Embed Size (px)
Citation preview
Journal of Orthopuedic Research n357-364 The Journal of Bone and Joint Surgery, Inc. 0 1994 Orthopaedic Research Society
Healing of the Rabbit Medial Collateral Ligament Following an O’Donoghue Triad Injury:
Effects of Anterior Cruciate Ligament Reconstruction
Carolyn P. Engle, Masahiko Noguchi, Karen J. Ohland, Franz J. Shelley, and Savio L-Y. Woo
Musculoskeletal Research Center, Department of Orthopaedic Surgery, University of Pittsburgh, Pennsylvania, U.S.A.
Summary: The effects of healing time and anterior cruciate ligament reconstruction on healing of the medial collateral ligament and stability of the knee joint were evaluated in a rabbit model of an O’Donoghue triad injury (rupture of the medial collateral ligament with removal of the anterior cruciate ligament and part of the medial meniscus). At time 0 and at 6 and 12 weeks postoperatively, the anterior-posterior translation and varus-valgus rotation of the knee, the structural properties of the femur-medial collateral ligament-tibia complex, and the mechanical properties of the substance of the medial collateral ligament were evaluated. Although anterior-posterior translation increased significantly with time, we could not demonstrate a significant temporal effect on varus-valgus rotation. The uiti- mate load, elongation at failure, and energy absorbed to failure improved with time. In addition, with time, failure of the complex occurred more often in the ligament substance than at the osseous insertion. Because healing time did not affect the cross-sectional area or modulus of the medial collateral ligament, the improved structural properties of the complex resulted not from improvements in the mechanical properties of the tissue but rather from healing of the tibia1 insertion site. By 12 weeks, the reconstructed knees had only minor signs of osteoarthrosis on the tibiofemoral surfaces; this is in contrast to the findings in anterior cruciate ligament-deficient knees in our earlier study. Initially, re- construction also improved stability of the knee. Additionally, at 12 weeks, the stiffness of the complexes from the reconstructed group was 1.3 times that of the anterior cruciate ligament-deficient group (p < 0.05), and the ultimate load had increased by a factor of 1.6 (p < 0.05). Our findings demonstrate that reconstruction of the anterior cruciate ligament in the rabbit helps to stabilize the joint, improves healing of the medial collateral ligament, and may decrease the incidence of early-onset osteoarthrosis after an O’Donoghue triad injury.
Although O’Donoghue ( 1 3 ~ 4 ) advocated the sur- gical repair of all ruptured ligaments, investigators have more recently achieved good or excellent re- sults with nonoperative management of complete tears of the medial collateral ligament (MCL) in knees from both humans and animals (4-6,15,17). In
Received January 11,1993; accepted July 26,1993. Address correspondence and reprint requests to Dr. S. L-Y.
Woo at Department of Orthopaedic Surgery, University of Pittsburgh, 1011 Liliane S. Kaufmann Building, 3471 5th Ave- nue, Pittsburgh, PA 15213, U.S.A.
cases of more extensive injuries that involve multiple ligaments, however, optimal conditions for healing of the MCL are not yet known. The “triad” injury named by O’Donoghue involves tearing of the MCL, the anterior cruciate ligament (ACL), and the medial meniscus (13,14) and is known to result in a very unstable knee. Opinion varies regarding surgical in- tervention for an active individual with such an in- jury, and quantitative data demonstrating its success are lacking (3,4,8,9,16,18,21). Nevertheless, inves- tigators in our laboratory and others have shown that following such an injury an ACL-deficient knee
357
C. P. ENGLE E T AL. 358
is predisposed to early-onset osteoarthrosis (1,8,9). Previously, we examined the effects of time on
gross morphology, knee stability, and MCL healing following a triad injury without reconstruction of the ACL (1). We hypothesized that surgical reconstruc- tion of the ACL after a triad injury and increased healing time would reduce instability of the joint, improve healing of the MCL, and slow the progres- sion of osteoarthrosis in the knee. Therefore, we con- ducted a study to examine the effect of postoperative healing time on the gross morphologic findings, the measurement of knee instability, and the biomechan- ical properties of the healing MCL after a triad in- jury and reconstruction of the ACL. To evaluate the effects of surgical reconstruction of the ACL, the results of this study were compared with those of our previous study (1).
MATERIALS AND METHODS We used 21 skeletally mature male New Zealand
White rabbits (body mass 3.8 -f_ 0.1 kg). Preoper- atively, each animal received an intramuscular injec- tion of ketaminelacepromazine, as a pre-anesthetic, and an appropriate preoperative antimicrobial agent. After adequate general anesthesia, both of the hind- limbs were prepared and draped in the usual sterile manner.
To create the triad injury, the MCL of the left hindlimb was exposed through a medial incision and was undermined with a 2.5 mm-diameter rod. Two small cuts were made at the anterior and posterior edges of the MCL along the rod, and the rod was pulled medially to rupture the ligament. This method of rupture frays the MCL and simultaneously dam- ages the insertions to bone (17). Next, a lateral para- patellar arthrotomy was made, and the patella was dislocated medially. The ACL was transected sharply from its tibial insertion. A valgus stress then was applied to the knee while approximately 50% of the inner rim of the medial meniscus was excised through the defect created in the MCL.
