Embed Size (px)
Citation preview

at SciVerse ScienceDirect
The Breast 21 (2012) 746e750
Contents lists available
The Breast
journal homepage: www.elsevier .com/brst
Original article
Health care utilization one year following the diagnosis benign breast diseaseor breast cancer
Claudia M.G. Keyzer-Dekker a,b, Lotje Van Esch c, Wilhelmina H. Schreurs d, Charles L.H. van Berlo e,Jan A. Roukema c,f, Jolanda De Vries c,g, Alida F.W. van der Steeg a,c, f,*
a Pediatric Surgical Center of Amsterdam, Emma Children’s Hospital AMC and VU University Medical Center, Meibergdreef 9, 1105 AZ, Amsterdam, The NetherlandsbDepartment of Pediatric Surgery, Beatrix Children’s Hospital, University Medical Center Groningen, Hanzeplein 1, 9700 RB, Groningen, The NetherlandscCoRPS - Center of Research on Psychology in Somatic Diseases, Tilburg University, Warandelaan 2, 5037 AB, Tilburg, The NetherlandsdDepartment of Surgery, Medical Centre Alkmaar, Wilhelminalaan 12, 1815 JD, Alkmaar, The NetherlandseDepartment of Surgery, VieCuri Medical Centre, Tegelseweg 210, 5912 BL, Venlo, The NetherlandsfDepartment of Surgery, St. Elisabeth Hospital, Hilvarenbeekseweg 60, 5022 GC, Tilburg, The NetherlandsgDepartment of Medical Psychology, St. Elisabeth Hospital, Hilvarenbeekseweg 60, 5022 GC, Tilburg, The Netherlands
a r t i c l e i n f o
Article history:Received 20 July 2011Received in revised form25 January 2012Accepted 29 January 2012
Keywords:Breast cancerBenign breast diseaseHealth care utilizationPersonalityHigh trait anxietyQuality of life
* Corresponding author. Department of pediatricHospital AMC, PO Box 22660, 1100 DD Amsterdam, T566 56 93; fax: þ31 20 566 92 87.
E-mail address: [email protected] (A.F.W
0960-9776/$ e see front matter � 2012 Elsevier Ltd.doi:10.1016/j.breast.2012.01.018
a b s t r a c t
Purpose: We analyzed health care utilization (HCU) and its predictors in the first year after the diagnosticprocess for breast cancer (BC) or benign breast disease (BBD) using questionnaires. The impact of traitanxiety on HCU was examined.Results: In total 591 women were analyzed, 440 with BBD and 151 with BC. In women with BBD and hightrait anxiety (HTA) increased HCU was found. In women with BC and HTA only more use of psychosocialcare (PS) was found. HCU in BBD was predicted by lower Quality of Life (QoL) and (adjuvant) treatmentpredicted HCU in BC.Conclusions: The most important factors for higher HCU were HTA and lower QoL, especially in BBD. Inwomen with BC increased PS use was seen in chronically anxious women. Therefore, it is important toidentify these women using a psychometric test and to anticipate to their specific (mental) health careneeds.
� 2012 Elsevier Ltd. All rights reserved.
Introduction
Nowadays, one in eight women in the western world will ulti-mately be diagnosed with breast cancer (BC).1e3 However, in ourexperience, the majority of women presenting at the surgicaloutpatient clinic with breast symptoms or referred after anabnormal screening mammogram, are diagnosed with benignbreast disease (BBD).4 This large group of women is important toconsider, because these women report increased levels of anxietybefore and during the diagnostic process comparable with womenwith BC.5e7 These levels of anxiety diminish after the diagnosticprocess is completed, but a significant amount of women with thediagnosis BBD are not completely reassured.7,8
A recent review revealed that trait anxiety was predictive forexperienced levels of anxiety during the diagnostic process for
surgery, Emma Children’she Netherlands. Tel.: þ31 20
. van der Steeg).
