Embed Size (px)
Citation preview

Copyrig
Guidelines for the implementation of culturally sensitive CBTamong refugees and in global contexts
Intervention 2014, Volume 12, Supplement 1, Page 78 - 93
Guidelines for the implementation ofculturally sensitive cognitivebehavioural therapy among refugeesand in global contexts
Devon E. Hinton & BalandJalal
In this article, we suggest guidelines that should be
followed in order to create a culturally sensitive cog-
nitive behavioural therapy among refugees and in
global contexts moregenerally, so as to maximise e⁄-
cacy and e¡ectiveness.These guidelines can be fol-
lowed to design culturally sensitive cognitive
behavioural therapy studies, or what might be called
‘contextually sensitive cognitive behavioural therapy’,
amongrefugeesorotherculturalgroups in agivenglo-
bal location, and the guidelines can be used to evalu-
ate such studies. Some examples of these guidelines
are culturally appropriate framing of cognitive beha-
vioural therapy techniques, assessing and addressing
key local complaints (e.g. somatic symptoms, spirit
possession and syndromes such as ‘thinking a lot’)
and catastrophic cognitions about those complaints,
and incorporating into treatment key local sources
of recovery and resilience.
Keywords: cognitive behavioural therapy,global health, refugees
IntroductionStudiesindicatethepotentiale⁄cacyofcogni-tive behavioural therapy (CBT) among refu-gees and in global contexts (e.g. Bass et al.,2013;Drozdek,Kamperman,Tol,Knipscheer,& Kleber, 2014; Murray et al., 2014). Thisarticle suggests ways to make the next waveofCBTtreatmentsamongrefugeesandwithingloballocationsmoresensitivetoculturalcon-text.Arecentarticleadvocatedthatachecklistbe used for all studies published in journals toassure their cultural sensitivity (Lewis-Fer-na¤ ndez et al., 2013). Here we suggest a kind of
ht © War Trauma Foundation. Unautho78
checklist that canbe used to evaluate the cul-tural sensitivity (or whatmight alsobe called‘contextual sensitivity’)ofaCBTinterventionamong refugees or other cultural groups in agiven global location. Many of theseparameters have guided our treatment devel-opmentandtheglobalhealthresearchagendamore generally (Hinton, Chhean, Pich, Saf-ren, Hofmann, & Pollack 2005; Hinton, Hof-mann, Pollack, & Otto, 2009; Hinton,Hofmann, Rivera, Otto, & Pollack, 2011a;Hinton, Pham,Tran, Safren, Otto, & Pollack,2004; Hinton, Rivera, Hofmann, Barlow, &Otto, 2012b; Patel, 2012; van Ginneken et al.,2013).
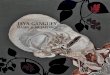
Guidelines for theimplementation of culturallysensitive CBTIn Figure 1, we give an overview of theparameters and a subgrouping of thoseparameters that should be assessed in deter-mining the cultural sensitivity of a treatment.
Background informationIdentify the cultural group Identifyingthe exact cultural group is importantbecauseitwill in£uencemanyoftheparametersbelow,such as a group’s history of trauma, stigma inthe group about mental illness, catastrophiccognitions about symptoms and religiousbased techniques that may be included intreatment. Moreover, determining the exactcultural group that a study involves givesinsights into generalisability. Moreover, in
rized reproduction of this article is prohibited.

Copyrig
Identify the exact cultural group
Specify language of group and oftreatment
Identify key demographics variables(gender, socioeconomic, education,
literacy) Making CBT techniques tolerable and credibleDetermine religious background
Address typical traumas in the group
Address key stressors of the group
Describe how and where the patient was identified and recruited in the health care system
Identify and address key DSM-5 disorders
Create models of how disorder is generated in thegroup in question to identify treatment targets
Identify and address complaints of most concern to the thosebeing treated (e.g., local illness categories)
Identify and address complaints of mostconcern to the community
Utilise local sources of resilience and recovery
Make the treatment consonant with the localethnopsychology, ethnophysiology and ethnospirituality
Utilise culturally appropriate metaphors and proverbs
Address stigma about the disorder and getting treatment for the disorder
Address structural barriers to treatment
Attend to social demand and economic effects
Increase credibility and positive expectancy
Maximise adherence
Specify scale-up and sustainability potential
Dimensions ofCulturally Sensitive
Treatment
Identify and address key psychopathological dimensions(e.g., somatic sensation and catastrophic cognitions)
Address mechanisms and dimensions of psychopathologyIdentify and address keylocal concerns
Assess relevant background informationand impact on treatment
Address key ecological factors Maximise access
Issues of patient–therapist matching
Maximise acceptablity and efficacy
Include local illness categories asoutcome measures
Figure 1: Key parameters for evaluating the degree of culturally sensitivity of a treatment.
DSM-5, Diagnostic and Statistical Manual of Mental Disorders, 5th Edition.
Hinton&Jalal
outcome studies, it allows a determination ofthe cultural heterogeneity of a sample andmakes possible some balancing of treatmentarms. However, often treatment studiessimply state that the participants are from acertain country without discussing the cul-tural group or whether all or some of theparticipants are from aminority or an ethnicgroup.As anexample, LatinosmaybeCarib-bean Latino (e.g. from Puerto Rico or theDominican Republic), Central American,Peruvian,orMexican,amongotherlocalities,with each of these groups having di¡erentsocial and cultural histories, further, withinthose countries there are large minoritygroups(e.g.QuechuainPeru).Or, foranotherexample, many Burmese are members ofKaren or other hill tribe groups, groups thatare culturally distinct from the majority ofBurmese.Likewise,apersonidenti¢edasIraqicould belong to an Arabic, Kurdish,Turkme-nian or Assyrian cultural group, and couldbe Muslim (Sunni, Shia, Alevi),Yezidi, Zor-oastrian, Christian or Jewish, with each ofthese groups falling under the general
ht © War Trauma Foundation. Unautho
categoryof Iraqi, and in somecasesbelongingtothesamereligiousdenomination(e.g.SunniIslam), and may have very di¡erent culturalcustoms. For example, although Arabs andKurds are both Iraqis and Sunni Muslims,their cultural customs di¡er.Specify the language of the group andlanguage of treatmentThelanguagesthatthe participants speak should be speci¢edandwhether the treatment was conducted inthe preferred or a secondary language, andwhether a translator was used. Degree of£uency of the client in the language in whichtherapywas conducted needs tobe described.For example, in many countries, there aremultiple languages spoken but a singlenational language, with variable £uency inthe national language. For example, in Iraq,whileArabicisthenationallanguage,inmajorparts of Northern Iraq Arabic is not spoken,but ratherKurdish andTurkman.Identify key demographic variables Inaddition to gender, the treatment populationshouldbe characterised intermsof keydemo-graphic variables such as socio-economic
rized reproduction of this article is prohibited.79