The ACL was reconstructed first by blunt dissec- tion of the muscles of the anterior compartment from the tibia. With a 3 mm-diameter drill bit cen- tered over the original insertion of the ACL on the tibia, a tibial tunnel was drilled toward the anterolat- era1 tibial cortex. (The tunnel was drilled in this di- rection to protect the tibial insertion of the MCL.) A 2.0 Prolene suture (polypropylene; Ethicon, New Brunswick, NJ, U.S.A.) on a straight needle was se- cured to both ends of a graft (Dacron; Baxter Ed- wards, Costa Mesa, CA, U.S.A.) on a custom-made
femur
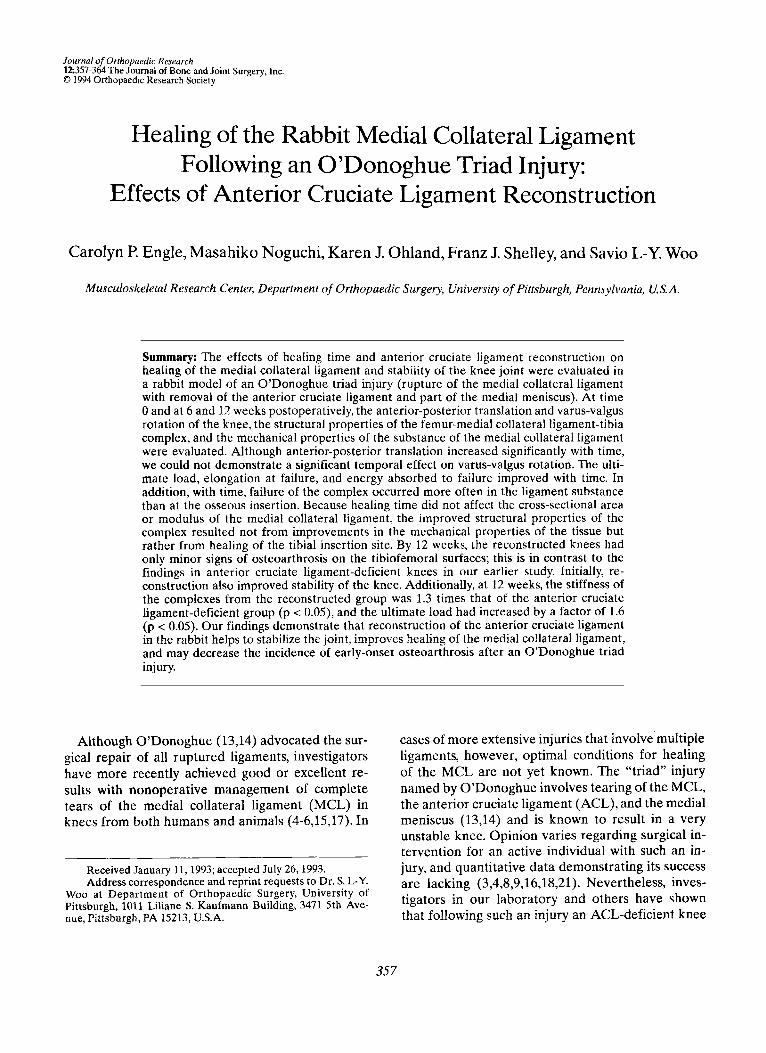
FIG. 1. Schematic representation of the “over-the-top’’ method for reconstruction of the anterior cruciate ligament (ACL) in the rabbit knee.
stainless-steel button for use as a graft-placement guide, A small curved hemostat was used for blunt dissection through the intercondylar notch and was directed laterally through a small arthrotomy. The graft then was guided through this area to simulate the “over-the-top’’ procedure (Fig. 1) (lOJ2). The graft was secured to the lateral femoral cortex with a screw and washer just proximal to the insertion of the lateral collateral ligament. The ends of the graft then were tied around the screw and knotted. The tension of the graft initially was adjusted with the knee joint in approximately 120” of flexion; final ad- justments were made by tightening of the screw af- ter the knee was extended to approximately 30” of flexion.
The ends of the knotted graft were fused with a sterile soldering gun. The restoration of anterior- posterior (A-P) stability and normal range of motion in the experimental knee were confirmed manually. The capsule and fascia were closed with interrupted 4.0 Prolene sutures. The subcutaneous tissue was ap- proximated with interrupted sutures of 4.0 Vicryl (polyglactin; Ethicon), and the skin was closed with the same type of suture, in a running subcuticular stitch.
In each rabbit, the right hindlimb served as a con- trol: a sham operation was done in which the MCL was exposed and undermined, a lateral parapatellar arthrotomy was created, and all incisions were closed as in the experimental limb.
Postoperatively, all animals were allowed unre-
J Orthop Re& Vol. 12, No. 3, 1994
HEALING OF RABBIT MEDIAL COLLATERAL LIGAMENT 359
stricted activity in a cage (size of the cage 4,000 cmz). Analgesics and antibiotics were administered twice a day for 3 days postoperatively or until they were no longer needed. Seven animals each were killed 6 and 12 weeks postoperatively for gross morphologic examination and biomechanical evaluation. Another group of seven was killed immediately before sur- gery; in this group (time 0), A-P translation and varus-valgus (V-V) rotation were measured preoper- atively in the intact limbs, again in the limbs after a triad injury was created, and a third time after the ACL had been reconstructed.
For morphologic and biomechanical evaluation, each hindlimb was disarticulated at the hip, wrapped in saline-soaked gauze, placed in an airtight bag, and stored at -20°C. Prior to testing, the specimens were thawed and all muscles were removed. With the periarticular connective tissues and the patella in- tact, the specimen was tested for A-P stability of the knee. The patella was removed, and V-V stability of the knee was measured. Then, all structures ex- cept the MCL were removed, which left only the
femur-MCL-tibia complex (FMTC), and the joint surfaces were examined for gross morphologic signs of osteoarthrosis.