All rights reserved.
suspected BC.9 In addition, previous studies have shown that traitanxiety is not only an important predictor for anxiety, but also forquality of life (QoL) in women with BBD or BC.4,7,10
Trait anxiety refers to the tendency to respond to situationsperceived as threatening with a rise in anxiety intensity.11 Womenwho are chronically anxious tend to perceive new situations, forexample a possible diagnosis BC, as threatening and thereforeexperience higher levels of anxiety. These higher levels of anxietyand lowered QoL could be reason for an increase in health careutilization (HCU) inwomenwith BBD or BC, especially in those whoscore high on trait anxiety (HTA). However, limited research con-cerning HCU in women with BBD or BC is performed. A few studiesexamined which factors may contribute to increased HCU for BCpatients only, resulting in the following predictors: younger age,breast amputation, co-morbidity, older age, not having a partner,radiotherapy, cancer-related health problems, depression, andbreast reconstruction.12e15
We believe it is important to determine the patterns and thepredictors of HCU in women with BBD or BD. With this knowledgeabout themedical and psychosocial needs of thesewomen it will be

C.M.G. Keyzer-Dekker et al. / The Breast 21 (2012) 746e750 747
possible to anticipate to those needs and eventually adjust thecurrent follow up protocol guidelines.
We evaluated the HCU and the predictors for HCU in womenwith BBD or BC during the first year following the diagnosis. Acomparison in HCU was done between women with BBD or BC.Contrary to most studies concerning personality and QoL, in thisprospective, longitudinal study women completed the first set ofquestionnaires before any diagnostic procedures were carried outand thus before diagnosis was known.
First, we hypothesized that women with HTA would haveincreased HCU in the first year after diagnosis, in both the BBD andthe BC group. Secondly, based on previous research and experiencewe expected that HCUwas predicted by QoL, fatigue and depressivesymptoms.
Methods
Participants
The present study was performed in five teaching hospitals inthe Netherlands. From June 2007 until October 2009 womenreferred with a palpable lump in the breast or an abnormality ona screening mammogram, were asked to participate in this study.The present study is part of a larger prospective, longitudinal studyfocusing on the impact of personality and QoL on morbidity,mortality and health care utilization in women with benign ormalignant breast disease. At the time women gave writteninformed consent and completed the first set of questionnaires, thediagnosis was not yet known. If women were not able to completeDutch questionnaires for linguistic or cognitive reasons, or if theyhad a medical history with breast cancer or a psychiatric disease,they were excluded from the study. Women with advanced BCdisease were excluded. The protocol of the study was approved bythe local Medical Ethical Committee.
Health care utilization
HCU was divided in three major categories: visits to the medicalspecialist (MD), visits to the general practitioner (GP), and the useof psychosocial health care (PS), i.e. psychologist, welfare worker,self-help groups. After twelve months HCU was measured by self-report questions concerning visits and contacts with the GP, MD,and PS during the first year after diagnosis.
Questionnaires
Questionnaires were completed before any diagnostic proce-dures were carried out and thus before diagnosis was known. Thequestionnaires used assessed personality (STAI-Trait, NEO-FFI),depressive symptoms (CES-D), fatigue (FAS), and Quality of Life(WHOQOL-BREF).
