Embed Size (px)
Citation preview

Urologic Oncology: Seminars and Original Investigations ] (2014) ∎∎∎–∎∎∎
http://dx.doi.org/10.1016/j1078-1439/r 2014 Elsev
Support was provided(PC094516 to F.D.) and(IG13562 to F.D.). AdHutchinson Cancer ReseFoundation, USA (J.L.S.)
* Corresponding authorE-mail addresses: demi
@gmail.com (F. Demiche
Seminar article
Genetic predisposition to prostate cancer: Update and future perspectives
Francesca Demichelis, Ph.D.a,b,c,*, Janet L. Stanford, M.P.H., Ph.D.d,e
a Centre for Integrative Biology, University of Trento, Trento, Italyb Institute for Computational Biomedicine, Weill Medical College of Cornell University, New York, NY
c Institute for Precision Medicine, Weill Medical College of Cornell University and New York Presbyterian Hospital, New York, NYd Division of Public Health Sciences, Fred Hutchinson Cancer Research Center, Seattle, WA
e Department of Epidemiology, School of Public Health, University of Washington, Seattle, WA
Received 19 December 2013; received in revised form 27 April 2014; accepted 28 April 2014
Abstract
Objective: Prostate cancer is the second most frequent cancer in men worldwide and kills over 250,000 men worldwide every year.Prostate cancer is a heterogeneous disease at the clinical and the molecular level. The Scandinavian Twin Registry Study demonstrated thatin contrast to most malignancies where environment was the overriding influence, heritable factors account for more than fifty percent ofprostate cancers.Methods and materials: We review the literature on prostate cancer risk variants (rare and common) including SNPs and Copy Number
Variants (CNVs) and discuss the potential implications of significant variants for prostate cancer patient care.Results: The search for prostate cancer susceptibility genes has included both family-based studies and case-control studies utilizing a
variety of approaches from array-based to sequencing-based studies. A major challenge is to identify genetic variants associated with moreaggressive, potentially lethal prostate cancer and to understand their role in the progression of the disease.Conclusion: Future risk models useful in the clinical setting will likely incorporate several risk loci rather than single variants and may be
dependent on an individual patient’s ethnic background. r 2014 Elsevier Inc. All rights reserved.
Keywords: Prostate cancer risk; Common variants; Rare variants; SNP; CNV
Introduction
Prostate cancer is the leading cause of cancer (excludingnonmelanoma skin cancer) in the United States and issecond only to lung cancer as the most frequent cancer inmen worldwide. In terms of mortality, prostate cancer rankssecond in the United States and sixth internationally as acause of cancer-related death in men. Each year prostatecancer kills approximately 30,000 men in the United States
.urolonc.2014.04.021ier Inc. All rights reserved.
by the U. S. Department of Defense, USAby the Italian Association for Cancer Researchditional support was provided by the Fredarch Center, USA and the Prostate Cancer.. Tel.: þ39-461-285305; fax: þ[email protected], francesca.demichelislis).
and more than 250,000 men worldwide [1,2]. Recentrelative survival data from the United States indicate thatapproximately 1 in 11 (9%) patients with prostate cancerwill die of their disease over the 15-year period followingdiagnosis [3].
Prostate cancer is a heterogeneous disease that exhibits arange of clinical behaviors, from indolent, slow-growingtumors to aggressive, fast-growing tumors with lethal pro-gression. Although most tumors follow an indolent clinicalcourse and may not cause morbidity even if left untreated,most clinically localized tumors are treated with curative intentvia surgery or radiation. Even with such treatment, however,up to 30% of tumors recur during long-term follow-up [4,5].Unfortunately, features of localized prostate cancer, such asclinical stage, prebiopsy prostate-specific antigen (PSA) level,and tumor grade (Gleason score), are not adequate for accu-rately distinguishing aggressive from indolent prostate cancer,especially in the intermediate risk category that represents

F. Demichelis, J.L. Stanford / Urologic Oncology: Seminars and Original Investigations ] (2014) 1–102
most cases diagnosed in recent years. Thus, research focusedon discovery, validation, and understanding of the molecularalterations and biological mechanisms that drive prostatetumor progression toward lethality is urgently needed.
