Embed Size (px)
Citation preview
Wgnjmi
r
F
MMs
Current Concepts
Glenohumeral Joint Preservation: Current Options for ManagingArticular Cartilage Lesions in Young, Active Patients
Florian Elser, M.D., Sepp Braun, M.D., Christopher B. Dewing, M.D.,and Peter J. Millett, M.D., M.Sc.
Abstract: This is a review of joint-preservation techniques for the shoulder. Whereas the management ofdiffuse articular cartilage loss in the glenohumeral joints of elderly and less active patients by totalshoulder arthroplasty is well accepted, significant controversy persists in selecting and refining successfuloperative techniques to repair symptomatic glenohumeral cartilage lesions in the shoulders of young,active patients. The principal causes of focal and diffuse articular cartilage damage in the glenohumeraljoint, including previous surgery, trauma, acute or recurrent dislocation, osteonecrosis, infection, chon-drolysis, osteochondritis dissecans, inflammatory arthritides, rotator cuff arthropathy, and osteoarthritis,are discussed. Focal cartilage lesions of the glenohumeral joint are often difficult to diagnose and requirea refined and focused physical examination as well as carefully selected imaging studies. This reviewoffers a concise guide to surgical decision making and up-to-date summaries of the current techniquesavailable to treat both focal chondral defects and more massive structural osteochondral defects. Thesetechniques include microfracture, osteoarticular transplantation (OATS [Osteochondral Autograft Trans-fer System]; Arthrex, Naples, FL), autologous chondrocyte implantation, bulk allograft reconstruction,and biologic resurfacing. As new approaches to glenohumeral cartilage repair and shoulder joint preser-vation evolve, there continues to be a heightened need for collaborative research and well-designedoutcomes analysis to facilitate successful patient care.
psgpr
avodcatsaSpt
ith an increasingly active population and withimprovements in medical technology and sur-
ical technique, there is both a need and an opportu-ity for joint-preserving surgery for the glenohumeraloint. Focal cartilage lesions of the glenoid and hu-erus have historically been underdiagnosed by clin-
cal examination and by imaging techniques, predis-
From the Steadman Hawkins Research Foundation, Vail, Colo-ado, U.S.A.
F.E., S.B., P.J.M. have received support from Arthrex, Naples,L, exceeding US $500 related to this research.Received August 27, 2009; accepted October 21, 2009.Address correspondence and reprint requests to Peter J. Millett,.D., M.Sc., Steadman Hawkins Research Foundation, 181 Weadow Dr, Ste 100, Vail, CO 81657, U.S.A. E-mail: drmillett@
teadman-hawkins.com© 2010 by the Arthroscopy Association of North America
a0749-8063/10/2605-9498$36.00/0doi:10.1016/j.arthro.2009.10.017
Arthroscopy: The Journal of Arthroscopic and Related
osing them to incidental discovery at the time ofurgery. The incidence of symptomatic Outerbridgerade II to IV lesions of the shoulder has been re-orted to be as high as 5% to 17% in patients withotator cuff tears1 or overhead athletes.2
Cartilage injury in the shoulder may be caused by orssociated with a myriad of factors that include pre-ious surgery, trauma, acute or recurrent dislocation,steonecrosis, infection, chondrolysis, osteochondritisissecans (OCD), inflammatory arthritides, rotatoruff arthropathy, and osteoarthritis. Though symptom-tic osteoarthritis of the shoulder can be successfullyreated with shoulder arthroplasty, focal cartilage le-ions in the younger, active patient population demandlternative treatment strategies that preserve the joint.urvival rates of total shoulder arthroplasty in youngeratients are not as good as in older, less active pa-ients, with survivorship being reported as low as 61%
t 10 years in a series of 33 patients with a mean age685Surgery, Vol 26, No 5 (May), 2010: pp 685-696

oest
sthsehctbre
deAstohfmitn(tcdslgato1ll
c
bsos
I
alssoHSota
mslafddo
gsaHraoeMpr
PPAOICOIRO
686 F. ELSER ET AL.
f 46 years at the time of surgery.3 This review willxplore joint-preserving techniques for cartilage le-ions of the glenohumeral joint that can be used whenreating young, active patients.
ANATOMY
Recent investigations have deepened our under-tanding of the dimensions of the chondral surfaces ofhe glenohumeral articulation. At the center of theumeral head, the hyaline cartilage on the articularurface is 1.2 to 1.3 mm deep,4 thinning at the periph-ry to 1.0 mm or slightly less. On the glenoid surface,yaline cartilage is thicker at the periphery than in theenter. Bone density in adults is also greater beneathhe cartilage at the center of the glenoid, which haseen attributed to the higher loads that are seen in thisegion.5 The glenohumeral articular surface is congru-nt because of this varying thickness of the cartilage.6
INCIDENCE
The true incidence of focal glenohumeral chondralefects is unknown, because most lesions are discov-red in the setting of treatment for concomitant injury.rthroscopic evaluation of the glenohumeral cartilage
urface in 200 shoulders (195 patients) with full-hickness rotator cuff tears showed a 13% prevalencef articular cartilage pathology.1 Of the patients, 17ad minor lesions (8.5%) and only 9 (4.5%) had majorull-thickness lesions that measured more than 150m2. The prevalence of high-grade articular cartilage
njury in high-level overhead athletes was 17% inhrowers, all located near the insertion of the supraspi-atus tendon.2 Ellman et al.7 found that 6% of patientsmean age, 51 years) who underwent arthroscopicreatment for impingement symptoms had articularartilage lesions, which ranged in size from 15 mm iniameter to comprising 50% of the humeral chondralurface. Other authors have reported a 29% preva-ence of humeral head lesions and 15% prevalence oflenoid cartilage lesions in patients who underwentrthroscopy for subacromial impingement.8 For pa-ients who underwent arthroscopic shoulder surgery atur institution between 1993 and 2008, there was a2.4% prevalence (280 of 2,251) of grade III and IVesions on 1 or both glenohumeral surfaces (unpub-ished data, P.J.M., September 2009).
ETIOLOGY OF CARTILAGE LESIONS
The causes of glenohumeral chondral injury may be
onsidered in a systematic fashion. Injury patterns can be wroadly considered in relation to acute or recurrent in-tability, high-impact trauma, post-traumatic changes ofsteonecrosis or OCD, and complications or sequelae ofurgery (Table 1).
nstability
There is a well-documented association betweencute and recurrent shoulder dislocation and cartilageesions in the glenohumeral joint. In 1934 Hermods-on9 was the first to describe the ubiquitous compres-ion fracture of the posterolateral humeral head thatccurs with traumatic anterior instability, but it wasill and Sachs for whom the lesion was named.10
tudies have shown a high incidence of 47% to 100%f cartilage compression fractures or shear injury tohe chondral surface in first-time anterior dislocationsnd recurrent dislocations of the shoulder.11-13
Another cause of glenoid articular cartilage defectsay be glenolabral articular disruption (GLAD) le-
ions.14,15 This lesion consists of an anterior-inferiorabral tear associated with an injury to the glenoidrticular cartilage (Fig 1) and is usually caused by aorced adduction injury to the shoulder from an ab-ucted and externally rotated position. They may beifficult to diagnose clinically, although magnetic res-nance imaging (MRI) will usually show them.Chronic instability has been clearly linked to early
lenohumeral osteoarthritis.16,17 The time period ofhoulder instability from first dislocation to surgicalnterior stabilization, glenoid rim impaction fracture,ill-Sachs lesion, age at the time of first dislocation,
ecurrent instability, presence of a rotator cuff tear,nd clearly, any cartilage injury with an index episodef dislocation have all been independently linked toarly glenohumeral osteoarthritis (Table 2).16,18,19
arx et al.18 showed that patients with a history ofrevious shoulder dislocation had a 19 times greaterisk of shoulder arthritis developing than patients
TABLE 1. Etiology of Cartilage Lesions
revious surgeryenetrating or high-impact traumacute or recurrent dislocationsteonecrosis
nfectionhondrolysisCD
nflammatory arthritidesotator cuff arthropathysteoarthritis
ithout such a history. We have shown older age and

ttrWiosst
tSmlcscdercdi
tmsHits
bhifmhr
dsnfipt
domAflomgs3
O
sirTlmyh
CGHARP
Fw lesion( ).