Trait and state anxiety were measured with the State-TraitAnxiety Inventory (STAI).11,16 Trait anxiety concerns differences inindividuals in the disposition to respond to stressful situations withvarying amounts of stress. State anxiety is a momentary emotionalcondition characterized by subjective feeling of apprehension andtension.11,16 The trait anxiety scores were dichotomized in high ornot high. In this study the short forms of both the STAI Trait and theSTAI State were completed. These short versions of the STAI State(6-items) and Trait (10-items) have good reliability and validity.17
The personality trait neuroticism was measured by the neurot-icism part (12-items) of the Neuroticism-Extraversion-Openness-Five Factor Inventory (NEO-FFI).18,19 Neuroticism describes thepredisposition to emotional instability, i.e. the tendency to
experience no distressing emotions such as fear, guilt and frustra-tion. The reliability and validity of this questionnaire are good.18
The Center for Epidemiological Studies-Depression Scale (CES-D) measures the presence and degree of depressive symptoms. Theshort version with 16-items was used, which was found to bea valid assessment of depressive symptoms in cancer patients.20,21
Fatigue was measured by the 10-items Fatigue Assessment Scale(FAS).22 The reliability and validity of the FAS appears to be good inwomen with breast problems.23
The World Health Organization Quality of Life instrument, shortform (WHOQOL-BREF) was used to assess QoL.24 This questionnaireconsists of four domains (Physical health, Psychological health,Social relationships, and Environment) and two items concerningOverall QoL and General health. Higher scores indicate a bettersubjective QoL. Reliability and validity are reported to be good inwomen with breast problems.25
Demographical and medical information
Demographic data were obtained at baseline concerning age,marital status, having children, education level, and work status.Information on disease stage at diagnosis,26 type of operation, andadjuvant therapy (chemotherapy, radiotherapy, hormone therapy)was retrieved from patients’ medical records.
Statistical procedure
For baseline measures, Chi-square (discrete variables) andindependent samples T-tests (continuous variables) were used tocompare drop-outs and non-drop-outs.
To examine differences in visits to the MD, GP and PS (i) in thegroups BBD and BC, and (ii) in patients with HTA or not high scoreon trait anxiety (NHTA) in the BBD and BC group, chi-square tests(discrete variables) and independent samples T-tests (continuousvariables) were used.
Multivariate regression analyses were used to assess whichfactors were significant predictors of the number of contacts withthe GP or MD and whether a patient used psychological health carein the first year following diagnosis. The independent variablesincluded in the analyses were the following: demographics, diseasestage, (adjuvant) therapy, personality, and baseline scores for stateanxiety, depression, fatigue, and QoL domains.
All analyses were performed with the Statistical Package forSocial Sciences (SPSS) version 18.0 (SPSS, Chicago, Illinois, USA).
Results
During the study period 754 women were included, of whom163 women did not complete all questionnaires after 12 monthsfollow up. Baseline demographics and personality were comparedbetween drop-outs (N ¼ 163) and non-drop-outs (N ¼ 591): in thedrop-out group more women were diagnosed with BBD, scoredhigh on trait anxiety, and were less often referred by the nationalscreening program.
In total 591 women were analyzed, of whom 440 were diag-nosed with BBD and 151 with BC. Women with BBD and BC werecompared concerning demographic variables, personality at base-line and HCU (Table 1). In the BBD group the HCU for the GP, MD,and PS was significantly lower in the first year after diagnosiscompared with the BC group (Table 2).