Genetic predisposition to prostate cancer
Familial clustering of prostate cancer was reported in1956 [6], but definitive evidence for an inherited form of thedisease did not appear until 1992 when the first segregationanalysis was completed [7]. Subsequent segregation studies,twin studies, case-control, and cohort studies provide strongsupport for a genetic predisposition to prostate cancer [8,9],with risk increasing 2- to 3-fold for men with a familyhistory of the disease in a first-degree relative. The relativerisk (RR) is further increased, 3- to 5-fold higher, if therelative was diagnosed before 65 years of age or if there are2 or more relatives with prostate cancer. Family history isone of the indications for the initiation of PSA screening atyounger ages for the early detection of prostate cancer [10].A recent analysis of data from the Scandinavian twinregistry of cancer estimates the heritability of prostatecancer to be 58% (95% CI: 52%–63%), which is higherthan the 42% (95% CI: 29%–50%) initial estimate ofincidence due to heritable factors [11,12].
The search for prostate cancer–susceptibility genes hasincluded both family-based studies aimed at finding rare,moderate- to high-penetrance genetic variants or mutationsthat lead to hereditary prostate cancer (HPC) or familialprostate cancer, and case-control association studies focusedon discovery of common, low-penetrance genetic variantsassociated with disease risk in the general population. Untilrecently, these studies were stymied by the lack oftechnology, but the availability of dense array-basedgenomic platforms and next-generation sequencing hasaccelerated discovery and characterization of molecularvariants associated with prostate cancer.
Table 1Variants associated with aggressive or lethal prostate cancer that were validated
Gene End point SNP/gen(GRCh37
DAB2IP Aggressive PCa (at diagnosis) rs157180HERC2 Aggressive PCa (at diagnosis or evidence of
progression)rs649728
LOC100505495 Aggressive PCa (at diagnosis) rs116726Intergenic Aggressive PCa (at diagnosis) chr15:54Intergenic PCa mortality (metastases or death) rs697381LEPR PCa mortality (death) rs113710RNASEL PCa mortality (death) rs627839IL4 PCa mortality (death) rs207087CRY1 PCa mortality (death) rs107785ARVCF PCa mortality (death) rs599389
PCa ¼ prostate cancer.
Common germ-line genetic variation
Single-nucleotide polymorphisms
Single-nucleotide polymorphisms (SNPs) representinherited DNA variations that have been associated withprostate cancer. Genome-wide association studies (GWAS)have found more than 90 common SNPs (minor allelefrequency [MAF], 5% or greater) that are confirmed to beassociated with weak to modest alterations (average perallele odds ratios [ORs]: 1.1–1.3) in overall risk of prostatecancer [13–20]. Taken together, these SNPs are estimated toexplain about a third of the overall inherited risk of prostatecancer [15]. However, these GWAS risk–associated SNPsare not uniquely associated with clinically aggressiveprostate cancer. This may be owing to the fact that mostearly GWAS were underpowered to address aggressivenessdue to the inclusion of predominantly cases with moreindolent tumors.