687GLENOHUMERAL JOINT PRESERVATION
ime from injury to surgery to be independent predic-ors of osteoarthritis, but no correlation between di-ection of instability and osteoarthritis was found.20
e detected no difference between acute and chronicnstability with regard to the prevalence and gradef cartilage injury. In contrast, Brophy and Marx21
howed that chondral damage was associated withhoulder instability that worsened over time, althoughhe relation has yet to be clearly defined.
Open Bankart reconstructions, as well as nonana-omic reconstructions such as the Bristow, Magnuson-tack, and Putti-Platt procedures, have well-docu-ented associations with degenerative chondral
esions.21-24 In addition to the trauma of the dislo-ations, chondral injury may occur by excessivehear forces from nonanatomic repairs on articularartilage. A single high-impact trauma to the shoul-er may also cause chondral injury.25 In high-en-rgy injuries the subchondral bone is also atisk.26-28 The underlying mechanisms relate to highompressive/shear forces during the impact withisruption of the extracellular matrix and decreasesn chondrocyte metabolism.25
Active patients and athletes are at higher risk forraumatic cartilage lesions.26,27 In overhead athletesost lesions are located near the insertion of the
upraspinatus tendon, superior to the site of a classicill-Sachs lesion. These lesions can be caused by
mpingement between the humeral head and the pos-erosuperior glenoid rim.2 Thus microinstability orhear on the cartilage plays a role in these settings.
Osteonecrosis of the humeral head may result inoth focal and diffuse cartilage lesions of the humeralead. Symptomatic osteonecrosis of the humeral heads not uncommon, second in location only to theemoral head, and it affects patients at younger agesore than other degenerative conditions of the gleno-
umeral joint. Given the diminished weight-bearing
IGURE 1. Right shoulder viewing from posterior. Asterisk, humeith associated labral tear (red arrow). (B) Microfracture of GLAD
C) Early thrombus formation at chondral defect side (blue arrow
ole of the shoulder, however, many cases are notT
etected until advanced stages occur. The articularurface of the humeral head in contact with the gle-oid in midrange levels of motion usually collapsesrst. It is critical to avoid loaded overhead activity toreserve the surrounding cartilage during nonopera-ive or postoperative rehabilitation.
Classification follows a modified Ficat scheme, asescribed by Cruess.29 If detected in early stages,steonecrosis of the humeral head may be surgicallyanaged by core decompression and bone grafting.30
rthroscopic debridement of unstable, focal cartilageaps and lesions has also shown good short-termutcomes at 28 months,20 with significant improve-ent in pain and function in 54 of 61 patients with
rade IV cartilage damage. Other authors have de-cribed good or excellent results in 80% of patients at0 months’ follow-up.31
steochondritis dissecans
OCD is rare in the shoulder and is more commonlyeen in the femoral condyles or the talus. The diseases attributed to fragmentation of the subchondral plateesulting in destabilized chondral flaps and lesions.he precise etiology of OCD remains unclear, but it
ikely results from repetitive microtrauma or isolatedajor trauma.32 Most lesions have been described in
oung male patients in the anterosuperior aspect of theumeral head.32-35
TABLE 2. Predisposing Factors for Early GlenohumeralOsteoarthritis in Chronic Instability
artilage injury with index episode of dislocationlenoid rim impaction fractureill-Sachs lesionge at time of first dislocationecurrent instabilityresence of rotator cuff tear
d. (A) GLAD lesion in right anterior inferior glenoid (blue arrow)(blue arrow, awl) after debridement and labral repair (red arrow).
ral hea
ime period from first dislocation to anterior stabilization

mbptp
C
cgbfobgpaaicesgot
I
sivdrosssbdaalpccassd
cu
afte
cfimasscd
osr
icprpya
s
●
●
●
●
●
cbTaPbssmd
688 F. ELSER ET AL.
Treatment options for OCD lesions include debride-ent, removal of loose flaps or bodies, microfracture,
one grafting with or without autologous cartilage im-lants (autologous chondrocyte implantation [ACI]), andransfer of osteochondral plugs.35,36 The optimal ap-roach to surgical management remains controversial.
artilage injury associated with rotator cuff tears
Several studies identify a correlation between rotatoruff pathology and articular cartilage damage in thelenohumeral joint.1,2,35 Focal cartilage lesions haveeen identified in 13% of shoulders in a large series ofull-thickness tears.1 Neer et al.37 described the conceptf rotator cuff arthropathy, which results from the com-ination of massive rotator cuff tears and destructivelenohumeral wear patterns. According to Neer et al., therocess is multifactorial. Both mechanical factors, suchs impingement and instability of the shoulder, and met-bolic considerations, such as malnutrition from inactiv-ty and synovial fluid extravasation in massive rotatoruff tears, have been proposed. Both atrophy and degen-ration of the articular cartilage and osteoporosis of theubchondral bone of the humeral head may result. Aenetic predisposition for increased calcium crystal dep-sition has also been shown to hasten the onset of arthri-is in the setting of massive cuff tears.38
atrogenic injury
Iatrogenic damage to the articular cartilage can beubclassified into chondrolysis (chemical, thermal, id-opathic), infection, and mechanical factors. The de-elopment of glenohumeral chondrolysis after shoul-er arthroscopy is devastating, and some of the moreecent reports in the literature have highlighted somef the potential causes.39 Several case reports havehown extensive glenohumeral chondrolysis aftereemingly routine shoulder arthroscopy, thermal cap-ulorrhaphy, or rotator cuff repairs.40-42 Little hadeen known about the underlying cause of this rare butevastating complication. Ablative thermal energynd intra-articular pain pumps are clearly implicateds causative factors. Thermal ablation in the setting ofittle or no flow may increase arthroscopic fluid tem-eratures above 50°C to 55°C and result in cartilageell death.43 Routine local anesthetics (e.g., bupiva-aine and lidocaine), which have been used for yearss single injections in and around joints, have beenhown to be cytotoxic to chondrocytes in severaltudies.44,45 There are likely to be dose- and time-
ependent effects with these medications, and it is furrently our strong recommendation that intra-artic-lar administration through pain pumps be avoided.Postoperative glenohumeral sepsis can also be dev-
stating to articular cartilage. The outcomes of surgeryor septic arthritis are related to timely management,he presence of irreparable rotator cuff tears, and thextent of cartilage loss.46
The risk of cartilage damage due to intra-articularorticosteroid injections remains controversial. Bene-cial results from suppression of local joint inflam-ation are mostly transient. We recommend judicious
nd limited use of intra-articular steroids. Animaltudies have shown that corticosteroids alter tendontructure and weaken collagen, but there are few if anylinical data to support disease progression or chon-ral injury.47
Finally, mechanical factors, such as malpositionedr proud anchors after labral repair or perforatingcrews after osteosynthesis of the humeral head, mayesult in rapid destruction of the chondral surfaces.48
CLINICAL EVALUATION
Symptomatic cartilage lesions rarely appear insolation, and thus concomitant conditions must bearefully and systematically addressed. The clinicalresentation of focal chondral lesions may closelyesemble findings of impingement syndromes.7 Arecise history and clinical examination, especially inoung and active patients, remain pivotal in arriving atn accurate diagnosis.
