Embed Size (px)
Citation preview

MEDICAL EDUCATION
Gross Anatomy Dissections and Self-DirectedLearning in Medicine
Ma DEL MAR ARROYO-JIMENEZ,1 PILAR MARCOS,1 ALINO MARTINEZ-MARCOS,1
EMILIO ARTACHO-PERULA,1 XAVIER BLAIZOT,1 MONICA MUNOZ,1
Ma TERESA ALFONSO-ROCA,2 AND RICARDO INSAUSTI1*
1Department of Health Sciences, Human Anatomy and Embryology Section, School of Medicine, University of Castilla-La Mancha, Spain2Medical Education Unit, School of Medicine, University of Castilla-La Mancha, Spain
The Medical School of the University of Castilla-La Mancha (UCLM, Albacete Spain)was launched in 1998 and is the most recent one in Spain. Teaching is based on smallgroups of students (20–25 students/group). An objective-oriented self-learning approachprovides maximal autonomy and independence in the achievement of objectives by the stu-dents in close association with academic staff. Gross Anatomy courses take place in thefirst and second years. The one in the first year is a single 10-credit course, where onecredit equals 10 hr of teaching activity. In the second year, Anatomy and Embryology areintegrated with Physiology and Histology, and comprise 70 credits altogether. In addition,all students carry out two mandatory gross anatomical dissections per year, in groups ofthree students, to allow direct handling of human anatomical material. Students are pro-vided with handouts containing general instructions on how to perform the dissection andthe structures (items) that they must expose in a given period of time (4 hr). Afterward, aFaculty member checks the number of items demonstrated and the quality of the dissec-tion. Each group submits a written report that contributes to the final score. We evaluatedthe number of items shown in each of two consecutive dissections for first and second yearmedical students. The data obtained indicate that students engaged in self-directed learningthrough small groups working with Faculty staff are able to self-improve their anatomicalskills. Clin. Anat. 18:385–391, 2005. VVC 2005 Wiley-Liss, Inc.
Key words: medical education; self-learning; modules; objectives; grossanatomy
INTRODUCTION
General Principles of Learning at the School of
Medicine of the University of Castilla-La Mancha
The educational goal of the School of Medicine
of the University of Castilla-La Mancha (UCLM) is
the development of a curriculum to produce medical
graduates who will be fully integrated in terms of
medical knowledge, technical proficiency and social
understanding. Our approach is an advance from the
traditional medical educational system, almost uni-
versally based on lectures, used by most of the med-
ical schools in Spain (Gomez and Pujol, 1998). The
UCLM uses an integrated learning model based on
the development of professional competencies as the
core of the medical curriculum. Although this educa-
tional method is used currently in more than 120
Medical Schools worldwide, it has not been adopted
widely in Europe.
The medical curriculum of the Medical School of
the UCLM is based on three main conceptual foun-
dations: (1) integration of disciplines, (2) active
learning methodology based on objectives, and (3)
*Correspondence to: Dr. Ricardo Insausti, Department of Health
Sciences, School of Medicine, University of Castilla-La Mancha,
Avda. de Almansa s/n, 02006 Albacete, Spain.
E-mail: [email protected]
Received 15 April 2004; Revised 22 July 2004; Accepted 29
December 2004
Published online inWiley InterScience (www.interscience.wiley.com).
DOI10.1002/ca.20129
VVC 2005 Wiley-Liss, Inc.
Clinical Anatomy 18:385–391 (2005)
problem-based learning (PBL), the main method of
education used widely in our clinical courses and
more sparingly on basic sciences (preclinical)
courses.
This educational approach emphasizes the active
participation of the students in developing autonomy
in their own learning process, as well as promoting
motivation and interest in the different topics of the
medical curriculum. The students are responsible for
their own learning, avoiding the passive attitude seen
in many students that follow the lecture system. This
approach is, basically, practice-oriented, and it aims
to integrate the biological, clinical, and psychosocial
sciences. The ultimate goal of this system is, there-
fore, the promotion of: (1) independent learning, (2)
communication skills and team-work among students,
and (3) integration of the basic and clinical sciences,
all three prepare students for the clinical decisions
they will take in medical practice in an atmosphere
of responsibility and guided by tutors.
