Embed Size (px)
Citation preview

Health Workforce Trends, Challenges and Opportunities:
A Federal Perspective
47th Semi-Annual Substance Abuse Research Consortium Meeting September 11th, 2013
Edward Salsberg, MPADirector, National Center for Health Workforce
AnalysisDepartment of Health and Human Services
Health Resources and Services AdministrationBureau of Health Professions

2
Overview of Presentation
Workforce Challenges & Goals
National Center for Health Workforce
Analysis
Health Workforce Trends & Developments
Substance Abuse Workforce
Closing Comments

3
HRSA • HRSA provides national leadership, program
resources and services needed to improve access to culturally competent, quality health care
• Improving access to health care services for people who are uninsured, isolated or medically vulnerable
• Training health professions to improve the supply, capacity and distribution of the health workforce
• Funds over 80 grant programs; FY2013 budget: $11.7 billion

4
Workforce Challenges• Potential shortages; specific areas of concern:
• Primary Care, Chronic/Long Term Care, Behavioral Health, Oral health
• Mal-distribution of existing workforce• Increasing need for workforce diversity• Using health workers to the maximum of their
education and skills• Assessing the impact of a changing health care
system on the need for individual health occupations• Developing comprehensive data to inform health
workforce decisions

5
Goals for the Future Workforce
• High quality care at a reasonable cost• Assuring access to care• Increasing diversity to improve health equity• Making effective use of the workforce we have• Health workers practicing consistent with their
education, training and competencies

6
National Center for Health Workforce Analysis
• To support more informed public and private sector decision making related to the health workforce through expanded and improved health workforce data, projections and information.
• To promote the supply and distribution of well-prepared health workers to ensure access to high quality, efficient care for the nation.

7
NCHWA : Core Activities
1. Expanded and improved health workforce data collection and analysis
2. Improved projections of supply and demand/need
3. Dissemination of findings, data and information especially to key stakeholders
4. Collaboration with states on data collection and analysis and identifying needs

8
Data Collection and Analysis
• Build on existing sources of data including from federal agencies, states and professional associations• ACS, NAMCS, IPEDS, NPI, BLS, AMA-MF, NCCPA
• Develop and promote national minimum data sets
• National Sample Survey of NPs• Improved Primary Care Service Areas

9
Health Professions Minimum Data Set (MDS)
• Extensive data collected across the health workforce but comparisons across states and professions difficult or not possible due to variations in approach to data collection
• MDS seeks to develop comparable data across health professions, locations and time
• Building on existing efforts is the most cost-effective approach to collecting the needed data
• State licensure boards are usually in the best position to support this endeavor

10
Physicians
Nurses (including advanced practice)
Physician assistants
Pharmacists
Dentists
Dental hygienists
Physical therapists
Occupational therapists
Psychiatrists
Psychologists
Social workers
Licensed professional counselors
Substance abuse counselors
MDS Professions
Behavio
ral H
ealth
Occu
patio
ns

The Area Health Resources Files
• The Area Health Resources Files (AHRF) is a county-level health resource information database
• The AHRF system and database change in response to user needs
• AHRF products: downloadable files and web-based tools
• The AHRF compiles data from over 50 different sources
• AHRF has over 6,000 variables, including data for over 20 health professions
• Downloaded as compressed zipped files• Downloadable for free: ASCII and Access versions

Area Health Resources Files: 2013
• New 2013 release• Renamed the Area Health Resources Files
(AHRF). • New data: Several environmental indicators (air
quality, ozone, toxic waste sites), National Health Service Corps sites and providers.
• Improved Web-based Tools: Health Resources County Comparison Tool & Mapping Tool.
• State and national level data coming soon.
• http://arf.hrsa.gov/

Other Data from the NCHWA
Compendium of Federal Data Sources for Health Workforce Analysis http://bhpr.hrsa.gov/healthworkforce/compendiumfederaldatasources.pdf
The U.S. Nursing Workforce: Trends in Supply and Educationhttp://bhpr.hrsa.gov/healthworkforce