Copyrig
Guidelines for the implementation of culturally sensitive CBTamong refugees and in global contexts
Intervention 2014, Volume 12, Supplement 1, Page 78 - 93
status (SES), educationand literacy level. It isimportant to know these variables so as toevaluate the generalisability of a particularintervention. For example, the level of edu-cation and literacy will determine whetherwritten handouts can be used. Similarly,DVDsmay notbewell accepted among somemembers of lower SESwho donot commonlyuse them. As an alternative to written hand-outs and DVDs, it may be necessary to draweasy-to-understand diagrams and ¢gures.SES may indicate adherence to traditionalculture and religion, a measure of accultura-tion. In addition, variables such as SES mayindicate current levels of stress, which mayin£uence the ability to tolerate and bene¢tfrom therapy: exposure may be contraindi-cated (Lester, Resick, Young-Xu, & Artz,2010; see also the section below,‘Identify andaddress key stressors’).Detail the religious background of thegroup and its impact on treatmentOne should characterise the group in ques-tion in respect to religious background. Isthe group mainly Buddhist, Christian, Mus-lim or another religion, and what is thedistribution in the group? Which type ofBuddhism (e.g.Theravandanor Zen), Chris-tianity (e.g. Pentecostal or Catholic) orIslam (e.g. Sunni or Shia)? Furthermore,the way religion is practised and the levelof religiosity may di¡er, even within thesame subbranch of a religion.Theway SunniIslam is practiced in Saudi Arabia (whereadherents often have a sala¢ orientation ofIslam) may di¡er in some respects from theway Sunni Islam is practiced in, say, Egyptor Morocco; for instance, gender inter-actions outside marriage and one’s immedi-ate family may be more restricted in theformer population. Religious hybridityshould also be taken into account: Christian-ity among the Sepedi tribe of South Africais an amalgamation of traditional Christian-ity and local beliefs in ancestral spirits, evilcurses and black magic.As is discussed in a section below, ideallylocal religious leaders should ¢rst be
ht © War Trauma Foundation. Unautho80
consulted to determine their understandingof the types of distress in the population,what religious and other treatments theythink should occur and how they thinkwestern type interventions might be success-fully conducted. Religious or spiritual beliefsmay provide sources of resilience or con-stitute obstacles to care. In some Islamiccultures, it may be necessary to match thera-pist and client in respect to gender as a wayof adapting treatment to religious beliefs(Murray et al., 2014). The local religionmay provide ways to frame treatment tomake it more acceptable. In our treatment,we incorporate local healing traditions toincrease e⁄cacy and treatment acceptabilityand positive expectancy; see the section‘Utilise local sources of resilience andrecovery’.Attend to social demand character-istics, economic incentives andeconomic e¡ects In a given context, socialdemand and ¢nancial aspects of the studymay a¡ect the results both at the level of thetherapist and patient: participants may feelpressure to report positive outcome. Identify-ing SES is important in terms of determiningthe e¡ect of compensation for participationintreatments. In lowerSESgroups, ifcompen-sation is provided, thismay serve as aprimarymotivator forthepatienttocompletethe study.Consequently, it is di⁄cult to determine thelevel of acceptability of the given treatment inthe culture at hand. Likewise, general well-beingmaybe enhancedby receiving compen-sation,whichine¡ectwouldmaketheoutcomedatadi⁄cultto interpret. It isalsoamodelthatcannot be used at the scale-up stage owing toeconomic limitations.
Key ecological factors to addressidentify and address key stressors Ithasbeen shownthat worrymaybe a keygen-erator of distress in traumatised populationsandother populations (Hinton&Lewis-Fer-na¤ ndez, 2011; Hinton, Nickerson, & Bryant,2011b). From a public health standpoint,when applying CBT in global contexts, it is
rized reproduction of this article is prohibited.

Copyrig
Hinton&Jalal
important to be aware of local problems thatmaybeaddressedfortheentiregroup:securityconcerns, refugee status, and access to water(Bolton, Michalopoulos, Ahmed, Murray, &Bass,2013;Hinton&Hinton, inpress). Ideally,thismaybe addressedat the community levelas a public health intervention. Also, oneshould specify whether the participant hasan advocatewho can help address key practi-cal problems such as the equivalent of a socialworker.TheCBTmayneed to address practi-cal problems as part of treatment, a kind ofbehaviouralactivationanddidacticsincoping(Nezu, Nezu,&Lombardo,2004).Identify and address typical traumasin the group The traumas that a groupbeingtreatedhasexperiencedandisexperien-cing should be identi¢ed and addressed.Thegroup inquestionmayhaveenduredmassvio-lence of somekind,maybe £eeing fromagen-ocide or civil war or may be experiencinghigh rates of sexual violence.Whenprovidingeducation about CBT, these traumas can bespeci¢callydescribedandaddressed. Identify-ing traumas is also crucially important fromapublichealthstandpoint: itmaybefoundthatsexual violence or domestic violence is ende-mic in a certain context. This has importantimplications inrespecttotreatmentandpublichealth interventions: the therapist should becareful to query speci¢cally about a history ofthe trauma such as domestic violence, shouldbe sensitive to its possible presence and shouldbe aware of what local resources are availablefor someone so impacted.
Identify and address key localconcernsIdentify and address complaints ofmost concern to those being treatedIn a cultural context, certain symptoms willbe of great concern; for example, amongmany Cambodian refugees, these mayinclude sleep paralysis, dizziness, poor sleepand panic attacks (Hinton, Kredlow, Pich,Bui, & Hofmann, 2013a).The key local com-plaints may be cultural syndromes. For
ht © War Trauma Foundation. Unautho
example, Cambodians frequently attributeanxiety symptoms to ‘heart weakness’ and‘windattacks’ (khya“ l attacks), and these attri-butions produce multiple catastrophic cog-nitions. Especially in some Africancontexts, possession fears are prevalent intraumatised populations, with posttrau-matic stress disorder (PTSD) and arousalsymptoms sometimes being attributed topossession, and so a particular social andcultural course created (de Jong & Reis,2010, 2013). As described below, framingtreatment as addressing these key com-plaints greatly increases CBT acceptabilityand adherence. Also, as described above,failure to assess and treat key concerns suchas somatic symptoms, possession and cul-tural syndromes would be a case of categorytruncation. See the following section forfurther discussion of the assessment issue.Include local illness categories as out-come measures More generally, we havesuggested that all outcome studies in cross-cultural settings should include a list oflocally salient, somatic complaints, cata-strophic cognitions and cultural syndromes,which we have called ‘Symptom and Syn-drome Inventories’, for example, a ‘Cambo-dian Symptom and Syndrome Inventory’,or C-SSI (Hinton, Hinton, Eng, & Choung,2012a; Hinton et al., 2013a). Or also, in atreatment of a Latino group, we showed thatataques de nervios improved across treatment(Hintonet al.,2011a) and so too, in aCambo-dian population, orthostatic dizziness (Hin-ton et al., 2009). Given that these localillness categories indicate the patient’s expla-natory model of the disorders in question,and given the importance of explanatorymodels in treatment, this makes the assess-ment all the more important (Benish, Quin-tana, & Wampold, 2011; Hinton, Lewis-Ferna¤ ndez, Kirmayer, & Weiss, in press).These are the experience-near categoriesand will be highly related to self-perceivedwellbeing. Inaddition, as atherapeutic inter-vention, the patient can be told that all theitems in the assessment battery, including
rized reproduction of this article is prohibited.81