Several studies have been completed (Table 1) thatspecifically focused on prostate cancer cases meetingaggressiveness criteria either based on pathoclinical featuresat time of diagnosis (e.g., higher tumor stage, grade, andPSA level) or on evidence of disease progression (e.g.,metastasis) or prostate cancer–specific mortality (PCSM).Results highlighted some SNPs that were associated withthe aggressive phenotype but were also associated with theindolent form of the disease [15,21]. A small GWAS ofcases (n = 202) with aggressive disease features, diseaseprogression, or fatal prostate cancer found a SNP onchromosome 15q13 (rs6497287) that was confirmed to bemost strongly associated with aggressive prostate cancer[22]. In the largest meta-analysis to date, Al Olama et al.[16] analyzed 5,953 cases of aggressive prostate cancerdefined as Gleason 7 or greater or regional/distant stage and11,463 controls. The investigators found 1 association(rs11672691) for a locus on chromosome 19q13 that wasslightly stronger in the subset of cases with aggressive
in independent study populations
omic region/hg19)
Relative risk or Hazardratio (95% CI)
References
1 1.36 (1.13–1.63) Duggan et. al. [21]7 1.46 (1.10–1.94) Fitzgerald et al. [22]
91 1.12 (1.03–1.21) Al Olama et al. [16]197663-54203357 1.42 (1.00–2.02) Demichelis et al. [54]4 1.95 (1.01–3.79) Penney et al. [23]0 0.82 (0.67–1.00) Lin et al. [24]
1.22 (1.00–1.50) Lin et al. [24]4 1.27 (1.04–1.56) Lin et al. [24]34 1.23 (1.00–1.51) Lin et al. [24]1 0.72 (0.52–1.01) Lin et al. [24]

F. Demichelis, J.L. Stanford / Urologic Oncology: Seminars and Original Investigations ] (2014) 1–10 3
disease (OR ¼ 1.12, 95% CI: 1.03–1.21) compared with allcases combined(OR ¼ 1.08, 95% CI: 1.05–1.12), but the difference wasnot significant.
Lethal prostate cancer is the most clinically importantphenotype, but the number of such cases included in geneticstudies to date is limited. A small GWAS (n ¼ 196 cases)of PCSM found a variant on chromosome 7q11 (rs6973814)that was borderline significant in a replication data set [23].In another analysis of SNPs in genes from defined bio-logical pathways hypothesized to affect prostate cancerprogression, a recent study found 22 genetic variants tobe significantly associated (P r 0.01) with PCSM, and 5SNPs were validated in a large independent patient cohortwith prostate cancer [24]. These results require furthervalidation, but emphasize the importance of studies focusedon the subset of patients with the most aggressive, lethalform of the disease.
Importantly, although common SNPs only confer weakto modest risk to prostate cancer, some studies indicate thatif a man carries multiple risk alleles, the risk increases [15] .Lindstrom et al. [25] showed that men in the highest 10thpercentile of the study risk allele counts had a 7-fold risk ofprostate cancer at age 65 or younger (OR ¼ 7.21, 95% CI:5.66–9.18). The estimated risk for men in the top 1% of therisk distribution was 4.4-fold greater than the populationaverage risk using 68 known prostate cancer–susceptibilityloci [15]. This estimate of risk is similar to that observed inmen with a strong family history of the disease. In a case-control study of Ashkenazi Jews from Agalliu et al. [26],the highest vs. lowest quartile of cumulative number of riskalleles demonstrated an OR of 3.76 (95% CI: 2.57–5.50) foraggressive disease defined by pathoclinical features at thetime of diagnosis.
Inherited copy-number variants
Although SNPs have long been considered powerfulmarkers to identify genetic loci that contribute to theetiology of human diseases, over the last few years a newform of common genetic variation is being appreciated—referred to as structural genomic variants. Although knownto exist at the cytogenetic and molecular levels for sometime [27], their prevalence on a genome-wide scale was notdiscovered until 2006 from 2 independent groups [28,29].Unbalanced structural genomic variants (involving loss orgain of genetic material) are referred to as copy-numbervariants (CNVs) [30,31] and are currently estimated toencompass more than 6% of human reference DNA [32].Like SNPs, they exert direct and indirect effects on genetranscription [33,34].
Before discovery of large-scale variations in the genome[28,29], specific germ-line CNVs were shown to causesporadic and highly penetrant Mendelian diseases [35–37].More recently, CNVs are being increasingly shown to beassociated with complex diseases (recently reviewed [38,39]),
neurological diseases, such as Alzheimer disease, Parkinsondisease, mental retardation, autism, bipolar disorder, andschizophrenia [40], including graft-vs.-host disease [41].
