrist and shoulders
- Recurrent joint hemorrhages can result to ankylosis
2. Hematoma can occur without known trauma in severe factor
deficiency
3. Damage sensation of the peripherals, weakness and atrophy
4. Spontaneous hematuria and GI bleeding
5. Most dangerous site of bleeding is the head
-
8/4/2019 Hematologic Studies
46/54
Medical Management1. Infusion of Factor VIII and IX
- Given during active bleeding or as preventive measure before
procedures
- Patient and family are instructed how to administer by IV at
home
- Patient sometimes develop antibodies to the concentrate- If
so, we give Recombinant Factor VIIa
2. Aminocaproic Acid (Amicar)
- Used to treat mucosal bleeding
3. Demopressin (DDAVP)
- Used for pt with mild forms of Hemophilia A
-
8/4/2019 Hematologic Studies
47/54
Nursing Management
A. Extensive teaching about activity restrictions and self care
measures
1. Avoid aspirin, NSAIDs, herbs and alcohol2. OTC cold remedies
are avoided
3. Dental hygiene to avoid dental extractions4. Nasal packing is
avoided5. Splint joints for signs of bleeding6. Avoid all
injections if possible
7. Invasive procedures should be minimized or performed
afteradministration of factor replacements
8. Frequently assess surgical sites post surgery
9. Wear Medic-Alert bracelet
10. Frequent v/s monitoring
-
8/4/2019 Hematologic Studies
48/54
B. Analgesicsfor pain associated with hematoma and hemorrhage to
joints
C. Warm bath promotes relaxation
bl d d bl d d
-
8/4/2019 Hematologic Studies
49/54
Procuring blood and blood productsDonors should be in good
health and without any of the ff:
1. History of viral hepatitis
2. History of blood transfusions
3. History of untreated syphilis or malaria
4. History of drug abuse of IV drug use5. Skin infections
6. Recent history of asthma, urticaria or allergy to
medications
7. Pregnant
8. History of untreated exposure to infectious diseases
9. Recent tattoo
10. Cancer
11. Aspirin usage within 48-72
-
8/4/2019 Hematologic Studies
50/54
All donors are expected to meet the ffminimal requirements:
1. Body weight should exceed 50 kg (110lbs) for 450 mL
donation
2. 17 y.o are disqualified
3. Oral temp should not exceed 37.5C
4. PR should be regular between 50-100 bpm
5. BP of 90/60180/100
6. Hgb should be at least: women - 12.5g/dL
men - 13.5g/dL
-
8/4/2019 Hematologic Studies
51/54
Complications of Blood Transfusion
A. Febrile Non-Hemolytic Reaction- Reaction of pts antibodies to
donor WBC
- s/sx: chills and fever
- Antipyretics for fever
B. Acute Hemolytic Reaction- Pt antibodies combine with donor
RBC and start hemolysis
- Incompatibility of blood (hemolysis)- Errors in blood
component labeling and patient identification- s/sx: fever, chills,
low-back pain
- n/v, chest tightness, dyspnea- hypotension, bronchospasm
- Most dangerous and life threatening
-
8/4/2019 Hematologic Studies
52/54
Management:
- Discontinue immediately- Meticulous attention to labels-
Accurate identification of recipient- Maintain blood volume
C. Allergic Reaction- Due to hypersensitivity to allergens found
in the transfused blood
- s/sx: urticaria, itching, flushing
Management:- anti-histamines for mild reactions
- Epinephrine and corticosteroid
-
8/4/2019 Hematologic Studies
53/54
D. Circulatory overload- Too much blood infused- s/sx: dyspnea,
orthopnea, tachycardia, sudden anxiety
- Jugular vein distention, increased BP- Crackles at the base of
the lungs
- if noted, transfusion is discontinued
- Notify physician
- KVO with NSS
-
8/4/2019 Hematologic Studies
54/54
E. Bacterial Contamination- Incidence is very low
- Usually due to organisms on the donors skin
- Most bacteria cannot survive in cold temperature used to
storeRBCplatelets are at greater risk
s/sx:
- Fever, chills & hypotension
- Transfusion is discontinued
- IV with NSS- Notify physician and blood bank is informed