Embed Size (px)
Citation preview

Carcinogenesis vol.29 no.12 pp.2341–2346, 2008doi:10.1093/carcin/bgn235Advance Access publication October 8, 2008
Genetic variants in fibroblast growth factor receptor 2 (FGFR2) contribute tosusceptibility of breast cancer in Chinese women
Jie Liangy, Peizhan Chen1,y, Zhibin Hu, Xiaoyi Zhou, LuChen1, Mian Li1, Yan Wang, Jinhai Tang2, Hui Wang1 andHongbing Shen�
Laboratory of Reproductive Medicine, Cancer Center, Nanjing MedicalUniversity, 140 Hanzhong Road, Nanjing 210029, China, 1Institute forNutritional Sciences, Shanghai Institutes for Biological Sciences, ChineseAcademy of Sciences, Shanghai 200031, People’s Republic of China and2Department of General Surgery, Jiangsu Cancer Hospital, Nanjing 210009,China
�To whom correspondence should be addressed. Tel/Fax: þ86 25 868 62756;Email: [email protected] may also be addressed to Hui Wang.Tel/Fax: þ86 21 5492 0941;Email: [email protected]
Fibroblast growth factor receptor 2 (FGFR2) belongs to theFGFR family, which plays an important role in cell growth, in-vasiveness, motility and angiogenesis. In human breast cancer,expression of FGFR2 is estrogen receptor (ER)-dependent andcorrelates with a lower rate of apoptosis. Recently, whole-genomeassociation studies have identified several single-nucleotide poly-morphisms (SNPs) of FGFR2 as novel breast cancer susceptibilityloci. In the present study of 1049 breast cancer patients and 1073cancer-free controls, we assessed whether polymorphisms ofFGFR2 are associated with breast cancer risk in Chinese womenand whether these associations are stronger in women with areproductive history suggestive of greater exposure to endogenousestrogens. We genotyped three FGFR2 polymorphisms(rs2981582C/T, rs1219648A/G and rs2420946C/T) using theSNPstream 12-plex platform. Each of the three SNPs was signif-icantly associated with increased breast cancer risk in a dose-dependent manner. Compared with women with 0–2 risk loci,those with 3 risk loci had a 1.36-fold increased odds of breastcancer (95% confidence interval 5 1.13–1.62, P 5 0.001). Instratified analyses, associations between the presence of 3 risk lociand breast cancer were stronger among women with ER- and/orprogesterone receptor-positive cancers, premenopausal womenand women with an older age at first live birth. Furthermore,there was a significant additive interaction between risk genotypesand menopausal status (P for multiplication interaction/additiveinteraction: 0.083/0.037). These findings indicate that genetic var-iants in FGFR2 may contribute to breast cancer occurrence inChinese women, possibly through pathways related to estrogenand/or progesterone.
Introduction
Breast cancer is the most commonly occurring cancer and the leadingcause of cancer death among women worldwide, accounting for 23% ofall cancers and .400 000 deaths annually (1). In China, the incidencerate of breast cancer has increased dramatically in recent years, witha sharp rise of 38.5% between 2000 and 2005 (2). The etiology of breastcancer appears to entail a complex combination of genetic, environ-mental and lifestyle factors; of these, menstrual and reproductive fac-tors, such as earlier menarche, nulliparity, later age at first birth andlater menopause, have a dominant relation to risk (3–5). In developingcountries, breast cancer tends to be diagnosed at an earlier age than in
European and American population, and the rapid rate of increase inincidence before menopause is not maintained afterwards, possiblyreflecting diminished levels of circulating estrogens (5).
Twin- and family-based studies indicate that a substantial propor-tion of breast cancer is due to inherited susceptibility, but only a smallfraction of cases are associated with inherited mutations of knownhigh-penetrance genes (e.g. BRCA1, BRCA2, ATM, etc.). Commonvariants in other lower penetrance genes may be more importantand may account for higher attributable risks (6). Recently, a large-scale genome-wide association study (7) identified five new indepen-dent low-penetrance susceptibility loci that were strongly associatedwith breast cancer in populations of diverse ethnicity. Four of these[fibroblast growth factor receptor 2 (FGFR2), TNRC9, MAP3K1 andLSP1] contain plausible causative genes, among which FGFR2 hasa prior relevance to breast cancer.
FGFR2 belongs to the FGFR family, which contributes to cellgrowth, invasiveness, motility and angiogenesis (8). Overexpressionof FGFR2 is observed in breast cancer cell lines (9), as well as inbreast tumor tissues (10). The FGFR2 gene, located at chromosome10q26, contains at least 22 exons (11). Recently, Easton et al. (7)found that rs2981582 in intron 2 of FGFR2 was associated with anincreased risk of breast cancer in a two-stage genome-wide associa-tion study among 4398 cases and 4316 controls, followed by a thirdstage of 21 860 cases and 22 578 controls from 22 studies. In addi-tion, in a genome-wide association study of 1145 post-menopausalwomen and 1142 controls of European ancestry, Hunter et al. (12)subsequently reported that four single-nucleotide polymorphisms(SNPs) (rs2420946, rs1219648, rs2981579 and rs11200014) in intron2 of FGFR2 were associated with breast cancer risk. Interestingly, thefive SNPs were in high linkage disequilibrium (LD) in people withEuropean ancestry (all pairwise r2 . 0.96).
Prior studies have not clearly documented possible relationshipsbetween FGFR2 polymorphisms and hormone receptor-defined sub-sets of breast cancer nor have possible interactions between FGFR2polymorphisms and breast cancer risk factors been reported. Weposited that FGFR2 polymorphisms may contribute to breast cancersusceptibility by acting through hormonal pathways, and we hypoth-esized that the risk associated with these polymorphisms would varydepending on the hormone receptor status of the breast tumor and onthe presence of known reproductive risk factors. To test this hypoth-esis, we performed genotyping analyses of rs2981582C/T (fromEaston et al.), rs1219648A/G and rs2420946C/T (the two mostsignificant SNPs from Hunter et al.) in FGFR2 in a case–controlstudy of 1049 breast cancer cases and 1073 cancer-free controls ina Chinese population.