Academic staff at the Medical School of the
UCLM guide the learning process of the students,
encouraging at all times self-learning, instead of lec-
turing on their own discipline. To achieve its goal,
the medical curriculum at the School of Medicine of
the UCLM tries to potentiate the active participa-
tion of students in every possible aspect of their
education.
The medical curriculum at the Medical School of
the UCLM is 6 years long (mandatory by law in
Spain). The number of students is 80 per year, div-
ided into groups of 20 students for basic courses,
and six for clinical ones.
The curriculum is arranged in modules of objec-
tives. Each module lasts for 2 or 3 weeks and con-
sists of five distinct phases. Phase I starts by careful
reading of the objectives, after which the students
are guided in the understanding of terms and con-
cepts germane to the objectives of the module. The
students pose questions, phrasing them clearly under
the supervision and guidance of academic staff. The
identification of the objective, its conceptual rela-
tionship to other objectives of the module, and the
educational resources required are strongly empha-
sized, aiming at achieving time-efficient work. Phase
2 is devoted to the students’ individual work to
achieve the objectives, with the help of complemen-
tary activities, mostly laboratory practicals. Phase 3 is
the period in which the students, usually a single
student or in groups of up to three students, present
to their peers the main content related to each
objective, supervised by Faculty staff. Participation
and active discussion by the students is encouraged
at all times to develop communication skills. Phase
4 is a self-learning period in which students have
the opportunity to request individual tutorials to
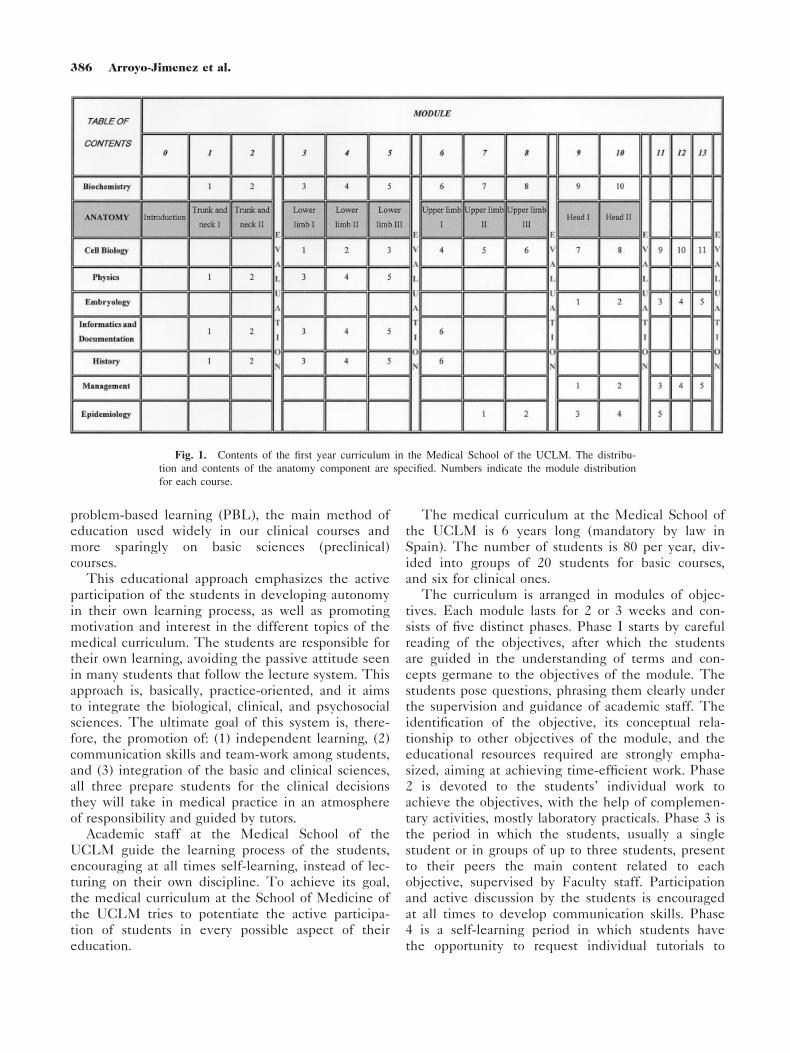
Fig. 1. Contents of the first year curriculum in the Medical School of the UCLM. The distribu-
tion and contents of the anatomy component are specified. Numbers indicate the module distribution
for each course.