As CNVs carry information independent of SNPs, fewemerging studies have addressed germ-line CNVs as play-ers in conferring cancer risk. Frank et al. [42] examined 593breast cancer cases and 732 controls from a Germanpopulation and showed that a deletion of exon 4 of themitochondrial tumor suppressor 1 (MTUS1) gene wasassociated with a decreased risk of familial and nonfamilialbreast cancer. The first genome-wide study of germ-lineCNVs and cancer risk was carried out by Shlien et al. [43]who showed an association between increased frequency ofgerm-line CNVs and risk of Li-Fraumeni syndrome. ACNV at 1q21.1 [44] showed an association with neuro-blastoma in a 2-stage case-control study and a 11q11 losswas suggested as a candidate susceptibility variant forcolorectal cancer [45].
The contribution of germ-line CNVs to prostate can-cer risk has also been investigated, providing an additionallayer of complexity to prostate cancer genetics. Cybulskiet al. [46] showed that a deletion in exons 9 and 10 of theChek2 kinase gene (CHEK2) was associated with anincreased risk for prostate cancer. Given their role in ste-roid metabolism and the high frequency of the polymor-phisms, multiple studies focused on the role of uridinediphosphoglucuronosyltransferase (UGT) genes from the2B subclass. Specifically, UGT2B17 mediates the glucuro-nidation and subsequent clearance of dihydrotestosterone inthe basal cells, whereas UGT2B15 mediates the clearance ofT and dihydrotestosterone in the luminal epithelial cells[47]. Some suggested homozygous deletions of UGT2B17are associated with increased risk [48–51], but overall datahave been conflicting possibly owing to the complexity ofthe genomic region and gene family homologies that mightimpair study assays [47] or by nonhomogeneous studycohorts.
To date, the largest study aimed at assessing the role ofconstitutional CNVs and prostate cancer risk was conductedon approximately 2,000 men from the Tyrol Early ProstateCancer Detection Program cohort [52,53], a population-based prostate cancer screening program started in 1993and intended to evaluate the utility of intensive PSA screen-ing in reducing prostate cancer–specific death. A total of 238low-frequency biallelic CNVs were analyzed. Of the top-ranked risk CNVs, 2 were validated in an independent cohortand further characterized [54]. The first risk locus maps to15q21.3 (P ¼ 7.7 � 10�4, OR ¼ 2.78) and overlaps anoncoding enhancer element that contains multiple AP-1transcription factor–binding sites. The second risk locus(P ¼ 2.6 � 10�3, OR ¼ 4.8) maps to the alpha-1,3-mannos-yl-glycoprotein 4-beta-N-acetylglucosaminyltransferase C(MGAT4C) gene on 12q21.31. In vitro cell line assaysfound this gene to significantly modulate cell proliferationand migration in both benign and prostate cancer cells.Further, MGAT4C was significantly overexpressed in

F. Demichelis, J.L. Stanford / Urologic Oncology: Seminars and Original Investigations ] (2014) 1–104
metastatic vs. localized prostate cancer. These 2 riskassociations were replicated in an independent PSA-screened cohort of 800 men (15q21.3, combined P ¼0.006; 12q21.31, combined P ¼ 0.026). These findingsestablish noncoding and coding germ-line CNVs as sig-nificant risk factors for prostate cancer susceptibility andimplicate their role in disease development and progression.
Taken together, these preliminary data suggest a key rolefor germ-line CNVs in prostate cancer progression.
Rare germ-line genetic variation
Less common SNPs (MAF 1%–5%) and rare (MAF o1%)single-nucleotide variants are hypothesized to confer stron-ger effect sizes on disease risk than common geneticvariants; and, rarer variants likely account for some of themissing disease heritability. To discover such variants,however, alternative approaches to GWAS are needed.One such approach focuses on familial or HPC families,where inherited genetic risk associated with less frequentmutations is concentrated. Estimates indicate that 5% to10% of all prostate cancer incidence is because of inher-itance of rare predisposition alleles.