Materials and methods
Study subjects
This study was approved by the institutional review board of Nanjing MedicalUniversity. The hospital-based case–control study included 1058 breast cancercases and 1078 cancer-free controls, and the process of participant recruitmenthas been described previously (13). In brief, incident breast cancer patientswere consecutively recruited from the First Affiliated Hospital of NanjingMedical University, the Cancer Hospital of Jiangsu Province and the GulouHospital, Nanjing, China, between January 2004 and May 2007. Exclusioncriteria included reported previous cancer history, metastasized cancer fromother organs and previous radiotherapy or chemotherapy. All breast cancercases were newly diagnosed and histopathologically confirmed without restric-tions of age or histological type. Cancer-free control women, frequency-matched to the cases on age (±5 years) and residential area (urban or rural),were randomly selected from a cohort of .30 000 participants in a commu-nity-based screening program for non-infectious diseases conducted from 2004to 2006 in the same Jiangsu Province, China. We determined the participants inthe cohort as cancer free if they did not report having cancer history at the time
Abbreviations: CI, confidence interval; ER, estrogen receptor; FGFR2, fibro-blast growth factor receptor 2; LD, linkage disequilibrium; OR, odds ratio; PR,progesterone receptor; SNP, single-nucleotide polymorphism.
yThese authors contributed equally to this work.
� The Author 2008. Published by Oxford University Press. All rights reserved. For Permissions, please email: [email protected] 2341
at J.N. D
esmarais L
ibrary, Laurentian U
niversity on October 6, 2014
http://carcin.oxfordjournals.org/D
ownloaded from
of interview and blood donation. All participants were genetically unrelated,ethnic Han Chinese women.
After providing informed consent, each woman was personally inter-viewed face-to-face by trained interviewers using a pretested standard ques-tionnaire to obtain information on demographic data, menstrual andreproductive history, environmental exposure history and family history ofany cancer in first-degree relatives (parents, siblings and children). The datacollection methods were similar for the cases and controls in terms of theinvestigation of reproductive history including number of births, numberof pregnancies, age at menopause and type of menopause. Natural post-menopausal was determined in both cases and controls for women withoutmenstrual flow for .12 months and also no history of sex hormone-relatedtreatment (e.g. surgery, radiation and drug treatment). After the interview,each subject provided 5 ml of venous blood. The estrogen receptor (ER) andprogesterone receptor (PR) status of breast cancers was determined from theresults of immunohistochemistry examinations contained in the medicalrecords of the hospitals. ER/PR statuses were carried out for the breast cancercases by established immunohistochemical method of avidin–biotin–peroxidase complex assay. Immunoreactivity scoring was performed by eval-uating the percentage of cancer cell nuclear staining, and the percentage ofstaining cells �10% was considered positive.
Genotype analyses
Genomic DNA was isolated from leukocyte pellets from venous blood byproteinase K digestion and followed by phenol–chloroform extraction. Thethree SNPs (rs2981582C/T, rs1219648A/G and rs2420946C/T) were geno-
typed on the GenomeLab SNPstream high-throughput 12-plex genotypingplatform (Beckman Coulter, Fullerton, CA) following the manufacturer’s in-structions. This platform uses a single-base pair extension reaction to incorpo-rate two-color fluorescence terminal nucleotides that are detected bya specialized imager (14).
Ge3notyping was performed without the knowledge of case or control status.Approximately equal numbers of case and control specimens were assayed ineach 384-well polymerase chain reaction plate with four blanks and 24 randomlyselected duplicates, and the coincidence rate was .99%. Genotyping failed innine cases (0.85%) and five controls (0.46%) due to DNA quality or quantity; alldata from these 14 women were excluded from analyses. Therefore, 1049 breastcancer cases and 1073 controls were included in the final analyses.
Statistical analyses
Differences between cases and controls in demographic characteristics, risk fac-tors and frequencies of FGFR2 variants were evaluated by v2 tests (for categor-ical variables) or Student’s t-test (for continuous variables). Associationsbetween FGFR2 genotypes and risk of breast cancer were estimated by com-puting odds ratios (ORs) and their 95% confidence intervals (CIs) from logisticregression analyses with adjustment for age, age at menarche, menopausal statusand family history of cancer. Hardy–Weinberg equilibrium was evaluated bya goodness-of-fit v2 test to compare the observed genotype frequencies with theexpected ones among the controls. We used the PHASE 2.0 program to inferhaplotype frequencies based on the observed FGFR2 genotypes. To performtests of possible gene–risk factor interactions for additive models, we imple-mented bootstrapping using Stata software (version 8.2; StataCorp LP, College
Table I. Distributions of select variables in breast cancer cases and cancer-free controls
Variables Cases, n 5 1049 Controls, n 5 1073 P OR (95% CI)
Age, year (mean ± SD) 51.59 ± 11.18 51.77 ± 11.10 0.712Age at menarche, year (mean ± SD) 15.29 ± 1.94 16.03 ± 1.92 ,0.0001Age at menopause, year (mean ± SD)a 48.99 ± 4.42 49.26 ± 4.23 0.318Age at first live birth, year (mean ± SD)b 25.58 ± 3.42 24.94 ± 3.20 ,0.0001Menopausal status 0.330
Premenopausal 509 (48.52%) 498 (46.41%)Post-menopausal 540 (51.48%) 575 (53.59%)
Family history of cancer ,0.0001Positive 305 (28.88%) 231 (21.53%)Negative 744 (70.92%) 842 (78.47%)
Parity 0.0041 589 (58.14) 528 (52.54) 1.002 236 (23.30) 259 (25.77) 0.82 (0.66–1.01)3 114 (11.25) 104 (10.35) 0.98 (0.74–1.31)�4 74 (7.31) 114 (11.34) 0.58 (0.43–0.80)
Pregnancy 0.0011 167 (17.04) 221 (22.37) 1.002 284 (28.98) 309 (31.28) 1.22 (0.94–1.57)3 246 (25.10) 186 (18.83) 1.75 (1.33–2.31)�4 283 (28.88) 272 (27.53) 1.38 (1.06–1.79)
Type of menopause ,0.0001Natural 458 (84.81) 571 (99.30) 1.00Unusualc 82 (15.19) 4 (0.70) 25.56 (9.30–70.25)
ERd
Positive 439 (54.00)Negative 374 (46.00)
PRd
Positive 446 (54.86)Negative 367 (45.14)
Menopausal status Premenopausal Post-menopausal ,0.0001ERþ/PRþ 189 (48.46) 175 (41.37)ER�/PRþ 49 (12.56) 33 (7.80)ERþ/PR� 20 (5.13) 55 (13.00)ER�/PR� 132 (33.85) 160 (37.83)
Age ,50 �50 0.0001ERþ/PRþ 182 (47.52) 182 (42.33)ER�/PRþ 53 (13.84) 29 (6.74)ERþ/PR� 25 (6.53) 50 (11.63)ER�/PR� 123 (32.11) 169 (39.30)
aAge at menopause information was available in 522 breast cancer cases (96.7%) and 518 controls (90.1%) with post-menopausal status.bAge at first live birth information was available in 1006 breast cancer cases (95.9%) and 1043 controls (97.2%).cUnusual menopause include operation, radiotherapy or other status.dInformation of ER and PR status was available in 813 breast cancer cases (77.5%).