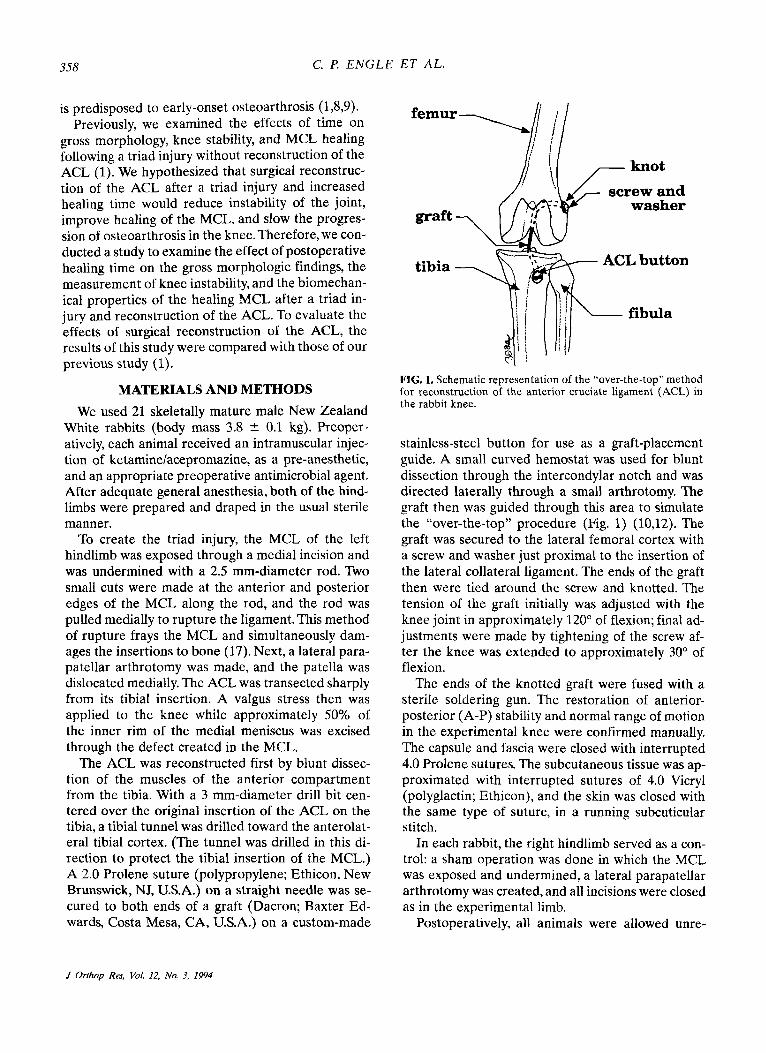
A-P translation of the knee was measured with a custom-built device with 4 degrees of freedom (Fig. 2). This device allowed A-P, medial-lateral, and proximal-distal translations as well as axial tibia1 ro- tation. With the knee held in 90" of flexion, a cyclic A-P load of k10 N was applied perpendicular to the long axis of the tibia, and the corresponding A-P translation was measured with a linear variable dif- ferential transformer. The limits for applied A-P load were scaled down from those recommended for A-P translation in humans (10). The scaling was based on the allometric relationship between body size and tensile strength of the mammalian ACL (2).
V-V rotation of the knee was measured by a de- vice described previously (17). With the knee in 90" of flexion, a bending moment of ? lo N-mm was applied to the knee. Care was taken to ensure that the longitudinal axis of the MCL was perpendicu- lar to the applied bending moment. When V-V mo-
medial-lateral translation
proximal-distal translation
L--- tibia
measures anterior-Posterior
translation anterior-posterior
FIG. 2. Experimental apparatus used to measure anterior-posterior translation of the knee. LVDT = linear 7
transformer. Iariable differential
J Orthop Res, Vol. 12, No. 3, 1994
360 C. l? E N G L E ET AL.
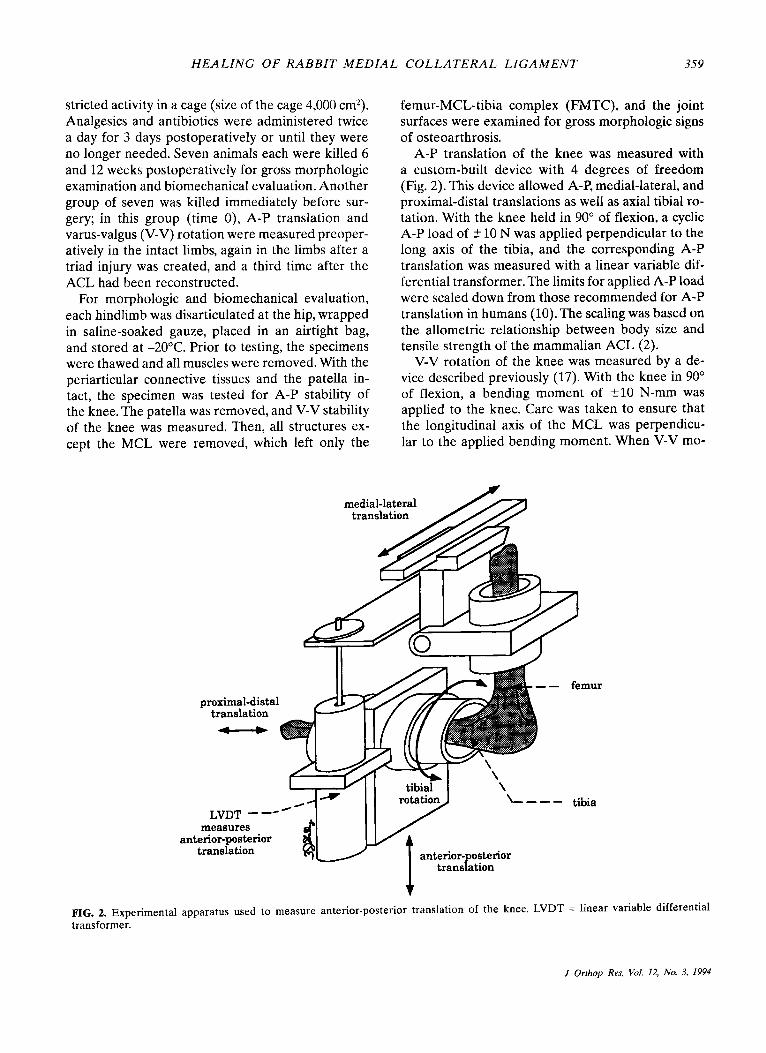
FIG. 3. Anterior-posterior (A-P) translation of the anterior cruciate ligament (ACL)-reconstructed knees for time 0 and 6 and 12 weeks postoperatively, expressed as a ratio of experimental to control (EIC) values. For comparison, the values for the ACL-deficient knees at time 0 are shown.
tion is limited to 3 degrees of freedom (V-V rota- tion and medial-lateral and proximal-distal transla- tions), the MCL is the primary restraint to valgus rotation (7).
After V-V rotation had been determined, all struc- tures except the MCL were resected, which left the FMTC. The MCL was finely dissected, and a laser micrometer system was used to measure the cross- sectional area of the MCL at the joint line, 3 mm proximal to the joint line, and 3 mrn distal to the joint line. Use of the laser micrometer is a noncontact method for measurement of the cross-sectional area and the shape of soft tissues (20) and has proved to be accurate to within 0.1 mm2.