14
Strengthen the Capacity of States
• Collaboration with federally supported programs with states: PCOs, AHECs, SORH, LMIs, WIBs
• Support for minimum data sets through state licensure boards
• Development of state data under AHRF and comparison tools
• Health Workforce Research Center – State TA

Other NCHWA Work
• Cooperative agreement with the National Governor’s Association (NGA)
• Health Workforce Research Centers (forthcoming)
• Primary Care Service Area Improvements• HHS representative on the Standard
Occupational Classification (SOC) Policy Committee

Major Health Workforce Trends and Developments

17
0
1,000
2,000
3,000
4,000
1950 1960 1970 1980 1990 2000 2010
.
Managers
Technicians
Therapists
Aides
LPNs
RNs
Pharmacists
Dentists
NPCs
Physicians
Adapted from Kendix and Getzen and the Bureau of Labor Statistics by Richard Cooper
Health Employment per 100,0001950-2010
Year
Em
ploy
ees
per
100,
000
Pop
ulat
ion
National Health Care Labor Supply

18
Trends Impacting the Health Workforce
• Demand rising as the US population is growing and aging • Health care reform to add insurance coverage for millions
and improve coverage for millions more• Unsustainable cost increases• Concerns about potential health workforce shortages• Concern with inefficiencies and potential overuse• Increasing interest in identifying ways to improve
efficiency and health outcomes

19
Trends Impacting the Health Workforce cont
• Delivery system reforms and growing size of health care organizations
• Increasing use of inter-professional teams • Disruptive innovations (e.g. increased use of non-
physician clinicians; retail clinics)• Technology • Increased attention on outcomes and metrics• Patient/consumer empowerment • Globalization and global responsibility

20
• Center for Medicare & Medicaid Innovation (CMMI)• CMMI Challenge grants• State Innovation Models• Medical home initiatives• Accountable Care Organizations /Bundled payment• Medicare 10% PC payment bump through 2015• Medicaid PC increase to at least Medicare levels for
2013 and 2014• Workforce development: THCs, APRNs, NPs, Teams
Federal Activities to Support Systems Redesign

21
CMMI Health Care Innovation Awards
• Most approved projects include plans to use workers in new ways
• Care coordinators and better management of patients;• Use of:
o inter-professional teams;o patient navigators;o community health workers;o advanced aides, assistants;
• Improved care transitions and in-home services • Greater use of telemedicine and Health Information
Technology (HIT)• 16 of the 107 grantees in 2012 focued on behavioral health

22
Team for Comprehensive CarePhysicians
Nurse practitioners
Physician assistants
Psychologists
Optometrists
Registered Nurses
Pharmacists
Case Managers
Nutritionists/Dieticians
Physical Therapists
Community Health Workers
Substance Abuse Disorder Providers
…And more
23
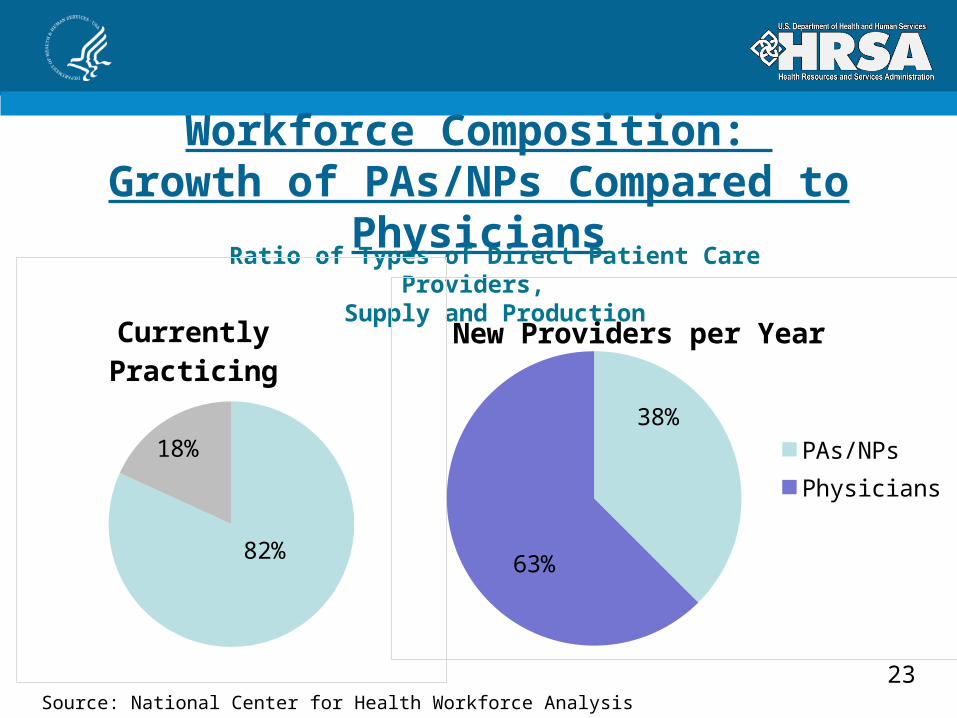
Workforce Composition: Growth of PAs/NPs Compared to Physicians
Source: National Center for Health Workforce Analysis
Ratio of Types of Direct Patient Care Providers,
Supply and Production
82%
18%
Currently Practicing
38%
63%
New Providers per Year
PAs/NPsPhysicians