J.Liang et al.
2342
at J.N. D
esmarais L
ibrary, Laurentian U
niversity on October 6, 2014
http://carcin.oxfordjournals.org/D
ownloaded from
Station, TX). All the statistical analyses were performed with Statistical AnalysisSystem software (9.1.3; SAS Institute, Cary, NC), unless indicated otherwise.
Results
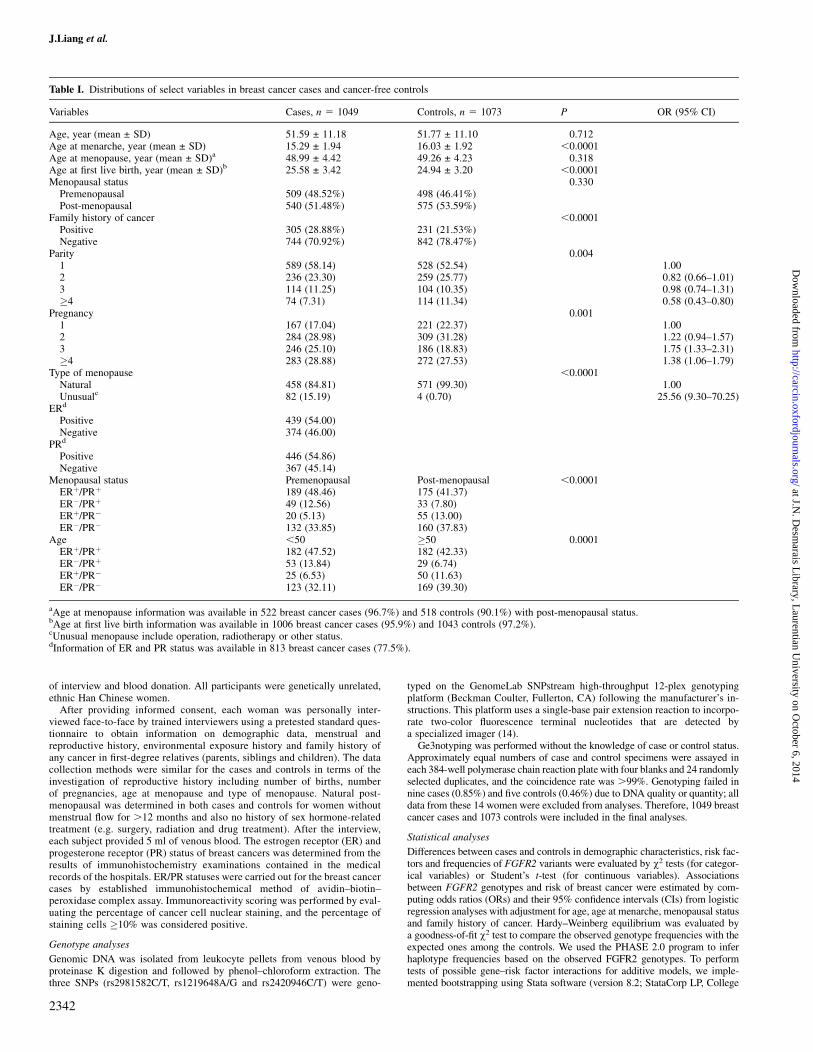
The 1049 breast cancer cases and 1073 cancer-free controls weresimilar with regard to age at interview, menopausal status and age atmenopause (Table I). However, cases differed from controls in havingan earlier age at menarche, a later age of first live birth, a greaterlikelihood of a positive family history of any cancer, less parities andmore pregnancies. Unusual menopause was also a major risk factorfor breast cancer. Among 813 breast cancer cases with known ER andPR status, 364 (44.8%) were positive with both ER and PR and 292(33.9%) were negative for both. When we stratified ER/PR status bymenopause status and age, post-menopausal and aged women weremore likely to be ER�/PR� breast cancer patients (Table I).