Next, the FMTC was mounted in specially de- signed clamps, immersed in a saline bath (37"C), and placed in a materials testing machine (model 4502; Instron, Canton, MA, U.S.A.) with the long axis of the MCL aligned with the axis of the machine. Each specimen was preconditioned by cycling between 0 and 1 mm for 10 cycles and then was loaded to failure at a rate of 10 mm/min. All tests were videotaped, and the load-elongation curves, representing the structural properties of the FMTC, were recorded (19). The mode of failure also was noted. For meas- urements of strain, two dye lines were placed on the midsubstance of the MCL, approximately 1 cm apart and centered about the joint line, to serve as gauge- length markers. The increase in gauge length during testing was recorded on videotape, and the ligament
strain was determined by means of a video dimen- sion analyzer system (19).
The following structural properties were obtained from the load-elongation curves: stiffness (slope of the load-elongation curve measured between 1 and 3 mm of elongation), ultimate load, elongation at failure, and energy absorbed to failure (area under the curve). To calculate stress for the substance of the MCL, load was divided by the cross-sectional area, and strain was determined with the video di- mension analyzer system. The mechanical proper- ties obtained from the stress-strain curves included the modulus (slope of the curve between 3 and 5% strain). For each specimen that failed in the midsub- stance, the tensile strength (ultimate tensile stress) and strain at failure also were obtained.
Paired Student's t tests were used to compare the results for the experimental and control limbs. A one- way analysis of variance (ANOVA) was used to as- sess the effect of healing time on A-P translation of the knee. Two-way ANOVAs were used to assess the effect of treatment regimen (reconstruction of the ACL and no reconstruction of the ACL) and healing time (6 and 12 weeks) on V-V rotation and the struc- tural and mechanical properties of the MCL. The sig- nificance for all tests was set at p < 0.05.
RESULTS After the triad injury, osteoarthrotic changes were
not seen grossly on the weight-bearing surfaces of the
J Orthop Res, Vol. 12, No. 3, 1994
HEALING OF RABBIT M E D l A L COLLATERAL LIGAMENT 361
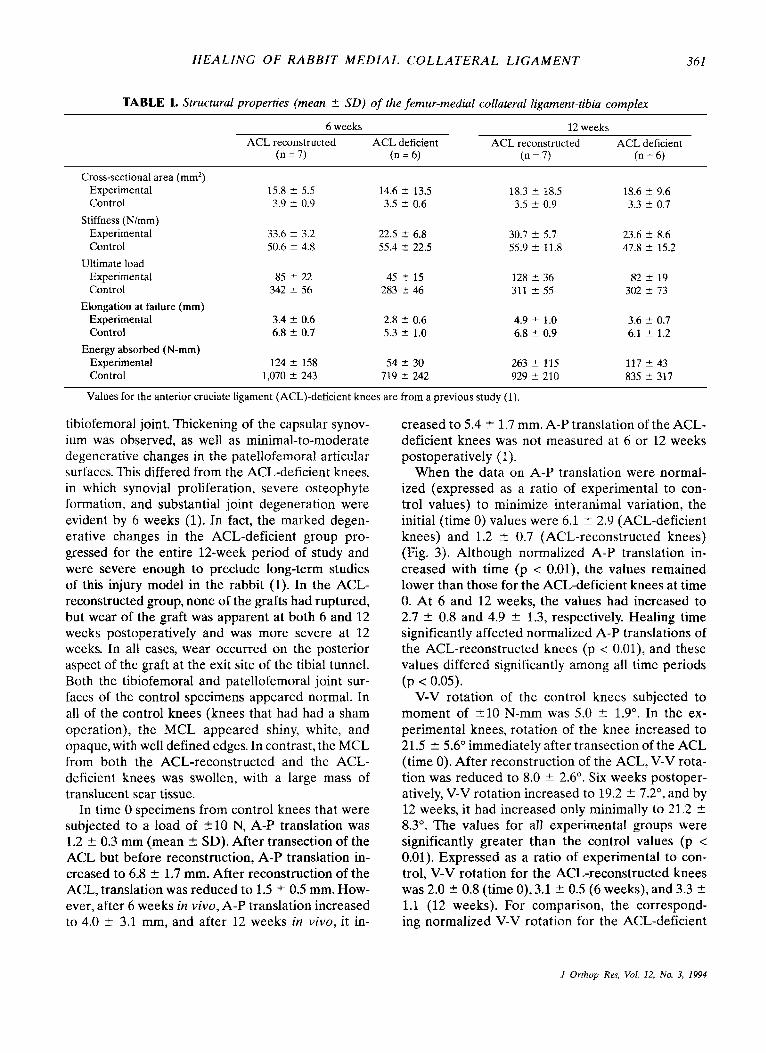
TABLE 1. Structural properties (mean ? SD) of the femur-medial collateral ligament-tibia complex
6 weeks 12 weeks ACL reconstructed ACL deficient ACL reconstructed ACL deficient
(n = 7) (n = 6) (n = 7) (n = 6)
Cross-sectional area (mm') Experimental Control
Stiffness (N/mm) Experimental Control
Experimental Control
Experimental Control
Experimental Control
Ultimate load
Elongation at failure (mm)
Energy absorbed (N-mm)
15.8 f 5.5 3.9 5 0.9
33.6 ? 3.2 50.6 f 4.8
85 ? 22 342 2 56
3.4 ? 0.6 6.8 -C 0.7
124 2 158 1,070 2 243
14.6 t 13.5 3.5 5 0.6
22.5 5 6.8 55.4 f 22.5
45 f 15 283 2 46
2.8 2 0.6 5.3 ? 1.0
54 2 30 719 2 242
18.3 t 18.5 3.5 2 0.9
30.7 i 5.7 55.9 f 11.8
128 i 36 311 2 55
4.9 2 1.0 6.8 ir 0.9
263 + 115 929 -+ 210
18.6 ? 9.6 3.3 2 0.7
23.6 i 8.6 47.8 ir 15.2
82 f 19 302 5 73
3.6 f 0.7 6.1 2 1.2
117 2 43 835 ir 317
Values for the anterior cruciate ligament (ACL)-deficient knees are from a previous study (1).