386 Arroyo-Jimenez et al.
clarify particular questions. Students can request as
many tutorials and complementary activities as they
deem necessary. In Phase 5, students take a multiple
choice test to evaluate a single module or a number
of modules in a given unit (a unit is a number of
regions anatomically related to a function, i.e., upper
limb and manipulation) (Figs. 1,2). Additional
selected lectures (one per unit) are also given to the
entire class.
The practical approach of both the basic and clini-
cal subjects is emphasized. For instance, beginning
at the second year, students attend family medicine
courses in community health centers concurrent with
basic science courses. In this way, students receive
an early exposure to the social aspects of their future
medical practice.
HUMAN ANATOMY AND EMBRYOLOGYAT THE UCLM
Traditionally, Human Anatomy and Embryology
was taught by lectures and laboratories. Because we
are experiencing an information era, with escalating
development of computer resources, appraisal of the
students’ approach and the methodology of teaching
seems necessary. This represents an enormous chal-
lenge to medical educators, particularly in the field
of the Human Anatomy and Embryology, where
imaging (X-ray, magnetic resonance imaging, compu-
terized tomography, etc.) forms an important part of
the learning materials. The enormous explosion of
molecular and cellular biology in modern medicine
has led to a decrease of time devoted to Anatomy
and Embryology (Yates, 1999; Paalman, 2000). We
need, therefore, to use time allocated to our subject
effectively. One of the institutional goals at the
School of Medicine of the UCLM is an increasingly
better medical education by directing student time
and effort efficiently.
Human Anatomy and Embryology are taught with
other preclinical courses (e.g., cell biology) under
the perspective of different levels of organization of
the human body: macroscopic, microscopic, and sub-
cellular (horizontal integration) and oriented toward
future clinical courses (vertical integration). During
the first year, ‘‘Topographical Anatomy,’’ which
comprises the Locomotor System, is presented as a
10-credit course (one credit equals 10 hr of lectures
or laboratory practicals, 100 hr in total). It is arranged
as 11 modules of objectives (Fig. 1). Topographical
Anatomy starts with an introductory module of gene-
ral principles and nomenclature. This is followed
by four main units or sections. Each unit consists of
2–3 modules of objectives: Unit 1 comprises trunk
and neck (postural systems of the trunk and neck:
two modules); Unit 2 is devoted to the lower limb
(general posture and locomotion: three modules, one
for each segment of the leg); Unit 3 is devoted to
the upper limb (motor system for grasping: three
modules, one for each segment) and, finally, Unit 4
deals with the head (skull, mandible, facial and mas-
ticatory activities: two modules). The number of
modules is related to the division of the total time
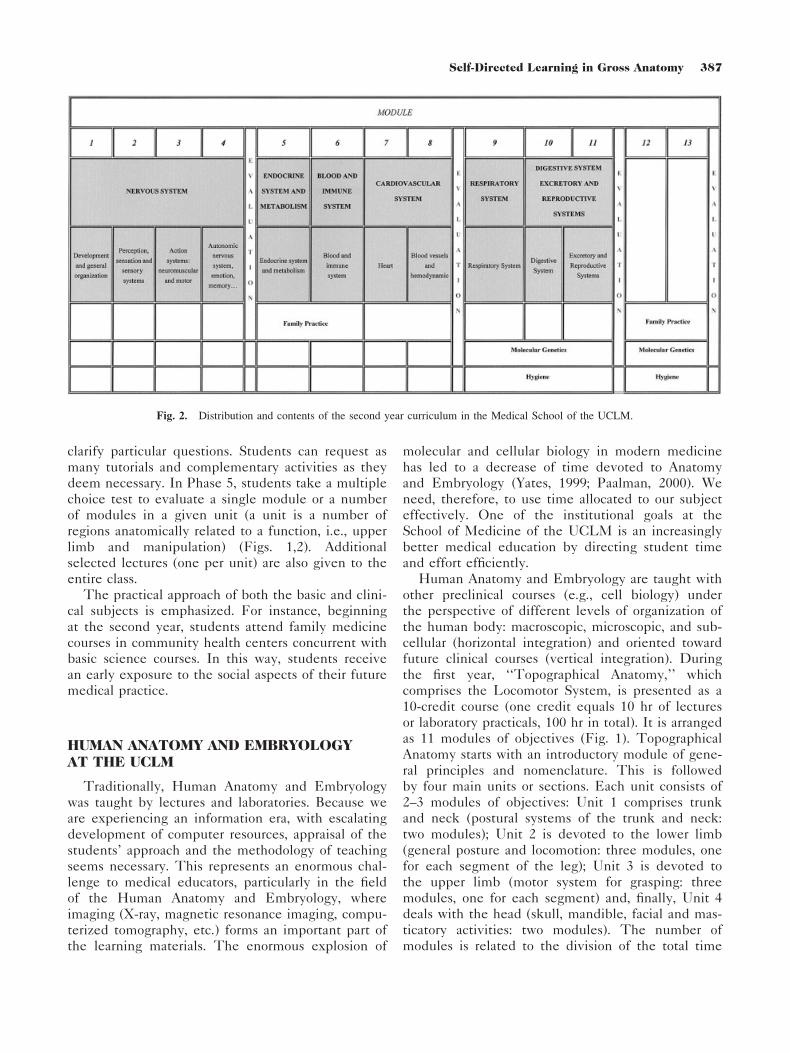