Of the 2 dozen or more putative loci identified fromfamily-based linkage studies of HPC, only a few havebeen shown to harbor genes with disease-associatedmutations [8]. In 1996, the first HPC-specific locus wasmapped to chromosome 1q24-25 [55], with subsequentattribution of the linkage signal to rare mutations in theRNASEL gene [56] that were observed in 1.4% of HPCfamilies tested. Another linkage region on chromosome22q12 that was highlighted in multiple HPC studies led toidentification of risk-associated gene variants in theApolipoprotein L3 (APOL3) gene [57]. However, mostof the suggested linkage signals have not led to identi-fication of specific genetic variants or mutations. Next-generation sequencing approaches, however, have recentlyresulted in discovery of genes with specific missensechanges that associate with both hereditary and sporadicprostate cancer.
In 2012, Ewing et al. [58] focused on a prostate cancer–susceptibility locus on 17q21-22, which was previouslyfound through linkage analysis. Targeted sequencing of 202genes in the 17q21-22 region in members of 94 families (85of European ancestry) with evidence for linkage to theregion resulted in identification of a rare variant in a genecoding for the transcription factor HOXB13 in 3 to 6affected men from 4 of these HPC families (Table 2). Thisgene was previously implicated in prostate developmentand was included in a 21-gene signature predictive of lethalprostate cancer when adjusted for clinical parameters [59].The missense change (rs13821319, G84E) was foundoverall in 1.4% of prostate cancer cases and in 0.1% ofunaffected controls (P ¼ 8.5 � 10�7), with a strongersignal in men with early-onset disease [58]. A confirmation
study that utilized 2,443 HPC families from the Interna-tional Consortium for Prostate Cancer Genetics confirmedthat 4.8% of HPC families of European ancestry have atleast one carrier of the HOXB13 missense mutation [60].Both affected and unaffected men in these families werefound to carry the G84E mutation, and there was asubstantial geographic variation in carrier frequency (0%–
22.4%) across regions represented by the 15 InternationalConsortium for Prostate Cancer Genetics groups contribu-ting data, with the highest frequency observed amongfamilies from Finland and Sweden.
Several subsequent studies of the G84E mutation indiverse populations confirm its association with prostatecancer. A recent meta-analysis of 7 studies [61] reportedthat HOXB13 G84E was associated with a 4-fold elevationin the risk of prostate cancer (OR ¼ 4.07, 95% CI: 3.05–5.45); estimates were similar for less aggressive (OR ¼3.90) and more aggressive (OR ¼ 3.65) prostate cancerphenotypes. In the population-based studies, the frequencyof the G84E variant was 1.3% to 4.4% in prostate cancercases and 0.4% to 1.3% in age-matched controls [62,63]. Toassess the potential utility of assessing G84E carrier statusto identify men at high risk of the disease, the researchgroup that first reported this mutation in high-risk HPCfamilies genotyped a cohort of 948 unselected men under-going diagnostic prostate biopsy. The G84E variant wasdetected in 4 (0.4%) men, and 3 of the 4 (75%) carriers hadprostate cancer on biopsy. However, none of the 301 menwith a family history of the disease and only 0.4% of themen r55 years of age tested positive [64]. These data donot support G84E testing of unselected men to identifythose at high risk. However, as more variants, particularlythose that confer moderate to large effect sizes, associatedwith elevated risk are identified, it may be possible todevelop an integrated panel of multiple rare genetic variantsthat will be clinically useful to target screening andprevention strategies to appropriate subsets of the popu-lation.