Copyrig
Guidelines for the implementation of culturally sensitive CBTamong refugees and in global contexts
Intervention 2014, Volume 12, Supplement 1, Page 78 - 93
the culturally salient categories of distress,should improve in treatment. As indicatedabove, we have used culturally sensitivemeasures in our treatment and found themto improve across treatment (Hinton et al.,2011a; 2012a; 2013a). Asking the patientsabout these locally salient distress formsand whether they have improved acrosstreatment is a key part of culturallysensitive treatment.Identify and address complaints ofmost concern to the community Oneshould ask local leaders about whichbehav-ioural and symptomatic issues are of keyconcern, asking speci¢cally about violence,substance abuse and suicidality in the com-munity. If the treatment is then framed asaddressing these issues, it will reduce stigmaabout the ailment and mobilise thecommunity. (Local leaders may includepolitical, religious, and informal and formalhealth providers, as well as heads of localadvocacy groups.) For example, once it isunderstood what social and psychologicalmechanisms generate the problem, then thefocus is on resolution rather thanonblamingthe victim or using other forms of nonpro-ductive labelling. It provides an alternativeframing.
Addressmechanism and dimensionsof psychopathologyIdentify and address key DSM1 dis-orders In some groups such as traumatisedrefugees, certain disorders such as PTSDand panic disorder may be particularly elev-ated (Hinton & Lewis-Ferna¤ ndez, 2011); forexample, among Cambodian refugees, otherthan PTSD, there are extremely high ratesof panic attacks and panic disorder. Eachgroupmayhave aunique pro¢le ofDSMdis-orders. The pro¢le of disorders will informtreatment and the design and implementa-tion ofmodules. For example, if panic attacksare common in a locality, then panic attacksshould be assessed and also addressedin modules.
ht © War Trauma Foundation. Unautho82
As indicated in several places in this article,the DSM has limitations as a diagnostic sys-tem, and so just addressing DSM disordersis not ideal, leaving out key treatment tar-gets. For one, the DSM often does not assesskey areas of concern, such as somatic com-plaints in the case of PTSD. Second, it is acategorical approach that minimises dimen-sional assessment. And third, the experi-ence-near categories according to whichdisorder is locally understood are usuallynot DSM categories, but other localcategories such as khya“ l attacks among Cam-bodian populations and ‘thinking a lot’among many cultural groups; see below.These non-DSM constructs should also beidenti¢ed and addressed (see below).Identify and address key psychopatho-logical dimensionsOther than DSM dis-orders, it is important to identify keypsychopathological dimensions in a group,such as pathological worry (rather than aGeneralized Anxiety Disorder), cata-strophic cognitions, somatic symptoms,panic attacks, anger, substance abuse or sui-cidality (Hinton et al., 2011b; Morris &Cuthbert, 2012). This analytic approach isin keeping with the call to use dimensionalanalysis to identify treatment targets (Casey,Craddock, Cuthbert, Hyman, Lee, &Ressler, 2013). Let us further highlight theimportance of identifying addressingsomatic sensations and catastrophic cogni-tions among refugee and global populationsin a culturally sensitive manner.It has been found that somatic symptoms areprominent in many nonwestern populations(de Jong, Komproe, Spinazzola, van derKolk, & van Ommeren, 2005; Hinton &Good, 2009; Hinton & Lewis-Ferna¤ ndez,2011). Ideally, one should identifykey somaticconcerns in a population so that these maybe addressed in CBT.This canbe consideredas the assessment of a psychopathologicaldimension, namely, somatic complaints,but with the aim of assessing key somaticcomplaints, in order to avoid an abstraction
error, that is, the error of only considering
rized reproduction of this article is prohibited.

Copyrig
Hinton&Jalal
somatic symptoms in general without asses-sing key symptoms of concern; for example,Cambodians often present with somaticcomplaints, but with dizziness and headachebeing particularly important complaints.(An abstraction error is also not consideringthe local meaning of the complaint, such asthe interpretation of a certain somatic symp-toms in terms of the local ethnopsychologyand ethnophysiology.) Not assessing keysomatic symptoms is also an example ofcategory truncation (Hinton & Good, inpress) in respect to assessing local distress,as is not assessing other key concerns suchas catastrophic cognitions. For example,among trauma survivors, not only ‘PTSD’but also these other complaints—somaticsymptoms and catastrophic cognitions—may be a key part of the presentation.A standard part of CBT is addressing cata-strophic cognitions about symptoms such asthose concerning PTSD and somatic symp-toms(Hintonetal.,2012b).Forexample,manyCambodian refugees fear that neck sorenessindicates that their neck vessels will burst,and they fear that dizziness on standingindicates the onsetofadangerouskhya“ lattack,or ‘wind attack’, a surge of khya“ l and bloodupward in the body that may cause varioussymptoms and disasters (Hinton & Good, inpress; Hinton, Pich, Marques, Nickerson, &Pollack,2010).OrmanyCambodians are con-cerned that worry will overheat the brainand cause permanent forgetfulness. OurrecentclinicalexperienceinSouthAfricawithmembersoftheSepeditribeofNorthernSothorevealed that catastrophic cognitions aboutPTSD symptoms and somatic symptomsinclude belief in ancestral curses and spiritsreferred to as amafufunyana (for possessionfears elsewhere in Africa, see deJong & Reis,2010, 2013). Among Egyptians, catastrophiccognitionsmay include concerns that anxietyand somatic symptoms are caused by heartproblems (alby beyrafraf). Learning the localethnopsychology, ethnophysiology and eth-nospirituality as it applies to symptoms andprocesses such as ‘worry’ is a key way of
ht © War Trauma Foundation. Unautho
identifying these catastrophic cognitions. Inevery culture, there will be local ideas abouthow symptoms of anxiety and depression aregenerated and treated. The clinician canaddress the catastrophic cognitions in severalways, such as giving an alternative framingin terms of the harmless biology of anxiety,byteachingtocontrolthe symptombyrelaxa-tion methods (breath-focused techniques orapplied stretching and muscle relaxation)and by interoceptive exposure2 that teachesthe innocuousness of the symptoms.Create ‘etic’ and ‘emic’ models of howdisorder is generated in the popu-lation in question to identify treat-ment targets How particular complaintscome to be generated should be identi¢ed,which have been called causal networkmodels (McNally, 2012). We have described‘etic’ and ‘emic’3 causal networks for keysymptoms among Cambodian refugees.Cambodians refugees have high rates ofsomatic complaints and panic attacks. Inrespect to the ‘etic’ model, we have deter-mined that panic attacks often began witha somatic symptom caused by a trigger, suchas worry or standing up from the sitting orlying position; the somatic symptom oftenthen gave rise to catastrophic cognitions,for example, dizziness resulting in fears ofthe onset of a dangerous khya“ l attack, andthe somatic symptomoften triggered traumaassociations, for example, dizziness givingrise to memories of doing slave labour whilestarving (Hinton & Good, 2009; Hinton,Hofmann, Pitman, Pollack, & Barlow,2008; Hinton et al., 2010, 2011b). The modelis also‘emic’ in that it takes into account localideas about the workings of the body andmind, and thus might be called an etic-emicmodel. Other than allowing the identi¢-cation of treatment targets, determiningthese locally informed transcultural causalmodels promotes treatment in many ways.For example, data would suggest that elicit-ing these causal narratives, which will alsobe shared with patients andwhich incorpor-ate the local conceptualisations of mind,
rized reproduction of this article is prohibited.83

