Embed Size (px)
Citation preview
Health Assessment in Libyan Holding Centres
__________________________
Key findings and Priorities for intervention
MI.
CO
.L P
RO
JE
CT
"PR
OJE
CT
TO
EN
HA
NC
E M
IGR
AN
TS
' C
ON
DIT
ION
S IN
LIB
YA
N H
OL
DIN
G C
EN
TR
ES
”
Fu
nd
ed
by IO
M 1
035 F
acilit
y

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
In the photo (F. Lembo): distribution of hygienic items to migrants in Tueisha Centre

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
TABLE OF CONTENTS Implementation partners Selected Abbreviations Definition of key terms
Chapter 1: Background and Justification Chapter 2: Methodology Chapter 3: Data Collection and Findings Chapter 4: Priorities for Intervention Chapter 5: Conclusions and Way Forward
Annexes

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
IMPLEMENTATION PARTNERS
The MI.C.O.L. Project has been carried out by IOM in close partnership with the following Libyan NGOs: World Islamic Call Society, Red Crescent and the National Centre for Infectious Diseases. International Organization for Migration (IOM) 1 Established in 1951, IOM is the leading inter-governmental organization in the field of migration and works closely with governmental, intergovernmental and non-governmental partners. With 127 member states, IOM is dedicated to promote humane and orderly migration for the benefit of all. It does so by providing services and advice to governments and migrants. The IOM Mission in Tripoli, established in April 2006, closely cooperates with Libyan Government and Libyan Civil Society: areas of collaboration include capacity building, assistance to stranded migrants including assisted voluntary return and reintegration, research, migration health, border management, as well as counter-trafficking. World Islamic Call Society (WICS) 2 Established in 1972, WICS is an Islamic NGO based in Tripoli with 34 field offices located in all continents. It works in several fields, including cooperation with International Organizations, education, support to migrants, victims of human or natural made disasters. Cooperation with IOM started in 2008, in a project which foresaw direct assistance to migrants kept in Libyan Holding Centres (Prometeo I). WICS scholars specifically trained and belonging to different African countries, still form part of the relief providers group, tasked with the implementation of relief activities into Holding Centres under the IOM managed Prometeo II Project. Libyan Red Crescent 3 Based in Benghazi, Libyan Red Crescent has branch offices throughout Libya. In the past, it has operated in Holding Centres for irregular migrants, providing specific responses to immediate needs of migrants. Cooperation with IOM started in 2010 under the Framework of Prometeo I, which foresaw direct assistance to migrants kept in Libyan Holding Centres. National Centre for Infectious Diseases (NCID) 4 Established in 2002 and based in Tripoli, NCID is one of the most important health Centres in Libya, covering a wide spectrum of areas, such as prevention and control of communicable diseases, health research, health-prevention education, collection and publication of epidemic data.
1 Additional information can be found at http://www.iom.int 2 Additional information can be found at http://www.islamic-call.net/english/ 3 Additional information can be found at http://lrc.org.ly/ 4 Additional information can be found at http://nidcc.org.ly/nidcc/
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
SELECTED ABBREVIATIONS
AOWYC: African Organization for Youth, Women and Children GPC: General People’s Committee IOPCR: International Organization for Peace, Care and Relief MRF: Mission with Regional Functions MHD: Medical Health Division MAC: Manila Administrative Centre NASD: National Association for Social Development NCID: National Centre for Infectious Diseases NGO: Non Governmental Organization WICS: World Islamic Call Society WHO: World Health Organization

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
DEFINITION OF KEY TERMS
Irregular Migrant The term irregular migrant refers to someone who lacks legal status in a transit or destination country. This can be due to the fact that this person has breached the entry regulations of a country or his/her visa or work permit has expired. In other words, irregular migrants are those non-nationals who have not been granted permission to enter or to stay in a given country. An irregular migrant is also referred to as clandestine, illegal, undocumented migrant or migrant in an irregular situation. However, the term irregular is preferable and does not have a criminal connotation. Detained migrant or detainee The term “detainee” is used in different ways in different countries. The term sometimes relates only to persons at the pretrial stage or under administrative detention, and not to convicted prisoners: according to the terminology used by International Organizations, the term “detained person” refers to someone who has been deprived of personal liberty, except as a result of conviction for an offence (see Body of Principles for the Protection of All Persons under Any Form of Detention or Imprisonment, Use of Terms, G.A. res. 43/173, annex, U.N. Doc. A/RES/43/173 (Mar. 19,1989). In the present report, the term “detainee” is used in its broadest possible sense to cover any person deprived of personal liberty as a result of arrest, administrative detention, pretrial detention or conviction and held in a place of detention. Terms such as “apprehended migrants”, “with-held migrants” will be also used with this meaning. .

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
Background and
Justification
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
10
1.1 Context of irregular migration to and through Libya With its location on the major crossroads to Southern Europe on the Mediterranean Sea and its extensive and complex borders mostly located in remote areas5, Libya has become one of the preferred transit routes for many migrants coming from Sub‐Sahara African and Asian countries. At the same time, Libya’s booming economy, based on oil and gas wealth, has amplified its role as a destination country, attracting every year thousands of workers. Although official data is scarce, it is estimated that approximately one and a half million migrants are present in the country (out of an estimated six million inhabitants), with a high proportion of them in irregular status. 1.2 Holding Centres for apprehended migrants in Libya It is reported that at least eighteen holding Centres6 in Libya accommodate thousands of irregular migrants apprehended a) at sea on their way to Europe, b) upon illegal entry on Libyan territory or c) in Libya without being in possession of proper documentation (i.e. over‐stayers), awaiting to be deported or returned to their countries (see map, Annex 1). In general, the premises and buildings currently used to host irregular migrants have not been designed for this purpose and therefore are inadequate, both in terms of quantitative capacity as well as in terms of management and services provided to the detainees. 1.3 Local NGOs and IOM engagement In close coordination with Libyan authorities and civil society (WICS, Red Crescent, Alwafa, NASD7), IOM has been undertaking significant steps to upgrade the conditions of such Centres. In April 2009, a pilot initiative (Prometeo I, funded by Italian Ministry of Foreign Affairs), was carried out in the Holding Centres of Garabulli and Zawya. With training and supervision from IOM, a group of relief providers from Libyan NGOs8 provided assistance services to migrants in these Centres. Services included the establishment of a functional medical clinic (with a doctor examining patients and prescribing medications), the distribution of hygienic and personal material (such as shampoo, soap, toothbrush, toothpaste, clothes,
5 4,000 km along the desert and 1,700 km on the Mediterranean shores. 6 The official holding Centres for migrants are Zwara, Surman, Al Jimayl, Al-Zawya, Tweisha, Garabulli, Ghariyan, Bani Walib, Zlitan, Misrata, Sirt, Ejdabiya, Benghazi, Al Marj, Sebha, Al Qatroun, Al Kufra, Sabratha. 7 National Association for Social Development 8 The Prometeo I Project was carried out in cooperation with the following NGOs: WICS, ALWAFA, NASD, IOPCR

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
11
slippers, etc.), and the provision of psycho‐social and religious support, through religious scholars studying at WICS. The successful implementation of the Prometeo I initiative set the basis for the design and implementation of the project’s second phase (Prometeo II, funded by Italian Ministry of Foreign Affairs), carried out in close cooperation with relevant Libyan Authorities and with a network of trained relief providers from Libyan NGOs (WICS, NCID, NASD, AOYWC, Red Crescent)9. In the framework of this initiative, the team of relief providers, seconded by local NGOs and supervised by IOM, is accessing, since April 2010, the Tueisha Centre twice a week, providing relief support and basic health counselling. 1.4 Request from the General People’s Committee(GPC) for Health – IOM 1035 Project Micol Recognizing IOM efforts to improve conditions in the holding Centres through previous project activities, and concerned about potential negative impact of the insanitary and unhealthy conditions inside holding Centres on the general Libyan population, the GPC for Health submitted, on 12 October 2009, a specific written request to IOM. The request was for “assessing priorities of intervention and needs to be addressed in order to improve living conditions for migrants detained in holding Centres and, eventually, decrease risks of diffusion to the Libyan population of transmittable diseases” (see Annex 2). In response to this request, the IOM Mission in Libya designed a pilot intervention to address the main concerns identified by local stakeholders. Thus, on 15 December 2009, a project, titled M.I.CO.L (“Project to improve Migrants` conditions in Libyan Holding Centres”) was approved and funded by IOM (1035 Facility). 1.5 MICOL project objectives Specifically designed to contribute to a better management and planning of health care services for the benefit of all persons being held and working in Libyan holding Centres (apprehended migrants, civil and security personnel), the MICOL Project aims to assess the public health/sanitary conditions in these premises and identify priorities for intervention to be submitted to the GPC for Health. To achieve this objective, the project has been structured according to three different phases: 1) design and development of the survey’s tools, as well as preparation of health professionals involved in the exercise; 2) implementation
9 WICS, World Islamic Call Society at http://www.islamic-call.net; NCID, National Centre for Infectious Diseases; AOYWC, African Organization for Youth, Women and Children.

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
12
activities including the assessment mission; 3) draft of priorities for intervention and follow‐up.
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
Methodology
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
14
2.1 Study Team The Study Team has been composed by 4 IOM Officers (from IOM missions in Tripoli, Rome and Manila) and 3 experts from WICS, Red Crescent and NCID respectively: it included 3 medical doctors, 1 epidemiologist, 1 health sociologist and 2 technical cooperation staff. 2.2 Assessment tools For the assessment of the hygienic and health conditions in the holding Centres, the MICOL Project envisaged the use of both quantitative (questionnaire) and qualitative (interview with directors and on site observations) assessment tools. 2.3 Quantitative instrument: the questionnaire Designed in close collaboration between IOM/MRF Rome, IOM/MHD‐MAC and the IOM Tripoli experts, the questionnaire for collecting quantitative information from apprehended migrants, drafted in English and subsequently translated into Arabic, addressed different topics to acquire the following sets of information:
1. Socio‐demographic and family information 2. Medical history prior to entry in holding Centres 3. Medical complaints and access to medical services during the stay in
the holding Centres 4. Reproductive health during the stay in the Centres (for women only) 5. Material/Living conditions 6. Opinions on activities and routine, including social interactions 7. Opinions on overall experience in the Centre 8. Stay in the Libyan Arab Jamahiriya
A sample of the questionnaire and related guidelines for its administration are available at Annex 3 2.4 Qualitative instruments: set of core open‐ended questions and checklist for observation For the collection of qualitative information, the study team developed two different tools:
a) A set of core open‐ended questions to be used in key informant interviews with the directors of the holding Centres. The following main categories were included:
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
15
i) General information on the situation of the Centres ii) Healthcare facilities for apprehended migrants iii) Hygiene conditions at the Centre iv) Health‐related concerns of Staff v) Any other additional comments from the Director
b) A checklist for the recording of the observation made by the study team in the holding Centres visited. This checklist included the following categories:
i) Material and hygiene conditions at the Centre – for apprehended
migrants and for staff ii) Healthcare facilities for apprehended migrants iii) General observations about staffing and management
All the tools developed for this project benefitted from the review of similar instruments available in literature10. 2.5 Field‐worker training Before the assessment in the selected holding Centres was carried out, a one‐ and‐half day training session, aimed at providing the necessary skills to the interviewers, was conducted in May 2010. The trainees‐interviewers, health professionals from NCID, Red Crescent and WICS, were trained on the administration of the questionnaire in the specific setting of the holding Centres. In particular the sessions featured the following modules:
- how to behave in respect of the human dignity of the interviewed - how to handle the tool – the questionnaire – designed by the research
team In order to get accustomed with the questionnaire’s administration, the interviewers’ skills were tested and refined through simulations. 2.6 Holding Centres selected for this exercise The selection of holding Centres to visit, conducted in close cooperation with Libyan Authorities, has taken into consideration different criteria, including:
a) Geographical coverage: holding Centres located in the three main areas of the country (Tripoli, Benghazi and Sebha), along the coast (usually hosting
10 See, among others, Guidelines and Best Practices for Migrant Accommodation Centres in Ukraine, IOM, 2007
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
16
migrants intercepted and apprehended at sea) or in the desert (usually hosting migrants trying to reach the coastal area).
b) Centres` typology: covering samples of “transit Centres”, usually hosting migrants for a limited period of time (few weeks/months) before being sent to other Centres or “long‐term Centres”, usually hosting migrants until deportation takes place (up to years).
c) Gender balance, targeting holding Centres hosting men, women or a mixed population
d) Nationality balance, focusing on Centres hosting different nationalities, not only from Sub‐Saharan Africa but also from other continents (i.e. Asia)
e) Centres` size, covering large, as well as small holding premises According to the criteria above specified, seven Centres had been identified as the most adequate to visit:
i) Zawya Centre ii) Tueisha Centre, Tripoli iii) Zlitan Centre iv) Alqwaa Centre, Garabulli v) Sebha Centre vi) Ajdabiya vii) Kamfouda, Benghazi
2.7 The key informant With respect to the qualitative interviews, the directors were selected as key informants: by virtue of their position, they have been considered to be in possession of the relevant information to achieve the assessment goals. 2.8 Sample of migrants The selection of migrants to be interviewed through the questionnaire has been conducted according to the following principles:
i) Include only those migrants voluntarily willing to give informed consent to participate in the interview.
ii) Envisage a threshold – set at 10% of respondents out of the total population hosted in the Centre – in order to consider the collected data statistically relevant (though not representative).
iii) Ensure representation of both genders through a threshold set at 25% of women out of the total number of interviewed migrants.

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
17
iv) Ensure representation of at least 20 different nationalities. v) Ensure representation of migrants having different ages (age balance).