In an effort to find additional rare germ-line variantsassociated with prostate cancer susceptibility, a whole-exome sequencing project was recently completed. FitzGeraldet al. [65] sequenced 80 men with prostate cancer and 11 oftheir relatives without prostate cancer from 19 HPCfamilies (Table 2). Of the 196 candidate single-nucleotidevariants/indels remaining after data filtering, 2 missensevariants (rs41441651 in exon 5, D336N and rs28362675 inexon 6, G454C) in the BTNL2 gene were found morefrequently in 819 prostate cancer cases (1.5%) than in 496male relatives without prostate cancer (none carried eithervariant; P ¼ 0.0032) in 270 independent HPC families.Genotyping of the 2 missense variants in 1,155 population-based prostate cancer cases and 1,060 age-matched controlsfrom the same general population revealed that �2%of cases and 0.9% of controls carried one or both variants(OR ¼ 2.73, 95% CI: 1.27–5.87 for rs41441651). This is thefirst data suggesting a role in prostate cancer susceptibility for

Table 2Results from next-generation sequencing studies of rare germ-line genetic variants and prostate cancer risk in men of European ancestry
Gene SNV (amino acidchange)
Study phase No. of PCa cases No. of carriers,frequency (%)
No. ofcontrols
No. of carriers,frequency (%)
Relative riskestimate(95% CI)
Comments References
HOXB13 rs138213197(G84E)
Discovery 85 HPC cases 4 (4.7) Ewing et al. [58]
Confirmation 5,083 Unrelated cases 72 (1.4) 1,401 1 (0.1) 20.1 (3.5–803.3) Subset with a familyhistory of PCa orearly age at diagnosis(r55 y) hadhigher risk estimates
6,422 HPC cases 194 (3.0) 3,705 Family-based
89 (2.4) 4.3a (2.3–8.0) Study included 2,443HPC families
Xu et al. [60]
BTNL2 rs41441651(D336N)
Discovery 80 HPC cases 10 (12.5) FitzGerald et al. [65]
rs28362675(G454C)
Confirmation 819 HPC cases 12 (1.5) forrs4144651
496 Family-based 0 P ¼ 0.0032 forrs4144651
Study included 270 HPC families
10 (1.2) forrs2836275
P ¼ 0.007 forrs28362675
1,155 Population-based cases
26 (2.3) 1,060 Population-based
9 (0.9) 2.7 (1.3–5.9) forrs4144651
24 (2.1) 9 (0.9) 2.5 (1.2–5.5) forrs28362675
PCa ¼ prostate cancer; SNV ¼ single-nucleotide variant.aRelative risk estimate based only on the 96 HPC families with at least one carrier of the G84E mutation (154 of 326 prostate cancer cases and 36 of 117 unaffected controls from the 112 families carried the
mutation).
F.Dem
ichelis,J.L
.Stanford
/Urologic
Oncology:
Seminars
andOriginal
Investigations](2014)
1–10
5

F. Demichelis, J.L. Stanford / Urologic Oncology: Seminars and Original Investigations ] (2014) 1–106
BTNL2, a gene thought to be involved in immune regulationvia inhibition of T-cell activation; confirmation in other studypopulations is awaited (Table 2).
Several other candidate genes with rare variants ormutations associated with prostate cancer have been sug-gested (e.g., RNASEL [56], MSR1 [66], and ELAC2 [67]),but confirmatory evidence from follow-up studies has beenweak. Recent studies of BRCA1 and BRCA2, however,provide some support for their role as prostate cancerpredisposition genes. Leongamornlert et al. [68] screenedthe entire coding region of the BRCA1 gene in 886 prostatecancer cases (90% were r65 y of age at diagnosis) andidentified 4 with distinct deleterious mutations for afrequency of 0.45%. These investigators utilized a priorestimate of the prevalence of BRCA1 mutations in the U.K.population to calculate a RR estimate of 3.75 (95% CI:1.02–9.6) for prostate cancer associated with rare germ-linemutations in BRCA1. However, the majority of studies havenot found an association of BRCA1 mutations with risk ofprostate cancer. The Breast Cancer Linkage Consortium[69] study of 173 breast-ovarian cancer families withBRCA2 mutations estimated that men in these familieswho were probable carriers had a RR of 4.65 (95% CI:3.48–6.22), which was stronger in men younger than 65years (RR ¼ 7.33, 95% CI: 4.66–11.52). Edwards et al.[70] then screened the complete coding sequence of BRCA2in 263 patients with early-onset (r55 y at diagnosis)prostate cancer and found 6 (2.3%) who carried protein-truncating mutations in the gene; only 1 carrier reported afamily history of prostate cancer and 2 reported a familyhistory of breast-ovarian cancer. In a subsequent study,Agalliu et al. [71] screened 257 population-based prostatecancer cases of European ancestry who were diagnosedbefore 55 years of age and found 2 (0.78%) carriers ofdistinct protein-truncating BRCA2 mutations in exon 11(RR ¼ 7.8, 95% CI: 1.8–9.4). The same group ofinvestigators also screened 253 men with prostate cancerfrom 194 HPC families [72]. The cases had a median age atdiagnosis of 58 years, and almost half had a moreaggressive phenotype (i.e., regional or distant stage, Glea-son score 7–10, diagnostic PSA level 420 ng/ml, or PCSMbefore 65 y of age). No BRCA2 mutations were found incases from these high-risk HPC families. Similar negativeresults were reported from 2 other studies of BRCA2mutations in HPC families [73,74], but another study of38 cases from HPC families found 2 (5.3%) mutationcarriers [75].