Subsequently, women were divided in four groups basedon diagnosis (BBD or BC) and score on trait anxiety at baseline (HTAor NHTA). Women with BBD and HTA visited the GP more oftenthan women with BBD and NHTA (p ¼ 0.003). The percentage ofwomen with BBD visiting the MD was higher in women with HTA
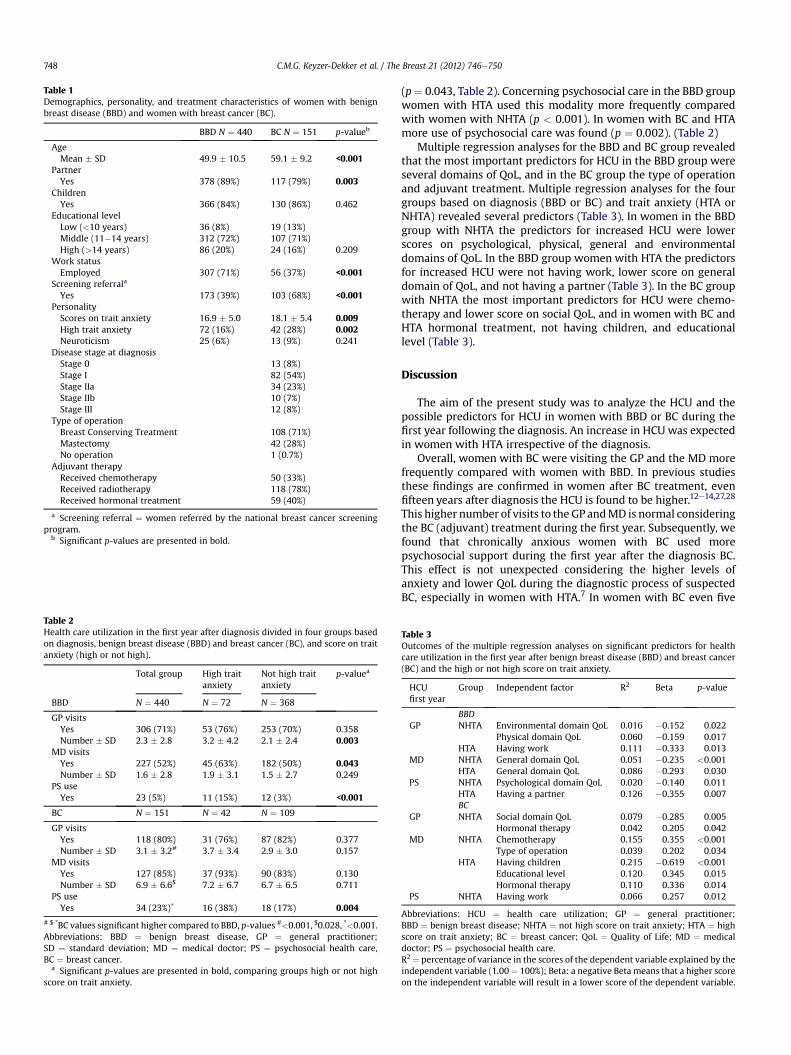
Table 2Health care utilization in the first year after diagnosis divided in four groups basedon diagnosis, benign breast disease (BBD) and breast cancer (BC), and score on traitanxiety (high or not high).
Total group High traitanxiety
Not high traitanxiety
p-valuea
BBD N ¼ 440 N ¼ 72 N ¼ 368
GP visitsYes 306 (71%) 53 (76%) 253 (70%) 0.358Number � SD 2.3 � 2.8 3.2 � 4.2 2.1 � 2.4 0.003
MD visitsYes 227 (52%) 45 (63%) 182 (50%) 0.043Number � SD 1.6 � 2.8 1.9 � 3.1 1.5 � 2.7 0.249
PS useYes 23 (5%) 11 (15%) 12 (3%) <0.001
BC N ¼ 151 N ¼ 42 N ¼ 109
GP visitsYes 118 (80%) 31 (76%) 87 (82%) 0.377Number � SD 3.1 � 3.2# 3.7 � 3.4 2.9 � 3.0 0.157
MD visitsYes 127 (85%) 37 (93%) 90 (83%) 0.130Number � SD 6.9 � 6.6$ 7.2 � 6.7 6.7 � 6.5 0.711
PS useYes 34 (23%)* 16 (38%) 18 (17%) 0.004
# $ *BC values significant higher compared to BBD, p-values #<0.001, $0.028, *<0.001.Abbreviations: BBD ¼ benign breast disease, GP ¼ general practitioner;SD ¼ standard deviation; MD ¼ medical doctor; PS ¼ psychosocial health care,BC ¼ breast cancer.
a Significant p-values are presented in bold, comparing groups high or not highscore on trait anxiety.
Table 1Demographics, personality, and treatment characteristics of women with benignbreast disease (BBD) and women with breast cancer (BC).