Fig. 2. Distribution and contents of the second year curriculum in the Medical School of the UCLM.
387Self-Directed Learning in Gross Anatomy

of the academic year from September to June. Func-
tional aspects of Anatomy are considered together
with sectional, radiological, and clinical examples.
Dissection courses play an important role. General
Human Embryology is presented in five modules
(Fig. 1) integrated with genetics and structure and
function of the cell (Cell Biology in Fig. 1). Those
modules include objectives that go from gametogene-
sis up to the fourth week of embryonic develop-
ment. Special Human Embryology (development of
the organs and systems) is included in the second
year in a course entitled ‘‘Development, morphol-
ogy, structure and function of the body systems in
health.’’ This course integrates in its modules of
objectives Anatomy (including Human Embryology
as stated above), Histology and Physiology in a 70-
credit course (Fig. 2, 250 hr for Anatomy and
Embryology). Students have to learn the develop-
ment and organization of the body systems, integrat-
ing anatomical, histological and physiological con-
tent. The material is organized in ‘‘units,’’ and each
unit relates to a functional system; overall, each unit
is equivalent to one module, except in those systems
where their extent requires more than one module,
(namely nervous and cardiovascular systems, with
four and two modules, respectively). The course
begins with the nervous system and is followed in
sequence by the endocrine, blood, cardiovascular,
respiratory (including phonatory apparatus), diges-
tive, and finally, in one single module, excretory and
reproductive systems.
The assessment of Human Anatomy and Embry-
ology has two parts, theoretical and practical. The
first consists of a variable number of multiple-choice
questions. In the practical examination, students are
required to pass a test based on the material avail-
able at the gross anatomy laboratory. They must rec-
ognize clearly marked structures previously selected
by the instructors using human bones, plastic mod-
els, prosections, images, etc. A maximum of 30 sec
per structure is allocated for identifying and writing
the name of the structure. All this material has been
demonstrated previously during the laboratory peri-
ods (Phases 2 and 4). The final score is the average
of all the tests.
GROSS ANATOMY DISSECTIONS
There are numerous and often divergent opinions
about effective and efficient use of dissection or pro-
sections as a part of a gross anatomy course (Utting
and Winnan, 1995; Jones, 1997; Dinsmore et al.,
1999). In general, even with the increasing availabil-
ity of computer programs and simulations of the
human body, there is a broad consensus that there is
no substitute for dissection (Ashraf-Aziz et al., 2002),
especially to understand the 3D relations of the
structures of the human body (Marks, 2000). We
believe that anatomical dissection offers a direct con-
tact with the human body and, at the same time,
provides the best workbench for students to under-
stand and learn gross anatomy.