tibiofemoral joint. Thickening of the capsular synov- ium was observed, as well as minimal-to-moderate degenerative changes in the patellofemoral articular surfaces. This differed from the ACL-deficient knees, in which synovial proliferation, severe osteophyte formation, and substantial joint degeneration were evident by 6 weeks (1). In fact, the marked degen- erative changes in the ACL-deficient group pro- gressed for the entire 12-week period of study and were severe enough to preclude long-term studies of this injury model in the rabbit (1). In the ACL- reconstructed group, none of the grafts had ruptured, but wear of the graft was apparent at both 6 and 12 weeks postoperatively and was more severe at 12 weeks. In all cases, wear occurred on the posterior aspect of the graft at the exit site of the tibia1 tunnel. Both the tibiofemoral and patellofemoral joint sur- faces of the control specimens appeared normal. In all of the control knees (knees that had had a sham operation), the MCL appeared shiny, white, and opaque, with well defined edges. In contrast, the MCL from both the ACL-reconstructed and the ACL- deficient knees was swollen, with a large mass of translucent scar tissue.
In time 0 specimens from control knees that were subjected to a load of 210 N, A-P translation was 1.2 k 0.3 mm (mean 2 SD). After transection of the ACL but before reconstruction, A-P translation in- creased to 6.8 ? 1.7 mm. After reconstruction of the ACL, translation was reduced to 1.5 ? 0.5 mm. How- ever, after 6 weeks in vivo, A-P translation increased to 4.0 f 3.1 mm, and after 12 weeks in vivo, it in-
creased to 5.4 ? 1.7 mm. A-P translation of the ACL- deficient knees was not measured at 6 or 12 weeks postoperatively (1).
When the data on A-P translation were normal- ized (expressed as a ratio of experimental to con- trol values) to minimize interanimal variation, the initial (time 0) values were 6.1 -C 2.9 (ACL-deficient knees) and 1.2 t 0.7 (ACL-reconstructed knees) (Fig. 3). Although normalized A-P translation in- creased with time (p < 0.01), the values remained lower than those for the ACL-deficient knees at time 0. At 6 and 12 weeks, the values had increased to 2.7 ? 0.8 and 4.9 2 1.3, respectively. Healing time significantly affected normalized A-P translations of the ACL-reconstructed knees (p < 0.01), and these values differed significantly among all time periods (p < 0.05).
V-V rotation of the control knees subjected to moment of 210 N-mm was 5.0 -C 1.9". In the ex- perimental knees, rotation of the knee increased to 21.5 ? 5.6" immediately after transection of the ACL (time 0). After reconstruction of the ACL, V-V rota- tion was reduced to 8.0 2 2.6". Six weeks postoper- atively, V-V rotation increased to 19.2 f 7.2", and by 12 weeks, it had increased only minimally to 21.2 k 8.3". The values for all experimental groups were significantly greater than the control values (p < 0.01). Expressed as a ratio of experimental to con- trol, V-V rotation for the ACL-reconstructed knees was 2.0 2 0.8 (time 0),3.1 2 0.5 (6 weeks), and 3.3 ? 1.1 (12 weeks). For comparison, the correspond- ing normalized V-V rotation for the ACL-deficient
.I Orthop Res, Vol. 12, No. 3, 1994
362 C. €! ENGLE ET AL.
knees was 5.2 -t 1.0,5.0 5 1.7, and 4.7 ? 3.0 (1). A two-way ANOVA examining the effects of ACL reconstruction and time on normalized V-V rota- tion revealed a significant difference between treat- ment groups (p < 0.05) but no effect of time (p > 0.3). No significant interaction was found between these main variables (p > 0.3).
There were no significant effects of either re- construction of the ACL (p > 0.2) or healing time (p > 0.8) on the cross-sectional areas of the healed MCLs, and no significant interaction between these two variables could be detected (p > 0.5). The cross- sectional area was 4.0 and 5.2 times greater in the ACL-reconstructed specimens than in the control specimens at 6 and 12 weeks, respectively (Table 1). The trends were similar in the ACL-deficient speci- mens: the areas were 4.2 and 5.6 times greater than the control specimens at 6 and 12 weeks (1). The difference between the areas of the MCL in all of the experimental knees and the areas in the control knees was significantly different at both 6 and 12 weeks (p < 0.001).