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
Data collection and
findings
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
20
3.1 Introduction This chapter presents the findings from all the data and information gathered through the interview with the directors of the Centres, the direct observation of the premises by the team and the analysis of the questionnaires administered to the detained migrants (see above, Chapter II). Findings from the two sources of information, Centre authorities and research team on the one hand, apprehended migrants on the other, are kept separated and reported in two different sections (3.2 and 3.3 respectively).
SECTION ONE 3.2 Site visits (Interview with directors and study team observations) In‐depth interviews were conducted by the study team during site visits to the Centres that were held from June 7 to 16, 2010. In each Centre, the study team spent approximately 45 minutes to an hour interviewing the Directors on core questions concerning living and health conditions in the Centres. Following the interviews with the Directors, the study team, accompanied by the staff, was allowed in the premises, accessing the living quarters of migrants, the common areas (like kitchen, outdoor spaces, storage rooms) and the working/rest areas for staff. The overall key findings from the site visits (interview with Directors and observation) are herewith listed: Generally the premises are not designed for hosting people because most of them are refurbished former warehouses.
Rooms are generally overcrowded with poor ventilation. Sanitary facilities (toilets, bathing areas, washing sinks) are commonly out of order or broken, without running water.
There is not enough bedding and linen for the migrants who often sleep on the same unclean mats/mattresses which are rarely changed or cleaned.
There is no provision for drinkable water in sufficient quantities. Most Centres lack on‐site medical clinics and none provide medical exams upon arrival. Generally there is no dedicated health care staff working in the Centres and no provisions for medical supplies.
Generally no ambulance services are available for transferring severe cases to health care facilities and no other emergency medical services are accessible.
Staff working in the holding Centres does not receive any training on migration or health issues; also, there are no provisions for staff for disease protection and occupational health promotion.
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
21
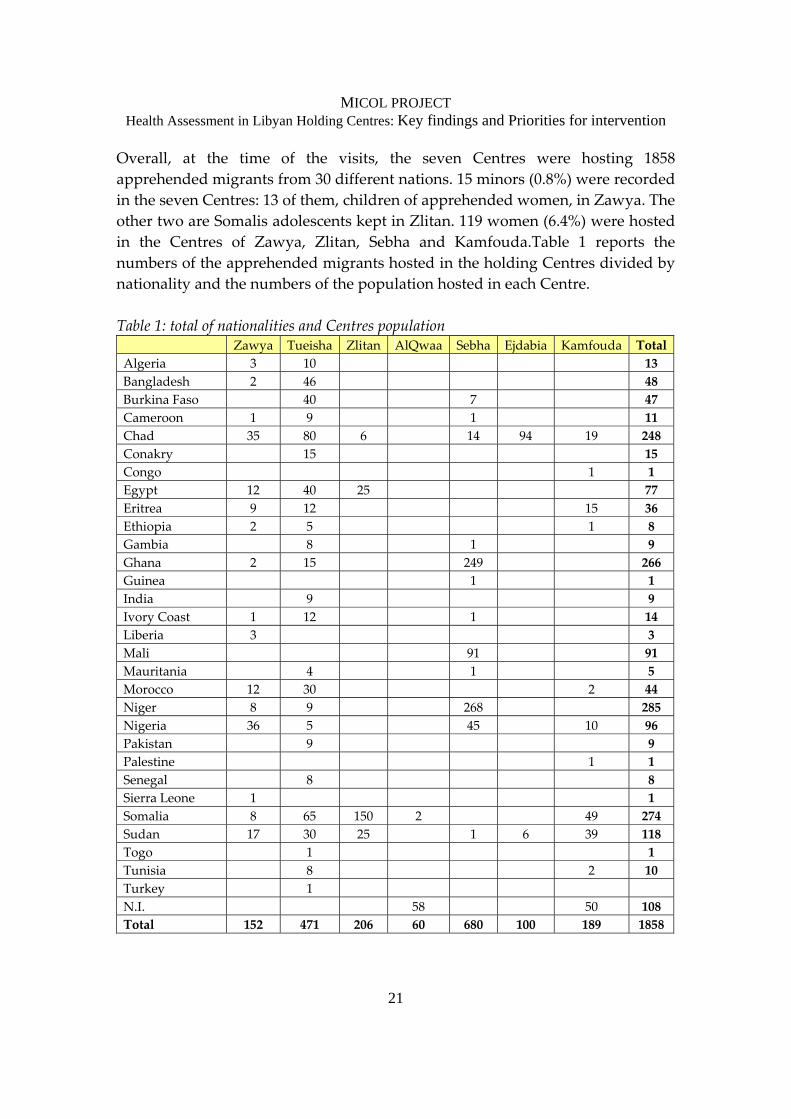
Overall, at the time of the visits, the seven Centres were hosting 1858 apprehended migrants from 30 different nations. 15 minors (0.8%) were recorded in the seven Centres: 13 of them, children of apprehended women, in Zawya. The other two are Somalis adolescents kept in Zlitan. 119 women (6.4%) were hosted in the Centres of Zawya, Zlitan, Sebha and Kamfouda.Table 1 reports the numbers of the apprehended migrants hosted in the holding Centres divided by nationality and the numbers of the population hosted in each Centre. Table 1: total of nationalities and Centres population Zawya Tueisha Zlitan AlQwaa Sebha Ejdabia Kamfouda Total Algeria 3 10 13 Bangladesh 2 46 48 Burkina Faso 40 7 47 Cameroon 1 9 1 11 Chad 35 80 6 14 94 19 248 Conakry 15 15 Congo 1 1 Egypt 12 40 25 77 Eritrea 9 12 15 36 Ethiopia 2 5 1 8 Gambia 8 1 9 Ghana 2 15 249 266 Guinea 1 1 India 9 9 Ivory Coast 1 12 1 14 Liberia 3 3 Mali 91 91 Mauritania 4 1 5 Morocco 12 30 2 44 Niger 8 9 268 285 Nigeria 36 5 45 10 96 Pakistan 9 9 Palestine 1 1 Senegal 8 8 Sierra Leone 1 1 Somalia 8 65 150 2 49 274 Sudan 17 30 25 1 6 39 118 Togo 1 1 Tunisia 8 2 10 Turkey 1 N.I. 58 50 108 Total 152 471 206 60 680 100 189 1858

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
22
Security for apprehended migrants and staff is very difficult to be managed in a Centre with high variety of nationalities. Riots among different national and ethnic groups have been reported to be frequent: to avoid this, the Directors separate rooms according to migrants` nationalities. As a consequence, the number of people per room is not always balanced: some rooms are overcrowded while others are almost empty. The key findings above listed are a summary of the following detailed description from the on‐site visits of the seven Centres.
I) ZAWYA General information Located sixty km East of Tripoli, in the town of Zawya, the Centre is a converted grain warehouse, with eight rooms – about 40‐60 square meters large – housing approximately 25‐40 migrants each. At the time of visit,11 the Centre was holding about 102 women, 36 men and 14 children: women and children are kept separated from men.12 Security is ensured by 40 police guards who work in shifts: additionally, six civilian staff are working in the kitchen. Material and Hygiene conditions for migrants and staff Overall, the general cleanliness of the Centre is poor. The sewage system is not properly functioning. Rooms do not have fans or lights, only windows or vents in the walls towards the ceiling. There is no furniture, only mats and blankets for sleeping on the floor. The bathrooms are in a separate part of each room, and are used for bathing and as toilets. It should be noted that there are no toilet fittings – only holes in the floor of the bathrooms. Also, the washbasins are broken and filled with rubbish. Hygiene supplies and drinking water are not distributed on a regular basis: migrants use the water from the bathrooms also for drinking. The migrants are themselves responsible for the cleaning of the rooms. There is no space provision for spiritual/religious/outdoor activities. Recreation is extremely limited: the administration rarely allows migrants to walk around within the main building itself, usually on a random basis.
11 Visit to Zawya took place on June 8 2010, morning. 12 The migrants are reported to stay in the Centre for about three months on average.
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
23
The staff has separate living quarters, composed by two‐three very basic rooms, furnished with few chairs and mattresses and with lavatories outside. There is no separate space for rest and recreation for the staff. Health‐care facilities for migrants The Centre has an on‐site healthcare facility, refurbished by IOM and IOPCR in 2009: it is however not utilized due to the absence of qualified medical staff working in this holding Centre. Medicines are often obtained from unused supplies at surrounding public and private clinics and are provided by WICS and IOM upon request. There are no medical examinations offered to migrants upon entry, as well as no routine vaccinations are provided. Pregnant women do not receive specific medical attention for antenatal care. As referred by the Director, infants delivered at the public hospital are vaccinated through the public health services, although details on types of vaccines are not available. Severe medical cases, urging immediate attention, are referred to local hospitals and transferred in police cars, since no ambulance is available. No separate quarters are available for sick persons. There are no regulations for notification in case of health‐related events or disease outbreaks at the Centre. Health related concerns for staff There are no special provisions for health care access for the staff. They do not receive any training on general health education or first‐aid, nor are mandatory vaccinations required to them. Additional Remarks The Centre has made efforts to improve migrants’ health conditions, resorting, especially in the past, to local and international organizations for the establishment of a medical clinic and provision of medications. Such efforts need to be sustained over time, ensuring that a health professional is present, on a regular schedule, within the clinic.
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
24
II) TUEISHA (TRIPOLI) General information Close to Tripoli International Airport, Tueisha Centre is located in a large compound composed by two big barracks of about 200‐250 square meters each (up to 200‐250 migrants) and twelve smaller rooms of about 100 square meters each (up to 60 migrants per room), the latter having a courtyard outside which migrants can use at will. At the time of visit13 the Centre was holding 471 migrants, all adult males.14 Security in the Centre is ensured by 40 guards, who work in shifts of 7‐8 persons (24 hours work followed by 48 hours break). Material and Hygiene conditions Overall, the general cleanliness of the Centre is poor. The rooms have scarce ventilation and are furnished only with mats. There are two bathrooms per room, that are used for washing, bathing and also, as toilets. Hygiene and cleaning material are not distributed on a regular basis to the detainees, responsible to clean their own rooms. Bottled water is not available for drinking: migrants use water from the taps in the bathrooms for this purpose. Furthermore, there do not seem to be any hygiene inspections or cleaning regulations. Recreation is extremely limited, since migrants rarely are allowed to step outside the rooms. Staff quarters and lavatories are not clean or well‐maintained: a new building, still under construction, would be used also for allocating guards. Rest and recreation is extremely limited.15 Health‐care facilities for migrants The Centre has a refurbished medical clinic, properly functioning since April 2010: under IOM supervision, a group of local NGOs (WICS, Red Crescent, NASD and AOYWC) is providing assistance – twice per week – to the detainees, including distribution of sanitary items, medical check‐up visits and delivery of medications. No medical examinations are offered by the Centre to the migrants upon entry, as well as no routine vaccinations are provided. Severe medical cases are transferred to local hospitals in private cars, taxis or police vehicles, since no ambulances are available. 13 Visit to Tueisha took place on June 8 2010, afternoon 14 On average, it was reported that migrants from Nigeria, Mali and Ghana stay for about five days and then transferred to Sebha Centre. Those from other countries like Eritrea, Somalia and Ethiopia stay for about six-nine months. 15 A television is available in the Staff quarters
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
25
There are no regulations for notification in case of health‐related events or disease outbreaks at the Centre. Health related concerns of staff There are no special provisions for health care access for the staff. They do not receive any training on general health education or first‐aid. No mandatory vaccinations are required to the staff; however the director often ensures that the staff, including cooks, is vaccinated. Additional Remarks Cooperation with local and international Organizations is effective and led to a functioning medical clinic, with the regular presence of a doctor and a nurse two‐three times per week for the screening of migrants and provision of medications. Due to guards understaffing, recreation for migrants is extremely limited: however, in few cases, the Director allowed them to have common activities out of their rooms, such as football matches.
III) ZLITAN General information Located 160 km East of Tripoli, in the town of Zlitan, the Centre is composed by five rooms in one section and another set of three rooms in another section. At the time of visit16, the Centre was holding about 206 migrants – about 201 men, four women and one child. Each of the eight rooms or cells ‐ about 70 square meters large – can host 60 migrants. Women are kept in separate quarters from men.17 Security in the Centre is granted by 36 guards, who work in shifts of 7‐8 persons. Material and Hygiene conditions for migrants and staff The general cleanliness of the Centre is average. Although equipped with external AC units and hot water devices18, rooms’ conditions are basic: furnished only with mats, with light fixtures available inside and generally overcrowded. Drinking water is not available; hygiene supplies are not provided on a regular basis to the detainees for cleaning their own rooms and toilets (2 per each room). Food provisions are properly stored in a cold room.
16 Visit to Zlitan took place on June 9 2010, morning 17 Two additional small rooms are used to confine migrants for punishment (two persons were seen to be detained at the time of visit). 18 It was not clear whether AC and hot water units were working and in use

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
26
Recreation activities are extremely limited, since migrants are never allowed to step outside their room. Security staff is accommodated in a big unfurnished room with a separate bathroom (used for washing, bathing and as toilet). An additional room is dedicated to rest and recreation. Health‐care facilities for migrants Health care facilities for migrants are extremely limited: a room is refurbished as medical clinic, but it is not functioning due to the lack of qualified medical personnel; examinations are not provided to the migrants upon entry, as well as vaccinations are not offered to them. In case of medical complaints, the migrants are referred to the local hospitals in police cars. If an out‐patient setting is possible, sick migrants are brought back.19 Similarly, staff working in the Centre has no access to on‐site health‐care services – no special arrangements are available for them. There are no regulations for notification in case of health related events: in case of a confirmed infectious disease, the Centre informs the local health authority that, in turn, informs the National Centre for Infectious Diseases. There are no set arrangements for the quarantine of sick persons affected by transmittable diseases. These cases have been handled in different ways, through isolation by emptying one room – thereby creating overcrowding in others – or through transfer to other Centres. Health related concerns of staff Staff does not receive any training on health education or first aid. No special allowances or health care services access is made available to them. There are no mandatory vaccination requirements but the Director often requires his staff to obtain vaccinations from local health Centres. Additional Remarks The Director created and maintains an electronic database where information for each migrant are filed, including personal information (such as name and nationality), date and cause of detention, referral to hospitals, next steps for transfer. The Director’s office is well maintained and equipped with a video‐surveillance system monitoring the entire space of the Centre, including the corridor of the five rooms and the courtyard of the three room space. 19 In the last six months, the administration received about two to three requests for medical referrals per week.
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
27
IV) ALQWAA (GARABULLI) General information Located some 50 km East from Tripoli, in the proximity of the town of Garabulli, the Al‐Qwaa Centre hosted, at the time of visit 20, around 60 people, all male and adults, in six rooms 21, each 50/60 square meters big. Security is granted by 19 police staff, working in shifts.22 Material and Hygiene conditions for migrants and staff In general, the Centre is characterized by extremely poor conditions and an overall unhealthy environment. The general cleanliness of the Centre is very poor: the premises (including the director’s office) looked very dirty and were infested with flies. The rooms, equipped with air‐condition units which did not seem to be functional, are small and dark, unfurnished, with one bathroom available in each. Food is stored in a compartment together with mats and cleaning devices. A kitchen, in which meals are prepared by apprehended migrants, is furnished with basic items. The rooms open in a central courtyard, where migrants, on rotation, are allowed to clean themselves up and take some steps in the morning sunlight. No separate room is available for staff as their living quarters (there used to be one refurbished by IOM in 2009, which is not available anymore). Health‐care facilities for migrants There is no clinic on‐site for migrants; those with medical complaints are taken to the local hospital and transferred in police cars. In 2009, IOM refurbished one room as a clinic, providing it with medical equipment (stretcher, drawer, examination bed, etc.): unfortunately, it is now closed and abandoned. Health related concerns of staff There are no medical examinations for staff and no mandatory vaccinations. Additional Remarks According to what referred, migrants are allowed to step in the central courtyard every day on rotation, thus having the possibility to get some sunlight.
20 Number of apprehended migrants per room varies (i.e. in 2009, there were up to 450 people hosted). 21 At time of visit, one room was out of order. 22 Differently from other Centres, here the guards are constantly carrying weapons.