BBD N ¼ 440 BC N ¼ 151 p-valueb
AgeMean � SD 49.9 � 10.5 59.1 � 9.2 <0.001
PartnerYes 378 (89%) 117 (79%) 0.003
ChildrenYes 366 (84%) 130 (86%) 0.462
Educational levelLow (<10 years) 36 (8%) 19 (13%)Middle (11�14 years) 312 (72%) 107 (71%)High (>14 years) 86 (20%) 24 (16%) 0.209
Work statusEmployed 307 (71%) 56 (37%) <0.001
Screening referrala
Yes 173 (39%) 103 (68%) <0.001PersonalityScores on trait anxiety 16.9 � 5.0 18.1 � 5.4 0.009High trait anxiety 72 (16%) 42 (28%) 0.002Neuroticism 25 (6%) 13 (9%) 0.241
Disease stage at diagnosisStage 0 13 (8%)Stage I 82 (54%)Stage IIa 34 (23%)Stage IIb 10 (7%)Stage III 12 (8%)
Type of operationBreast Conserving Treatment 108 (71%)Mastectomy 42 (28%)No operation 1 (0.7%)
Adjuvant therapyReceived chemotherapy 50 (33%)Received radiotherapy 118 (78%)Received hormonal treatment 59 (40%)
a Screening referral ¼ women referred by the national breast cancer screeningprogram.
b Significant p-values are presented in bold.
C.M.G. Keyzer-Dekker et al. / The Breast 21 (2012) 746e750748
(p¼ 0.043, Table 2). Concerning psychosocial care in the BBD groupwomen with HTA used this modality more frequently comparedwith women with NHTA (p < 0.001). In women with BC and HTAmore use of psychosocial care was found (p ¼ 0.002). (Table 2)
Multiple regression analyses for the BBD and BC group revealedthat the most important predictors for HCU in the BBD group wereseveral domains of QoL, and in the BC group the type of operationand adjuvant treatment. Multiple regression analyses for the fourgroups based on diagnosis (BBD or BC) and trait anxiety (HTA orNHTA) revealed several predictors (Table 3). In women in the BBDgroup with NHTA the predictors for increased HCU were lowerscores on psychological, physical, general and environmentaldomains of QoL. In the BBD group women with HTA the predictorsfor increased HCU were not having work, lower score on generaldomain of QoL, and not having a partner (Table 3). In the BC groupwith NHTA the most important predictors for HCU were chemo-therapy and lower score on social QoL, and in women with BC andHTA hormonal treatment, not having children, and educationallevel (Table 3).
Discussion
The aim of the present study was to analyze the HCU and thepossible predictors for HCU in women with BBD or BC during thefirst year following the diagnosis. An increase in HCU was expectedin women with HTA irrespective of the diagnosis.
Overall, women with BC were visiting the GP and the MD morefrequently compared with women with BBD. In previous studiesthese findings are confirmed in women after BC treatment, evenfifteen years after diagnosis the HCU is found to be higher.12e14,27,28
This higher number of visits to the GP andMD is normal consideringthe BC (adjuvant) treatment during the first year. Subsequently, wefound that chronically anxious women with BC used morepsychosocial support during the first year after the diagnosis BC.This effect is not unexpected considering the higher levels ofanxiety and lower QoL during the diagnostic process of suspectedBC, especially in women with HTA.7 In women with BC even five
Table 3Outcomes of the multiple regression analyses on significant predictors for healthcare utilization in the first year after benign breast disease (BBD) and breast cancer(BC) and the high or not high score on trait anxiety.