The Anatomy Section at the Medical School of
the UCLM has implemented a curriculum in which
40% of the students’ time is devoted to regular prac-
tical anatomical sessions with both prosections and
anatomical models (Phases 2 and 4). Every module,
new prosections are prepared by the instructors to
demonstrate anatomical features related to the forth-
coming module. In addition, the students are
required to perform two gross anatomy dissections
per year of a pre-established anatomical region. The
dissection makes up to 10% of the final score. After
they acquire the theoretical concepts of the region to
be dissected, groups of three students carry out a
gross anatomical dissection with the help of a hand-
out, reference atlases, and also some general intro-
ductory information about gross anatomy dissection
procedures. Students must identify a number of ana-
tomical structures (arteries, nerves, muscles, etc.) pre-
viously determined for each dissection. They have a
maximum of four hours to identify those structures,
after which the students complete a list of the struc-
tures dissected, as well as specific problems and diffi-
culties encountered during the dissection. At the end
of the dissection time, the instructor evaluates the
degree of accomplishment of the dissection and clari-
fies students’ questions on the dissection for the
preparation of the final report. It is worth noting that
the students work on their own, and the role of the
instructor is to answer the students’ questions after
the dissection has been completed.
To validate the effectiveness of self-learning
shown in these dissections, we analyzed the results
obtained for each group of three students in the first
and second medical years. All data shown here corre-
spond to the year 2000 at the Medical School of the
UCLM. The scoring of the gross anatomical dissec-
tion was calculated as the percentage of anatomical
structures listed in the handout provided shown in
the dissection. Figure 3a shows the percentage of
items correctly identified by the students. Figure 3b
shows the same data for the second year. The mean
percentage of successfully dissected items was
always >60% with limits of 0% (one group) and
100% (11 groups). Furthermore, we have analyzed
the variation between the first and the second dis-
sections of the same group of students.
388 Arroyo-Jimenez et al.
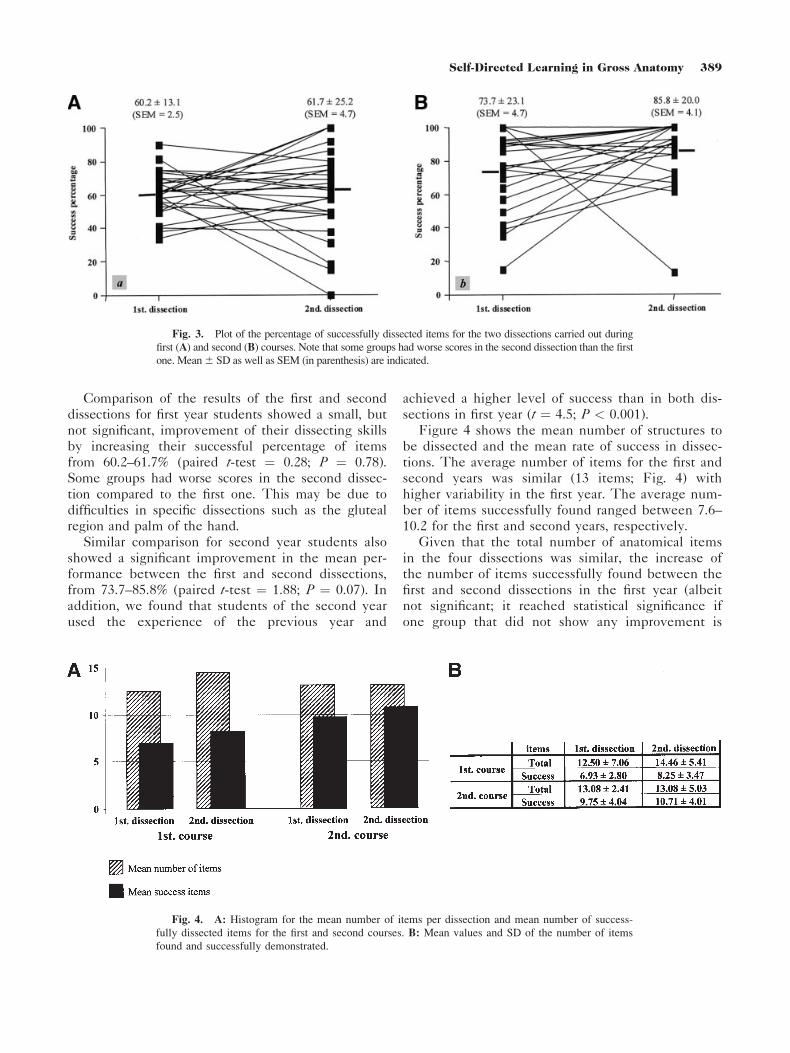
Comparison of the results of the first and second
dissections for first year students showed a small, but
not significant, improvement of their dissecting skills
by increasing their successful percentage of items
from 60.2–61.7% (paired t-test ¼ 0.28; P ¼ 0.78).