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
28
Cooperation with local and international organizations, although started for a limited period in 2009 with the establishment of a medical clinic, was then stopped. It however represented an effort to improve the precarious health conditions for migrants.
V) SEBHA General information Located in the South‐West part of Libya, in the town of Sebha, the Centre represents the main gateway for the repatriation of those living in Sub‐Saharan countries.23 It hosted at the time of the visit 24 680 apprehended migrants, 17 of whom were women.25 There are two big buildings which contain twelve rooms, each measuring 80‐100 square meters and hosting up to 90 migrants. Material and Hygiene conditions for migrants and staff The general cleanliness of the Centre is average. There are light fixtures inside the rooms. Some rooms are equipped with standing fans and TV sets (belonging to the detainees themselves). There are bathrooms with common bathing/wash/toilet area, about three per room (36 in total) located in separate living quarters. Daily, about 60000 liters of sewage is cleared out of the Centre. There is scheduled hygienic supply distribution to migrants – each person receives one soap bar and one shampoo every ten days. The rooms are sprayed against insects and cleaned by the detainees themselves on a daily basis. The kitchen is very clean, and the food very well kept in different storage rooms. The officer in charge has a house on‐site. Other staff has separate living quarters, with separate lavatories and bathrooms in good conditions. Health‐care facilities for migrants A furnished medical clinic has been established and is functional, with a doctor and six nurses, paid by the Centre and affiliated with the National Centre for Infectious Diseases: patients’ examination and medications’ provision are carried out every alternate day.
23 The Centre is composed by different separate buildings: the entrance gate leads into a big courtyard. Director’s office, storage room and staff quarters are on one side while kitchen and dining hall (around 170 square meters) on another side. Guards are not armed 24 Visit to Sebha took place on June 11 2010, morning 25 Duration of stay depends on nationality, but generally it doesn’t exceed 6 months. If a large number of migrants belonging to the same nationality are present in the Centre, an aircraft is usually arranged to return them back to their home country (i.e. Ghana, Mali, Nigeria).
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
29
Severe cases are referred to the local hospital in Sebha (2 km far) and transferred in police cars, since no ambulance is available: admitted until cured, sick migrants are then brought back to the Centre, unless infectious. There are no medical screening upon migrants’ admission into the Centre and no procedures for the notification in case of health‐related events. Similarly, there are no quarters for sick persons. Health related concerns of staff The staff does not receive any training on health and first aid. They are requested to obtain vaccinations. There are no other special provisions for their healthcare access. Additional Remarks It has been observed, during the visit, that detainees step out of the rooms for their meals, queuing up in the courtyard for collecting food items and eating together in small groups in the dining hall. Management maintains a register with records of the valuable belongings of the detainees, such as mobile phones that are stored in a locked safe. These are returned to the detainees when they leave the Centre. A small shop in the Centre sells basic food items and bottled beverages: detainees have been observed to move freely to this shop, during the meals.
VI) AJDABIYA General information Located 160 km South of Benghazi, in the town of Ajdabiya, the Centre is composed of six rooms, divided into two sets of three rooms each – each set with five toilets. The rooms measure about 40 square meters each and accommodate, at times, up to 50 migrants. At time of visit26 there were 100 detainees, all male and adults.27 Security is granted by 30 police staff, who work in shifts of 7‐8 (24 hours working followed by 48 hours break).
26 Visit to Ajdabiya took place on June 12 2010, morning 27 The maximum capacity of the Centre is about 250 detainees. The duration of stay varies from nationality, Usually within one month they are transferred to the respective home country, unless there are any political concerns such as the case for Eritreans or Somalis, whose stay is longer (up to 5/6 months). When deported, migrants are taken by bus to Al Kufrah, then in private buses and cars to Chad. Recently, about one week ago, 521 Sudanese were sent back to their home country.
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
30
Material and Hygiene conditions for migrants and staff The general cleanliness of the Centre is average. Rooms are equipped with two windows per room close to the ceiling and two ceiling fans each. Light fixtures were not observed. Migrants are provided only with thin mattresses. For every three rooms there is a separate area for washing and sanitary facilities – with water taps and five toilets, some of which have no doors. There is no separate shower/bathing area, these are combined with toilets and general wash area. The detainees are provided with hygienic supplies (soap, shampoo, etc): distribution of such items to the migrants depends on availability (material arrives from Tripoli) which is not regularly scheduled. Water from the taps in the cleaning/bathing area is used for drinking. Water tanks bring the water supply, which is distributed in common for cleaning and drinking, but there are no filtration mechanisms. The kitchen is clean and kitchen staff (four civilians) was reported to have received medical check‐ups. Food is well kept in a storage room located next to the kitchen: meals are distributed into the rooms in stainless steel bowls through a small hole in the wall from outside. Due to understaffing, migrants are usually not allowed to get out of the rooms, unless in smaller groups which guards can easily supervise. Staff’s quarters are separate with own bathrooms and lavatories, where running water is available. There is provision of bottled water for drinking. Although equipped with TV and AC units, staff’s offices and rest area are poor. Health‐care facilities for migrants A medical clinic has not yet been established in the Centre. In case of suspected disease, migrants are transferred by “box car”28 to local or Benghazi hospitals for appropriate follow‐up. Sometimes there are 15‐20 persons with potential infections within the same vehicle.29 There are no regulations for notification in case of health‐related events and no separate quarters for sick people/quarantine. Health related concerns of staff Although not trained, police staff provides basic medical care and medicines (like painkillers, antibiotics, topical antiseptic creams, etc.), if available, to
28 Re-arranged police pick-ups 29 Director reported that when the Centre has about 400-500 persons, then on average 20 requests are submitted per day for medical check-ups. This makes it difficult for the Centre to manage hospital transfers without a clinic on-site or ambulance.
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
31
migrants. There are no mandatory vaccinations or other health care provisions for staff. Additional Remarks It was observed, during the visit, a migrant receiving and having the opportunity to speak with two external visitors, accepting a drinking water container and some other items in three bags. Furthermore, it seems that migrants held in the Centre are allowed to retain and use their mobile phones.
VII) KAMFOUDA (BENGHAZI) General information Located in the suburbs of Benghazi, adjacent to a chemical factory and its dump‐yards30, Kamfouda Centre – the biggest visited – hosted, in four hangars containing each six rooms measuring 80 to 100 square meters, a mixed population of 188 migrants (11 of which women), at time of visit31. Women and men are kept in separated rooms.32 Security is ensured by 15 guards who work in shifts (one day working and three days off); additionally, 20 staff from the anti‐riot police wearing uniforms and working in shifts (one week working and two weeks off) are tasked with the surveillance of walls and gates.33 Material and Hygiene conditions The general cleanliness is average. Garbage is collected and placed outside the main Centre premises (since they have access to a large space). Sewage is also collected as needed. The big room at the end of the hangar has nine windows; smaller rooms with two windows each. There are no fans or light fixtures. Only thin mattresses are provided as furniture. There are bathrooms with common washing area and toilets, although it seems that no running water was available.
30 The burnt waste and its smoke heavily pollute the air. 31 Visit to Kamfouda took place on June 13 2010, morning; a week before the Centre hosted 800 persons 32 Kamfouda is a very big complex. External gate leads through a compound to another gate that leads to the main compound where the offices and living quarters are located. The average duration of the stay depends on nationality; Somalis usually stay up to 7-8 months, while Egyptians and Sudanese can leave in few days. For others, the Centre requests respective embassies to identify their citizens and issue travel documents. Detainees are also sometimes transferred to other Centres – those from Sudan and Chad go to Ejdabiya for repatriation purposes, while Somalis are usually transferred to Tripoli. 33 Only two anti-riot police officers were armed.
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
32
Hygiene materials are provided to migrants for cleaning themselves (soap and shampoo) and the premises every week. A water tanker is used to bring water supply to the Centre – it is of drinkable quality, but due to lack of appropriate treatment and storage facility in the Centre, it gets contaminated (salted).34 The kitchen complex has about 3‐4 rooms, including the main kitchen area (clean), cold storage, rest quarters for staff and bathrooms. Expired food products are placed in a separate area within the general storage room, separated from the provisions for daily cooking. There are separate quarters for staff, but no appropriate provisions like furniture and bedding are provided. Staff also has separate cooking provisions and kitchen. Given the large size of the premises, there are guards located at the four corners of the grounds – but they do not have appropriate watch stations or good chairs to adequately stay for long hours. Health‐care facilities for migrants Medical facilities are not available, therefore no medical examination is provided upon admission to the Centre.35 Sick migrants, as well as pregnant women are usually referred to the hospitals and transported in box cars, since no ambulance is available: the Centre maintains medical records and files of all detainees who have been transferred. There is no separate accommodation for sick persons. Health related concerns of staff Staff does not receive any special training on any health aspect. No special healthcare access or allowances for medical care are provided. Additional Remarks During the visit, it has been observed that detainees are allowed to move around freely within the Centre and in its grounds. The doors are unlocked – both on the rooms and on the main door of the halls. There are football goalposts in the grounds where migrants can play among themselves and/or with the guards. They freely step outside to sit, walk around, hang out clothes in the sun, etc. Detainees are also allowed to keep their mobile phones, if without cameras.
34 It is very difficult to dig and maintain water wells in this region. 35 Sometimes the Centre receives doctors from the hospital, e.g. two dermatologists recently visited the Centre for examinations.