Copyrig
Guidelines for the implementation of culturally sensitive CBTamong refugees and in global contexts
Intervention 2014, Volume 12, Supplement 1, Page 78 - 93
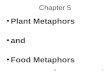
body and spirituality, improve positiveexpectancy, among other e¡ects (Hinton &Lewis-Ferna¤ ndez, 2010); see below forfurther discussion.A type of syndrome found in manycultures, ‘thinking a lot’, can be describedby such causal network models (Hinton etal., 2008; Hinton, Reis, & de Jong, in press),providing an important entre¤ e to localethnopsychology and ethnophysiology. (On‘thinking a lot’, see also Bolton, Surkan,Gray, & Desmousseaux, 2012; Kaiser et al.,2014; Patel, Simunyu, & Gwanzura, 1995.)Figure 2 shows how the syndrome of ‘think-ing too much’ is conceptualised amongCambodian refugees.The local ‘emic’modelpostulates distress episodes to involve certainpathological processes: the trigger of an epi-sode, which may be various causes, particu-larly worry, thoughts about past traumas,rumination on past failures, or pained recallof someone who has died or lives far away;and then this ‘thinking too much’may causepoor sleep and weakness, which in turnscauses more ‘thinking too much’, and
ht © War Trauma Foundation. Unautho
‘Thinking too much’(about current worries,
trauma events,depressive themes,
bereavement issues)
Anger and irrita
Khyâl attacks(caused by a disruptionthe flow of blood and kh
in the body)
Treating ‘thinking too much’ and its induced symptoms by mindfulness, obeisance to the Buddha, ‘coining,’ snapping the
‘For
Poor sleepand
appetite
Weakness
Figure 2: The Cambodian explanatory model of
84
furthermore ‘thinking too much’ may causeelevated anger and various serious disturb-ances of mind and body, like permanent for-getfulness and ‘khya“ l attacks’. Figure 2 alsoshows how Cambodians traditionally treat‘thinking a lot’.This ‘emic’model canbe con-ceptualised in terms of the ‘etic’ modeldescribed in the paragraph above. The ‘etic’and ‘emic’ models reveal multiple possibletreatment targets and how to discuss symp-toms and interventions in a way that willbe locally understood. Determining ‘emic’models give a central place to local ideas ofcausation, culturally speci¢c concerns andcatastrophic cognitions, and local ideas ofideal treatment allows the researcher/clini-cian to ground the treatment in the localcontext and to bridge from current psycho-logical theory to local explanatory models.Thus, for example, assessment of ‘thinkinga lot’ in a locality where it occurs, and inves-tigating the causal network, is an importantpart of treatment localisation, and we haveproposed a questionnaire that can be usedto do so (Hinton, Reis, & deJong, in press).
rized reproduction of this article is prohibited.
bility Toxique(dangerous toself and others
owing to extremeirritablity)
Crazy (lâp)
ofyâl
Many symptoms (dizziness, SOB,neck soreness) and possibly deathfrom bodily dysfunction (syncope,
asphyxia, neck rupture)
various methods such as attentional control, meditation, joints, and taking tonics and sleep and appetite promoters
getful-and-distracted’(pluc pleang)
Overheated brain
‘thinking a lot’.

Copyrig
Hinton&Jalal
Utilise local sources of resilience andrecoveryIn certain localities, there may be healingtraditions suchasBuddhistmeditationorIsla-mic spirituality (e.g.Tazkiyah-tul-nafs, or‘puri-¢cation of the soul’) that are helpful topatients (Hinton & Kirmayer, 2013). Incor-porating these practices into CBT alsoincreases acceptability and positive expect-ancy. These techniques can inform the CBTtreatment itself and its components, andparticipants may be encouraged to use suchmethods: for Buddhists, incorporating medi-tation into the treatment may be useful, andfor some Islamic populations, incorporatinga type of supplication known as Dhikr whereGod is repeatedlypraised, oftenusing varioushonori¢cnames. Inourtreatment for trauma-tised Southeast Asian refugees, we utilisemultiple mindfulness techniques (Hinton,Ojserkis, Jalal,Peou,&Hofmann,2013b;Hin-ton, Pich, Hofmann, & Otto, 2013c). In ourtreatment for Islamic populations, we haveincorporated traditional healing practicesthat involveattentional focusandcentrednesson a positive e¡ect and that are compatiblewith CBT in those and other respects (Amer& Jalal, 2011). For one, there isDhikr. Second,there numerous supplications recommendedby the Islamic Prophet, Muhammad, for thepersonwho is indistress, anxiousorovercomebysadnessorgrief.Andthird, thereareawidevarietyof spiritualhealingtechniques,knownas Ruqyah, that to a great extent are commonto the major Islamic denominations andgroups in the Islamic world (e.g. Sunnis andShias). Ruqyah is the Arabic term fortraditional Islamic healing practice, whichincludesrecitationoftheQuran,theholybookof Islam (often in a trance-like or meditativestate), usually of certain Quranic versesthought to promote healing. Other practicesof Ruqyah have traditionally been to reciteQuranic verses over buckets of water thatone may drink or bath in, and to apply oliveoil (the olive is considered a blessed fruit inIslam) on the entire body, for examplebefore sleep.
ht © War Trauma Foundation. Unautho
Ideally, the treatment intervention can beframed in terms of these local traditions. Insome cases, it is useful to end the CBT treat-ment with local rituals that indicate puri¢-cation or healing in a general sense, whichhelps to change self-image and creates asense of positive expectancy (Hinton et al.,2012b). As an example of this, for an Islamicpopulation, there are Wudhu and Ghusl
(ritualistic washing of face, arms and feetor the entire body), which are types of spiri-tual puri¢cation techniques signifying atransition from spiritual impurity to purity.Or among Southeast Asian populations, thistakes the form of various types of steamingrituals. Such rituals help to change self-ima-gery, which is a key issue in traumatisedand other populations, and increase thesense of being transformed, promotingpositive expectancy (Agger, Igreja, Kiehle,& Polatin, 2012; Hinton et al., 2012b). (How-ever, the clinician must also be aware thatsome local healing practices may have nega-tive e¡ects [Dyregrov, Gupta, Gjestad, &Raundalen, 2002; Kohrt, in press].)
Maximise acceptability and e⁄cacyBelow we discuss ways to address treatmentacceptability and to improve e⁄cacy.Theseare closely related because whatever makesthe treatment acceptable will usually makeit more e⁄cacious.Make the treatment consonant withthe local ethnopsychology, ethnophy-siology and ethnospiritualityAs empha-sised throughout this article, one shoulddetermine how the psychological distress islocally understood (e.g. in terms of local syn-dromes and certain key symptoms) and howit is locally thought that treatment should beconducted for the condition (Hinton et al.,2012b;Kohrt,Maharjan,Timsina,&Gri⁄th,2012; Ventevogel, Jordans, Reis, & de Jong,2013). Investigating this local understandingof symptoms gives key insights for adaptationin respect to many of the parameters(Figure 1): locally emphasised complaintsand sources of resilience and recovery. For
rized reproduction of this article is prohibited.85