24
Overview: • Five-year cooperative agreement• Main site: University of Minnesota
Aims:• Provide unbiased, expert guidance• Enhance the coordination and capacity building of IPECP among
health professions and particularly medically underserved areas• Raise the visibility of high quality, coordinated, team-based care
that is well-informed by interprofessional education and best practice models
National Center for Inter-professional Practice and Education

25
The Substance Abuse Workforce
• Integrated care is the future; Flexible use of workers will be key. This includes integration of behavioral health and primary health providers.
• Primary care settings have become the gateway to the behavioral health system, and primary care providers need support and resources to screen and treat individuals with behavioral and general healthcare needs.
• Delivering mental health and addiction services in collaborative primary care settings supports a “no wrong door” approach to care.

26
SAMHSA-HRSA Center for Integrated Health Solutions (CIHS)• Promotes the development of integrated primary and behavioral
health services to better address the needs of individuals with mental health and substance use conditions, whether seen in specialty behavioral health or primary care provider settings.
• Funded jointly by the Substance Abuse and Mental Health Services Administration (SAMHSA) and the Health Resources and Services Administration (HRSA), and run by the National Council for Behavioral Health.
• The Center provides training and technical assistance to 93 community behavioral health organizations as well as to community health centers and other primary care and behavioral health organizations.

27
Trends Impacting the Behavioral Health Workforce
• The Affordable Care Act will provide one of the largest expansions of mental health and substance use disorder coverage in a generation, through its insurance expansion provisions.
• 47.5 million Americans lack health insurance coverage, and 25% of uninsured adults have a mental health condition or substance abuse disorder or both.

28
Trends Impacting the Behavioral Health Workforce, cont
• The Affordable Care Act builds on the Mental Health Parity and Addiction Equity Act of 2008, which requires group health plans and insurers that offer mental health & substance use disorder benefits to provide coverage that is comparable to coverage for general medicine and surgical care.
• Implementation of the Affordable Care Act will require an expanded and appropriately trained workforce.

29
Workforce Implications of Health Systems Change
• Encourage strategies to make better use of existing workers • Teams and collaborative practice and education• New categories/variations on support/assistive personnel• Reassess scope of practice and scope of work• Increased use of technology including HIT
• Require flexibility to define and redefine roles and responsibilities to promote quality and efficiency
• Need for better data to guide decision making
30
Contact Information
Edward Salsberg, MPADirector, National Center for
Health Workforce Analysis301-443-9355


























![[47th KUG PP] Visual Presentation](https://img.dokumen.tips/doc/110x75/55568e37d8b42a182f8b4da0/47th-kug-pp-visual-presentation.jpg)