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
33
The administration maintains separate records for each detainee – with their identification/registration, trying also to facilitate the issuance of travel documents by Embassies for repatriation purposes. Migrants’ personal belonging (such as mobile phones with camera) are stored in a locked safe. Also counterfeited money (Libyan dinars, USD) are kept. Director referred that external visitors are allowed from 8:00 a.m. to 1:00 p.m.
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
34
SECTION TWO
3.3 Interview with apprehended migrants (outcomes from the questionnaires administered in the seven Centres) This section presents the findings from the 116 questionnaires administered between May‐June 2010 in the premises of seven holding Centres by the trained field‐workers (see above, chapter 2). The interviews were conducted in the respect of the following guiding principles:
Confidentiality: A secluded room was requested for the interviews, and only the field workers and migrants were allowed to be present inside this room.
Informed based consent: At the beginning of each interview, the field‐worker read out the information sheet to the migrant (included with questionnaire at Annex 3), following which consent was obtained. Only those migrants who provided voluntary consent were invited to continue the interview.
Anonymity: Given the sensitive settings in which the study was conducted, no information concerning identification was obtained as part of the consent or interview process to ensure anonymity.
Data protection: Each interview lasted approximately 15‐20 minutes. After the conclusion of all the interviews in the seven Centres, the data was coded, entered and cleaned by IOM Tripoli, where it is filed in a confidential de‐identified manner.
Sample description The sample designed for the selection of migrants to be interviewed envisaged different criteria, including:
i) Informed based consent ii) Sample, ensuring, if possible, a threshold – set at 10% of respondents
out of the total population hosted in the centre iii) Gender balance, with a threshold set at 25% of women out of the total
number of interviewed migrants iv) Nationalities balance, ensuring, if possible, at least 20 different
nationalities v) Age balance
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
35
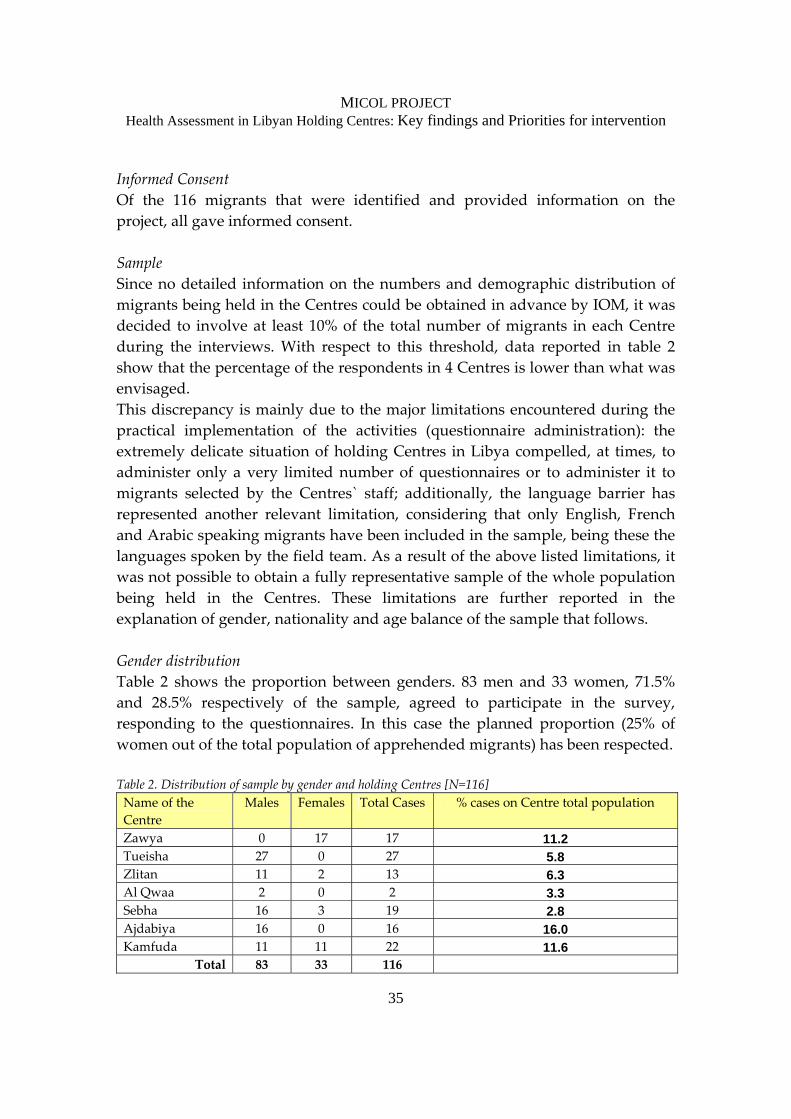
Informed Consent Of the 116 migrants that were identified and provided information on the project, all gave informed consent. Sample Since no detailed information on the numbers and demographic distribution of migrants being held in the Centres could be obtained in advance by IOM, it was decided to involve at least 10% of the total number of migrants in each Centre during the interviews. With respect to this threshold, data reported in table 2 show that the percentage of the respondents in 4 Centres is lower than what was envisaged. This discrepancy is mainly due to the major limitations encountered during the practical implementation of the activities (questionnaire administration): the extremely delicate situation of holding Centres in Libya compelled, at times, to administer only a very limited number of questionnaires or to administer it to migrants selected by the Centres` staff; additionally, the language barrier has represented another relevant limitation, considering that only English, French and Arabic speaking migrants have been included in the sample, being these the languages spoken by the field team. As a result of the above listed limitations, it was not possible to obtain a fully representative sample of the whole population being held in the Centres. These limitations are further reported in the explanation of gender, nationality and age balance of the sample that follows. Gender distribution Table 2 shows the proportion between genders. 83 men and 33 women, 71.5% and 28.5% respectively of the sample, agreed to participate in the survey, responding to the questionnaires. In this case the planned proportion (25% of women out of the total population of apprehended migrants) has been respected. Table 2. Distribution of sample by gender and holding Centres [N=116] Name of the Centre
Males Females Total Cases % cases on Centre total population
Zawya 0 17 17 11.2 Tueisha 27 0 27 5.8 Zlitan 11 2 13 6.3 Al Qwaa 2 0 2 3.3 Sebha 16 3 19 2.8 Ajdabiya 16 0 16 16.0 Kamfuda 11 11 22 11.6
Total 83 33 116
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
36
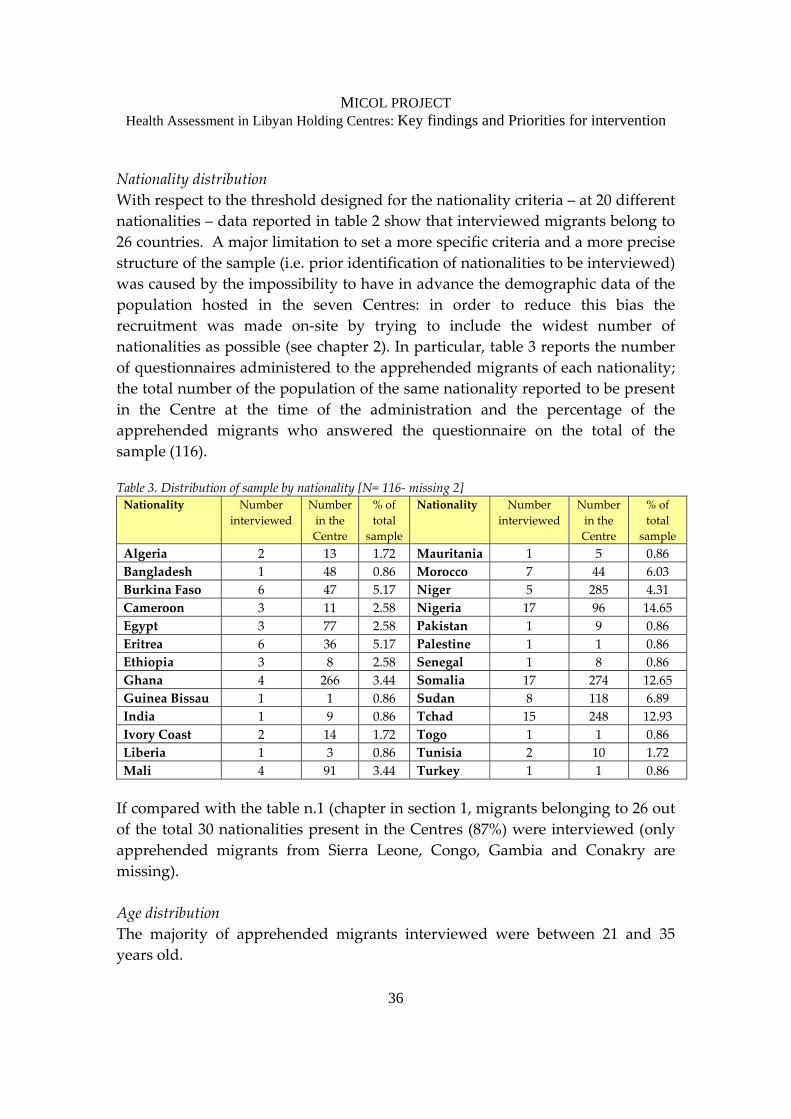
Nationality distribution With respect to the threshold designed for the nationality criteria – at 20 different nationalities – data reported in table 2 show that interviewed migrants belong to 26 countries. A major limitation to set a more specific criteria and a more precise structure of the sample (i.e. prior identification of nationalities to be interviewed) was caused by the impossibility to have in advance the demographic data of the population hosted in the seven Centres: in order to reduce this bias the recruitment was made on‐site by trying to include the widest number of nationalities as possible (see chapter 2). In particular, table 3 reports the number of questionnaires administered to the apprehended migrants of each nationality; the total number of the population of the same nationality reported to be present in the Centre at the time of the administration and the percentage of the apprehended migrants who answered the questionnaire on the total of the sample (116). Table 3. Distribution of sample by nationality [N= 116‐ missing 2] Nationality Number
interviewed Number in the Centre
% of total
sample
Nationality Numberinterviewed
Number in the Centre
% of total
sample Algeria 2 13 1.72 Mauritania 1 5 0.86 Bangladesh 1 48 0.86 Morocco 7 44 6.03 Burkina Faso 6 47 5.17 Niger 5 285 4.31 Cameroon 3 11 2.58 Nigeria 17 96 14.65 Egypt 3 77 2.58 Pakistan 1 9 0.86 Eritrea 6 36 5.17 Palestine 1 1 0.86 Ethiopia 3 8 2.58 Senegal 1 8 0.86 Ghana 4 266 3.44 Somalia 17 274 12.65 Guinea Bissau 1 1 0.86 Sudan 8 118 6.89 India 1 9 0.86 Tchad 15 248 12.93 Ivory Coast 2 14 1.72 Togo 1 1 0.86 Liberia 1 3 0.86 Tunisia 2 10 1.72 Mali 4 91 3.44 Turkey 1 1 0.86 If compared with the table n.1 (chapter in section 1, migrants belonging to 26 out of the total 30 nationalities present in the Centres (87%) were interviewed (only apprehended migrants from Sierra Leone, Congo, Gambia and Conakry are missing). Age distribution The majority of apprehended migrants interviewed were between 21 and 35 years old.
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
37
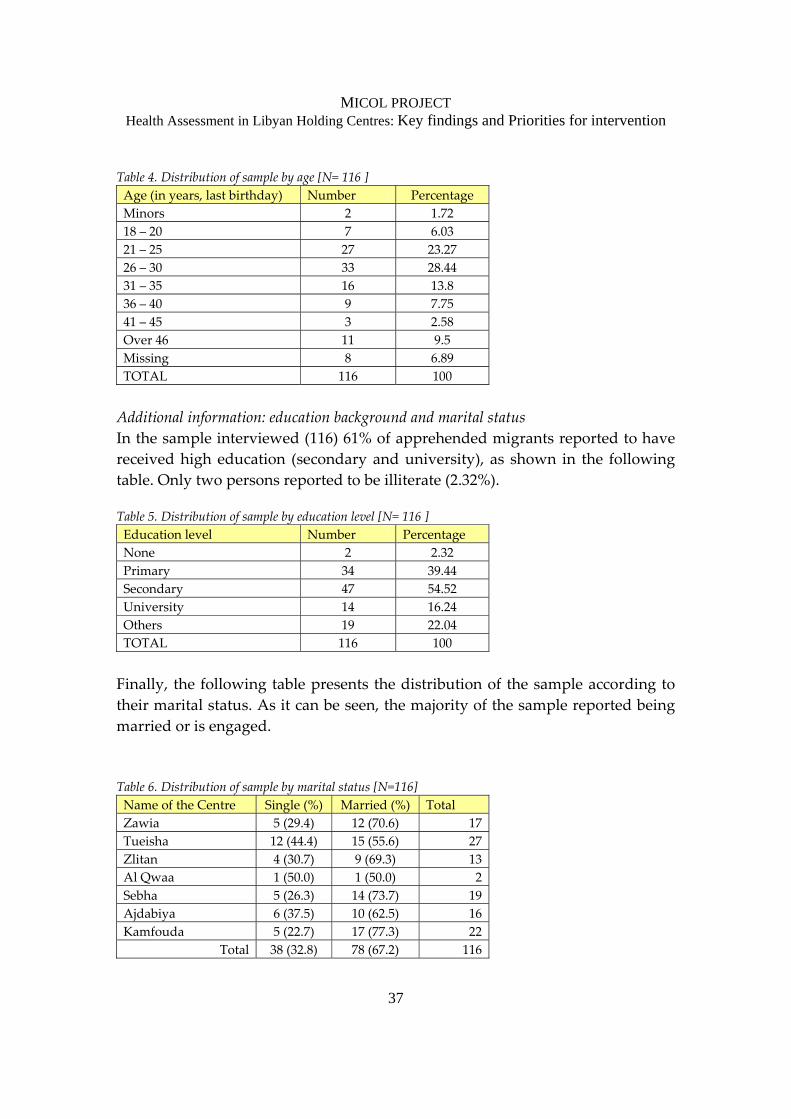
Table 4. Distribution of sample by age [N= 116 ] Age (in years, last birthday) Number Percentage Minors 2 1.72 18 – 20 7 6.03 21 – 25 27 23.2726 – 30 33 28.44 31 – 35 16 13.8 36 – 40 9 7.75 41 – 45 3 2.58 Over 46 11 9.5 Missing 8 6.89 TOTAL 116 100 Additional information: education background and marital status In the sample interviewed (116) 61% of apprehended migrants reported to have received high education (secondary and university), as shown in the following table. Only two persons reported to be illiterate (2.32%). Table 5. Distribution of sample by education level [N= 116 ] Education level Number Percentage None 2 2.32 Primary 34 39.44Secondary 47 54.52 University 14 16.24 Others 19 22.04 TOTAL 116 100 Finally, the following table presents the distribution of the sample according to their marital status. As it can be seen, the majority of the sample reported being married or is engaged. Table 6. Distribution of sample by marital status [N=116] Name of the Centre Single (%) Married (%) TotalZawia 5 (29.4) 12 (70.6) 17 Tueisha 12 (44.4) 15 (55.6) 27 Zlitan 4 (30.7) 9 (69.3) 13 Al Qwaa 1 (50.0) 1 (50.0) 2 Sebha 5 (26.3) 14 (73.7) 19Ajdabiya 6 (37.5) 10 (62.5) 16 Kamfouda 5 (22.7) 17 (77.3) 22
Total 38 (32.8) 78 (67.2) 116
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
38
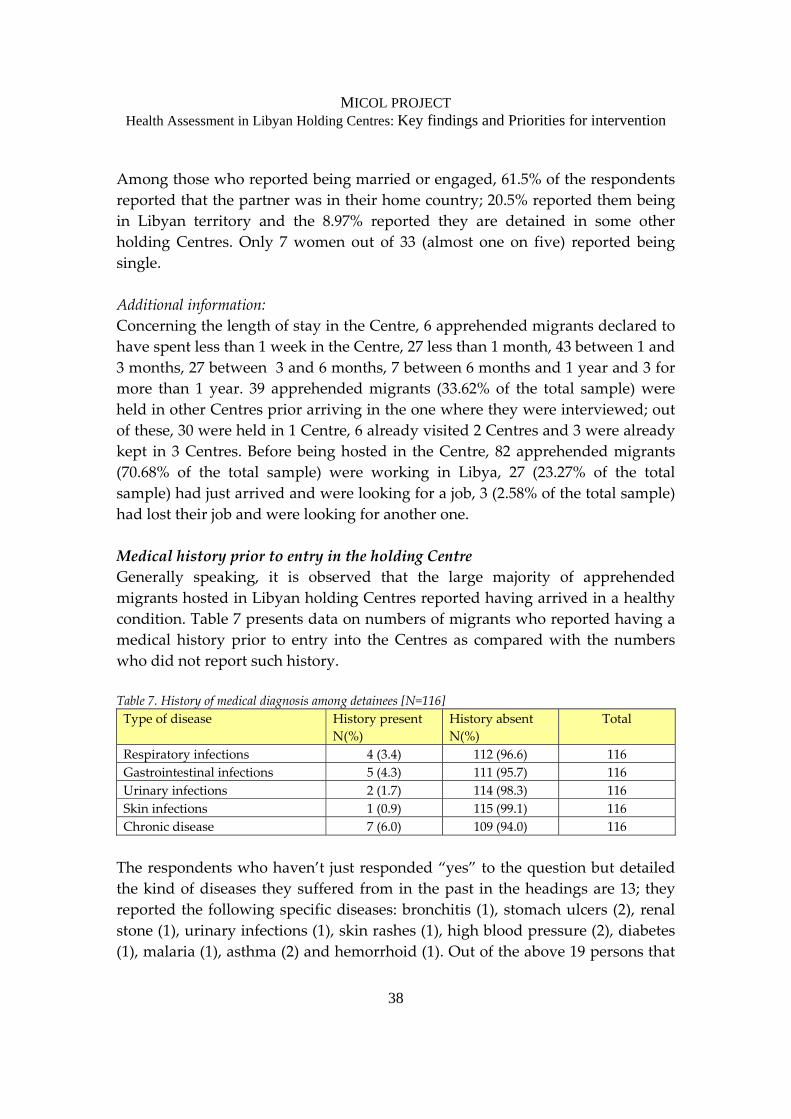
Among those who reported being married or engaged, 61.5% of the respondents reported that the partner was in their home country; 20.5% reported them being in Libyan territory and the 8.97% reported they are detained in some other holding Centres. Only 7 women out of 33 (almost one on five) reported being single. Additional information: Concerning the length of stay in the Centre, 6 apprehended migrants declared to have spent less than 1 week in the Centre, 27 less than 1 month, 43 between 1 and 3 months, 27 between 3 and 6 months, 7 between 6 months and 1 year and 3 for more than 1 year. 39 apprehended migrants (33.62% of the total sample) were held in other Centres prior arriving in the one where they were interviewed; out of these, 30 were held in 1 Centre, 6 already visited 2 Centres and 3 were already kept in 3 Centres. Before being hosted in the Centre, 82 apprehended migrants (70.68% of the total sample) were working in Libya, 27 (23.27% of the total sample) had just arrived and were looking for a job, 3 (2.58% of the total sample) had lost their job and were looking for another one. Medical history prior to entry in the holding Centre Generally speaking, it is observed that the large majority of apprehended migrants hosted in Libyan holding Centres reported having arrived in a healthy condition. Table 7 presents data on numbers of migrants who reported having a medical history prior to entry into the Centres as compared with the numbers who did not report such history. Table 7. History of medical diagnosis among detainees [N=116] Type of disease History present
N(%) History absent N(%)
Total
Respiratory infections 4 (3.4) 112 (96.6) 116 Gastrointestinal infections 5 (4.3) 111 (95.7) 116 Urinary infections 2 (1.7) 114 (98.3) 116 Skin infections 1 (0.9) 115 (99.1) 116 Chronic disease 7 (6.0) 109 (94.0) 116 The respondents who haven’t just responded “yes” to the question but detailed the kind of diseases they suffered from in the past in the headings are 13; they reported the following specific diseases: bronchitis (1), stomach ulcers (2), renal stone (1), urinary infections (1), skin rashes (1), high blood pressure (2), diabetes (1), malaria (1), asthma (2) and hemorrhoid (1). Out of the above 19 persons that
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
39
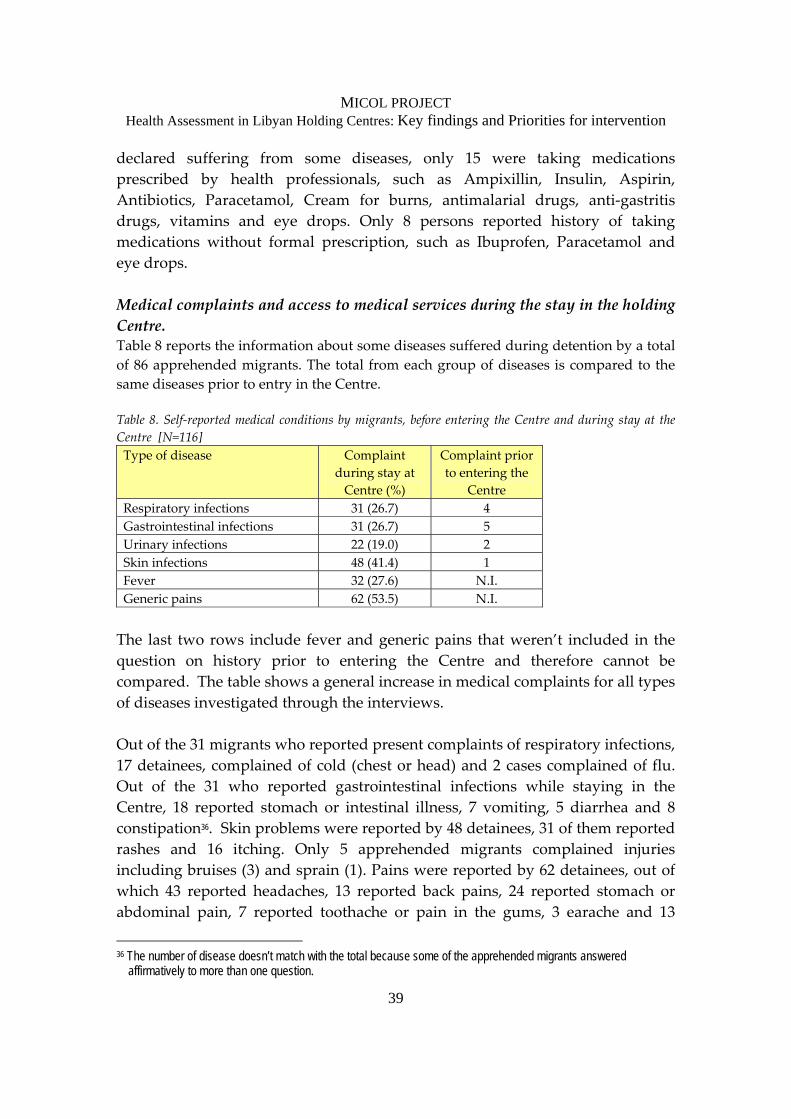
declared suffering from some diseases, only 15 were taking medications prescribed by health professionals, such as Ampixillin, Insulin, Aspirin, Antibiotics, Paracetamol, Cream for burns, antimalarial drugs, anti‐gastritis drugs, vitamins and eye drops. Only 8 persons reported history of taking medications without formal prescription, such as Ibuprofen, Paracetamol and eye drops. Medical complaints and access to medical services during the stay in the holding Centre. Table 8 reports the information about some diseases suffered during detention by a total of 86 apprehended migrants. The total from each group of diseases is compared to the same diseases prior to entry in the Centre. Table 8. Self‐reported medical conditions by migrants, before entering the Centre and during stay at the Centre [N=116] Type of disease Complaint
during stay at Centre (%)
Complaint prior to entering the
Centre Respiratory infections 31 (26.7) 4 Gastrointestinal infections 31 (26.7) 5 Urinary infections 22 (19.0) 2 Skin infections 48 (41.4) 1 Fever 32 (27.6) N.I. Generic pains 62 (53.5) N.I. The last two rows include fever and generic pains that weren’t included in the question on history prior to entering the Centre and therefore cannot be compared. The table shows a general increase in medical complaints for all types of diseases investigated through the interviews. Out of the 31 migrants who reported present complaints of respiratory infections, 17 detainees, complained of cold (chest or head) and 2 cases complained of flu. Out of the 31 who reported gastrointestinal infections while staying in the Centre, 18 reported stomach or intestinal illness, 7 vomiting, 5 diarrhea and 8 constipation36. Skin problems were reported by 48 detainees, 31 of them reported rashes and 16 itching. Only 5 apprehended migrants complained injuries including bruises (3) and sprain (1). Pains were reported by 62 detainees, out of which 43 reported headaches, 13 reported back pains, 24 reported stomach or abdominal pain, 7 reported toothache or pain in the gums, 3 earache and 13
36 The number of disease doesn’t match with the total because some of the apprehended migrants answered
affirmatively to more than one question.
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
40
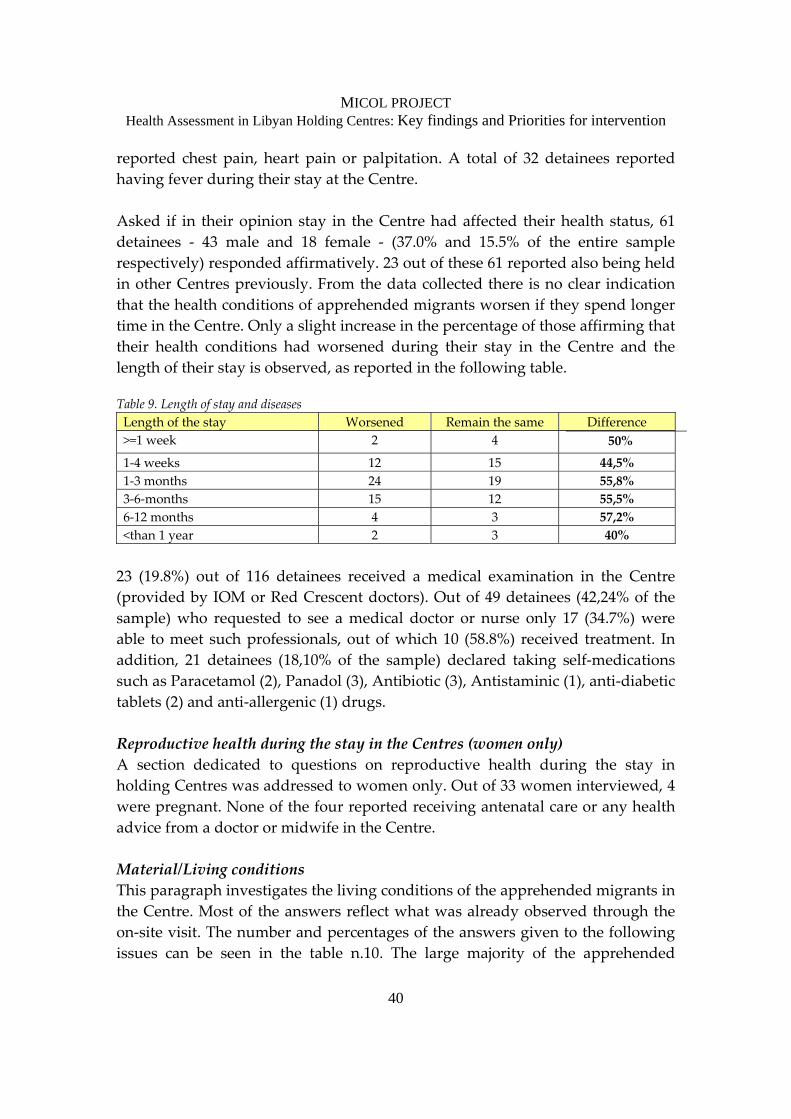
reported chest pain, heart pain or palpitation. A total of 32 detainees reported having fever during their stay at the Centre. Asked if in their opinion stay in the Centre had affected their health status, 61 detainees ‐ 43 male and 18 female ‐ (37.0% and 15.5% of the entire sample respectively) responded affirmatively. 23 out of these 61 reported also being held in other Centres previously. From the data collected there is no clear indication that the health conditions of apprehended migrants worsen if they spend longer time in the Centre. Only a slight increase in the percentage of those affirming that their health conditions had worsened during their stay in the Centre and the length of their stay is observed, as reported in the following table. Table 9. Length of stay and diseases Length of the stay Worsened Remain the same Difference >=1 week 2 4 50%
1‐4 weeks 12 15 44,5% 1‐3 months 24 19 55,8% 3‐6‐months 15 12 55,5% 6‐12 months 4 3 57,2% <than 1 year 2 3 40% 23 (19.8%) out of 116 detainees received a medical examination in the Centre (provided by IOM or Red Crescent doctors). Out of 49 detainees (42,24% of the sample) who requested to see a medical doctor or nurse only 17 (34.7%) were able to meet such professionals, out of which 10 (58.8%) received treatment. In addition, 21 detainees (18,10% of the sample) declared taking self‐medications such as Paracetamol (2), Panadol (3), Antibiotic (3), Antistaminic (1), anti‐diabetic tablets (2) and anti‐allergenic (1) drugs. Reproductive health during the stay in the Centres (women only) A section dedicated to questions on reproductive health during the stay in holding Centres was addressed to women only. Out of 33 women interviewed, 4 were pregnant. None of the four reported receiving antenatal care or any health advice from a doctor or midwife in the Centre. Material/Living conditions This paragraph investigates the living conditions of the apprehended migrants in the Centre. Most of the answers reflect what was already observed through the on‐site visit. The number and percentages of the answers given to the following issues can be seen in the table n.10. The large majority of the apprehended
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
41
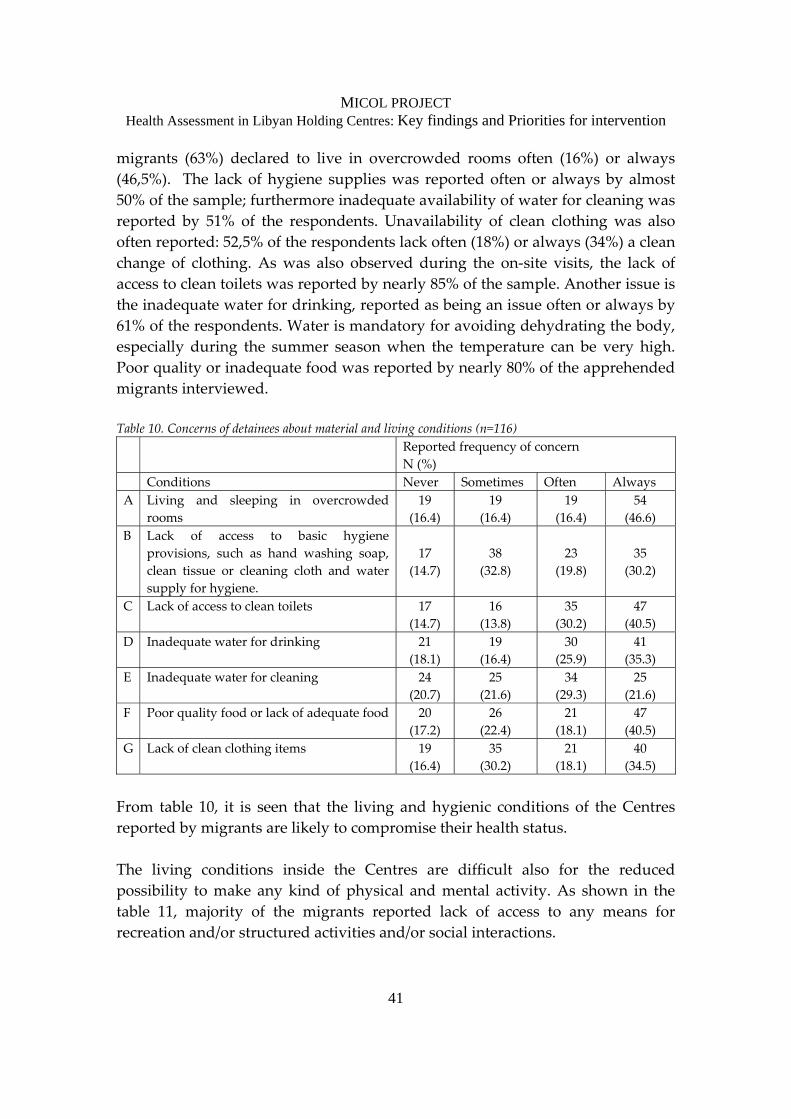
migrants (63%) declared to live in overcrowded rooms often (16%) or always (46,5%). The lack of hygiene supplies was reported often or always by almost 50% of the sample; furthermore inadequate availability of water for cleaning was reported by 51% of the respondents. Unavailability of clean clothing was also often reported: 52,5% of the respondents lack often (18%) or always (34%) a clean change of clothing. As was also observed during the on‐site visits, the lack of access to clean toilets was reported by nearly 85% of the sample. Another issue is the inadequate water for drinking, reported as being an issue often or always by 61% of the respondents. Water is mandatory for avoiding dehydrating the body, especially during the summer season when the temperature can be very high. Poor quality or inadequate food was reported by nearly 80% of the apprehended migrants interviewed. Table 10. Concerns of detainees about material and living conditions (n=116) Reported frequency of concern
N (%) Conditions Never Sometimes Often Always A Living and sleeping in overcrowded
rooms 19
(16.4) 19
(16.4) 19
(16.4) 54
(46.6) B Lack of access to basic hygiene
provisions, such as hand washing soap, clean tissue or cleaning cloth and water supply for hygiene.
17
(14.7)
38
(32.8)
23
(19.8)
35
(30.2)
C Lack of access to clean toilets 17 (14.7)
16 (13.8)
35 (30.2)
47 (40.5)
D Inadequate water for drinking 21 (18.1)
19 (16.4)
30 (25.9)
41 (35.3)
E Inadequate water for cleaning 24 (20.7)
25 (21.6)
34 (29.3)
25 (21.6)
F Poor quality food or lack of adequate food 20 (17.2)
26 (22.4)
21 (18.1)
47 (40.5)
G Lack of clean clothing items 19 (16.4)
35 (30.2)
21 (18.1)
40 (34.5)
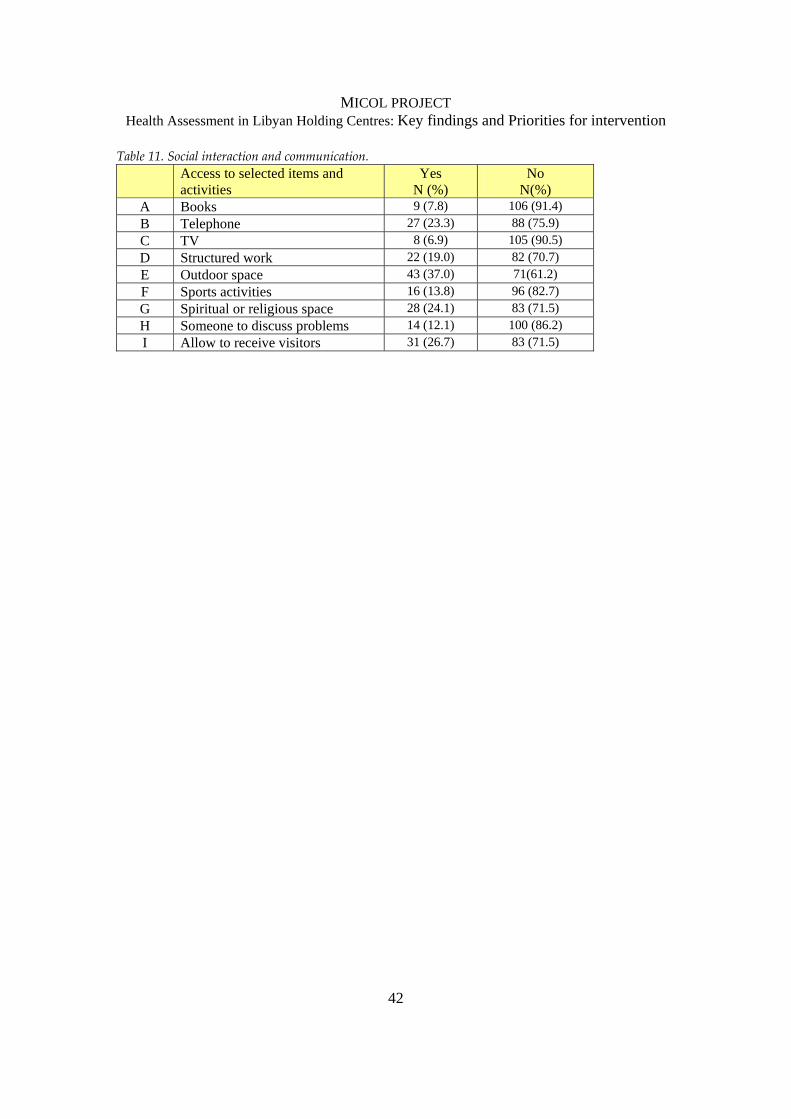
From table 10, it is seen that the living and hygienic conditions of the Centres reported by migrants are likely to compromise their health status. The living conditions inside the Centres are difficult also for the reduced possibility to make any kind of physical and mental activity. As shown in the table 11, majority of the migrants reported lack of access to any means for recreation and/or structured activities and/or social interactions.
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
42
Table 11. Social interaction and communication. Access to selected items and
activities Yes
N (%) No
N(%) A Books 9 (7.8) 106 (91.4) B Telephone 27 (23.3) 88 (75.9) C TV 8 (6.9) 105 (90.5) D Structured work 22 (19.0) 82 (70.7) E Outdoor space 43 (37.0) 71(61.2) F Sports activities 16 (13.8) 96 (82.7) G Spiritual or religious space 28 (24.1) 83 (71.5) H Someone to discuss problems 14 (12.1) 100 (86.2) I Allow to receive visitors 31 (26.7) 83 (71.5)
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
Prioritiesfor
Intervention