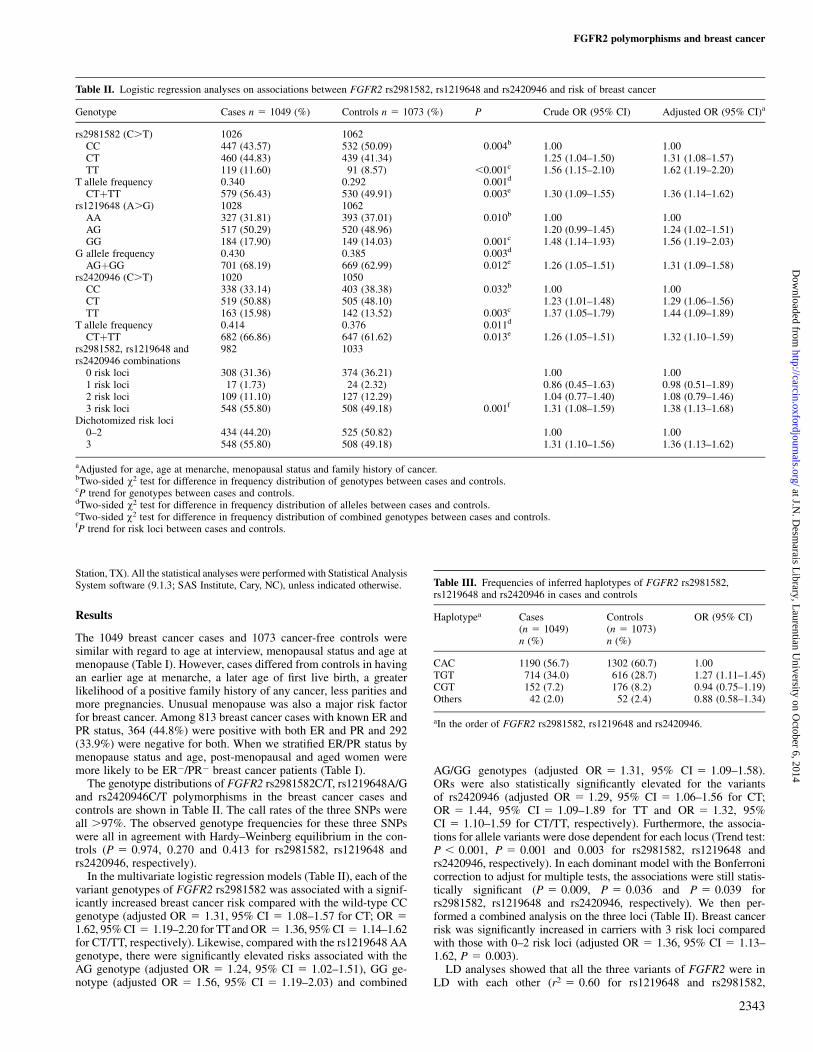
The genotype distributions of FGFR2 rs2981582C/T, rs1219648A/Gand rs2420946C/T polymorphisms in the breast cancer cases andcontrols are shown in Table II. The call rates of the three SNPs wereall .97%. The observed genotype frequencies for these three SNPswere all in agreement with Hardy–Weinberg equilibrium in the con-trols (P 5 0.974, 0.270 and 0.413 for rs2981582, rs1219648 andrs2420946, respectively).
In the multivariate logistic regression models (Table II), each of thevariant genotypes of FGFR2 rs2981582 was associated with a signif-icantly increased breast cancer risk compared with the wild-type CCgenotype (adjusted OR 5 1.31, 95% CI 5 1.08–1.57 for CT; OR 51.62, 95% CI 5 1.19–2.20 for TTand OR 5 1.36, 95% CI 5 1.14–1.62for CT/TT, respectively). Likewise, compared with the rs1219648 AAgenotype, there were significantly elevated risks associated with theAG genotype (adjusted OR 5 1.24, 95% CI 5 1.02–1.51), GG ge-notype (adjusted OR 5 1.56, 95% CI 5 1.19–2.03) and combined
AG/GG genotypes (adjusted OR 5 1.31, 95% CI 5 1.09–1.58).ORs were also statistically significantly elevated for the variantsof rs2420946 (adjusted OR 5 1.29, 95% CI 5 1.06–1.56 for CT;OR 5 1.44, 95% CI 5 1.09–1.89 for TT and OR 5 1.32, 95%CI 5 1.10–1.59 for CT/TT, respectively). Furthermore, the associa-tions for allele variants were dose dependent for each locus (Trend test:P , 0.001, P 5 0.001 and 0.003 for rs2981582, rs1219648 andrs2420946, respectively). In each dominant model with the Bonferronicorrection to adjust for multiple tests, the associations were still statis-tically significant (P 5 0.009, P 5 0.036 and P 5 0.039 forrs2981582, rs1219648 and rs2420946, respectively). We then per-formed a combined analysis on the three loci (Table II). Breast cancerrisk was significantly increased in carriers with 3 risk loci comparedwith those with 0–2 risk loci (adjusted OR 5 1.36, 95% CI 5 1.13–1.62, P 5 0.003).
LD analyses showed that all the three variants of FGFR2 were inLD with each other (r2 5 0.60 for rs1219648 and rs2981582,
Table II. Logistic regression analyses on associations between FGFR2 rs2981582, rs1219648 and rs2420946 and risk of breast cancer
Genotype Cases n 5 1049 (%) Controls n 5 1073 (%) P Crude OR (95% CI) Adjusted OR (95% CI)a
rs2981582 (C.T) 1026 1062CC 447 (43.57) 532 (50.09) 0.004b 1.00 1.00CT 460 (44.83) 439 (41.34) 1.25 (1.04–1.50) 1.31 (1.08–1.57)TT 119 (11.60) 91 (8.57) ,0.001c 1.56 (1.15–2.10) 1.62 (1.19–2.20)
T allele frequency 0.340 0.292 0.001d
CTþTT 579 (56.43) 530 (49.91) 0.003e 1.30 (1.09–1.55) 1.36 (1.14–1.62)rs1219648 (A.G) 1028 1062
AA 327 (31.81) 393 (37.01) 0.010b 1.00 1.00AG 517 (50.29) 520 (48.96) 1.20 (0.99–1.45) 1.24 (1.02–1.51)GG 184 (17.90) 149 (14.03) 0.001c 1.48 (1.14–1.93) 1.56 (1.19–2.03)
G allele frequency 0.430 0.385 0.003d
AGþGG 701 (68.19) 669 (62.99) 0.012e 1.26 (1.05–1.51) 1.31 (1.09–1.58)rs2420946 (C.T) 1020 1050
CC 338 (33.14) 403 (38.38) 0.032b 1.00 1.00CT 519 (50.88) 505 (48.10) 1.23 (1.01–1.48) 1.29 (1.06–1.56)TT 163 (15.98) 142 (13.52) 0.003c 1.37 (1.05–1.79) 1.44 (1.09–1.89)
T allele frequency 0.414 0.376 0.011d
CTþTT 682 (66.86) 647 (61.62) 0.013e 1.26 (1.05–1.51) 1.32 (1.10–1.59)rs2981582, rs1219648 andrs2420946 combinations
982 1033
0 risk loci 308 (31.36) 374 (36.21) 1.00 1.001 risk loci 17 (1.73) 24 (2.32) 0.86 (0.45–1.63) 0.98 (0.51–1.89)2 risk loci 109 (11.10) 127 (12.29) 1.04 (0.77–1.40) 1.08 (0.79–1.46)3 risk loci 548 (55.80) 508 (49.18) 0.001f 1.31 (1.08–1.59) 1.38 (1.13–1.68)
Dichotomized risk loci0–2 434 (44.20) 525 (50.82) 1.00 1.003 548 (55.80) 508 (49.18) 1.31 (1.10–1.56) 1.36 (1.13–1.62)
aAdjusted for age, age at menarche, menopausal status and family history of cancer.bTwo-sided v2 test for difference in frequency distribution of genotypes between cases and controls.cP trend for genotypes between cases and controls.dTwo-sided v2 test for difference in frequency distribution of alleles between cases and controls.eTwo-sided v2 test for difference in frequency distribution of combined genotypes between cases and controls.fP trend for risk loci between cases and controls.