Copyrig
Guidelines for the implementation of culturally sensitive CBTamong refugees and in global contexts
Intervention 2014, Volume 12, Supplement 1, Page 78 - 93
example, among the Cambodian culture, thecomplaintof ‘thinkingtoomuch’is commonlydescribed in terms of lack of mindfulness andattentional control, and so we have incorpor-ated mindfulness (e.g. attending to sensorialinput inthepresentmoment) inour treatmentfor that group. A recent review indicated thatcultural adaptation of treatment increasede¡ect size and that the key aspect of culturaladaptationwas eliciting the patient’s explana-tory model of disorder (Benish et al., 2011);the cultural adaptation should explain theintervention in a culturally consonant way,whichmightbecalled explanatorymodelbridging.Thus, the attempt at bridging, which requireseliciting the patient’s explanatory model, isseemingly e⁄cacious on its own for variousreasons: the building of empathy and thepatient’s feelingthatthetherapistunderstandshis/her concerns, with the therapist ideallyaddressing catastrophic cognitions about thedisorder (Hinton, Lewis-Ferna¤ ndez, et al., inpress).Make CBT techniques tolerable andcredible for the cultural groupExposure for traumamaybeparticularly pro-blematic. It has been found that conductingexposure among ethnic populations presentschallenges andmay lead to drop-out andwor-sening (Hinton, 2012). With western popu-lations, even when conducted by a doctorallevel therapist, this approach has been foundtobeproblematic (Hinton,2012). But narrativeexposure therapy uses traditional exposure—minimal preparation or modi¢cation—andhas been shown to be e¡ective in severalcountries (Morkved et al., 2014). Comparativestudies of traditional exposure approachescompared to phase and modi¢ed approachesneeds to be donewith refugees having a rangeof severityoftrauma,of levelofcurrentanxietyandof current stressors.To increase exposure tolerability, a phaseapproach and other methods have beensuggested. Metaphors used to frame treat-ment may promote acceptance (Hintonet al., 2012b; Hwang, 2006). For example,some researchers have employed analogies to
ht © War Trauma Foundation. Unautho86
make exposure more tolerable and to createpositive expectancy: one group con¢guredimaginal exposure as cleaning a wound andcompared fear of exposure to the fear localwomen initially have of making bread on anopen ¢re, a fear that diminishes over time(Murray et al., 2014). In our treatment, toincrease tolerability and e⁄cacy, we use thedistress resulting from exposure as an oppor-tunitytoteachemotion-regulationtechniques(Hinton et al., 2012b), with these emotion-regulation techniques informed by the localculture. To increase tolerability of interocep-tive exposure, we frame the techniques as a‘game’and try to create positive associationsto somatic sensations; for example, duringhead rolling, evoking the joy experienced bya child while rolling down a hill and alsofeeling dizziness.Utilise culturally appropriate meta-phors and proverbs This increasesacceptability and positive expectation, andit helps in the retention of taught infor-mation.Thesemetaphorsmaybe taken fromthe religious tradition. For example, inCambodian Buddhism, anger is comparedto a dangerous ¢re, which one should notbring into the house, and there is theproverb, ‘Not getting angry once results in a
hundred days of happiness’ (Nickerson &Hinton, 2011). These sorts of analogies andproverbs canbe used in treatment. Likewise,anger is highly discouraged in the Islamictradition. For example, it is told that theProphet of Islam, Muhammad, advised,‘The strong man is not the one who can throw
another down. The strong man is the one who
can keep hold of himself when he is angry’ and‘Anger is from Satan, and Satan was created from
¢re. Fire is extinguished bywater, so if one of yougets
angry, he/she should performWudhu’ (ritualisticwashing of face, arms and feet; i.e. to cooldown). We would consider these uses ofmetaphor and proverb as other examples ofexplanatory model bridging—of bridgingbetween the clinician’s and patient’s view ofdisorder.This might be calledmetaphor- andproverb-type bridging.
rized reproduction of this article is prohibited.

Copyrig
Hinton&Jalal
Identify issues of therapist^clientmatching This is particularly importantin respect to gender. For example, in sometraditional cultures, such as in some Islamiccultures, the therapist should ideally be ofthe same gender as the patient, to reducesocial uneasiness (Murrayet al.,2014). If gen-der matching cannot be achieved, a thirdperson should be present during treatmentsessions (preferably of the same gender asthe patient), to make the patient feel moreat ease. In respect to cultural matching,one study (Benish et al., 2011) suggested thatexplanatory model matching was the keytherapeutic element: the therapist’s elicita-tion of the patient’s explanatory model andthe creation of an explanatory model oftreatment acceptable to the patient, whichwe have referred to as explanatory modelbridging.Increase credibility and positiveexpectancyThis will be achieved by var-ious means such as stating that treatmentwill helpwith symptoms of greatest concern,like cultural syndromes and somatic com-plaints such as dizziness or poor appetite.Showing videos of those who have becomebetter through the treatment may helpimprove credibility/expectancy; videos oflocal leaders who advocate treatment andattest to its e⁄cacymayhave the same e¡ect.Credibility/expectancy may be enhancedby framing the treatment as incorporatinglocal therapeutic techniques such as medita-tion in a Buddhist context and Dhikr andRuqyah in an Islamic context. Credibilityand positive expectancy will arise in largepart fromthe credibility andpositive expect-ancy of key CBT techniques, which can bemaximised by appropriate framing. Credi-bility and expectancy canbe built by certaindescriptions of the entire treatment, andabout speci¢c elements. For example, in ourtreatment, we compare the treatment tothe making of a special local dish thatinvolves multiple culinary steps in orderto promote positive expectancy and toteach patience about the time frame of
ht © War Trauma Foundation. Unautho
improvement. Multiple studies indicatehow positive expectancy increases e⁄cacy(Rutherford & Roose, 2013; Tsai, Ogrodnic-zuk, Sochting, & Mirmiran, 2014).
Maximise accessDescribe how and where the patient wasidenti¢ed and recruited in the healthcare systemIt is important to specify how patients wererecruited, such as in a mental health clinic,aprimarycare setting or other location.Thisgives insight into the nature of the healthcare system and gives information aboutthe generalisability to other contexts (Jor-dans & Tol, 2013).Address stigma about the disorderand getting treatment for the disorderOne should determine how various psycho-logical disorders are viewed in the treatmentlocality. The order should be normalised asmuch as possible. This helps to reduce self-stigma and stigmatisation by others. It maybe necessary to educate family members.Videos of patients and community leadersin which they talk about the disorder andthe importance of treatment may help. Itmay be necessary to frame the treatment asaddressing locally salient concerns that arenot stigmatising, such as poor sleep, night-mares or somatic complaints. It may be thatcoming to the location of treatment is stig-matising. This may lead to the need to dothe treatment in aprimarycare orother non-stigmatising locality. In this category, onewould place various types of social blamingand self-blaming. In some localities, the vic-tim may be blamed (e.g. in the case of rape)and stigmatised. Or also, in many Asiancountries, the concept of karma (i.e. the ideathat what happens to one is a result of pastbad actions and so is deserved) can have thise¡ect. So for example, in the case of thekarma explanation, various techniques canbe used. If the personthinks the current stateis due to ‘low merit’ or past bad actions(‘bad karma’), ideally cultural means used
rized reproduction of this article is prohibited.87