HCUfirst year
Group Independent factor R2 Beta p-value
BBDGP NHTA Environmental domain QoL 0.016 �0.152 0.022
Physical domain QoL 0.060 �0.159 0.017HTA Having work 0.111 �0.333 0.013
MD NHTA General domain QoL 0.051 �0.235 <0.001HTA General domain QoL 0.086 �0.293 0.030
PS NHTA Psychological domain QoL 0.020 �0.140 0.011HTA Having a partner 0.126 �0.355 0.007BC
GP NHTA Social domain QoL 0.079 �0.285 0.005Hormonal therapy 0.042 0.205 0.042
MD NHTA Chemotherapy 0.155 0.355 <0.001Type of operation 0.039 0.202 0.034
HTA Having children 0.215 �0.619 <0.001Educational level 0.120 0.345 0.015Hormonal therapy 0.110 0.336 0.014
PS NHTA Having work 0.066 0.257 0.012
Abbreviations: HCU ¼ health care utilization; GP ¼ general practitioner;BBD ¼ benign breast disease; NHTA ¼ not high score on trait anxiety; HTA ¼ highscore on trait anxiety; BC ¼ breast cancer; QoL ¼ Quality of Life; MD ¼ medicaldoctor; PS ¼ psychosocial health care.R2 ¼ percentage of variance in the scores of the dependent variable explained by theindependent variable (1.00¼ 100%); Beta: a negative Beta means that a higher scoreon the independent variable will result in a lower score of the dependent variable.

C.M.G. Keyzer-Dekker et al. / The Breast 21 (2012) 746e750 749
years after the diagnosis a higher use of mental health care is stillfound, especially because of anxiety and sleep disorders.29 Inwomenwith BC no significant influence of HTA on GP andMD visitswas seen. This effect is partly explained by the fact that all womenwith BC visit the GP andMDalready very frequently as a part of their(adjuvant) treatment and follow up protocol for BC. Apparently,even chronically anxiouswomen experience this intensive standardfollow up as sufficient enough for comforting their fears and needs.
However, in women with BBD, HTA had an evident impact onthe use of GP, MD and PS. Trait anxiety can be defined as a relativelystable individual difference in anxiety proneness.11 Those chroni-cally anxious women become even more anxious during the diag-nostic process, and need more reassurance to confirm that thediagnosis is not BC. Apparently, this higher need for reassurancecauses an increase in HCU. Previously, the higher need for reas-surance was found especially in women with higher levels ofanxiety and perceived stress.8
In addition, important predictors for increased HCU in themultivariate regression analysis were lower scores on several QoLdomains at baseline, irrespective of diagnosis. QoL as predictor forHCU in women was not found before, but in previous studies QoLwas measured with SF-36 or SF-12 and QOL-CS.30,31 These ques-tionnaires measure health status, which indicates whether thereare limitations in physical possibilities, social activities, and state ofmind, but reveals nothing about the feelings individuals haveconcerning their functioning. (General) QoL, however, also reflectsto what extent a patient is bothered by limitations in daily life.Therefore, health status and QoL cannot be considered comparableor interchangeable for that matter.32 It is known that trait anxietyhas a very profound impact on QoL, this influence is even moreimportant than the diagnosis being BBD or BC.4 The importantinfluence of QoL on HCU is probably partly explained by this effectof trait anxiety on QoL. Apparently, chronically anxious womenhave an increased need for health care because the possibility ofhaving BC is causing an extreme disturbance of their life withimpaired QoL as a result.
To our knowledge, this is the first study analyzing trait anxietyand QoL scores as factors for predicting HCU inwomenwith BBD orBC. In this study a true and valid baseline measurement, i.e. beforethe diagnosis was known, of both trait anxiety and QoL was done.This study is based on self-reported use of health care. Therefore, anunderestimation of HCU is possible because of the effort of recallingall medical contacts in the previous twelve months. However, inboth groups (BBD and BC) the same method was applied. In addi-tion, more women with BBD and HTA were found in the drop-outgroup. If these women had not dropped out, we can assume thatour results would have been even more convincing.