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
44
4.1 Priority interventions to improve Health and Living conditions in holding Centres 1. Overall management: Staff should be sensitized to the need for humane and
orderly management of persons being held in the Centres, and trained on issues related to irregular migration and public health in detention settings.
2. Physical infrastructure: Adequate ventilation (windows and fans), lighting and general cleanliness should be ensured in the premises of the holding Centres, including the rooms where migrants live and the staff offices and quarters. Sewage waters should be regularly cleaned up to prevent outbreak of diseases.
3. Living space: Under current conditions in the holding Centres, it is difficult to avoid overcrowding, which greatly restricts daily routine movements of the migrants, hinders maintenance of clean living quarters and increases risk of disease transmission, such as respiratory and skin infections. Better coordination should be established between the Libyan authorities for appropriate referral of apprehended migrants to the Centres in order to reduce or avoid overcrowded living conditions that directly impact health status of migrants.
4. Sleeping arrangement: All migrants should be provided with clean set of bedding and linens that should be cleaned regularly. Bedding and linens should be changed for sick persons, as needed. This is important to prevent incidence and transmission of contagious diseases, including skin infections like scabies.
5. Sanitary facilities: Sanitation and good hygiene practices are critical in the holding Centres to ensure both personal cleanliness of individual migrants and to maintain a hygienic physical environment in which large numbers of migrants often reside in close quarters. This is important for the Centres to prevent and control outbreaks of diseases such gastrointestinal infections that could potentially also impact Libyan staff working in the premises. Therefore, all migrants should have access to hygienic and private sanitary facilities. Running water should be regularly available for personal needs and to keep the facilities clean. Hygiene provisions should be provided to all migrants at a regular schedule or per needs. Cleaning supplies should be available to