Some groups had worse scores in the second dissec-
tion compared to the first one. This may be due to
difficulties in specific dissections such as the gluteal
region and palm of the hand.
Similar comparison for second year students also
showed a significant improvement in the mean per-
formance between the first and second dissections,
from 73.7–85.8% (paired t-test ¼ 1.88; P ¼ 0.07). In
addition, we found that students of the second year
used the experience of the previous year and
achieved a higher level of success than in both dis-
sections in first year (t ¼ 4.5; P < 0.001).
Figure 4 shows the mean number of structures to
be dissected and the mean rate of success in dissec-
tions. The average number of items for the first and
second years was similar (13 items; Fig. 4) with
higher variability in the first year. The average num-
ber of items successfully found ranged between 7.6–
10.2 for the first and second years, respectively.
Given that the total number of anatomical items
in the four dissections was similar, the increase of
the number of items successfully found between the
first and second dissections in the first year (albeit
not significant; it reached statistical significance if
one group that did not show any improvement is
Fig. 3. Plot of the percentage of successfully dissected items for the two dissections carried out during
first (A) and second (B) courses. Note that some groups had worse scores in the second dissection than the first
one. Mean6 SD as well as SEM (in parenthesis) are indicated.
Fig. 4. A: Histogram for the mean number of items per dissection and mean number of success-
fully dissected items for the first and second courses. B: Mean values and SD of the number of items
found and successfully demonstrated.
389Self-Directed Learning in Gross Anatomy

removed), and in the second year, indicates that pre-
vious experience, although short, improved the score
in subsequent dissections. Likewise, comparisons of
first and second year scores showed an improvement
in the second round of dissections. The increasing
level of dissection time and experience thus allowed
a better performance, even though several months
elapsed between the first and second years.
Failure in the demonstration of assigned items may
be due to lack of interest or cooperative skills (noted
only in one single group of 3 of 160 students) or diffi-
culty in defining the depth of a structure through inad-
equate dissection by the preceding group (i.e., superfi-
cial and deep dissections of the anterior forearm). This
occurred occasionally, although usually very few items
were affected.
At the end of the dissections, students completed
a questionnaire where three questions were asked:
1. What is the value of gross dissections for the
understanding of the Anatomy course?
2. What expectations did you have of dissection?
3. What did you think about dissection?
Analysis of the questionnaires showed that most
students (47%) felt that personal experience of dissec-
tion was very useful, and that it was an efficient and
effective way of understanding and learning gross
anatomy. 32.8% stated that direct contact with a
human body helped to know the ‘‘real’’ structure.
Only 7.4% mentioned dissection as a means to
improve the final score, 6% saw dissection as a train-
ing for surgical practice, 5.8% expressed a genuine
interest in knowing dissection techniques, and 4.3%
mentioned the value of team work. In general, the
students expressed a great interest in having more ses-
sions because dissections increased comprehension of
material learned during the modules. They regarded
the dissection as putting into practice the ‘‘theory’’
presented in textbooks and atlases, and as a work-
bench for appraisal of the human body organization.