Table III. Frequencies of inferred haplotypes of FGFR2 rs2981582,rs1219648 and rs2420946 in cases and controls
Haplotypea Cases(n 5 1049)
Controls(n 5 1073)
OR (95% CI)
n (%) n (%)
CAC 1190 (56.7) 1302 (60.7) 1.00TGT 714 (34.0) 616 (28.7) 1.27 (1.11–1.45)CGT 152 (7.2) 176 (8.2) 0.94 (0.75–1.19)Others 42 (2.0) 52 (2.4) 0.88 (0.58–1.34)
aIn the order of FGFR2 rs2981582, rs1219648 and rs2420946.
FGFR2 polymorphisms and breast cancer
2343
at J.N. D
esmarais L
ibrary, Laurentian U
niversity on October 6, 2014
http://carcin.oxfordjournals.org/D
ownloaded from
r2 5 0.68 for rs2420946 and rs2981582 and r2 5 0.89 for rs1219648and rs2420946). Therefore, we performed haplotype inference onthese three polymorphisms. As shown in Table III, three commonhaplotypes were identified to account for .95% of all haplotypesconstructed by these three SNPs. Compared with the most commonhaplotype CAC, the TGT haplotype was associated with a 1.27-fold(95% CI 5 1.11–1.45) elevated risk of breast cancer.
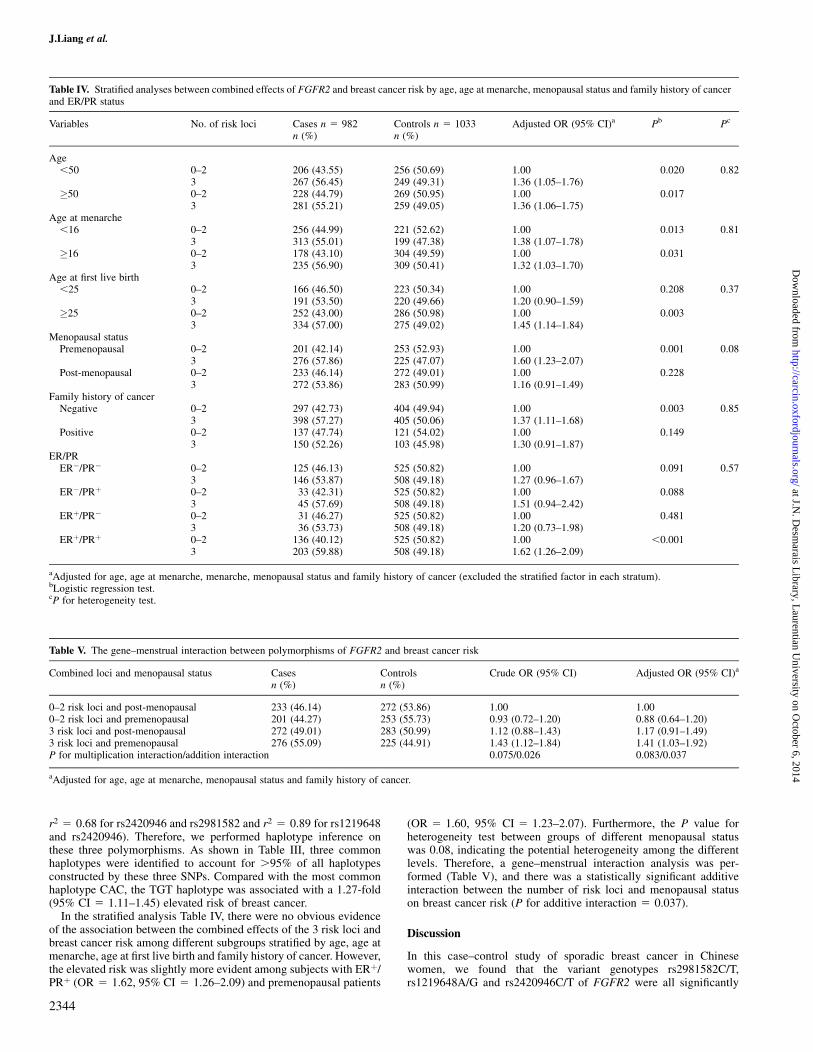
In the stratified analysis Table IV, there were no obvious evidenceof the association between the combined effects of the 3 risk loci andbreast cancer risk among different subgroups stratified by age, age atmenarche, age at first live birth and family history of cancer. However,the elevated risk was slightly more evident among subjects with ERþ/PRþ (OR 5 1.62, 95% CI 5 1.26–2.09) and premenopausal patients
(OR 5 1.60, 95% CI 5 1.23–2.07). Furthermore, the P value forheterogeneity test between groups of different menopausal statuswas 0.08, indicating the potential heterogeneity among the differentlevels. Therefore, a gene–menstrual interaction analysis was per-formed (Table V), and there was a statistically significant additiveinteraction between the number of risk loci and menopausal statuson breast cancer risk (P for additive interaction 5 0.037).