Focal cartilage lesions should be considered in theetting of
Previous trauma or shoulder surgeryRecent or recurrent shoulder dislocations or sub-luxationsMechanical symptoms (clicking or catching)Discomfort, pain, or interrupted sleepWeakness or loss of range of motion
As part of a comprehensive shoulder examination, theompression-rotation test7 may help in differentiatingetween subacromial impingement and chondral lesions.he patient actively internally and externally rotates therm under axial compression of the glenohumeral joint.ain in the mid ranges of motion has been shown to beoth sensitive and specific for cartilage lesions in thehoulder.7 Subacromial injection can make this test morepecific by eliminating pain provocation from subacro-ial impingement. Crepitation or mechanical symptoms
uring active and passive range of motion may also arise
rom chondral lesions.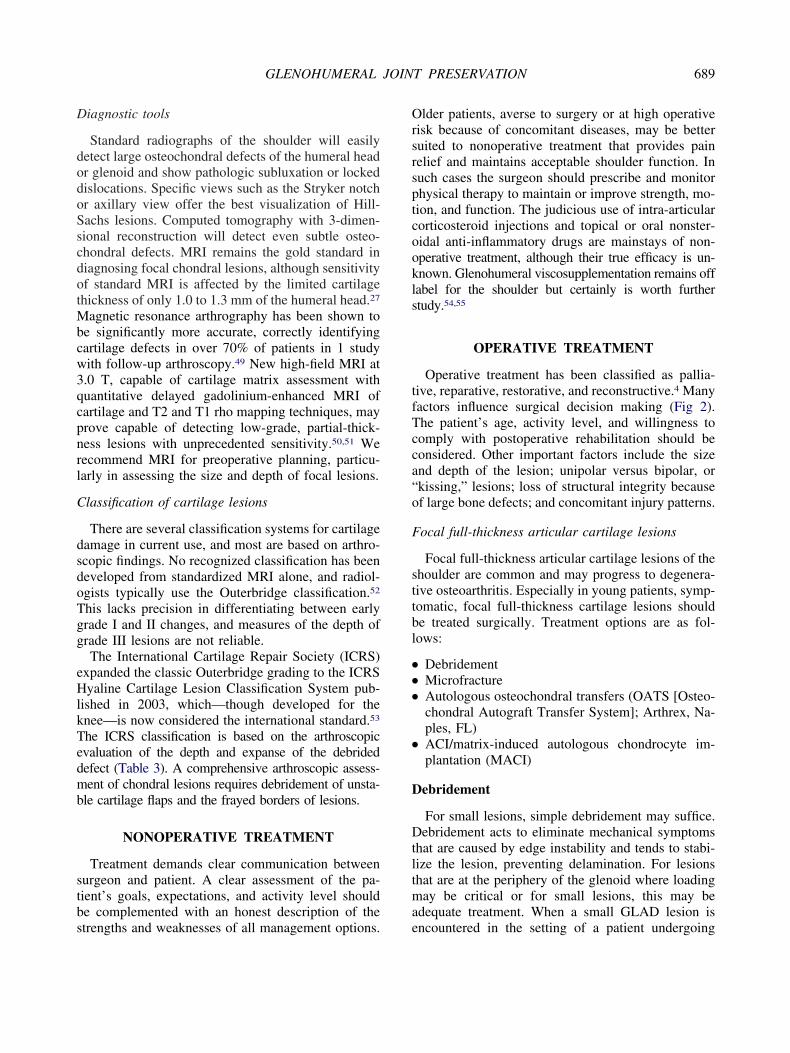
D
dodoSscdotMbcw3qcpnrl
C
dsdoTgg
eHlkTedmb
stbs
Orsrsptcookls
tfTcca“o
F
sttbl
●
●
●
●
D
Dtltma
689GLENOHUMERAL JOINT PRESERVATION
iagnostic tools
Standard radiographs of the shoulder will easilyetect large osteochondral defects of the humeral headr glenoid and show pathologic subluxation or lockedislocations. Specific views such as the Stryker notchr axillary view offer the best visualization of Hill-achs lesions. Computed tomography with 3-dimen-ional reconstruction will detect even subtle osteo-hondral defects. MRI remains the gold standard iniagnosing focal chondral lesions, although sensitivityf standard MRI is affected by the limited cartilagehickness of only 1.0 to 1.3 mm of the humeral head.27
agnetic resonance arthrography has been shown toe significantly more accurate, correctly identifyingartilage defects in over 70% of patients in 1 studyith follow-up arthroscopy.49 New high-field MRI at.0 T, capable of cartilage matrix assessment withuantitative delayed gadolinium-enhanced MRI ofartilage and T2 and T1 rho mapping techniques, mayrove capable of detecting low-grade, partial-thick-ess lesions with unprecedented sensitivity.50,51 Weecommend MRI for preoperative planning, particu-arly in assessing the size and depth of focal lesions.
lassification of cartilage lesions
There are several classification systems for cartilageamage in current use, and most are based on arthro-copic findings. No recognized classification has beeneveloped from standardized MRI alone, and radiol-gists typically use the Outerbridge classification.52
his lacks precision in differentiating between earlyrade I and II changes, and measures of the depth ofrade III lesions are not reliable.The International Cartilage Repair Society (ICRS)
xpanded the classic Outerbridge grading to the ICRSyaline Cartilage Lesion Classification System pub-
ished in 2003, which—though developed for thenee—is now considered the international standard.53
he ICRS classification is based on the arthroscopicvaluation of the depth and expanse of the debridedefect (Table 3). A comprehensive arthroscopic assess-ent of chondral lesions requires debridement of unsta-
le cartilage flaps and the frayed borders of lesions.
NONOPERATIVE TREATMENT
Treatment demands clear communication betweenurgeon and patient. A clear assessment of the pa-ient’s goals, expectations, and activity level shoulde complemented with an honest description of the
trengths and weaknesses of all management options. elder patients, averse to surgery or at high operativeisk because of concomitant diseases, may be betteruited to nonoperative treatment that provides painelief and maintains acceptable shoulder function. Inuch cases the surgeon should prescribe and monitorhysical therapy to maintain or improve strength, mo-ion, and function. The judicious use of intra-articularorticosteroid injections and topical or oral nonster-idal anti-inflammatory drugs are mainstays of non-perative treatment, although their true efficacy is un-nown. Glenohumeral viscosupplementation remains offabel for the shoulder but certainly is worth furthertudy.54,55
OPERATIVE TREATMENT
Operative treatment has been classified as pallia-ive, reparative, restorative, and reconstructive.4 Manyactors influence surgical decision making (Fig 2).he patient’s age, activity level, and willingness toomply with postoperative rehabilitation should beonsidered. Other important factors include the sizend depth of the lesion; unipolar versus bipolar, orkissing,” lesions; loss of structural integrity becausef large bone defects; and concomitant injury patterns.