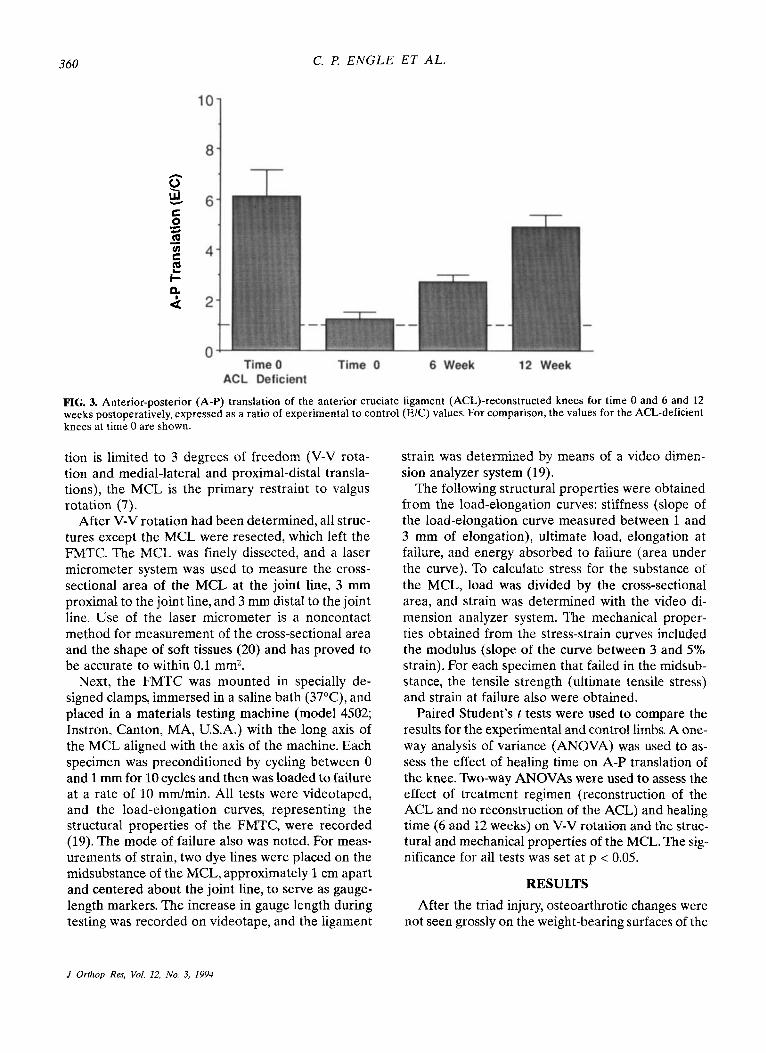
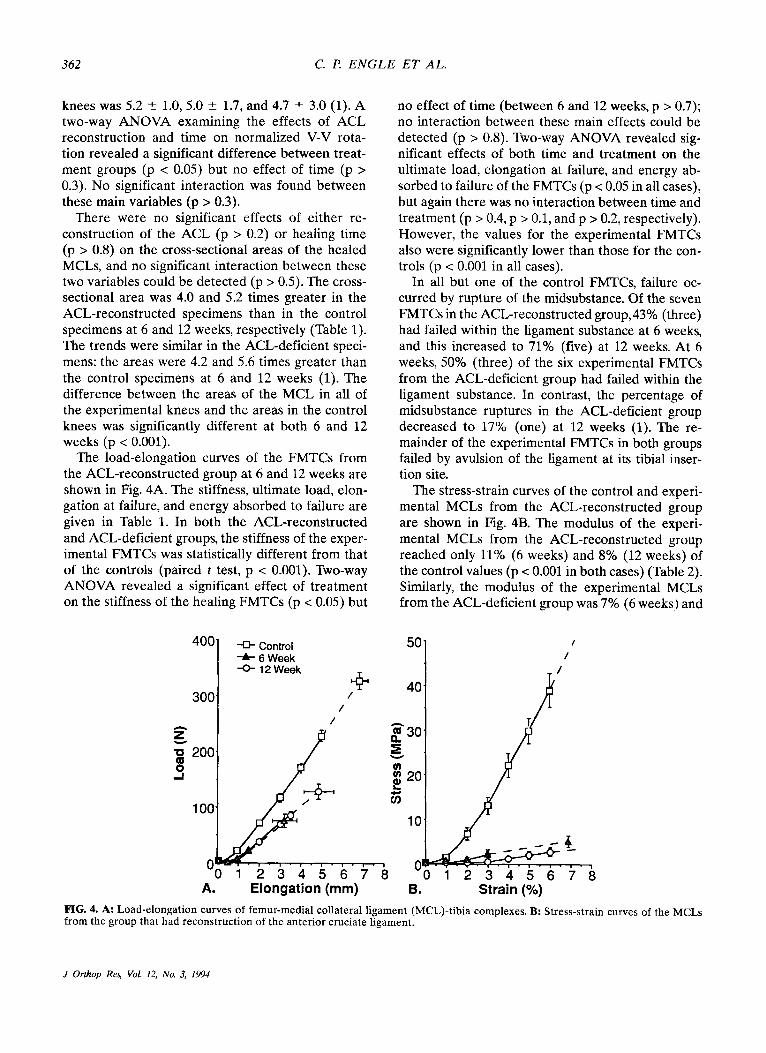
The load-elongation curves of the FMTCs from the ACL-reconstructed group at 6 and 12 weeks are shown in Fig. 4A. The stiffness, ultimate load, elon- gation at failure, and energy absorbed to failure are given in Table 1. In both the ACL-reconstructed and ACL-deficient groups, the stiffness of the exper- imental FMTCs was statistically different from that of the controls (paired t test, p < 0.001). Two-way ANOVA revealed a significant effect of treatment on the stiffness of the healing FMTCs (p < 0.05) but
no effect of time (between 6 and 12 weeks, p > 0.7); no interaction between these main effects could be detected (p > 0.8). Two-way ANOVA revealed sig- nificant effects of both time and treatment on the ultimate load, elongation at failure, and energy ab- sorbed to failure of the FMTCs (p < 0.05 in all cases), but again there was no interaction between time and treatment (p > 0.4, p > 0.1, and p > 0.2, respectively). However, the values for the experimental FMTCs also were significantly lower than those for the con- trols (p < 0.001 in all cases).
In all but one of the control FMTCs, failure oc- curred by rupture of the midsubstance. Of the seven FMTCs in the ACL-reconstructed group, 43% (three) had failed within the ligament substance at 6 weeks, and this increased to 71% (five) at 12 weeks. At 6 weeks, 50% (three) of the six experimental FMTCs from the ACL-deficient group had failed within the ligament substance. In contrast, the percentage of midsubstance ruptures in the ACL-deficient group decreased to 17% (one) at 12 weeks (1). The re- mainder of the experimental FMTCs in both groups failed by avulsion of the ligament at its tibia1 inser- tion site.
The stress-strain curves of the control and experi- mental MCLs from the ACL-reconstructed group are shown in Fig. 4B. The modulus of the experi- mental MCLs from the ACL-reconstructed group reached only 11% (6 weeks) and 8% (12 weeks) of the control values (p < 0.001 in both cases) (Table 2). Similarly, the modulus of the experimental MCLs from the ACL-deficient group was 7% (6 weeks) and
P - Q 30 n E
g 20 G
Y
v)
L
10
' 0 1 2 3 4 5 6 7 8 A. Elongation (mm) B. Strain (%)
FIG. 4. A: Load-elongation curves of femur-medial collateral ligament (MCL)-tibia complexes. B: Stress-strain curves of the MCLs from the group that had reconstruction of the anterior cruciate ligament.