Discussion
In this case–control study of sporadic breast cancer in Chinesewomen, we found that the variant genotypes rs2981582C/T,rs1219648A/G and rs2420946C/T of FGFR2 were all significantly
Table IV. Stratified analyses between combined effects of FGFR2 and breast cancer risk by age, age at menarche, menopausal status and family history of cancerand ER/PR status
Variables No. of risk loci Cases n 5 982 Controls n 5 1033 Adjusted OR (95% CI)a Pb Pc
n (%) n (%)
Age,50 0–2 206 (43.55) 256 (50.69) 1.00 0.020 0.82
3 267 (56.45) 249 (49.31) 1.36 (1.05–1.76)�50 0–2 228 (44.79) 269 (50.95) 1.00 0.017
3 281 (55.21) 259 (49.05) 1.36 (1.06–1.75)Age at menarche
,16 0–2 256 (44.99) 221 (52.62) 1.00 0.013 0.813 313 (55.01) 199 (47.38) 1.38 (1.07–1.78)
�16 0–2 178 (43.10) 304 (49.59) 1.00 0.0313 235 (56.90) 309 (50.41) 1.32 (1.03–1.70)
Age at first live birth,25 0–2 166 (46.50) 223 (50.34) 1.00 0.208 0.37
3 191 (53.50) 220 (49.66) 1.20 (0.90–1.59)�25 0–2 252 (43.00) 286 (50.98) 1.00 0.003
3 334 (57.00) 275 (49.02) 1.45 (1.14–1.84)Menopausal status
Premenopausal 0–2 201 (42.14) 253 (52.93) 1.00 0.001 0.083 276 (57.86) 225 (47.07) 1.60 (1.23–2.07)
Post-menopausal 0–2 233 (46.14) 272 (49.01) 1.00 0.2283 272 (53.86) 283 (50.99) 1.16 (0.91–1.49)
Family history of cancerNegative 0–2 297 (42.73) 404 (49.94) 1.00 0.003 0.85
3 398 (57.27) 405 (50.06) 1.37 (1.11–1.68)Positive 0–2 137 (47.74) 121 (54.02) 1.00 0.149
3 150 (52.26) 103 (45.98) 1.30 (0.91–1.87)ER/PR
ER�/PR� 0–2 125 (46.13) 525 (50.82) 1.00 0.091 0.573 146 (53.87) 508 (49.18) 1.27 (0.96–1.67)
ER�/PRþ 0–2 33 (42.31) 525 (50.82) 1.00 0.0883 45 (57.69) 508 (49.18) 1.51 (0.94–2.42)
ERþ/PR� 0–2 31 (46.27) 525 (50.82) 1.00 0.4813 36 (53.73) 508 (49.18) 1.20 (0.73–1.98)
ERþ/PRþ 0–2 136 (40.12) 525 (50.82) 1.00 ,0.0013 203 (59.88) 508 (49.18) 1.62 (1.26–2.09)
aAdjusted for age, age at menarche, menarche, menopausal status and family history of cancer (excluded the stratified factor in each stratum).bLogistic regression test.cP for heterogeneity test.
Table V. The gene–menstrual interaction between polymorphisms of FGFR2 and breast cancer risk
Combined loci and menopausal status Cases Controls Crude OR (95% CI) Adjusted OR (95% CI)a
n (%) n (%)
0–2 risk loci and post-menopausal 233 (46.14) 272 (53.86) 1.00 1.000–2 risk loci and premenopausal 201 (44.27) 253 (55.73) 0.93 (0.72–1.20) 0.88 (0.64–1.20)3 risk loci and post-menopausal 272 (49.01) 283 (50.99) 1.12 (0.88–1.43) 1.17 (0.91–1.49)3 risk loci and premenopausal 276 (55.09) 225 (44.91) 1.43 (1.12–1.84) 1.41 (1.03–1.92)P for multiplication interaction/addition interaction 0.075/0.026 0.083/0.037
aAdjusted for age, age at menarche, menopausal status and family history of cancer.
J.Liang et al.
2344
at J.N. D
esmarais L
ibrary, Laurentian U
niversity on October 6, 2014
http://carcin.oxfordjournals.org/D
ownloaded from
associated with increased breast cancer risk. The associations ap-peared to be strongest in premenopausal women and those with ER/PR-positive tumors indicating that these variant genotypes may beinvolved in the etiology of breast cancer through pathways relatedto estrogen and/or progesterone.