Copyrig
Guidelines for the implementation of culturally sensitive CBTamong refugees and in global contexts
Intervention 2014, Volume 12, Supplement 1, Page 78 - 93
to elevate spiritual status canbe encouraged:in Buddhism, an act such as meditating orprojecting loving kindness are consideredmerit-making. By doing these activities, thepatient regains a sense of agency (there is atransformation of self-image), and thepatient engages in a practice that is thera-peutic by both local and ‘scienti¢c’ stan-dards. (Note that addressing stigma is oftenpart of addressing catastrophic cognitions,because the perception of low spiritualpower and great vulnerability leads tomultiple types of catastrophic cognitions.)This is another example of explanatorymodel bridging: one uses local explanatoryframes to convince the patient to engage inpractices that, from the current state ofpsychological science, are considered to bee¡ective. It should be noted that localmodels such as that of karma may be usedas a justi¢catory frame for perpetration ofviolence and need to be addressed at thecommunity level. More generally, stigmatis-ation of a victim may need to be addressedat such a level, such as through ¢nding groupconsensus and ¢nding local religious andtransnational human rights frames.Address structural barriers to treat-ment These include transportation issues,payment issues and the ability to take timeo¡ to go to the clinic.Maximise adherenceWhatever increasescredibility and expectancy will tend toincrease adherence. Also, adherence, suchas not dropping out or missing sessions, willrelate to various other issues such as stigmaabout treatment and structural barriers, forexample, lack of transportation or inabilityto take time o¡ from a busy work schedule.A person may attend sessions but not actu-ally do homework or other potentially help-ful aspects of a treatment, which is anotherexample of nonadherence. Metaphors thatemphasise the need to complete all partsof the treatment, like those in which allelements of the treatment are analogised toall the steps needed to prepare a dish that ishighly prized in the culture, may help to
ht © War Trauma Foundation. Unautho88
increase adherence, and adherence will beincreasedby anything that decreases stigma,helps to increase credibility/expectancy, ortolerability, or addresses structural barriers.Specify scale-up and sustainabilitypotential Scale-up and sustainability willbe greatly in£uenced by the level of edu-cation required of the service provider, howmuch time is needed to be trained, whetherthe treatment can be taught to multiple pro-viders, how many sessions the treatmententails, whether the treatment is based on agroup or individual and whether it allowstask shifting (Lancet Global Mental HealthGroup et al., 2007; Patel, 2012). In addition,the scale-up and sustainability potential willbe in£uenced by public health system vari-ables: by whether there is a place in thehealth care system to situate the treatment,whether the government is willing to incor-porate the CBT into standard treatmentand whether there is funding available forthe programme (Jordans & Tol, 2013).
ConclusionsAs reviewed above, recent studies show thepotential of CBTamong refugees and othergroups in various global contexts. We haveattempted to outline somekey ways of imple-menting CBTamong refugees and in globalcontextsmore generally tomake it culturallysensitive so as tomaximise e⁄cacyande¡ec-tiveness. In studies involving implementa-tion of CBT among refugees and in globalcontexts, the guidelines outlined this article(see Figure1) canbe usedas a sortof checklistof cultural sensitivity. (The parameters arealso applicable to studies of ethnic minoritypopulations.) Here we consider culture in abroad sense that includes context, that is,context-sensitive CBT. Elsewhere, we havereferred to ignoring parameters such as out-lined in this study (Figure 1) as an error of
decontextualisation (Hinton & Good, in press;Hinton & Hinton, in press). So the currentstudy might also be considered a delineationof parameters of contextually sensitive CBT.
rized reproduction of this article is prohibited.

Copyrig
Hinton&Jalal
The type of information speci¢ed in Figure1can be gathered in various ways. It may bethrough a review of the literature, discussionwith community leaders, ethnographic sur-veys and pilot studies in a population. Also,the treatment itself may involve askingparticipants about these domains. Forexample, in our treatment (Hinton et al.,2012b), we speci¢cally ask participantswhether they are using any other means tocope with distress, such as local religiouslyinformed techniques, and we use probes toelicit local catastrophic cognitions and keysomatic complaints. As one approach tobegin to elicit this information, the explana-tory module from the cultural formulationcould be used to assess the typical presentingcomplaint of the population in question(Hinton, Lewis-Ferna¤ ndez, et al., in press).As indicated above, we have developed a‘thinking a lot’ questionnaire to assess thatconstruct in various cultural contexts, andthe questionnaire can also be adapted toassess any complaint (Hinton, Reis, et al.,in press). In localities where ‘thinking a lot’is common, using the questionnaire is a goodway to learn about the local ethnopsych-ology, ethnophysiology, and current stressors.In summary, the treatment developer canreview the parameters presented in thisarticle to further re¢ne treatment at eachstage of the treatment’s development and totry to address each of the indicatedparameters of culturally sensitive treatment.The parameters can also be used to assessthe cultural sensitivity of CBT treatmentsand treatment studies. Aswe have suggested,in designing a treatment, a good initial start-ing point is the determination of commonpresenting key complaints within a com-munity; then the relationship of the com-plaint to DSM disorders and dimensions ofpathology should be determined, and thecomplaint evaluated in respect to localunderstanding such as perceived cause,how it disturbs the psychological, physiologi-cal and spiritual state and how it is thoughtto be best treated. Then all the parameters
ht © War Trauma Foundation. Unautho
shown in Figure 1 can be progressivelyassessed and designed.Certain limitations of the current article,and future research directions, should benoted. The extent to which culturally sensi-tive CBT as operationalised in this publi-cation improves e⁄cacy needs to bedetermined. One meta-analytic review(Benish et al., 2011) gave support forincreased e⁄cacy with cultural adaptationof treatment elements, in particular, elicitingthe patient’s explanatory model of the dis-order; however, more studies need tobe doneto see how and why the various parametersof culturally sensitive CBT improve treat-ment outcome. The current study is basedon data mainly from studies in Asian popu-lations (mainly, Southeast Asian), thoughwe also refer to work with other culturalgroups: Latinos and certain Middle Easterngroups. Applicability to other culturalgroups needs further investigation.
ReferencesAgger, I., Igreja,V.,Kiehle,R.&Polatin, P. (2012).Testimony ceremonies in Asia: Integrating spir-ituality in testimonial therapy for torture survivorsin India, Sri Lanka, Cambodia, and the Philip-pines.Transcultural Psychiatry, 49(3^4), 568-589.
Amer,M.&Jalal, B. (2011). Individualpsychother-apy/counseling: Psychodynamic, cognitive beha-vioral and humanistic-experiential model. In: S.Ahmed & M. Amer (Eds.), Counseling Muslims:
Handbook of mental health issues and interventions.
NewYork: Routledge.
Bass, J.K.,Annan, J.,McIvorMurray, S.,Kaysen,D., Gri⁄ths, S., Cetinoglu, T., . . . Bolton, P. A.(2013). Controlled trial of psychotherapy for Con-golese survivors of sexual violence. New England
Journal ofMedecine, 368(23), 2182-2191.
Benish, S. G., Quintana, S. & Wampold, B. E.(2011). Culturally adapted psychotherapy and thelegitimacy of myth: A direct-comparison meta-analysis. Journal of Counseling Psychology, 58(3), 279-289.
rized reproduction of this article is prohibited.89