J Orthop Res, Vol. 12, No. 3, 1994
HEALING OF RABBIT MEDIAL COLLATERAL LIGAMENT 363
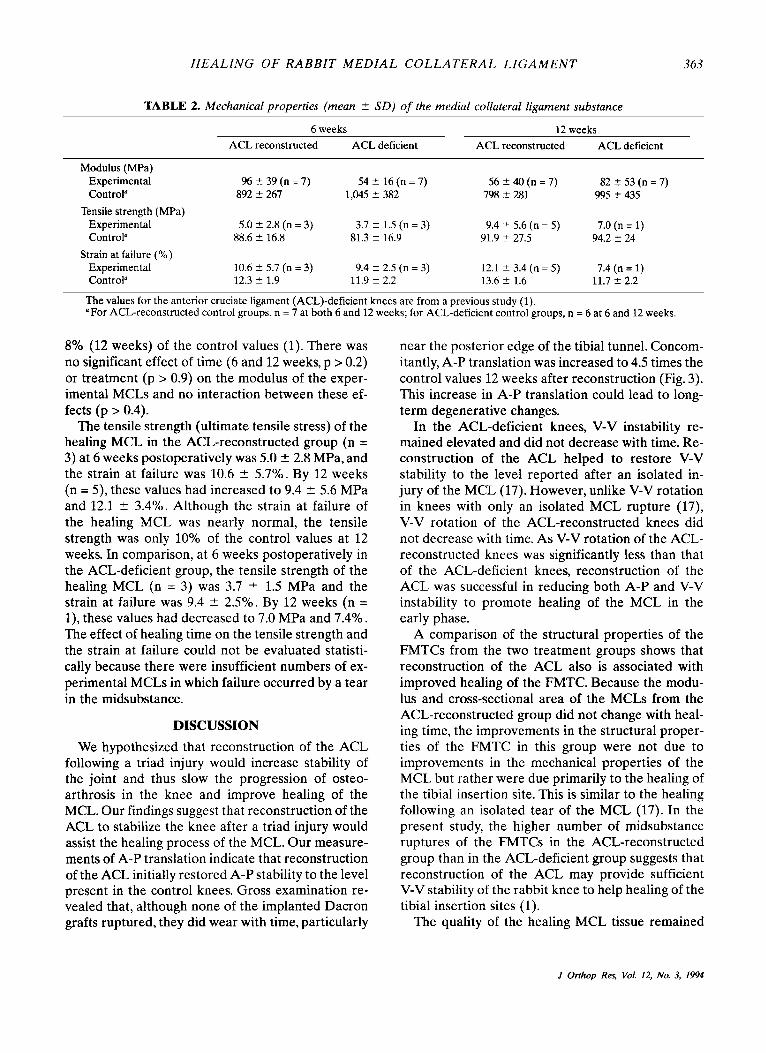
TABLE 2. Mechanical properties (mean ? SD) of the medial collateral ligament substance
6 weeks 12 weeks ACL reconstructed ACL deficient ACL reconstructed ACL deficient
Modulus (MPa) Experimental 96 2 39 (n = 7) 54 2 16 (n = 7) 56 t 40 (n = 7) 82 2 53 (n = 7) Control" 892 2 267 1,045 5 382 798 t 281 995 2 435
Tensile strength (MPa) Experimental Control" 88.6 2 16.8 81.3 -C 16.9 91.9 ? 27.5 94.2 2 24
Experimental Control" 12.3 IT 1.9 11.9 t 2.2 13.6 2 1.6 11.7 2 2.2
5.0 2 2.8 (n = 3) 3.7 2 1.5 (n = 3) 9.4 5 5.6 (n = 5) 7.0 (n = 1)
Strain at failure (YO) 10.6 t 5.7 (n = 3 ) 9.4 t 2.5 (n = 3) 12.1 t 3.4 (n = 5) 7.4 (n = 1)
The values for the anterior cruciate ligament (ACL)-deficient knees are from a previous study (1). "For ACL-reconstructed control groups, n = 7 at both 6 and 12 weeks; for ACL-deficient control groups, n = 6 at 6 and 12 weeks.
8% (12 weeks) of the control values (1). There was no significant effect of time (6 and 12 weeks, p > 0.2) or treatment (p > 0.9) on the modulus of the exper- imental MCLs and no interaction between these ef- fects (p > 0.4).
The tensile strength (ultimate tensile stress) of the healing MCL in the ACL-reconstructed group (n = 3) at 6 weeks postoperatively was 5.0 2 2.8 MPa, and the strain at failure was 10.6 t- 5.7%. By 12 weeks (n = 5) , these values had increased to 9.4 2 5.6 MPa and 12.1 2 3.4%. Although the strain at failure of the healing MCL was nearly normal, the tensile strength was only 10% of the control values at 12 weeks. In comparison, at 6 weeks postoperatively in the ACL-deficient group, the tensile strength of the healing MCL (n = 3) was 3.7 ? 1.5 MPa and the strain at failure was 9.4 5 2.5%. By 12 weeks (n = l), these values had decreased to 7.0 MPa and 7.4%. The effect of healing time on the tensile strength and the strain at failure could not be evaluated statisti- cally because there were insufficient numbers of ex- perimental MCLs in which failure occurred by a tear in the midsubstance.
DISCUSSION We hypothesized that reconstruction of the ACL
following a triad injury would increase stability of the joint and thus slow the progression of osteo- arthrosis in the knee and improve healing of the MCL. Our findings suggest that reconstruction of the ACL to stabilize the knee after a triad injury would assist the healing process of the MCL. Our measure- ments of A-P translation indicate that reconstruction of the ACL initially restored A-P stability to the level present in the control knees. Gross examination re- vealed that, although none of the implanted Dacron grafts ruptured, they did wear with time, particularly
near the posterior edge of the tibial tunnel. Concom- itantly, A-P translation was increased to 4.5 times the control values 12 weeks after reconstruction (Fig. 3). This increase in A-P translation could lead to long- term degenerative changes.
In the ACL-deficient knees, V-V instability re- mained elevated and did not decrease with time. Re- construction of the ACL helped to restore v-V stability to the level reported after an isolated in- jury of the MCL (17). However, unlike V-V rotation in knees with only an isolated MCL rupture (17), V-V rotation of the ACL-reconstructed knees did not decrease with time. As V-V rotation of the ACL- reconstructed knees was significantly less than that of the ACL-deficient knees, reconstruction of the ACL was successful in reducing both A-P and V-V instability to promote healing of the MCL in the early phase.