The Breast Cancer Association Consortium genome-wide associa-tion study has identified FGFR2 rs2981582 in intron 2 as the mostsignificant breast cancer risk locus (7). Hunter et al. (12) conductedanother independent genome-wide association study and identifiedseveral novel low-penetrance loci of FGFR2 (rs1219648A/G andrs2420946C/T) that were associated with sporadic post-menopausalbreast cancer susceptibility in a group of women who were predom-inantly of European origin. However, premenopausal women were notincluded. During the manuscript was in preparation, Garcia-Closaset al. (15) conducted a stratified analysis on breast cancer risk andFGFR2 rs2981582 by clinical and pathological characteristics and
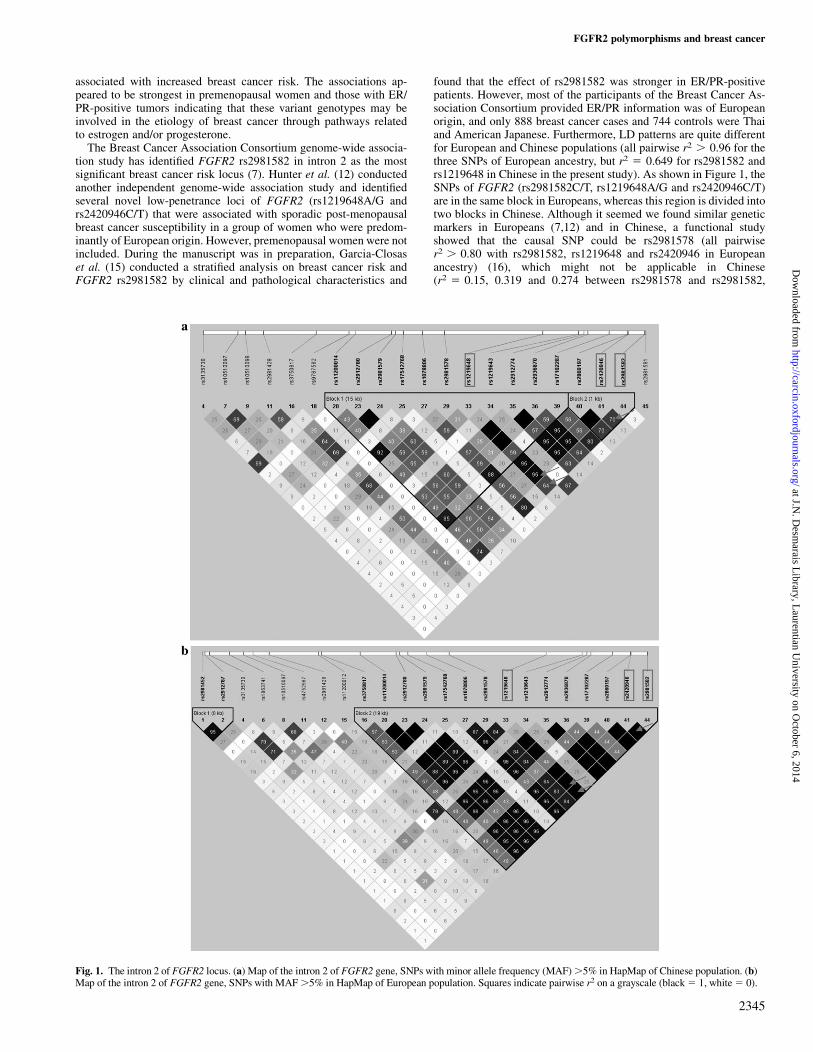
found that the effect of rs2981582 was stronger in ER/PR-positivepatients. However, most of the participants of the Breast Cancer As-sociation Consortium provided ER/PR information was of Europeanorigin, and only 888 breast cancer cases and 744 controls were Thaiand American Japanese. Furthermore, LD patterns are quite differentfor European and Chinese populations (all pairwise r2 . 0.96 for thethree SNPs of European ancestry, but r2 5 0.649 for rs2981582 andrs1219648 in Chinese in the present study). As shown in Figure 1, theSNPs of FGFR2 (rs2981582C/T, rs1219648A/G and rs2420946C/T)are in the same block in Europeans, whereas this region is divided intotwo blocks in Chinese. Although it seemed we found similar geneticmarkers in Europeans (7,12) and in Chinese, a functional studyshowed that the causal SNP could be rs2981578 (all pairwiser2 . 0.80 with rs2981582, rs1219648 and rs2420946 in Europeanancestry) (16), which might not be applicable in Chinese(r2 5 0.15, 0.319 and 0.274 between rs2981578 and rs2981582,
Fig. 1. The intron 2 of FGFR2 locus. (a) Map of the intron 2 of FGFR2 gene, SNPs with minor allele frequency (MAF) .5% in HapMap of Chinese population. (b)Map of the intron 2 of FGFR2 gene, SNPs with MAF .5% in HapMap of European population. Squares indicate pairwise r2 on a grayscale (black 5 1, white 5 0).
FGFR2 polymorphisms and breast cancer
2345
at J.N. D
esmarais L
ibrary, Laurentian U
niversity on October 6, 2014
http://carcin.oxfordjournals.org/D
ownloaded from

rs1219648 and rs2420946, respectively). In Chinese populations, finemapping and/or functional characterizations were warranted to de-termine the causal variants related to breast cancer risk.
FGFR2 is amplified and overexpressed in 10% of human breastcancers (10), but different splicing isoforms may also lead to differ-ential transforming activities in human mammary epithelial cells (12).Therefore, it is biologically plausible that genetic variants in intron 2of FGFR2 or nearby may be important in breast cancer etiology,although the detailed mechanism needs to be explored further.
It has long been hypothesized that high levels of endogenoussex hormones, especially estrogens, may increase breast cancer risk(17). Further, post-menopausal hormone replacement therapy withestrogen/progesterone combinations is associated with greater riskof breast cancer than use of estrogen alone (18). Menstrual and re-productive factors, including early age at menarche and later age atfirst birth, which might be indicators of endogenous sex hormoneslevels, are recognized breast cancer risk factors (3,19,20). For exam-ple, menarche can induce proliferation of breast cells (19), whereaspregnancy can induce differentiation of breast tissue through mediat-ing levels of endogenous sex hormones (21–23). In premenopausalwomen, the ovaries are the predominant source of serum estrogen, andexposure is much higher than for post-menopausal women (23).
FGFR2 has been reported to be significantly more likely to beupregulated in ERa-positive breast tumors compared with ERa-negative breast tumors (24). Keratinocyte growth factor and keratino-cyte growth factor receptor (KGFR, FGFR2IIIb) act as growth factorsmediating estrogen action, and their expression, which is ER depen-dent, significantly correlates with an antiapoptotic role in humanbreast cancer (25). Furthermore, in mouse mammary glands, KGFRexpression is determined by the ratio of estradiol and progesterone,indicating a mechanism through which these hormones can cooperateto optimize their growth-promoting effects (26). Our findings that thecombined effects of FGFR2 variants are greater in ER-positive and/orPR-positive breast cancer and FGFR2 variants interact with meno-pausal status appear to be consistent with an activity that is hormon-ally mediated. Further studies are warranted to explore the role ofFGFR2 variants in mediating apoptosis, proliferation and differenti-ation of breast cells, together with estrogen and progesterone.
In conclusion, this is the first study to demonstrate that geneticvariants in intron 2 of FGFR2 are significantly associated withincreased risk of breast cancer in Chinese women, possibly associ-ated with the status of hormone receptors and the reproductivehistory of women. Considering the different LD block patternsamong populations, we called for a fine mapping of this region indifferent populations.