In conclusion, the most important factors for increased HCUwere HTA and lower scores on QoL, especially in women with BBD.In women with BC a higher PS use was seen in chronically anxiouswomen. Therefore, it is very important to identify women witha lower QoL score and/or HTA with a psychometric test, who mayneed extra (psychosocial) health care during and after the diag-nostic process in case of a first event of breast disease. Thesewomen can then be offered a tailor-made follow-up protocol whichwill anticipate to their specific (mental) health care needs after thediagnosis BBD or BC. Through this individual approach womenwhoneed more support will be recognized and this will prevent thatthese women are unnecessary suffering without receiving extra(psychosocial) health care.
Ethical approval
Approval of the study protocol was given by the Medical EthicalCommittee of the primary research hospital.
Funding source
This work had no specific funding.
Conflict of interest statement
All authors have no conflict of interest and no financialdisclosures.
Acknowledgments
The authors acknowledge M.F. Ernst and G.A.P. Nieuwenhuijzenfor their help in patient accrual. The authors thank the registrationteam of the Comprehensive Cancer Center South for the collectionof data for the Cancer Registry and the scientific staff of theComprehensive Cancer Center South for their contribution to theselection and interpretation.
References
1. Ferlay J, Parkin DM, Steliarova-Foucher E. Estimates of cancer incidence andmortality in Europe in 2008. Eur J Cancer 2010;46:765e81.
2. National Cancer Institute. Probability of breast cancer in American women[updated 2010; cited 2010 14-12-2010]; Available from, http://www.cancer.gov/cancertopics/factsheet/Detection/probability-breast-cancer;2010.
3. Integraal Kanker Centrum Nederland. Meest voorkomende kankersoorten inNederland [updated 2010; cited 2010 14-12-2010]; Available from: http://www.ikcnet.nl/page.php?id¼2985&nav_id¼114; 2010.
4. Van der Steeg AFW, De Vries J, van der Ent FWC, Roukema JA. Personalitypredicts QoL six months after the diagnosis and treatment of breast disease.Ann Surg Onco 2007;14:678e85.
5. Woodward V, Webb C. Women’s anxieties surrounding breast disorders:a systematic review of the literature. J Adv Nurs 2001;33:29e41.
6. Witek-Janusek L, Gabram S, Mathews HL. Psychologic stress, reduced NK cellactivity, and cytokine regulation in women experiencing diagnostic breastbiopsy. Psychoneuroendocrinology 2007;32:22e35.
7. van der Steeg AFW, Keyzer-Dekker CMG, De Vries J, Roukema JA. Effectof abnormal screening mammogram on quality of life. Br J Surg2011;98:537e42.
8. Meechan GT, Collins JP, Moss-Morris RE, Petrie KJ. Who is notreassured following benign diagnosis of breast symptoms? Psycho-Oncology2005;14:239e46.
9. Montgomery M, McCrone SH. Psychological distress associated with the diag-nostic phase for suspected breast cancer: systematic review. J Adv Nurs2010;66:2372e90.
10. Schreier AM, Williams SA. Anxiety and quality of life of women whoreceive radiation or chemotherapy for breast cancer. Oncol Nurs Forum2004;31:127e30.
11. Spielberger CD, Gorsuch RL, Lushene RE. The state-trait anxiety inventorymanual. Palo Alto, CA: Consulting Psychologists Press; 1970.
12. Peuckmann V, Ekholm O, Sjogren P, Rasmussen NK, Christiansen P, Moller S,et al. Health care utilisation and characteristics of long-term breast cancersurvivors: nationwide survey in Denmark. Eur J Cancer 2009;45:625e33.
13. Van de Poll-Franse LV, Mols F, Vingerhoets AJ, Voogd AC, Roumen RM,Coebergh JW. Increased health care utilisation among 10-year breast cancersurvivors. Support Care Cancer 2006;14:436e43.
14. Mandelblatt JS, Lawrence WF, Cullen J, Stanton AL, Krupnick JL, Kwan L, et al.Patterns of care in early-stage breast cancer survivors in the first year aftercessation of active treatment. J Clin Oncol 2006;24:77e84.