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
45
maintain clean facilities. Special consideration should be made to the sanitary needs of women, especially during pregnancy and menstruation.
6. Food and drinking water: Food provisions should be available at all times at the Centres, and stored under appropriate conditions to avoid spoilage. This should be in proportion to the number of migrants being held at the Centre, to ensure that sufficient and unspoiled food is provided to all. Balanced nutrition‐based meals should be provided to all migrants at regular intervals on a daily basis with special consideration to the dietary needs of pregnant women, minors, elders and sick persons to avoid malnutrition. Clean (filtered or treated for pollutants) drinking water should be provided to all migrants – separate from the water in bathrooms. This is very important to prevent and control outbreaks of water‐borne infections and for the migrants to maintain adequate levels of hydration.
7. Clothing: All migrants should be provided with cleaning supplies and should be allowed to access cleaning areas with running water to wash and clean personal clothing items. This is especially important for sick persons. Persons without change of clothes should be provided fresh clothes. Cleanliness of the personal clothing items of each migrant will help to control spread of infections.
8. Daily routine and material conditions: All migrants should be allowed to access an outdoor space outside their living quarters on a daily basis. Structured voluntary activities should be available to migrants in the Centres (such as sports, participating in activities at the Centre). As the resources become available, migrants should be given access to materials such as books or television for recreation. This should be seen as a priority for the mental and psychological well‐being of the detained migrants, and will also facilitate management of the Centres.
4.2 Priority interventions to improve provision of healthcare services 1. Medical care: all Centres should establish a medical clinic on‐site where
doctors and/or nursing professionals can provide regular medical exams (including basic entry and departure exams). Basic medical exams upon entry

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
46
are important to identify and document any acute or chronic health condition that can influence the migrants’ stay within the Centres, as well as infectious diseases that could potentially pose a risk to other migrants and staff. Depending on resources, the clinics can be operated by healthcare staff from the Libyan government, or in collaboration with partners (international organizations, civil society). Minimum medical provisions for common diseases and emergency medical kits should be available in all Centres. Staff should be trained in providing emergency medical care. Often, staff working in the Centres have to provide such assistance at short notice, and they should be entitled to adequate training to deal with such situations. All Centres should have access to at least one ambulance that can be used when migrants are referred to medical clinics or hospitals, as well as during medical emergencies.
2. Disease prevention: Given the common overcrowded conditions in which the migrants are held, it is important to ensure timely medical care for persons with signs and symptoms of infectious diseases. Separate quarters should be available for the sick persons to rest and recuperate. Staff should also receive basic medical exams and vaccinations per the national recommendations.
3. Health education: Healthcare professionals should be made available at the Centres to provide health education on topics related to spread of infectious diseases, risky health behaviors, coping strategies in confinement, violence and injury prevention, among others.
4. Health regulations in holding Centres: In line with the WHO regulations, the GPC for Health should consider establishing regulations for documenting and reporting on infectious diseases and other conditions. Issues of confidentiality, documentation and sharing medical records should be dealt with uniformly across all Centres.
5. Health referral mechanisms: Effective and functional referral mechanisms between holding Centers and hospitals should be established for hospitalization and adequate treatment of severe cases requiring urgent medical attention.
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
Conclusions and
Way Forward
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
48
The assessment of the seven Centres, conducted within the framework of the MICOL project, identifies critical areas with respect to the health and hygienic conditions experienced by the all the characters (apprehended migrants, civil and security personnel) living in such premises. The holding Centres are refurbished commercial structures that do not fit with human life, the sanitary facilities – rooms, pipes, toilets – are often insufficient for hosting people in a dignified way and Directors have to deal with complex management issues with few resources and staff at disposal. The poor conditions observed and shared with the staff during the on‐site visit in the Centres can inevitably affect the physical and psychological health of the with‐held migrants, along with that of Libyan staff: ‐ Physical: the poor quality of the hygienic and health standards (i.e. the
insufficient quality of ventilation and water, both for cleaning and drinking, the use of unhygienic and shared bed linen and mats, as well as the lack of clean clothing) facilitates the proliferation and the transmission of bacteria and viruses that in the long run can result in severe pathologies
‐ Psychological: life in the holding Centres is monotonous and repetitive. The
detainees are lying in the rooms for long time, sometimes years in a serious cognitive and intellectual deprivation. The time spent in the holding Centre is lost and empty and it sums up the sense of waste, defeat and failure that is commonly perceived by the migrants when their migratory project ends. Apprehended migrants are blocked and frustrated, the wall is the fence and the only goal is to get out of there.
Through the survey important insights about health and hygiene in the Centre were gathered: the most serious diseases are those related to the skin, affecting approximately 50% of the detainees; the other group of diseases mostly pointed out by the apprehended migrants are what we referred to as “generic pains”: they are headache, toothache, earache, chest and heart pain and palpitation. In lower percentages, other diseases follow: respiratory and gastrointestinal infections, and urinary problems. Little percentage of the sample referred to physical injuries suffered in the premises. To avoid possible outbreak of inter‐ethnical violence among the detainees, the Directors of the Centres usually assign each migrant to a room, according to his/her nationality. On the one hand this is very effective, but on the other it turns out in the impossibility to rule the balance of the detainees in the rooms.
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
49
According to the nationalities present at a given time, rooms can be overcrowded or almost empty. And again this facilitates the spread of diseases. Despite the fact that these outcomes can’t be generalised to the whole population in the Centres and despite the serious limitations highlighted above (see previous chapter), data collected provide, indeed, an important feedback about the way to improve the premises` standards. Through a solid plan of action, the health and hygienic conditions could be dramatically improved. This sentence is corroborated by the availability (and sensibility) of the directors and staff in doing what is in their power for improving the living conditions of the migrants held in the Centres. Different problems depend by the lack of effective coordination among the different actors involved: for example four of the Centres visited have a clinic, but lack of coordination among authorities and relief agencies impairs their functioning. The consequences of providing used mats for sleeping to the detainees are well known; the problem is the lack of regular distribution from the central warehouses. The need of outdoor activities for the detainees is recognized; but due to the understaffing situation the security in the Centres cannot be guaranteed. These are only few examples, chosen among the amount of data gathered through the interviews, the on‐site observation and the analysis of the questionnaires. Empowerment of Libyan Security personnel with theoretical and practical skills concerning the migration phenomenon and health aspects, including disease prevention and emergency care could also play an important role: to this purpose specific training sessions should be carried out. Eventually, the way ahead should also lay its foundations on a strong involvement of Libyan Civil Society and International Organizations into the Centres, for issues other than security (i.e. medical, relief as well as social activities): such cooperation could positively improve the overall conditions into the holding premises, lowering, at the same time, the burden of responsibilities put on the Directors and its staff.

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
1) Map of Libyan Holding Centres 2) Request by GPC Health to IOM 3) Questionnaire and guidelines