Copyrig
Guidelines for the implementation of culturally sensitive CBTamong refugees and in global contexts
Intervention 2014, Volume 12, Supplement 1, Page 78 - 93
Bolton, P., Michalopoulos, L., Ahmed, A. M.,Murray, L. K.& Bass, J. (2013).Themental healthand psychosocial problems of survivors of tortureandgenocide inKurdistan,Northern Iraq:Abriefqualitative study.Torture, 23(1),1-14.
Bolton,P.,Surkan,P.J.,Gray,A.E.&Desmousseaux,M. (2012).Themental healthandpsychosocial e¡ectsoforganizedviolence:Aqualitative study innorthernHaiti.Transcultural Psychiatry, 49(3^4), 590-612.
Casey, B. J., Craddock, N., Cuthbert, B. N.,Hyman, S. E., Lee, F. S. & Ressler, K. J. (2013).DSM-5 and RDoC: Progress in psychiatryresearch? [Review]. Nature Reviews: Neuroscience,
14(11), 810-814.
DeJong, J.T., Komproe, I. H., Spinazzola, J., vander Kolk, B. S. & van Ommeren, M. H. (2005).DESNOS in three postcon£ict settings: Assessingcross-cultural construct equivalence. Journal of
Traumatic Stress, 18,13-21.
De Jong, J. T. & Reis, R. (2010). Kiyang-yang, aWest-African postwar idiom of distress. Culture,Medicine, and Psychiatry, 34, 301-321.
DeJong, J.T. & Reis, R. (2013). Collective traumaresolution: Dissociation as a way of processingpost-war traumatic stress in Guinea Bissau.Trans-cultural Psychiatry, 50, 644-661.
Drozdek, B., Kamperman, A. M., Tol, W. A.,Knipscheer, J. W. & Kleber, R. J. (2014). Seven-year follow-up study of symptoms in asylum seek-ers and refugees with PTSD treated withtrauma-focused groups. Journal of Clinical Psychol-ogy, 70(4), 376-387.
Dyregrov, A., Gupta, L., Gjestad, R. & Raunda-len,M. (2002). Is the culture always right?Trauma-tology, 8,135-145.
Gone, J. P. (2013). Redressing First Nations histori-cal trauma: Theorizing mechanisms for indigen-ous culture as mental health treatment.Transcultural Psychiatry, 50, 683-706.
Hinton, D. E. (2012). Multicultural challenges inthe delivery of anxiety treatment. Depression andAnxiety, 29,1-3.
ht © War Trauma Foundation. Unautho90
Hinton, D. E., Chhean, D., Pich,V., Safren, S. A.,Hofmann, S. G. & Pollack, M. H. (2005). Arandomizedcontrolled trial of cognitive-behaviortherapy for Cambodian refugees with treatment-resistant PTSD and panic attacks: A cross-overdesign. Journal ofTraumatic Stress, 18(6), 617-629.
Hinton, D. E. & Good, B. J. (in press).The cultu-rally sensitive assessment of trauma: Elevenanalytic perspectives, a typology of errors, andthe multiplex models of distress generation. In D.E. Hinton & B. J. Good (Eds.), Culture and PTSD:Trauma in historical and global perspective. Philadel-phia, PA: University of Pennsylvania Press.
Hinton, D. E. & Good, B. J. (Eds.). (2009). CultureandPanicDisorder. PaloAlto, CA: StanfordUniver-sity Press.
Hinton, D. E. & Hinton, A. L. (in press). Ananthropology of the e¡ects of genocide and massviolence: Memory, symptom, and recovery. In D.E.Hinton&A.L.Hinton (Eds.),GenocideandMass
Violence:Memory, symptom, and recovery. Cambridge:Cambridge University Press.
Hinton, D. E., Hinton, A. L., Eng, K.-T., &Choung, S. (2012a). PTSD and key somaticcomplaints and cultural syndromes amongrural Cambodians: The results of a needs assess-ment survey. Medical Anthropology Quarterly, 29,147-154.
Hinton,D.E.,Hofmann,S.G.,Pitman,R.K.,Pol-lack, M. H. & Barlow, D. H. (2008). The panicattack^PTSDmodel: Applicability to orthostaticpanic among Cambodian refugees. Cognitive Beha-viourTherapy, 27,101-116.
Hinton, D. E., Hofmann, S. G., Pollack, M. H. &Otto, M. W. (2009). Mechanisms of e⁄cacy ofCBT for Cambodian refugees with PTSD:Improvement in emotion regulation and ortho-static blood pressure response. CNSNeuroscience andTherapeutics, 15(3), 255-263.
Hinton,D.E.,Hofmann,S.G.,Rivera,E.,Otto,M.W.& Pollack, M. H. (2011a). Culturally adapted CBTfor Latino women with treatment-resistant PTSD:A pilot study comparing CA-CBT to Applied
rized reproduction of this article is prohibited.

Copyrig
Hinton&Jalal
Muscle Relaxation. Behaviour Research andTherapy, 49,275-280.
Hinton, D. E. & Kirmayer, L. J. (2013). Localresponses to trauma: Symptom, a¡ect, and heal-ing.Transcultural Psychiatry, 50, 607-621.
Hinton, D. E., Kredlow,M. A., Pich,V., Bui, E. &Hofmann, S.G. (2013a).The relationship of PTSDto key somatic complaints andcultural syndromesamong Cambodian refugees attending a psychia-tric clinic: The Cambodian Somatic Symptomand Syndrome Inventory (SSI).Transcultural Psy-chiatry, 50, 347-370.
Hinton, D. E. & Lewis-Ferna¤ ndez, R. (2010).Idioms of distress among trauma survivors: Sub-types and clinical utility. Culture,Medicine, and Psy-
chiatry, 34, 209-218.
Hinton, D. E. & Lewis-Ferna¤ ndez, R. (2011). Thecross-cultural validity of posttraumatic stress dis-order: Implications for DSM-5. Depression and
Anxiety, 28,783-801.
Hinton,D. E., Lewis-Ferna¤ ndez,R.,Kirmayer, L.J., & Weiss, M. (in press). Illness explanations.In R. Lewis-Ferna¤ ndez, N. Aggarwal, L.Hinton, D. Hinton, & L. J. Kirmayer (Eds.),The
DSM-5 Handbook on the Cultural Formulation
Interview. Washington DC: American PsychiatricPress.
Hinton, D. E., Nickerson, A. & Bryant, R. A.(2011b).Worry, worry attacks, and PTSD amongCambodian refugees: A path analysis investi-gation. Social Science andMedicine, 72,1817-1825.
Hinton, D. E., Ojserkis, R., Jalal, B., Peou, S. &Hofmann, S. G. (2013b). Loving kindness to treattraumatized refugees and minority groups:A typology of mindfulness and the NodalNetwork Model (NNM) of A¡ect and A¡ectRegulation. Journal of Clinical Psychology, 69, 817-828.
Hinton, D. E., Pham,T., Tran, M., Safren, S. A.,Otto,M.W.&Pollack,M.H. (2004). CBTforViet-namese refugees with treatment-resistant PTSD
ht © War Trauma Foundation. Unautho
andpanic attacks:Apilot study.JournalofTraumaticStress, 17(5), 429-433.
Hinton,D.E., Pich,V.,Hofmann, S.G.&Otto,M.W. (2013c). Mindfulness and acceptance tech-niques as applied to refugee and ethnic minoritypopulations: Examples from culturally adaptedCBT (CA-CBT). Cognitive and Behavioral Practice,
20, 33-46.
Hinton, D. E., Pich,V.,Marques, L., Nickerson, A.&Pollack,M.H. (2010).Khya“ lattacks:Akey idiomofdistress amongtraumatizedCambodia refugees.Culture,Medicine, and Psychiatry, 34, 244-278.
Hinton, D. E., Reis, R., & deJong, J.T. (in press).The ‘thinking a lot’ idiom of distress and PTSD:An examination of their relationship among trau-matizedCambodian refugees using the‘Thinkinga Lot’ Questionnaire. Medical Anthropology Quar-
terly.
Hinton,D.E.,Rivera,E.,Hofmann,S.G., Barlow,D. H. & Otto, M.W. (2012b). Adapting CBT fortraumatized refugees and ethnic minoritypatients: Examples from culturally adapted CBT(CA-CBT).Transcultural Psychiatry, 49, 340-365.
Hwang, W. C. (2006). The psychotherapy adap-tation and modi¢cation framework: Applicationto Asian Americans. American Psychologist, 61(7),702-715.
Jordans,M. J.&Tol,W.A. (2013).Mental health inhumanitarian settings: Shifting focus to care sys-tems. International Health, 5(1), 9-10.
Kaiser, B., McLean, K., Kohrt, B. A., Hagaman,A., Wagenaar, B., Khoury, N., . . . Keys, H.M.(2014). Re£echi tw˚p^thinking too much: Descrip-tion of a cultural syndrome in Haiti’s Central Pla-teau.Culture,Medicine, andPsychiatry, 38(3),448-472.
Kohrt, B. A. (in press). The role of traditionalrituals for reintegration and psychosocial well-being of child soldiers in Nepal. In D. E. Hinton& A. L. Hinton (Eds.), Genocide and MassViolence:
Memory, symptom, and recovery. Cambridge: Cam-bridge University Press.
rized reproduction of this article is prohibited.91