ocal full-thickness articular cartilage lesions
Focal full-thickness articular cartilage lesions of thehoulder are common and may progress to degenera-ive osteoarthritis. Especially in young patients, symp-omatic, focal full-thickness cartilage lesions shoulde treated surgically. Treatment options are as fol-ows:
DebridementMicrofractureAutologous osteochondral transfers (OATS [Osteo-chondral Autograft Transfer System]; Arthrex, Na-ples, FL)ACI/matrix-induced autologous chondrocyte im-plantation (MACI)
ebridement
For small lesions, simple debridement may suffice.ebridement acts to eliminate mechanical symptoms
hat are caused by edge instability and tends to stabi-ize the lesion, preventing delamination. For lesionshat are at the periphery of the glenoid where loadingay be critical or for small lesions, this may be
dequate treatment. When a small GLAD lesion is
ncountered in the setting of a patient undergoing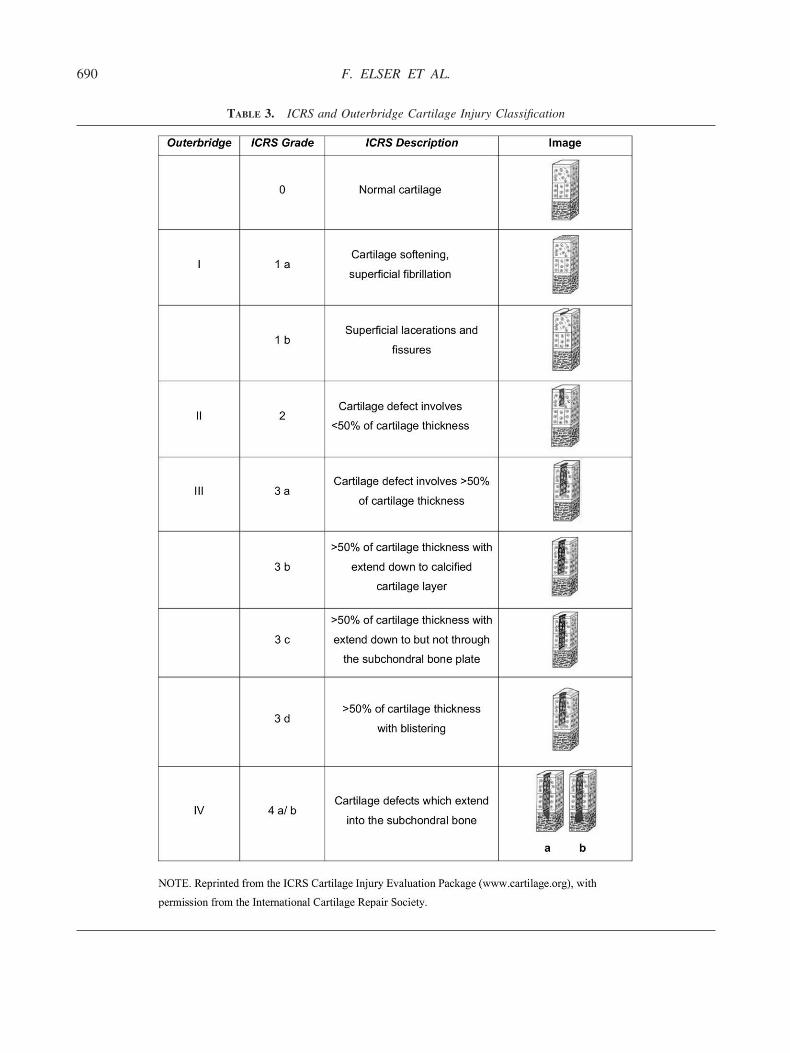
690 F. ELSER ET AL.
TABLE 3. ICRS and Outerbridge Cartilage Injury Classification
sti1usmsf
M
ttgi(dpoaa
ar
scio1mio(path
tAesc
cfsscm
O
asCmatA
Fo
FhP
691GLENOHUMERAL JOINT PRESERVATION
urgery for instability, 1 option is to simply debridehe unstable articular flap and then advance the labrumnto the defect when performing the labral repair (Fig). This effectively covers the defect and protects thenderlying bone. When diffuse cartilage loss exists,uch as in the setting of osteoarthritis, debridementay be undertaken to stabilize the remaining articular
urface and to eliminate joint irritation and synovitisrom cartilage detritus.
icrofracture
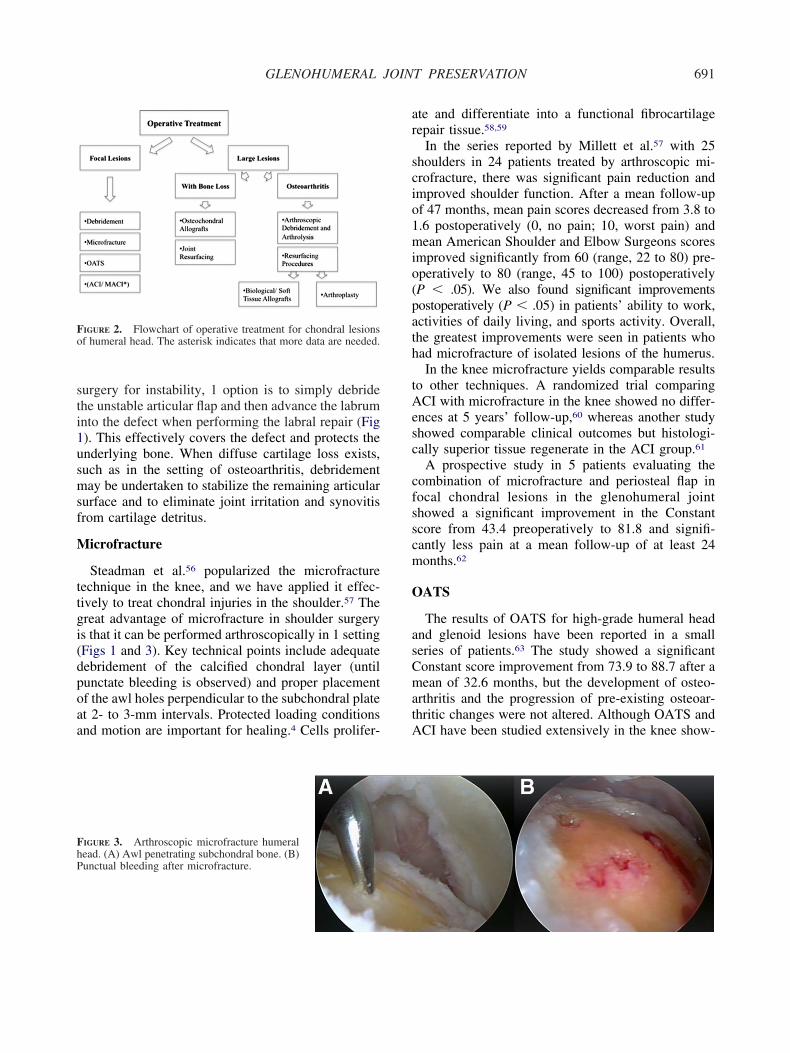
Steadman et al.56 popularized the microfractureechnique in the knee, and we have applied it effec-ively to treat chondral injuries in the shoulder.57 Thereat advantage of microfracture in shoulder surgerys that it can be performed arthroscopically in 1 settingFigs 1 and 3). Key technical points include adequateebridement of the calcified chondral layer (untilunctate bleeding is observed) and proper placementf the awl holes perpendicular to the subchondral platet 2- to 3-mm intervals. Protected loading conditionsnd motion are important for healing.4 Cells prolifer-
IGURE 2. Flowchart of operative treatment for chondral lesionsf humeral head. The asterisk indicates that more data are needed.
IGURE 3. Arthroscopic microfracture humeralead. (A) Awl penetrating subchondral bone. (B)unctual bleeding after microfracture.
te and differentiate into a functional fibrocartilageepair tissue.58,59
In the series reported by Millett et al.57 with 25houlders in 24 patients treated by arthroscopic mi-rofracture, there was significant pain reduction andmproved shoulder function. After a mean follow-upf 47 months, mean pain scores decreased from 3.8 to.6 postoperatively (0, no pain; 10, worst pain) andean American Shoulder and Elbow Surgeons scores
mproved significantly from 60 (range, 22 to 80) pre-peratively to 80 (range, 45 to 100) postoperativelyP � .05). We also found significant improvementsostoperatively (P � .05) in patients’ ability to work,ctivities of daily living, and sports activity. Overall,he greatest improvements were seen in patients whoad microfracture of isolated lesions of the humerus.In the knee microfracture yields comparable results
o other techniques. A randomized trial comparingCI with microfracture in the knee showed no differ-
nces at 5 years’ follow-up,60 whereas another studyhowed comparable clinical outcomes but histologi-ally superior tissue regenerate in the ACI group.61
A prospective study in 5 patients evaluating theombination of microfracture and periosteal flap inocal chondral lesions in the glenohumeral jointhowed a significant improvement in the Constantcore from 43.4 preoperatively to 81.8 and signifi-antly less pain at a mean follow-up of at least 24onths.62
ATS
The results of OATS for high-grade humeral headnd glenoid lesions have been reported in a smalleries of patients.63 The study showed a significantonstant score improvement from 73.9 to 88.7 after aean of 32.6 months, but the development of osteo-
rthritis and the progression of pre-existing osteoar-hritic changes were not altered. Although OATS andCI have been studied extensively in the knee show-

its
A
scguna
cm7apsga
L
LH
lhg
gwtaoiStw3bs
geprajna
mhuorst(vc
O
astidcowwCtch
FJ
692 F. ELSER ET AL.
ng their efficacy,64,65 similar trials are needed to de-ermine the relative success of these techniques in thehoulder.