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
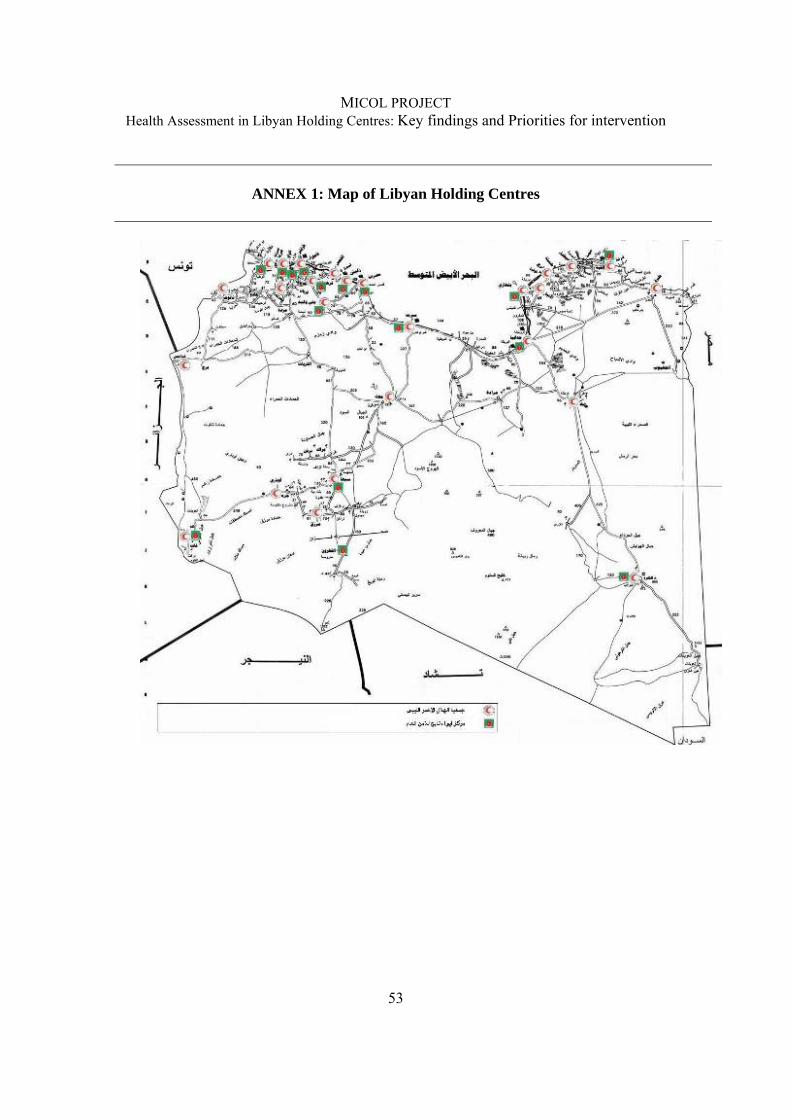
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
53
ANNEX 1: Map of Libyan Holding Centres
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
54
ANNEX 2: Request from GPC Health to IOM
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
55
ANNEX 3: Questionnaire and Guidelines
1035 Facility: "Project to Enhance Migrants' Conditions in Libyan Holding Centres (MICOL)” Questionnaire to assess migrants’ health status and living conditions in holding Centres
TO BE READ ALOUD BY INTERVIEWER Good morning/afternoon. My name is ___________________________ and I work for the International Organization for Migration (IOM). IOM is an intergovernmental agency committed to the principle that humane and orderly migration benefits migrants and society. The IOM office in Tripoli is currently conducting a research project titled ‘Project to enhance migrants’ conditions in Libyan holding Centres (MICOL)’. This study is being conducted to assess public health conditions in the holding Centres to plan future interventions to benefit migrants such as yourself.
You are invited to participate in an interview for this research study. This interview will require you to share information on your medical history, any current medical complaints and your opinions about living conditions in this Centre. Your decision to take part is entirely voluntary and you may refuse to take part, or choose to stop taking part, at any time. You may refuse to answer any one or more of the questions asked during the interview. Your decision whether or not to participate in this study will not affect your current or future stay at this Centre.
The interview will take about 30 minutes to finish. All interviews will be confidential and no personal identifier will be included on the interview form, so it is strictly anonymous. All responses will be kept strictly confidential. The interview form will only be handled by IOM’s research team and will not be shared with any other unauthorized persons. The information you provide will only be used for this study. You will not be personally identified in any reports or publications that may result from this study.
This study is expected to be beneficial to migrants like you, by reviewing health conditions in holding Centre settings. Findings from this study will be used to better understand the current situation and plan possible, future interventions for vulnerable migrants in immigration holding Centres. Your participation in this research is very important to us, so we hope you will consider taking part in this interview. You can ask any questions you may have about this study now. If you have decided to participate in this interview, please indicate with ‘YES’ on the Informed Consent Form, which means that you voluntarily agree to participate in this study.
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
56
INFORMED CONSENT FORM I HAVE BEEN INFORMED ABOUT THE IOM PROJECT “MICOL” AND UNDERSTAND ITS OBJECTIVES AND ACTIVITIES. Do you agree to VOLUNTARILY participate in this interview? [Please put a X against the appropriate answer] Yes No TO BE FILLED IN BY IOM TRIPOLI/Study team only: Interviewer Name: NAME OF DETENTION CENTRE: Date of Interview: Consent obtained: YES NO
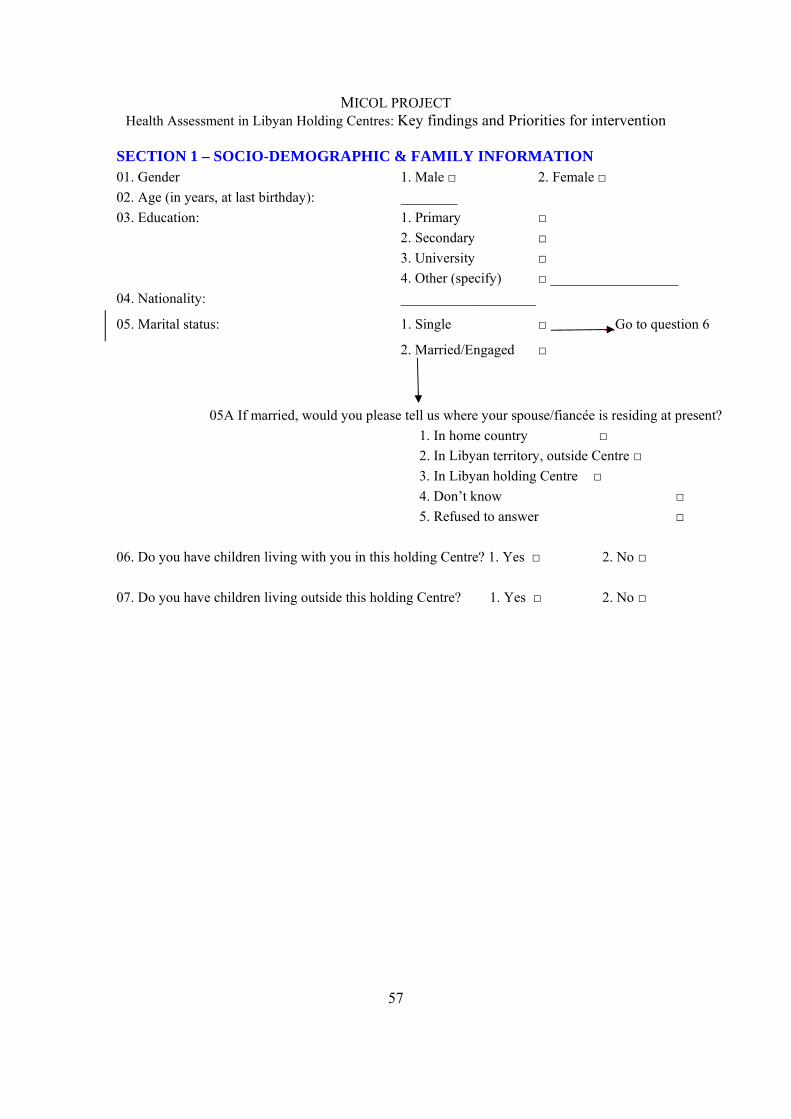
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
57
SECTION 1 – SOCIO-DEMOGRAPHIC & FAMILY INFORMATION 01. Gender 1. Male □ 2. Female □ 02. Age (in years, at last birthday): ________ 03. Education: 1. Primary □ 2. Secondary □ 3. University □ 4. Other (specify) □ __________________ 04. Nationality: ___________________
05. Marital status: 1. Single □ Go to question 6
2. Married/Engaged □
05A If married, would you please tell us where your spouse/fiancée is residing at present? 1. In home country □ 2. In Libyan territory, outside Centre □ 3. In Libyan holding Centre □ 4. Don’t know □ 5. Refused to answer □
06. Do you have children living with you in this holding Centre? 1. Yes □ 2. No □ 07. Do you have children living outside this holding Centre? 1. Yes □ 2. No □
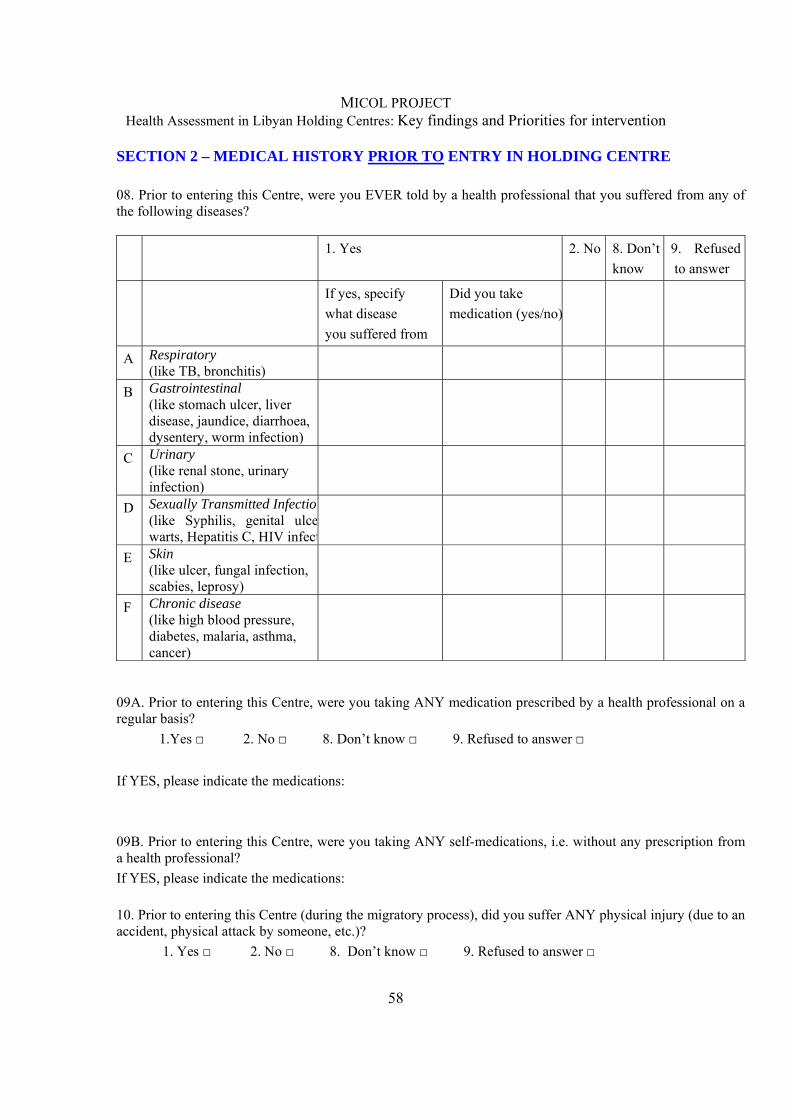
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
58
SECTION 2 – MEDICAL HISTORY PRIOR TO ENTRY IN HOLDING CENTRE 08. Prior to entering this Centre, were you EVER told by a health professional that you suffered from any of the following diseases? 1. Yes
2. No 8. Don’t
know 9. Refused to answer
If yes, specify what disease you suffered from
Did you take medication (yes/no)
A Respiratory (like TB, bronchitis)
B Gastrointestinal (like stomach ulcer, liver disease, jaundice, diarrhoea, dysentery, worm infection)
C Urinary (like renal stone, urinary infection)
D Sexually Transmitted Infection(like Syphilis, genital ulcewarts, Hepatitis C, HIV infect
E Skin (like ulcer, fungal infection, scabies, leprosy)
F Chronic disease (like high blood pressure, diabetes, malaria, asthma, cancer)
09A. Prior to entering this Centre, were you taking ANY medication prescribed by a health professional on a regular basis? 1.Yes □ 2. No □ 8. Don’t know □ 9. Refused to answer □ If YES, please indicate the medications: 09B. Prior to entering this Centre, were you taking ANY self-medications, i.e. without any prescription from a health professional? If YES, please indicate the medications: 10. Prior to entering this Centre (during the migratory process), did you suffer ANY physical injury (due to an accident, physical attack by someone, etc.)? 1. Yes □ 2. No □ 8. Don’t know □ 9. Refused to answer □
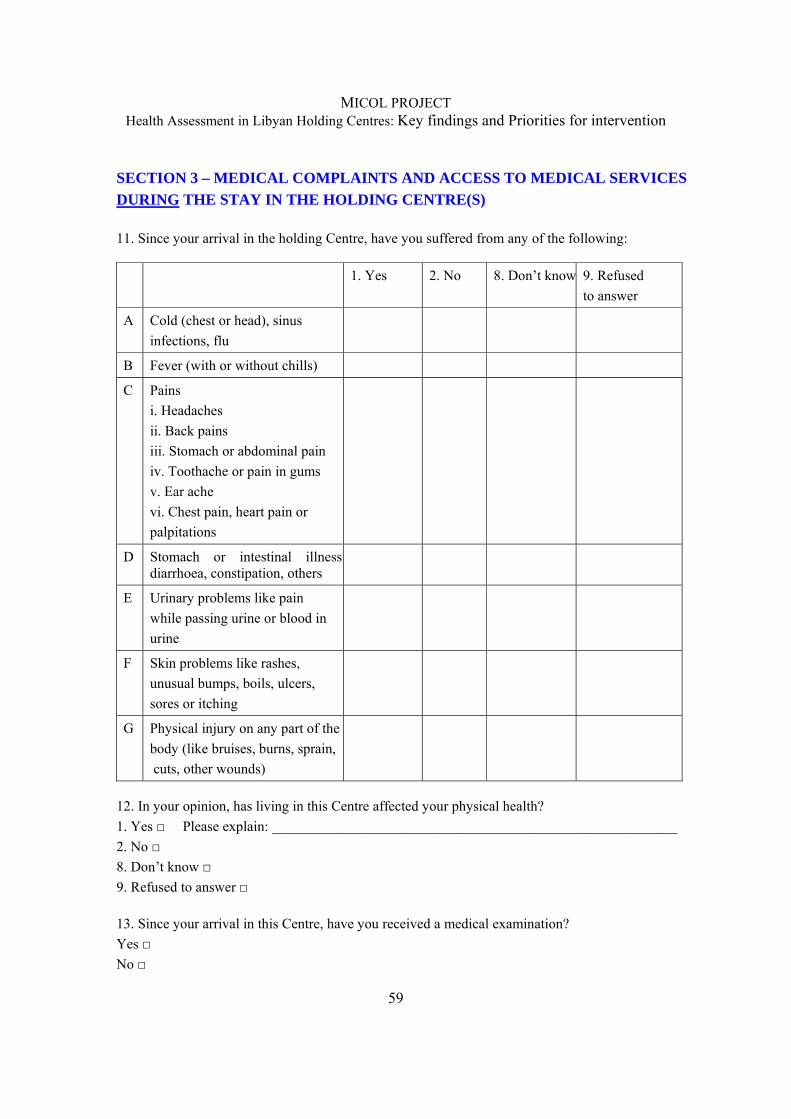
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
59
SECTION 3 – MEDICAL COMPLAINTS AND ACCESS TO MEDICAL SERVICES DURING THE STAY IN THE HOLDING CENTRE(S) 11. Since your arrival in the holding Centre, have you suffered from any of the following: 1. Yes
2. No 8. Don’t know 9. Refused
to answer
A Cold (chest or head), sinus infections, flu
B Fever (with or without chills)
C Pains i. Headaches ii. Back pains iii. Stomach or abdominal pain iv. Toothache or pain in gums v. Ear ache vi. Chest pain, heart pain or palpitations
D Stomach or intestinal illness diarrhoea, constipation, others
E Urinary problems like pain while passing urine or blood in urine
F Skin problems like rashes, unusual bumps, boils, ulcers, sores or itching
G Physical injury on any part of the body (like bruises, burns, sprain, cuts, other wounds)
12. In your opinion, has living in this Centre affected your physical health? 1. Yes □ Please explain: _________________________________________________________ 2. No □ 8. Don’t know □ 9. Refused to answer □ 13. Since your arrival in this Centre, have you received a medical examination? Yes □ No □
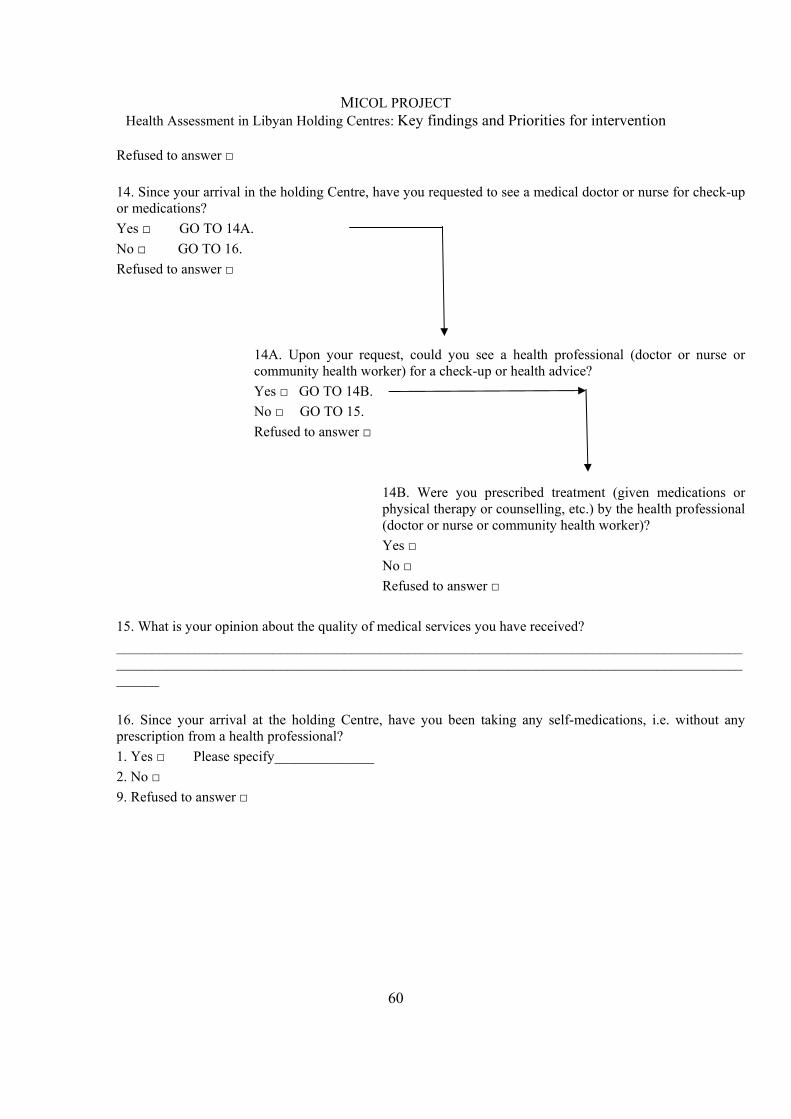
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
60
Refused to answer □ 14. Since your arrival in the holding Centre, have you requested to see a medical doctor or nurse for check-up or medications? Yes □ GO TO 14A. No □ GO TO 16. Refused to answer □
14A. Upon your request, could you see a health professional (doctor or nurse or community health worker) for a check-up or health advice? Yes □ GO TO 14B. No □ GO TO 15. Refused to answer □
14B. Were you prescribed treatment (given medications or physical therapy or counselling, etc.) by the health professional (doctor or nurse or community health worker)? Yes □ No □ Refused to answer □
15. What is your opinion about the quality of medical services you have received? ______________________________________________________________________________________________________________________________________________________________________________________ 16. Since your arrival at the holding Centre, have you been taking any self-medications, i.e. without any prescription from a health professional? 1. Yes □ Please specify______________ 2. No □ 9. Refused to answer □
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
61
SECTION 4 – REPRODUCTIVE HEALTH DURING THE STAY IN THE CENTRE(S) (WOMEN ONLY) (MEN GO STRAIGHT TO Q.18) 17. Are you currently pregnant? Yes □ GO TO 17A. No □ GO TO 18. Don’t know □ Refused to answer □
17A. Have you received antenatal care or any health advice from a doctor or nurse or midwife in this Centre for your pregnancy? Yes □ GO TO 17B. No □ GO TO 18. Refused to answer □
17B. Were you prescribed treatment (given medications or others) or any supplements (like iron and calcium) by the health professional (doctor or nurse or community health worker)? Yes □ No □ Refused to answer □
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
62
SECTION 5 – MATERIAL/LIVING CONDITIONS 18. Please tell us how frequently you experienced the following, since your arrival at this holding Centre Never = 0 Sometimes = 1 Often = 2 Always = 3 A Living and sleeping in
overcrowded rooms
B Lack of access to basic hygiene provisions, such as hand washing soap, clean tissue or cleaning cloth and water supply for hygiene.
C Lack of access to clean toilets D Inadequate water for drinking E Inadequate water for cleaning F Poor quality food or lack of
adequate food
G Lack of clean clothing items SECTION 6 - OPINIONS ON ACTIVITIES AND ROUTINE - SOCIAL INTERACTIONS 19. Do you have access to the following in this Centre? Yes = 1 No = 0 A Books B Telephone C TV D Structured work E Outdoor space F Sports activities G Spiritual or religious space H Someone to discuss problem I Allow to receive visitors
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
63
SECTION 7 - OPINIONS ON OVERALL EXPERIENCE IN CENTRE 20. In addition to the topics we discussed, do you have any special concerns or needs that you would like to share? ______________________________________________________________________________ SECTION 8 – STAY IN LIBYAN ARAB JAMAHIRIYA 21. When did you arrive in this Centre ________ (DD/MM/YYYY) 22. Prior to this Centre, were you held in other Centres? 1. Yes □ 2. No □ If yes, where? _________ 23. Before being detained in this Centre, what were you doing in Libya? 1. Working □ 2. Just arrived, looking for a job □ 3. Lost the job, looking for a NEW one □
4. In transit on the way to destination country □ 5. Other: _______________________________ TO BE READ ALOUD Thank you very much for participating in this interview.
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
64
Guidelines for the administration of the questionnaire The following guidelines are meant to facilitate the work of the interviewers tasked with the administration of this questionnaire to the detainees of the Libyan holding Centres. Avoiding any possible uncertainty in the administration increases the validity of the answers given to the questionnaire’s items. Presentation: It is important to provide to the interviewed persons, i.e. the migrants at the holding Centres, a clear picture of the aim of the survey they are asked to participate in. It is in this moment that the trust between interviewer and interviewed is built. Therefore, the information sheet provided for obtaining the consent from migrants should be read out clearly to them. It must be taken into consideration the particular psychological status that the apprehended migrants are experiencing: the more a person is institutionalized the lower is the consideration of their “self”. Usually this feeling leads to a state of frustration and depression that are counter-balanced by rage and anger. Furthermore, the opportunities to share their own concerns about the present and the future are very limited in a holding Centre, a place where the sense of solitude and isolation is naturally amplified. On the one hand, the detainees may be eager to talk with somebody who is not perceived as a threat and is perceived as someone who can be of some help. On the other hand, they may be very suspicious about the aims of the interviews, given that these will be held in the setting of the detention Centres. In order to deal with such difficult and sensitive issues, the interviewers are required to observe the following: - The questionnaire should be administered in a proper setting, such as a separate room where the migrants may be able to respond to the questionnaire in a private and confidential manner37. - The interviewer has the duty to answer all the questions coming from the interviewee,
provided they refer to the questionnaire itself. For example, if the interviewee does not understand a particular question or response option, this should be clearly explained to him/her. Other topics (i.e. “how long I’ll be here”; “Will they move me to another Centre”; “When I’ll be freed?” etc.) should be gently but firmly discarded by explaining that the interviewers are not linked with the Libyan institutions and therefore unable to provide any answer.
- Some time of “thinking-wandering” should be allowed to the interviewed. They should be gently carried back to the question by linking the topic the detainees are talking about to the investigated issue.
37 Talking about the health status force a person to stop and reflect about past, present and future experiences, along
with the associated risks, threats, hopes and including personal relationships such as friendships and love affairs, possibly opening a breach in their already fragile psychological status.
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
65
- The interviewer must respect the pace of the interviewed. For no reason the interviewer should put pressure to the interviewed for giving an answer to a question.
- The interviewed has the right not to answer to a question. The interviewers shouldn’t insist. Maybe at the end of the administration the interviewer can ask the interviewed if he/she is available in filling up the skipped questions. If the interviewed reaffirm his/her willingness of not responding to the question no other attempt should be made. This should simply be noted on the questionnaire.
The informed consent: The informed consent is very important and for no reasons should be considered as a mere bureaucratic act. It represents a sort of pact between the interviewer and the interviewee and it states the mutual collaboration between the two characters. The interviewees must be told that no personal identifiers are being collected, and that only IOM will have access to the information collected through the interviews. Filling in the Interview form: Most of the questions on the interview form are close-ended. The interviewers should read aloud each question to the subjects, followed by all the response options. Once the subject has selected their response option, please check the appropriate box against that response, like this: X. For questions with skip patterns, please note ‘Not applicable’ for those respondents who should not answer that question, and move on to the next applicable question. At the end of each interview, please check all the interview pages, to ensure that you have noted the answers to all questions that the subject responded to. SECTION 1 – SOCIO-DEMOGRAPHICAL & FAMILY INFORMATION Question n.1: The interviewer can check the right box directly the gender, no need of asking. Question n.2: Please report the age at the moment of the interviews. The last birthday is the reference even if the new one is two months ahead. In case the interviewed doesn’t remember or has no precise clue (in some countries the birth is not registered) the interviewer must specify, next to the answer that the reported age is not official. Question n.3: Here we want to know the highest completed education or schooling of the respondent. T response options are simple – primary/secondary/university - to hopefully cover the possible variability in the schooling patterns. The answer option “other” can be used to report other levels of schooling reported by respondents (e.g. college, vocational training, etc.) Question n.4: Here, we would like to inquire about the nationality or country of origin of the respondent. The purpose of asking this question is to make appropriate analysis of this information to understand if the respondent reports certain pathologies, diseases and illnesses that may be endemic in some countries. In case of concern expressed by the respondent, please
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
66
clarify to them that this is the only purpose for asking this question – there are no legal or other administrative reasons here. Question n.5: This question maybe sensitive for some respondents because it could easily remind the respondent about good or bad experiences shared with the spouse/partner with regard to the migratory experience and detention; understandably this could cause anxiety. The question has three specific response options, and also allows for the respondent to indicate ‘don’t know’ or ‘refuse to answer’. The question 5 has a stem question no. 5A that will only be asked to those who reply that they are ‘married/engaged’. The interviewer must carefully consider the feelings of the respondent and if needed, suspend the interview for a few minutes for the respondent to be able to continue further with the interview.
Question n.6; Question n.7. In these two questions, we would like to know if the respondent has any children that may be living in the holding Centre (qn.n.6) or outside the Centre (qn.n.7).
SECTION 2 – MEDICAL HISTORY PRIOR TO ENTRY IN THE HOLDING CENTRE
Question n.8. Please stress out that the questions in this section refer to the health status before entering the Libyan territory. No self diagnosis should be mentioned, only diseases certified by a professional. The interviewer should help the interviewed by investigating from the general to the particular, that is to say from the category of diseases (respiratory, sexually transmitted etc.) and then digging into it in order to get the exact pathology. Question n.9: 9A refers to medications prescribed by a professional. 9B refers to self medications. If the response to either of the two questions is Yes, then please note down the names of medications, if the respondent can provide. Question n.10: the question strives to get information about possible injuries that the respondent might have suffered from during the journey to Libya. Please note that we are interested in any physical injuries that the respondent suffered PRIOR to entering the detention Centre. The interviewer could be reluctant in answering them. Pls stress out that in any case the information given won’t be disclosed to Libyan authorities and affect the stay in the Centre and in general in Libya.
SECTION 3 – MEDICAL COMPLAINTS AND ACCESS TO MEDICAL SERVICES DURING THE STAY IN THE HOLDING CENTRE(S)
Question n.11: Here, we would like to inquire about the general medical complaints that the respondent may have experienced since their arrival in the holding Centre i.e. during the entire period in which they have been in the Centre. The interviewer should read out each of the symptom options from A) to G) and allow some time for the respondents to answer. For each