15. Nord C, Mykletun A, Thorsen L, Bjoro T, Fossa SD. Self-reported health and useof health care services in long-term cancer survivors. Int J Cancer2005;114:307e16.
16. Van der Ploeg HM, Defares PB, Spielberger CD, ZBV. A dutch-language adapta-tion of the Spielberger state-trait anxiety inventory. Lisse, The Netherlands:Swets&Zeitlinger; 1980.
17. Van der Bij AK, De Weerd S, Cikot RJ, Steegers EA, Braspenning JC. Validation ofthe Dutch short form of the state scale of the Spielberger State-Trait AnxietyInventory: considerations for usage in screening outcomes. Community Genet2003;6:84e7.
18. Hoekstra HA, Ormel J, De Fruyt F. Handleiding bij de NEO Persoonlijkheidsvragenlijsten NEO-PI-R, NEO-FFI. [manual for the NEO Personality InventoriesNEO-PI-R and NEO-FFI]. Lisse, the Netherlands: Swets & Zeitlinger B.V;1996.
19. Costa PT, McCrae RR. NEO-PI-R: professional manual. Odessa, FL: PsychologicalAssessment Resources; 1992.
20. Hann D, Winter K, Jacobsen P. Measurement of depressive symptoms in cancerpatients: evaluation of the Center for Epidemiological Studies Depression Scale(CES-D). J Psychosom Res 1999;46:437e43.

C.M.G. Keyzer-Dekker et al. / The Breast 21 (2012) 746e750750
21. Schroevers MJ, Sanderman R, van Sonderen E, Ranchor AV. The evaluation ofthe Center for Epidemiologic Studies Depression (CES-D) scale: depressed andpositive affect in cancer patients and healthy reference subjects. Qual Life Res2000;9:1015e29.
22. MichielsenHJ, DeVries J, VanHeckGL. Psychometric qualities of a brief self-ratedfatiguemeasure: the fatigue assessment scale. J PsychosomRes 2003;54:345e52.
23. Michielsen HJ, Van der Steeg AF, Roukema JA, De Vries J. Personality and fatiguein patients with benign or malignant breast disease. Support Care Cancer2007;15:1067e73.
24. WHOQOL group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol Med 1998;28:551e8.
25. Van Esch L, Den Oudsten BL, De Vries J. The World Health Organization Qualityof Life instrument - Short orm (WHOQOL-BREF) in women with breast prob-lems. Int J Clin Health Psychol 2011;11:5e22.
26. Greene FL, Page DL, Fleming ID, Fritz AG, Balch CM, Haller DG, et al. AmericanJoint Committee on cancer staging manual. 6th ed. New York, NY: Springer;2002.
27. Kataja V, Castiglione M. Primary breast cancer: ESMO clinical recommenda-tions for diagnosis, treatment and follow-up. Ann Oncol 2009;20(S4):10e4.
28. Hanchate AD, Clough-Gorr KM, Ash AS, Thwin SS, Silliman RA. Longitudinalpatterns in survival, comorbidity, healthcare utilization and quality of careamong older women following breast cancer diagnosis. J Gen Intern Med2010;25:1045e50.
29. Earle CC, Neville BA, Fletcher R. Mental health service utilization among long-term cancer survivors. J Cancer Surviv 2007;1:156e60.
30. Hodgkinson K, Butow P, Hunt GE, Pendlebury S, Hobbs KM, Wain G. BreastCancer survivors’ supportive care needs 2e10 years after diagnosis. SupportCare Cancer 2007;15:515e23.
31. Mols F, Helfenrath KA, Vingerhoets AJJM, Coebergh JWW, van de Poll-Franse LV. Increased health care utilization among long-term cancer survivorscompared to the average Dutch population: a population-based study. Int JCancer 2007;121:871e7.
32. Van der Steeg AFW, De Vries J, Roukema JA. Quality of life and health status inbreast carcinoma. Eur J Surg Oncol 2004;30:1051e7.