CI and MACI
ACI in the shoulder has only been reported in aingle case study.66 Outcome studies of full-thicknessartilage defects of the knee treated by ACI showood to excellent results, even at long-term follow-p.67 Many surgeons continue to prefer alternate tech-iques that do not require the staged approach anddditional expense of ACI.
MACI, a collagen bio-scaffold that delivers in vitroultured autologous chondrocytes into the defect, is aore recent innovation.68 Studies on MACI showed
5% hyaline-like cartilage regeneration after 6 monthsnd good to excellent outcomes.69 MACI might showromise for the glenohumeral joint, because it is atable cell-based delivery system that enables the re-eneration of hyaline-like cartilage in a high percent-ge.
arge full-thickness articular cartilage lesions
esions With Significant Bone Loss or Partialumeral Head Necrosis
Large full-thickness articular cartilage lesions andesions with significant bone loss and partial humeralead necrosis can be treated by osteochondral allo-rafts or resurfacing procedures.Osteochondral Allografts: Osteochondral allo-
rafts do not impair the overall results for the patientith donor-site morbidity, and thus there is no limi-
ation to size. However, there are also potential dis-dvantages, such as limited chondrocyte viability, lossf matrix viability as shown by cationic staining,mmunogenicity, and possible disease transmission.70
tudies have shown better outcomes in traumatic os-eochondral lesions and younger patients (�50 years)ith success rates between 75% and 85% at a mean of.8 to 7.5 years’ follow-up.71,72 Rigid fixation of hostone to graft bone is important for long-term allografturvival.70
The use of osteochondral allografts in shoulder sur-ery is not common. Allografts have been used to fillngaging Hill-Sachs lesions,73 as well as defects fromroximal humeral bone tumor resections, with goodesults.74 There is limited experience with the use ofllografts for treatment of OCD of the glenohumeraloint.36 Osteochondral allografts are a promising alter-ative to resurfacing procedures, particularly in young,
thletic patients (Fig 4). tJoint Resurfacing: Recently, new partial replace-ents and stem-less implants for shoulder arthroplasty
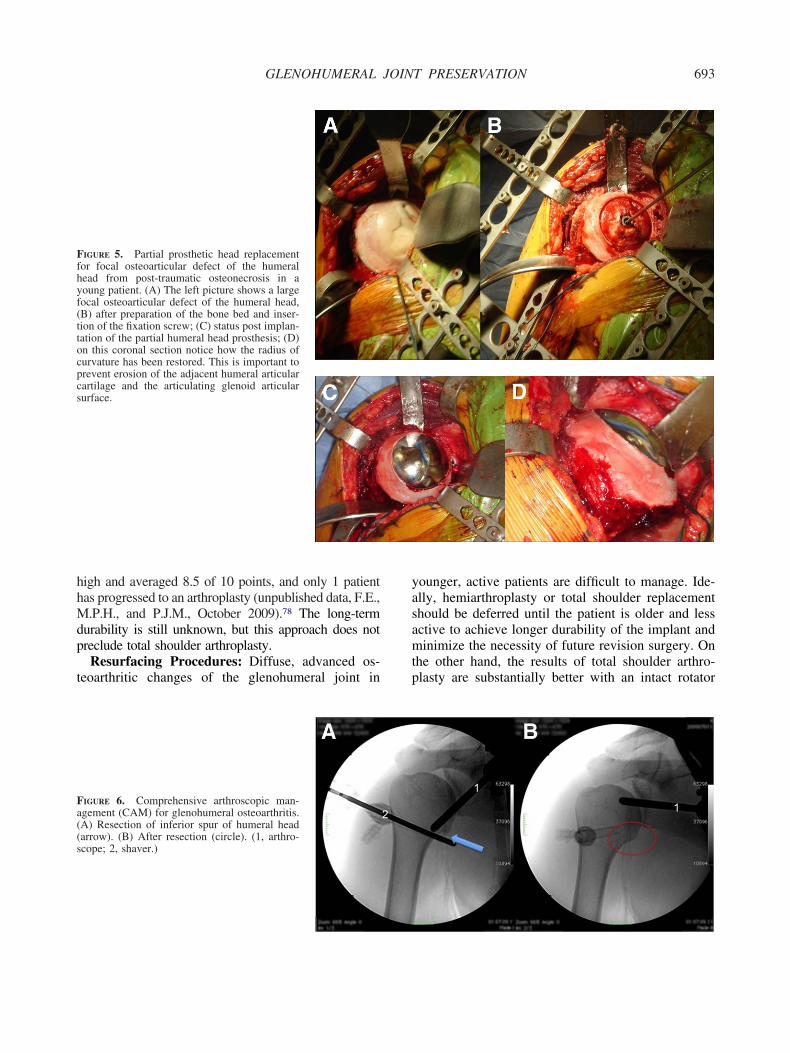
ave been developed that are particularly attractive forse in young patients. These implants preserve anat-my and leave open various options for subsequentevision surgery (Fig 5). In contrast to older prosthe-es, the new implants provide the ability to adjusthem to the cortical rim of the resected humeral headi.e., reconstruction of the humeral offset) and offer aariety of anatomic head sizes.75 Unfortunately, out-omes analyses are still forthcoming.
steoarthritisPalliative Procedures: Palliative procedures, such
s arthroscopic debridement31,76 and arthroscopic cap-ular release, can be performed in cases of osteoar-hritis, especially in younger patients to delay morenvasive surgery. The goals of the procedure are toiminish pain and increase motion, by reducing jointontact pressures and impingement from engagingsteophytes.76,77 At our institution, 27 young patients,ith a minimum 1-year follow-up, have been treatedith a surgical procedure that we have called theAM procedure—an acronym for “comprehensive ar-
hroscopic management” of shoulder arthritis that in-ludes an extensive debridement, capsular release, andumeral osteoplasty (Fig 6). At short-term follow-up,
IGURE 4. Allograft reconstruction of humeral head. (Courtesy ofon J. P. Warner, M.D.)
he mean patient satisfaction rate with the procedure was
hhMdp
t
yasamtp
Ffhyf(ttocpcs
Fa((s
693GLENOHUMERAL JOINT PRESERVATION
igh and averaged 8.5 of 10 points, and only 1 patientas progressed to an arthroplasty (unpublished data, F.E.,.P.H., and P.J.M., October 2009).78 The long-term
urability is still unknown, but this approach does notreclude total shoulder arthroplasty.Resurfacing Procedures: Diffuse, advanced os-
eoarthritic changes of the glenohumeral joint in
IGURE 5. Partial prosthetic head replacementor focal osteoarticular defect of the humeralead from post-traumatic osteonecrosis in aoung patient. (A) The left picture shows a largeocal osteoarticular defect of the humeral head,B) after preparation of the bone bed and inser-ion of the fixation screw; (C) status post implan-ation of the partial humeral head prosthesis; (D)n this coronal section notice how the radius ofurvature has been restored. This is important torevent erosion of the adjacent humeral articularartilage and the articulating glenoid articularurface.
IGURE 6. Comprehensive arthroscopic man-gement (CAM) for glenohumeral osteoarthritis.A) Resection of inferior spur of humeral headarrow). (B) After resection (circle). (1, arthro-cope; 2, shaver.)
ounger, active patients are difficult to manage. Ide-lly, hemiarthroplasty or total shoulder replacementhould be deferred until the patient is older and lessctive to achieve longer durability of the implant andinimize the necessity of future revision surgery. On
he other hand, the results of total shoulder arthro-lasty are substantially better with an intact rotator

clovpatvbor
tlalsAralegt
nb3m
hds1etf
srrdd5tMahpimlne
TmfbsccdthpmisTttpAndss
A
C
A
G
I
E
I
M
694 F. ELSER ET AL.
uff and good bone stock of the glenoid. New stem-ess implants for shoulder arthroplasty are promisingptions if palliative procedures fail. Results after con-entional arthroplasty/hemiarthroplasty in youngeratients performed for the treatment of osteoarthritisfter failed surgical stabilization procedures are rela-ively poor.3 Arthroplasty or hemiarthroplasty pro-ided satisfactory pain relief and improved motion,ut these procedures were associated with high ratesf revision surgery because of component failure,ecurrent instability, and pain.3
Biologic Glenoid Resurfacing/Interposition Ar-hroplasty: Alternative approaches to address unipo-ar glenoid arthritis have been proposed. Krishnan etl.79 recently published a prospective study on bio-ogic glenoid resurfacing using anterior capsule (7houlders), autogenous fascia lata (11 shoulders), andchilles tendon allograft (18 shoulders). The early
esults were comparable to the results of total shoulderrthroplasty without the inherent risks of the nonbio-ogical replacements. Achilles tendon allograft hasvolved as a preferred resurfacing material for thelenoid.79 Other authors, however, have not been ableo reproduce these results.