CONCLUSION
Gross anatomy is one of the fundamental topics in a
medical curriculum. In gross anatomy, we face the
well-known dilemma that at the time students have to
master a large body of anatomical information, they are
not aware of its application to clinical medicine. When
they are ready to use anatomical knowledge, a substan-
tial part of the information is forgotten. The importance
of anatomical reasoning and the application of anatomi-
cal principles in the explanation of clinical signs and
symptoms, however, is clear. The theoretical develop-
ment of the methodology we use is borne out by the
satisfaction of the students expressed in the answers to
the questionnaire. In addition, staff profited from a very
direct experience of the students’ difficulties in the
learning process in the anatomy courses, and learn how
to direct tutorials more efficiently.
Nevertheless, there is still a long way to go. Diffi-
culties found by both teachers and students relate
mainly to the identification of individual student
participation on the assigned dissections (groups
were of three students because of the number of
cadavers available) and to the evaluation system
(i.e., some items were not identified due to inappro-
priate exposure by a previous dissection). We are
now hoping to introduce individual student dissec-
tion that would allow personal assessment and
greater benefit for the students.
The Spanish medical educational system is based
on individual disciplines, most often by lectures to
large groups of students, not only in the medical cur-
riculum, but in primary and secondary schools as
well. When students enter our novel system they
usually are surprised and challenged by their active
participation and the integration of the different sub-
jects. Our system challenges students’ learning hab-
its, and requires additional effort to adapt to self-
learning, especially at the beginning of the first year.
Once they become familiar with the system, most of
them appreciate the benefits of active learning and
increase their motivation to learn. This model also
brings about a more direct interaction with Faculty
members. Additional benefits of the method are the
honing of the students’ communication skills in peer
teaching, the learning of the importance of collabora-
tive effort and the appreciation of the need to organ-
ize their thoughts for an oral presentation (Phase 3,
see Introduction), taking into account that every stu-
dent, on average, must give at least six oral presenta-
tions (peer-teaching) per academic year. Group-work
provides additional incentive to study, as well as a
preparation for future medical practice. Staff must
cope with the additional effort required in working
with students and in providing quality cooperative
teaching. This system, however, promotes integration
of the different courses in basic and clinical sciences.
In the academic year 2003/2004, the first students
have completed their medical studies under this
teaching system. After that, they take the Spanish
national examination that allows them to initiate
their specialty training. After that examination, we
will know how our students have scored. We will
then be in a better position to assess the results of
our curriculum and decide whether we ought to
implement further educational strategies in Human
390 Arroyo-Jimenez et al.

Anatomy and Embryology and their integration with
other basic and clinical sciences.
ACKNOWLEDGMENTS
This work is dedicated to Prof. J. Fermoso and to
Prof. L. Arroyo, two visionaries of the implementa-
tion of new educational approaches to medical cur-
ricula in Spain. We thank Prof. L. Branda for reading
the first draft of the manuscript.
REFERENCES
Ashraf-Aziz M, Mckenzie JC, Wilson JS, Cowie RJ, Ayeni
SA, Dunn BK. 2002. The human cadaver in the age of
biomedical informatics. Anat Rec (New Anat) 269:20–32.
Dinsmore CE, Daugherty S, Zeitz HJ. 1999. Teaching and
learning Gross Anatomy: dissection, prosection, or ‘‘both
of the above?’’ Clin Anat 12:110–114.
Gomez JM, Pujol R. 1998. Changes in medical education in
Spain. Acad Med 73:1076–1080.
Jones DG. 1997. Reassessing the importance of dissection: a
critique and elaboration. Clin Anat 10:123–127.
Paalman MH. 2000. Why teach anatomy? Anatomists
respond. Anat Rec (New Anat) 261:1–2.
Marks SC. 2000. The role of three-dimensional information
in health care and medical education: the implications for
anatomy and dissection. Clin Anat 13:448–452.
Utting M, Winnan P. 1995. What future for dissection in
courses of human topographical anatomy in universities in
the UK? Clin Anat 8:414–417.
Yates RD. 1999. The present and future of anatomy. Anat
Rec (New Anat) 257:43–44.
391Self-Directed Learning in Gross Anatomy





