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
67
option, the respondent may choose to pick ‘don’t know’ or refuse to answer. For each option, the questionnaire gives some examples of conditions that will help the respondent in answering the question. Remember that this question will be answered based on the respondents’ complaints – we are NOT asking about whether these complaints were discussed with health professionals here. Question n.12: This question will allow us to obtain the respondent’s own opinion on whether living in the holding Centre has affected their health. If the response is YES, then please ask the respondent to explain ‘How’ in 1-2 sentences and note these down verbatim to the extent possible. Question n.13: Here we simply want to know whether or not the respondent had a medical examination since they started living in the holding Centre. The response options are close-ended – with Yes or No or refused. If the respondent says he/she never had a medical exam in the holding Centre, then check NO. If the respondent replies that he/she had one or more medical exams in the holding Centre, then check YES. Question n.14, 14A, 14B: This set of questions will give more information on the access of migrants in holding Centres to health services. First, you should ask the main question 14 to the respondent. Only if the reply is Yes to question 14, question 14A will be asked. If the reply to question 14 is No, then go straight to question 15 for that respondent and just write down ‘Not Applicable’ next to questions 14A and 14B. Similarly, if answer to question 14A is No, then continue to question 15 and write down ‘Not Applicable’ next to question 14B. Please review these instructions for the skip pattern very closely to avoid errors in entering the interview responses. Question n.15: This is an open-ended question. Read the question aloud and clearly to the respondent and explain that they should answer based on their own personal opinion. Write down the response verbatim, in 3-4 sentences, to the extent possible. If the respondent needs a few minutes to think over, please allow for such time and then again ask them the question. If the respondent chooses not to answer, please note ‘Refused to answer’ in the space provided and proceed to question 16. Question n.16: This question aims at investigating if the respondent took medications on his/her own initiative without a health professional’s prescription, during their stay in the holding Centre. This may include any types of medications, drugs, and also traditional medications (like homeopathic, etc.)
SECTION 4 – REPRODUCTIVE HEALTH DURING THE STAY IN THE CENTRE(S) (WOMEN ONLY) (MALE GO STRAIGHT TO Q.18)
MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
68
Question n.17: This set of questions is exclusively for Female respondents. For Males, skip this question, note ‘Not applicable’ on the form and go to Question 18. If the respondent replies that she is pregnant, then also ask Question 17A and B. If not pregnant, skip to question 18. Read the questions 17A and B very clearly to inquire about whether or not the pregnant respondent received antenatal care services and/or any related treatment. If the respondent proffers other concerns related to the pregnancy, please listen for a moment and tell them they can share such special concerns at the end of the interview in two open questions (21, 22)
SECTION 5 – MATERIAL/LIVING CONDITIONS
Question n.18: Through this question, we would like to obtain the opinions of the respondent on the material and living conditions in the Centre. Indeed, the study team will also be conducting an assessment through direct observation of these Centres, but it is also very important to obtain the respondent’s point of view in this regard. Please explain this to the respondents in case of queries. Also, it will be important to reiterate here that none of the respondents are being personally identified, thus their responses cannot, under any circumstances, be linked to them personally. Also, none of this information will be individually disclosed to any authorities. For each of the six items listed in the table in question 5, read each aloud to the respondent. Then tell them to pick from one of four options from 0 to 3, where 0=never; 1=sometimes; 2=often; 3=always. If need be, kindly allow the respondents to understand the response options and explain as needed.
SECTION 6 – OPINIONS ON ACTIVITIES AND ROUTINE
Question n.19 Here, we will obtain information on the access respondents in the holding Centre have, to certain basic items relevant to their daily routine in the Centres. For each of the nine items, they can pick either ‘yes’ or ‘no’ as an option.
SECTION 7 – OPINIONS ON OVERALL EXPERIENCE IN THE CENTRE
This section has one open-ended question. Since most of the interview uses close-ended questions where the response options are predetermined by the study team, this question will serve the purpose of allowing the respondents to provide some qualitative information. This will also let them express their priority concerns, which are not already covered in the previous closed questions. For this question, please allow the respondent 1-2 minutes to think about it, and then write down their response as verbatim as possible.
Question n.20. For this question, write down in 3-4 sentences any other special concerns or needs expressed by the respondent.
SECTION 8 - STAY IN LIBYAN ARAB JAMAHIRIYA

MICOL PROJECT Health Assessment in Libyan Holding Centres: Key findings and Priorities for intervention
69
Question n.21: Here, you should simply ask for the exact date of entry in the holding Centre. If the respondent doesn’t remember the precise date the interviewer must ask for an approx period of time (months, week etc.). Question n.22: Sometimes, individuals being held at the holding Centre, were previously also held at another Centre. Therefore, if the respondent replies with a ‘Yes’ please ask them where they were held before. If yes report the name or the place and in case they don’t remember well, ask for an approx indication of the geographical coordinates (south Libya, north Libya, close to the border, close to the sea etc.). If they cannot recall or refuse to specify, please do not insist. Simply write ‘refused to answer’ or ‘do not know’ in the space provided and move to the next question. Question n.23: Here, we would like to know what the respondent was doing last, before being brought to the holding Centre by the authorities. Therefore, please read each of the four options provided here, and check the appropriate one. If the respondent wishes to give another response, this can be noted under ‘Others’.





