The use of meniscal allografts to resurface the gle-oid in conjunction with hemiarthroplasty has alsoeen proposed. Nicholson et al.80 published a series of0 young patients (mean age, 42 years) using lateraleniscus allograft for glenoid resurfacing during
TABLE 4. Key Points and Current Concepts in TreatingCartilage Lesions in Young, Active Patients
t the center of the humeral head, the hyaline cartilage thicknessis 1.2 to 1.3 mm, thinning at the periphery to 1.0 mm.
hronic instability has been clearly linked to early glenohumeralosteoarthritis.
ctive patients and athletes are at higher risk for traumaticcartilage lesions.
iven the diminished weight-bearing role of the shoulder, manycases of glenohumeral cartilage defects are not detected untiladvanced stages occur.
ntra-articular administration of local anesthetics (bupivacaine,lidocaine) through pain pumps should be avoided because ofthe risk of chondrolysis.
arly treatment of cartilage lesions is recommended in young,active patients to avoid the premature onset of osteoarthritis.
nnovative strategies for the treatment of cartilage lesions suchas ACI/MACI, OATS, and microfracture show excellentpromise, but they must still be established as effectivetechniques in the shoulder.icrofracture has the best evidence for treating focal cartilagelesions in the glenohumeral joint to date. Furthermore, it iscost-effective and can be performed arthroscopically in 1
ssetting.
emiarthroplasty. Their overall results were good,ocumenting significant improvements in outcomecores, but they found a moderate complication rate of7% requiring reoperation. Longer-term data, how-ver, have shown deterioration of the procedure, andhe initial enthusiasm for this technique seems to haveaded somewhat.
Arthroplasty: For older patients with severeymptomatic osteoarthritis, total shoulder arthroplastyemains the gold standard. The number of shouldereplacement surgeries performed in the United Statesoubled from 10,000 to 20,000 per year over the lastecade,81 and it is now estimated to be closer to0,000 per year. There is a clear correlation betweenhe surgeon’s volume and the outcome after surgery.81
ortality rates, rates of postoperative complications,nd inpatient days have been shown to be significantlyigher for operations that are performed by surgeonserforming fewer than 5 procedures per year.81 Theres a role for shoulder replacement surgery in the treat-ent of young, active patients with diffuse cartilage
oss, but given the high rates of revision surgery,on-arthroplasty options should be carefully consid-red and used if appropriate.
CONCLUSIONS
The key points of this article are summarized inable 4. Evolving innovative strategies for the treat-ent of cartilage lesions in the knee joint have been
ollowed by good short- to intermediate-term resultsut are yet to be established as effective techniques forimilar lesions in the shoulder. Investigators mustontinue to evaluate the safety and efficacy of newartilage repair and restorative strategies in the shoul-er. There is a preponderance of evidence to supporthe early treatment of cartilage lesions of the gleno-umeral joint in young, active patients to avoid theremature onset of osteoarthritis. Surgeons shouldaintain a heightened awareness of chondral injuries
n the glenohumeral joint and should be more aggres-ive in early diagnostic and therapeutic interventions.here is growing evidence to support the claim that
he progression of chondral injury may be slowed ifhe time between injury and surgery is minimized inatients with traumatic, recurrent shoulder instability.lthough the next decade is certain to bring excitingew technologies to bear on the treatment of focal andiffuse cartilage injury, successful intervention willtill depend on the sensitive diagnostic skills andound, principled decision making of the shoulder
urgeon.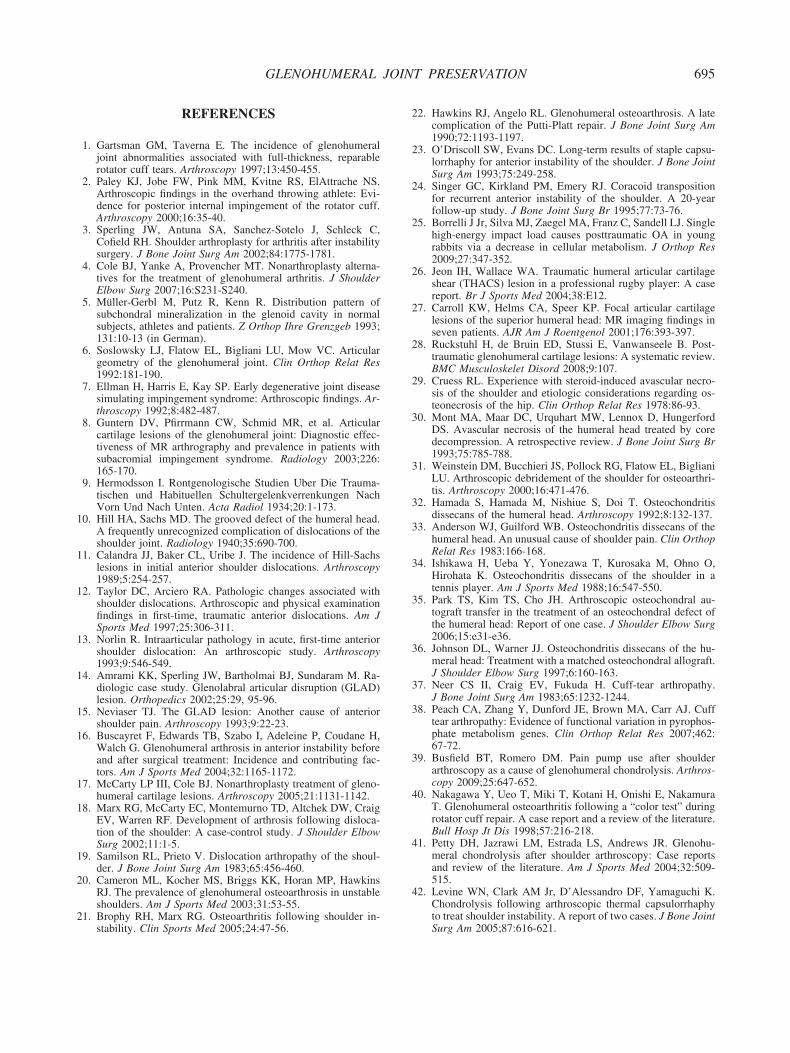
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
695GLENOHUMERAL JOINT PRESERVATION
REFERENCES
1. Gartsman GM, Taverna E. The incidence of glenohumeraljoint abnormalities associated with full-thickness, reparablerotator cuff tears. Arthroscopy 1997;13:450-455.
2. Paley KJ, Jobe FW, Pink MM, Kvitne RS, ElAttrache NS.Arthroscopic findings in the overhand throwing athlete: Evi-dence for posterior internal impingement of the rotator cuff.Arthroscopy 2000;16:35-40.
3. Sperling JW, Antuna SA, Sanchez-Sotelo J, Schleck C,Cofield RH. Shoulder arthroplasty for arthritis after instabilitysurgery. J Bone Joint Surg Am 2002;84:1775-1781.
4. Cole BJ, Yanke A, Provencher MT. Nonarthroplasty alterna-tives for the treatment of glenohumeral arthritis. J ShoulderElbow Surg 2007;16:S231-S240.
5. Müller-Gerbl M, Putz R, Kenn R. Distribution pattern ofsubchondral mineralization in the glenoid cavity in normalsubjects, athletes and patients. Z Orthop Ihre Grenzgeb 1993;131:10-13 (in German).