A comparison of the structural properties of the FMTCs from the two treatment groups shows that reconstruction of the ACL also is associated with improved healing of the FMTC. Because the modu- lus and cross-sectional area of the MCLs from the ACL-reconstructed group did not change with heal- ing time, the improvements in the structural proper- ties of the FMTC in this group were not due to improvements in the mechanical properties of the MCL but rather were due primarily to the healing of the tibial insertion site. This is similar to the healing following an isolated tear of the MCL (17). In the present study, the higher number of midsubstance ruptures of the FMTCs in the ACL-reconstructed group than in the ACL-deficient group suggests that reconstruction of the ACL may provide sufficient V-V stability of the rabbit knee to help healing of the tibial insertion sites (1).
The quality of the healing MCL tissue remained
I Orthop Res, Vol. 12, No. 3, 1994

364 C. P. ENGLE ET AL.
poor, as the modulus of the experimental specimens reached only 10% of the control values. The healing MCL consisted of large quantities of ligamentous scar tissue; the cross-sectional area of the midsub- stance reached more than 18 mm2 at 12 weeks. It should be noted that, during dissection, there were some difficulties in distinguishing the healing MCL from the surrounding soft tissues in both groups.
In this study, we have shown that reconstruction of the ACL initially stabilizes the rabbit knee joint by decreasing V-V rotation and A-P translation, which may, in turn, promote healing of the MCL. Additionally, joint stabilization decreased the inci- dence of early-onset osteoarthrosis in rabbits. Thus, reconstruction of the ACL in a patient with a triad injury may be preferable to nonoperative treatment. However, whether concomitant repair of the MCL would lead to improved tensile properties of the healed MCL remains unknown and should be inves- tigated. Additional studies also are needed to exam- ine alternative grafting materials and to monitor the effect of ACL reconstruction on long-term stability of the knee joint and on morphology of the joint.
Acknowledgment: This work was supported by Vet- e rans Administration Rehabilitation, Research and De- velopment G r a n t A188-4RA and by the University of Pittsburgh Medical Center.
1.
2.
3.
4.
5.
REFERENCES Anderson DR, Weiss JA, Takai S, Ohland KJ, Woo SL-Y Healing of the medial collateral ligament following a triad injury: a biomechanical and histological study of the knee in rabbits. J Orthop Res 10:485-495,1992 Bain JR: Body size and tensile strength of the mammalian anterior cruciate ligament. Trans Orthop Res Soc 14:325, 1989 Ballmer PM, Ballmer FT, Jakob RP: Reconstruction of the anterior cruciate ligament alone in the treatment of a com- bined instability with complete rupture of the medial collat- eral ligament. Arch Orthop Trauma Surg 110:139-141,1991 Hastings DE: The non-operative management of collateral ligament injuries of the knee joint. Clin Orthop 147:22-28, 1980 Holden DL, Eggert AW, Butler JE: The nonoperative treat-
6.
7.
8.
9.
10.
11.
12.
13.
ment of grade I and I1 medial collateral ligament injuries to the knee. A m J Sports Med 11:340-344.1983 Indelicato PA: Non-operative treatment of complete tears of the medial collateral ligament of the knee. J Bone Joint Surg [Am] 65:323-329,1983 Inoue M, McGurk-Burleson E, Hollis JM, Woo SL-Y Treat- ment of the medial collateral ligament injury. I: The impor- tance of anterior cruciate ligament on the varus-valgus knee laxity. A m J Sports Med 15:15-21,1987 Kannus P: Long-term results of conservatively treated me- dial collateral ligament injuries of the knee joint. Clin Or-
Larson RL. Combined instabilities of the knee. Clin Orthop
Markolf KL, Kochan A , Amstutz HC: Measurement of knee stiffness and laxity in patients with documented absence of the anterior cruciate ligament. J Bone Joint Surg [Am]
McIntosh D L The anterior cruciate ligament: “over the top” repair. In: Proceedings of the Canadian Orthopaedic Association. J Bone Joint Surg [Br] 56591,1974 Montgomery RD, Milton JL, Terry GC, McLeod WD, Mad- sen N: Comparison of over-the-top and tunnel techniques for anterior cruciate ligament replacement. Clin Orthop 231:144-153,1988 O’Donoghue DH: Surgical treatment of fresh injuries to the major ligaments of the knee. J Bone Joint Surg [Am] 32:721-738,1950
thop 226:103-112,1988
147:68-81,1980
66:242-253,1984
14. O’Donoghue DH: An analysis of end results of surgical treatment of major injuries to the ligaments of the knee. J Bone Joint Surg [Am] 37:l-13,124,1955
15. Sandberg R, Balkfors B, Nilsson B, Westlin N: Operative versus non-operative treatment of recent injuries to the ligaments of the knee: a prospective randomized study. J Bone Joint Surg [Am] 69:1120-1126,1987
16. Shelbourne DK, Baele JR: Treatment of combined anterior cruciate ligament and medial collateral ligament injuries. A m J Knee Surg 156-62,1988
17. Weiss JA, Woo SL-Y, Ohland KJ, Horibe S, Newton PO: Evaluation of a new injury model to study medial collateral ligament healing: primary repair versus nonoperative treat- ment. J Orthop Res 9516-528,1991
18. Wilson WJ, Scranton PE Jr: Combined reconstruction of the anterior cruciate ligament in competitive athletes. J Bone Joint Surg [Am] 72:742-748,1990
19. Woo SL-Y, Gomez MA, Seguchi Y, Endo CM, Akeson WH: Measurement of mechanical propcrties of ligament sub- stance from a bone-ligament-bone preparation. J Orthop Res 1:22-29,1983
20. Woo SL-Y, Danto MI, Lee TQ, Newton PO: The use of a laser micrometer system to determine the cross-sectional shape and area of ligaments: a comparative study with two existing methods. J Biomech Eng 112:426-431, 1990
21. Zarins B, Adams M: Knee injuries in sports. N EngI J Med 318:950-960,1988
J Orthop Rrs, Vol. 12, No. 3, 1994




