Copyrig
Guidelines for the implementation of culturally sensitive CBTamong refugees and in global contexts
Intervention 2014, Volume 12, Supplement 1, Page 78 - 93
Kohrt, B. A., Maharjan, S. M., Timsina, D. &Gri⁄th, J. L. (2012). Applying Nepali ethnopsy-chology to psychotherapy for the treatment ofmental illness and prevention of suicide amongBhutanese refugees. Annals of Anthropological Prac-tice, 36, 88-112.
Lancet Global Mental Health Group, Chisholm,D., Flisher, A. J., Lund, C., Patel,V., Saxena, S.,. . . Tomlinson, M. (2007). Scale up services formental disorders: A call for action. Lancet,370(9594),1241-1252.
Lester, K., Resick, P. A.,Young-Xu,Y. & Artz, C.(2010). Impact of race on early treatment termin-ation and outcomes in posttraumatic stress dis-order treatment. Journal of Consulting and ClinicalPsychology, 78(4), 480-489.
Lewis-Ferna¤ ndez, R., Raggio, G. A., Gorritz, M.,Duan, N., Marcus, S., Cabassa, L. J., . . . Hinton,D. E. (2013). GAP-REACH: A checklist to assesscomprehensive reporting of race, ethnicity, andculture in psychiatric publications. Journal of Ner-vous andMental Disease, 201(10), 860-871.
McNally, R. J. (2012). The ontology of posttrau-matic stress disorder: Natural kind, social con-struction, or causal system? Clinical Psychology
Science and Practice, 19(3), 220-228.
Morkved, N., Hartmann, K., Aarsheim, L. M.,Holen, D., Milde, A. M., Bomyea, J., . . .Thorp,S. R. (2014). A comparison of Narrative ExposureTherapy and Prolonged Exposure therapy forPTSD. [Review]. Clinical Psychology Review, 34(6),453-467.
Morris, S. E. & Cuthbert, B. N. (2012). ResearchDomain Criteria: Cognitive systems, neural cir-cuits, and dimensions of behavior. Dialogues in
Clinical Neuroscience, 14(1), 29-37.
Murray, L.K., Dorsey, S., Haroz, E., Lee, E., Alsi-ary, M. M., Haydary, A., . . . Bolton, P. (2014). Acommon elements approach for adult mentalhealth problems in low- and middle-incomecountries.CognitiveandBehavioralPractice, 21,111-123.
ht © War Trauma Foundation. Unautho92
Nezu, A.M., Nezu, C.M.&Lombardo, E. (2004).Cognitive-behavioral Case Formulation to Treatment
Design a Problem-solving Approach. New York, NY:Springer.
Nickerson, A. &Hinton, D. E. (2011). Anger regu-lation in traumatized Cambodian refugees: Theperspectives of Buddhist Monks. Culture,Medicine,
and Psychiatry, 35, 396-416.
Patel, V. (2012). Global mental health: Fromscience to action. Harvard Review of Psychiatry,
20(1), 6-12.
Patel, V., Simunyu, E. & Gwanzura, F. (1995).Kufungisisa (thinking too much): A Shona idiomfor non-psychotic mental illness. Central AfricanJournal ofMedicine, 41(7), 209-215.
Rutherford, B. R.&Roose, S. P. (2013). Amodel ofplacebo response in antidepressant clinical trials.AmericanJournal of Psychiatry, 170(7),723-733.
Tsai, M., Ogrodniczuk, J. S., Sochting, I. & Mir-miran, J. (2014). Forecasting success: Patients’expectations for improvement and their relationsto baseline, process and outcome variables ingroup cognitive-behavioural therapy for depres-sion. Clinical Psycholology and Psychotherapy, 21(2), 97-107.
VanGinneken,N.,Tharyan, P., Lewin, S.,Rao,G.N., Meera, S., Pian, J., . . . Patel, V. (2013). Non-specialist healthworker interventions for the careof mental, neurological and substance-abuse dis-orders in low- and middle-income countries.CochraneDatabase of Systemic Reviews, 11, CD009149.
Ventevogel, P., Jordans, M., Reis, R. & deJong, J.(2013). Madness or sadness? Local concepts ofmental illness in four con£ict-a¡ected Africancommunities. Con£ict and Health, 7(1), 3.
1 DSM=Diagnostic and StatisticalManual ofMental
Disorders Arlington, VA: American PsychiatricAssociation.
rized reproduction of this article is prohibited.

Copyrig
Hinton&Jalal
2 Interoceptive exposure is a cognitive beha-vioural therapy technique used in the treatmentof panic disorder in which the individual isexposed to interoceptive sensations like dizzinessto decrease fear of them.
ht © War Trauma Foundation. Unautho
Devon E. Hinton, MD, PhD is a psychiatrist and a
Psychiatry at Massachusetts General Hospital and i
at HarvardMedical School. email: devon_hinton@h
3 Etic and emic refer to two kinds of view-points; etic is the universalistic model andthe emic model is that from within thesocial group, that is, from the perspective ofthe subject.
rized reproduction of this article is prohibited.
n anthropologist who is an Associate Professor of
n the Department of Global and Social Medicine
ms.harvard.edu
93

![Theory of Planned Behavior, Self‑Stigma, and Perceived ...file.qums.ac.ir/repository/sdh/Theory of Planned...self-stigma (also known as internalized stigma).[5,6] Self-stigma was](https://img.dokumen.tips/doc/110x75/5f59324ffcada40fd01f4b2a/theory-of-planned-behavior-selfastigma-and-perceived-filequmsacirrepositorysdhtheory.jpg)