6. Soslowsky LJ, Flatow EL, Bigliani LU, Mow VC. Articulargeometry of the glenohumeral joint. Clin Orthop Relat Res1992:181-190.
7. Ellman H, Harris E, Kay SP. Early degenerative joint diseasesimulating impingement syndrome: Arthroscopic findings. Ar-throscopy 1992;8:482-487.
8. Guntern DV, Pfirrmann CW, Schmid MR, et al. Articularcartilage lesions of the glenohumeral joint: Diagnostic effec-tiveness of MR arthrography and prevalence in patients withsubacromial impingement syndrome. Radiology 2003;226:165-170.
9. Hermodsson I. Rontgenologische Studien Uber Die Trauma-tischen und Habituellen Schultergelenkverrenkungen NachVorn Und Nach Unten. Acta Radiol 1934;20:1-173.
0. Hill HA, Sachs MD. The grooved defect of the humeral head.A frequently unrecognized complication of dislocations of theshoulder joint. Radiology 1940;35:690-700.
1. Calandra JJ, Baker CL, Uribe J. The incidence of Hill-Sachslesions in initial anterior shoulder dislocations. Arthroscopy1989;5:254-257.
2. Taylor DC, Arciero RA. Pathologic changes associated withshoulder dislocations. Arthroscopic and physical examinationfindings in first-time, traumatic anterior dislocations. Am JSports Med 1997;25:306-311.
3. Norlin R. Intraarticular pathology in acute, first-time anteriorshoulder dislocation: An arthroscopic study. Arthroscopy1993;9:546-549.
4. Amrami KK, Sperling JW, Bartholmai BJ, Sundaram M. Ra-diologic case study. Glenolabral articular disruption (GLAD)lesion. Orthopedics 2002;25:29, 95-96.
5. Neviaser TJ. The GLAD lesion: Another cause of anteriorshoulder pain. Arthroscopy 1993;9:22-23.
6. Buscayret F, Edwards TB, Szabo I, Adeleine P, Coudane H,Walch G. Glenohumeral arthrosis in anterior instability beforeand after surgical treatment: Incidence and contributing fac-tors. Am J Sports Med 2004;32:1165-1172.
7. McCarty LP III, Cole BJ. Nonarthroplasty treatment of gleno-humeral cartilage lesions. Arthroscopy 2005;21:1131-1142.
8. Marx RG, McCarty EC, Montemurno TD, Altchek DW, CraigEV, Warren RF. Development of arthrosis following disloca-tion of the shoulder: A case-control study. J Shoulder ElbowSurg 2002;11:1-5.
9. Samilson RL, Prieto V. Dislocation arthropathy of the shoul-der. J Bone Joint Surg Am 1983;65:456-460.
0. Cameron ML, Kocher MS, Briggs KK, Horan MP, HawkinsRJ. The prevalence of glenohumeral osteoarthrosis in unstableshoulders. Am J Sports Med 2003;31:53-55.
1. Brophy RH, Marx RG. Osteoarthritis following shoulder in-
stability. Clin Sports Med 2005;24:47-56.2. Hawkins RJ, Angelo RL. Glenohumeral osteoarthrosis. A latecomplication of the Putti-Platt repair. J Bone Joint Surg Am1990;72:1193-1197.
3. O’Driscoll SW, Evans DC. Long-term results of staple capsu-lorrhaphy for anterior instability of the shoulder. J Bone JointSurg Am 1993;75:249-258.
4. Singer GC, Kirkland PM, Emery RJ. Coracoid transpositionfor recurrent anterior instability of the shoulder. A 20-yearfollow-up study. J Bone Joint Surg Br 1995;77:73-76.
5. Borrelli J Jr, Silva MJ, Zaegel MA, Franz C, Sandell LJ. Singlehigh-energy impact load causes posttraumatic OA in youngrabbits via a decrease in cellular metabolism. J Orthop Res2009;27:347-352.
6. Jeon IH, Wallace WA. Traumatic humeral articular cartilageshear (THACS) lesion in a professional rugby player: A casereport. Br J Sports Med 2004;38:E12.
7. Carroll KW, Helms CA, Speer KP. Focal articular cartilagelesions of the superior humeral head: MR imaging findings inseven patients. AJR Am J Roentgenol 2001;176:393-397.
8. Ruckstuhl H, de Bruin ED, Stussi E, Vanwanseele B. Post-traumatic glenohumeral cartilage lesions: A systematic review.BMC Musculoskelet Disord 2008;9:107.
9. Cruess RL. Experience with steroid-induced avascular necro-sis of the shoulder and etiologic considerations regarding os-teonecrosis of the hip. Clin Orthop Relat Res 1978:86-93.
0. Mont MA, Maar DC, Urquhart MW, Lennox D, HungerfordDS. Avascular necrosis of the humeral head treated by coredecompression. A retrospective review. J Bone Joint Surg Br1993;75:785-788.
1. Weinstein DM, Bucchieri JS, Pollock RG, Flatow EL, BiglianiLU. Arthroscopic debridement of the shoulder for osteoarthri-tis. Arthroscopy 2000;16:471-476.
2. Hamada S, Hamada M, Nishiue S, Doi T. Osteochondritisdissecans of the humeral head. Arthroscopy 1992;8:132-137.
3. Anderson WJ, Guilford WB. Osteochondritis dissecans of thehumeral head. An unusual cause of shoulder pain. Clin OrthopRelat Res 1983:166-168.
4. Ishikawa H, Ueba Y, Yonezawa T, Kurosaka M, Ohno O,Hirohata K. Osteochondritis dissecans of the shoulder in atennis player. Am J Sports Med 1988;16:547-550.
5. Park TS, Kim TS, Cho JH. Arthroscopic osteochondral au-tograft transfer in the treatment of an osteochondral defect ofthe humeral head: Report of one case. J Shoulder Elbow Surg2006;15:e31-e36.
6. Johnson DL, Warner JJ. Osteochondritis dissecans of the hu-meral head: Treatment with a matched osteochondral allograft.J Shoulder Elbow Surg 1997;6:160-163.
7. Neer CS II, Craig EV, Fukuda H. Cuff-tear arthropathy.J Bone Joint Surg Am 1983;65:1232-1244.
8. Peach CA, Zhang Y, Dunford JE, Brown MA, Carr AJ. Cufftear arthropathy: Evidence of functional variation in pyrophos-phate metabolism genes. Clin Orthop Relat Res 2007;462:67-72.
9. Busfield BT, Romero DM. Pain pump use after shoulderarthroscopy as a cause of glenohumeral chondrolysis. Arthros-copy 2009;25:647-652.
0. Nakagawa Y, Ueo T, Miki T, Kotani H, Onishi E, NakamuraT. Glenohumeral osteoarthritis following a “color test” duringrotator cuff repair. A case report and a review of the literature.Bull Hosp Jt Dis 1998;57:216-218.
1. Petty DH, Jazrawi LM, Estrada LS, Andrews JR. Glenohu-meral chondrolysis after shoulder arthroscopy: Case reportsand review of the literature. Am J Sports Med 2004;32:509-515.
2. Levine WN, Clark AM Jr, D’Alessandro DF, Yamaguchi K.Chondrolysis following arthroscopic thermal capsulorrhaphyto treat shoulder instability. A report of two cases. J Bone Joint
Surg Am 2005;87:616-621.
4
4
4
4
4
4
4
5
5
5
5
5
5
5
5
5
5
6
6
6
6
6
6
6
6
6
6
7
7
7
7
7
7
7
7
7
7
8
8
696 F. ELSER ET AL.
3. Zoric B, Horn N, Braun S, Millett PJ. Factors influencingintra-articular fluid temperature profiles with radiofrequencyablation. J Bone Joint Surg Am 2009;91:2448-2454.
4. Karpie JC, Chu CR. Lidocaine exhibits dose- and time-depen-dent cytotoxic effects on bovine articular chondrocytes invitro. Am J Sports Med 2007;35:1621-1627.