Funding
Innovative Key Grant of Department of Education (#705023);National Key Basic Research Program Grants (2002CB512908);Program for Changjiang Scholars and Innovative Research Team inUniversity (IRT0631); Jiangsu Society Development Foundation(BS2006006); 863 program (2007AA02Z474); Science and Technol-ogy Commission of Shanghai Municipality (06DZ19021); PujiangTalent Program (06PJ14107).
Acknowledgements
We would like to thank Prof. E.R.Greenberg of the Fred Hutchinson CancerResearch Center for his scientific editing and our collaborators in the Depart-ment of General Surgery, Jiangsu Cancer Hospital (Jianwei Qin) and in theDepartment of General Surgery (Shui Wang), The First Affiliated Hospital ofNanjing Medical University.
Conflict of Interest Statement: None declared.
References
1.Parkin,D.M. et al. (2005) Global cancer statistics, 2002. CA CancerJ. Clin., 55, 74–108.
2.Yang,L. et al. (2005) Estimates of cancer incidence in China for 2000 andprojections for 2005. Cancer Epidemiol. Biomarkers Prev., 14, 243–250.
3.Kelsey,J.L. et al. (1991) The epidemiology of breast cancer. CA CancerJ. Clin., 41, 146–165.
4.McPherson,K. et al. (2000) ABC of breast diseases. Breast cancer-epidemiology, risk factors, and genetics. BMJ, 321, 624–628.
5.Bray,F. et al. (2004) The changing global patterns of female breast cancerincidence and mortality. Breast Cancer Res., 6, 229–239.
6.Chen,Y.C. et al. (2005) Molecular epidemiology of cancer. CA CancerJ. Clin., 55, 45–54.
7.Easton,D.F. et al. (2007) Genome-wide association study identifies novelbreast cancer susceptibility loci. Nature, 447, 1087–1093.
8.Ricol,D. et al. (1999) Tumour suppressive properties of fibroblast growthfactor receptor 2-IIIb in human bladder cancer. Oncogene, 18, 7234–7243.
9.Tannheimer,S.L. et al. (2000) Characterization of fibroblast growth factorreceptor 2 overexpression in the human breast cancer cell line SUM-52PE.Breast Cancer Res., 2, 311–320.
10.Adnane,J. et al. (1991) BEK and FLG, two receptors to members of theFGF family, are amplified in subsets of human breast cancers. Oncogene, 6,659–663.
11. Ingersoll,R.G. et al. (2001) Fibroblast growth factor receptor 2 (FGFR2):genomic sequence and variations. Cytogenet. Cell Genet., 94, 121–126.
12.Hunter,D.J. et al. (2007) A genome-wide association study identifies allelesin FGFR2 associated with risk of sporadic postmenopausal breast cancer.Nat. Genet., 39, 870–874.
13.Wang,Y. et al. (2007) EGF promoter SNPs, plasma EGF levels and risk ofbreast cancer in Chinese women. Breast Cancer Res. Treat., 111, 321–327.
14.Terra,S.G. et al. (2005) Beta-adrenergic receptor polymorphisms and re-sponses during titration of metoprolol controlled release/extended releasein heart failure. Clin. Pharmacol. Ther., 77, 127–137.
15.Garcia-Closas,M. et al. (2008) Heterogeneity of breast cancer associationswith five susceptibility loci by clinical and pathological characteristics.PLoS Genet., 4, e1000054.
16.Meyer,K.B. et al. (2008) Allele-specific up-regulation of FGFR2 increasessusceptibility to breast cancer. PLoS Biol., 6, e108.
17.Key,T. et al. (2002) Endogenous sex hormones and breast cancer in post-menopausal women: reanalysis of nine prospective studies. J. Natl CancerInst., 94, 606–616.
18.ESHRE Capri Workshop Group. (2004) Hormones and breast cancer. Hum.Reprod. Update, 10, 281–293.
19.Clavel-Chapelon,F. (2002) Differential effects of reproductive factors onthe risk of pre- and postmenopausal breast cancer. Results from a largecohort of French women. Br. J. Cancer, 86, 723–727.
20.Gao,Y.T. et al. (2000) Association of menstrual and reproductive factorswith breast cancer risk: results from the Shanghai Breast Cancer Study. Int.J. Cancer, 87, 295–300.
21.Li,C.I. et al. (2008) Timing of menarche and first full-term birth in relationto breast cancer risk. Am. J. Epidemiol., 167, 230–239.
22.Krieger,N. (1989) Exposure, susceptibility, and breast cancer risk: a hypoth-esis regarding exogenous carcinogens, breast tissue development, and so-cial gradients, including black/white differences, in breast cancerincidence. Breast Cancer Res. Treat., 13, 205–223.
23.Clemons,M. et al. (2001) Estrogen and the risk of breast cancer. N. Engl.J. Med., 344, 276–285.
24.Tozlu,S. et al. (2006) Identification of novel genes that co-cluster withestrogen receptor alpha in breast tumor biopsy specimens, using a large-scale real-time reverse transcription-PCR approach. Endocr. Relat. Cancer,13, 1109–1120.
25.Tamaru,N. et al. (2004) Estrogen receptor-associated expression of kerati-nocyte growth factor and its possible role in the inhibition of apoptosis inhuman breast cancer. Lab. Invest., 84, 1460–1471.
26. Imagawa,W. et al. (2001) In vivo inhibition of keratinocyte growth factorreceptor expression by estrogen and antagonism by progesterone in themouse mammary gland. J. Endocrinol., 171, 319–327.
Received June 19, 2008; revised September 15, 2008;accepted September 30, 2008
J.Liang et al.
2346
at J.N. D
esmarais L
ibrary, Laurentian U
niversity on October 6, 2014
http://carcin.oxfordjournals.org/D
ownloaded from







![2016 Gastric Cancer: Global view Fibroblast growth factor ... · to their ligands, the fibroblast growth factors (FGFs), with high affinity[11]. FGFR1, FGFR2, and FGFR3 are divided](https://img.dokumen.tips/doc/110x75/5ee06d96ad6a402d666b9d16/2016-gastric-cancer-global-view-fibroblast-growth-factor-to-their-ligands.jpg)