5. Chu CR, Izzo NJ, Coyle CH, Papas NE, Logar A. The in vitroeffects of bupivacaine on articular chondrocytes. J Bone JointSurg Br 2008;90:814-820.
6. Duncan SF, Sperling JW. Treatment of primary isolated shoul-der sepsis in the adult patient. Clin Orthop Relat Res 2008;466:1392-1396.
7. Wei AS, Callaci JJ, Juknelis D, et al. The effect of cortico-steroid on collagen expression in injured rotator cuff tendon.J Bone Joint Surg Am 2006;88:1331-1338.
8. Millett PJ, Clavert P, Warner JJ. Open operative treatment foranterior shoulder instability: When and why? J Bone JointSurg Am 2005;87:419-432.
9. Millett PJ, Neumann G, Yoshioka CS, Winalski CS, Carrino J,Lang P. Articular cartilage in the shoulder: Correlation of MRarthrography and surgical arthroscopy. Radiological Society ofNorth America. Presented at the 90th Scientific Assembly andAnnual Meeting, Chicago, Illinois, November 2004. Availableat: http://rsna2004.rsna.org/rsna2004/V2004/conference/event_display.cfm?em_id�4409527. Accessed May 6, 2008.
0. Gold GE, Reeder SB, Beaulieu CF. Advanced MR imaging ofthe shoulder: Dedicated cartilage techniques. Magn ResonImaging Clin N Am 2004;12:143-159, vii.
1. Link TM, Stahl R, Woertler K. Cartilage imaging: Motivation,techniques, current and future significance. Eur Radiol 2007;17:1135-1146.
2. Outerbridge RE. The etiology of chondromalacia patellae.J Bone Joint Surg Br 1961;43:752-757.
3. Brittberg M, Winalski CS. Evaluation of cartilage injuries andrepair. J Bone Joint Surg Am 2003;85:58-69 (Suppl 2).
4. Blaine T, Moskowitz R, Udell J, et al. Treatment of persistentshoulder pain with sodium hyaluronate: A randomized, con-trolled trial. A multicenter study. J Bone Joint Surg Am 2008;90:970-979.
5. Silverstein E, Leger R, Shea KP. The use of intra-articularhylan G-F 20 in the treatment of symptomatic osteoarthritis ofthe shoulder: A preliminary study. Am J Sports Med 2007;35:979-985.
6. Steadman JR, Rodkey WG, Rodrigo JJ. Microfracture: Surgi-cal technique and rehabilitation to treat chondral defects. ClinOrthop Relat Res 2001:S362-S369.
7. Millett PJ, Huffard BH, Horan MP, Hawkins RJ, Steadman JR.Outcomes of full-thickness articular cartilage injuries of theshoulder treated with microfracture. Arthroscopy 2009;25:856-863.
8. Shapiro F, Koide S, Glimcher MJ. Cell origin and differenti-ation in the repair of full-thickness defects of articular carti-lage. J Bone Joint Surg Am 1993;75:532-553.
9. Alford JW, Cole BJ. Cartilage restoration, part 2: Techniques,outcomes, and future directions. Am J Sports Med 2005;33:443-460.
0. Knutsen G, Drogset JO, Engebretsen L, et al. A randomizedtrial comparing autologous chondrocyte implantation with mi-crofracture. Findings at five years. J Bone Joint Surg Am2007;89:2105-2112.
1. Saris DB, Vanlauwe J, Victor J, et al. Characterized chondro-cyte implantation results in better structural repair when treat-ing symptomatic cartilage defects of the knee in a randomizedcontrolled trial versus microfracture. Am J Sports Med 2008;36:235-246.
2. Siebold R, Lichtenberg S, Habermeyer P. Combination of
microfracture and periostal-flap for the treatment of focal fullthickness articular cartilage lesions of the shoulder: A prospec-tive study. Knee Surg Sports Traumatol Arthrosc 2003;11:183-189.
3. Scheibel M, Bartl C, Magosch P, Lichtenberg S, HabermeyerP. Osteochondral autologous transplantation for the treatmentof full-thickness articular cartilage defects of the shoulder.J Bone Joint Surg Br 2004;86:991-997.
4. Hangody L, Füles P. Autologous osteochondral mosaicplastyfor the treatment of full-thickness defects of weight-bearingjoints: Ten years of experimental and clinical experience.J Bone Joint Surg Am 2003;85:25-32 (Suppl 2).
5. Bentley G, Biant LC, Carrington RW, et al. A prospective,randomised comparison of autologous chondrocyte implanta-tion versus mosaicplasty for osteochondral defects in the knee.J Bone Joint Surg Br 2003;85:223-230.
6. Romeo AA, Cole BJ, Mazzocca AD, Fox JA, Freeman KB,Joy E. Autologous chondrocyte repair of an articular defect inthe humeral head. Arthroscopy 2002;18:925-929.
7. Peterson L, Brittberg M, Kiviranta I, Akerlund EL, Lindahl A.Autologous chondrocyte transplantation. Biomechanics andlong-term durability. Am J Sports Med 2002;30:2-12.
8. Cherubino P, Grassi FA, Bulgheroni P, Ronga M. Autologouschondrocyte implantation using a bilayer collagen membrane:A preliminary report. J Orthop Surg (Hong Kong) 2003;11:10-15.
9. Zheng MH, Willers C, Kirilak L, et al. Matrix-induced autol-ogous chondrocyte implantation (MACI): Biological and his-tological assessment. Tissue Eng 2007;13:737-746.
0. Gross AE, Kim W, Las Heras F, Backstein D, Safir O, PritzkerKP. Fresh osteochondral allografts for posttraumatic knee de-fects: Long-term followup. Clin Orthop Relat Res 2008;466:1863-1870.
1. McDermott AG, Langer F, Pritzker KP, Gross AE. Freshsmall-fragment osteochondral allografts. Long-term follow-upstudy on first 100 cases. Clin Orthop Relat Res 1985:96-102.
2. Ghazavi MT, Pritzker KP, Davis AM, Gross AE. Fresh osteo-chondral allografts for post-traumatic osteochondral defects ofthe knee. J Bone Joint Surg Br 1997;79:1008-1013.
3. Chapovsky F, Kelly JD IV. Osteochondral allograft transplan-tation for treatment of glenohumeral instability. Arthroscopy2005;21:1007.
4. DeGroot H, Donati D, Di Liddo M, Gozzi E, Mercuri M. Theuse of cement in osteoarticular allografts for proximal humeralbone tumors. Clin Orthop Relat Res 2004:190-197.
5. Jensen KL. Humeral resurfacing arthroplasty: Rationale, indi-cations, technique, and results. Am J Orthop 2007;36:4-8.
6. Richards DP, Burkhart SS. Arthroscopic debridement and cap-sular release for glenohumeral osteoarthritis. Arthroscopy2007;23:1019-1022.
7. Millett PJ, Gobezie R, Boykin RE. Shoulder osteoarthritis:Diagnosis and management. Am Fam Physician 2008;78:605-611.
8. Elser F, Horan MP, Millett PJ. Comprehensive arthroscopicmanagement (CAM) of shoulder osteoarthritis in young activepatients. Accepted for presentation by E-poster at the 2010Arthroscopy Association of North America Annual Meeting,Hollywood, Florida, May 20-23, 2010.
9. Krishnan SG, Nowinski RJ, Harrison D, Burkhead WZ. Hu-meral hemiarthroplasty with biologic resurfacing of the gle-noid for glenohumeral arthritis. Two to fifteen-year outcomes.J Bone Joint Surg Am 2007;89:727-734.
0. Nicholson GP, Goldstein JL, Romeo AA, et al. Lateral menis-cus allograft biologic glenoid arthroplasty in total shoulderarthroplasty for young shoulders with degenerative joint dis-ease. J Shoulder Elbow Surg 2007;16:S261-S266.
1. Jain N, Pietrobon R, Hocker S, Guller U, Shankar A, HigginsLD. The relationship between surgeon and hospital volume
and outcomes for shoulder arthroplasty. J Bone Joint Surg Am2004;86:496-505.




