To further evaluate the association of BRCA2 withprostate cancer in Ashkenazi Jewish men, Agalliu et al.[76] screened 979 cases and 1,251 controls for the6174delT founder mutation in BRCA2. An increased riskfor mutation carriers was observed (OR ¼ 1.9, 95% CI:0.9–4.1), but it was significant only in those with higher-grade tumors defined as Gleason score 7 to 10 (OR¼ 3.2;95% CI: 1.4–7.3). In another recent study, Kote-Jarai et al.[77] screened 1,864 sporadic prostate cancer cases in the
United Kingdom for BRCA2 mutations and found 19mutation carriers, all of whom were diagnosed at r65years of age. Comparing the mutation frequency (1.2%) inthese earlier-onset cases with that in the general U.K.population (0.16%), these investigators estimated a RR of8.6 (95% CI: 5.1–12.6). Of the 19 mutation carriers, 12(63%) had high-grade tumors (Gleason score Z 8) and 8(42%) died of prostate cancer. Most carriers also had afamily history of prostate cancer (63%) or breast-ovariancancer (53%). Overall, evidence suggests that BRCA1mutations do not play a major role in prostate cancer, butrare, deleterious mutations in BRCA2 are associated withhigher risk for early-onset (r55 y) or more aggressiveprostate cancer [78].
The first international, multicenter effort evaluating therole of targeted PSA screening in men with BRCA1/2mutations (IMPACT study, Identification of Men with agenetic predisposition to ProstAte Cancer: Targeted screen-ing in BRCA1/2 mutation carriers and controls) recentlyreported [79] on the first year's screening round for all menenrolled from October 2005 to February 2013. The studyshowed a positive predictive value for biopsy using a PSAthreshold of 3.0 ng/ml in BRCA2 mutation carriers of 48%,2-fold more than the value from population screeningstudies, supporting the utility of rare germ-line geneticmarkers for targeted screening.
Elucidating molecular mechanisms of genetic variation
Strategies exploiting technological advances andgenome-wide annotation of the human genome have beenrecently pursued to formulate and test hypotheses on thebiological and functional meaning of prostate cancer–riskloci. International coordinated efforts, such as the Encyclo-pedia of DNA Elements (ENCODE) project [80], nowprovide enormous resources to the research community.Through hundreds of experiments on various platforms anddiverse biological samples, the purpose of ENCODE is todelineate all functional elements encoded in the humangenome, thus providing complete annotations of histonemarks, methylation marks, DNAase sites, and transcriptionfactors–binding sites [15,54]. The ENCODE annotationswill provide more insight into GWAS SNPs or CNVsassociated with risk but in noncoding areas that currentlyhave no known function or regulatory roles.
By combining risk loci information and relevant (tissue-specific) transcript data, another strategy to start elucidatingthe meaning of prostate cancer–risk loci is to search for cis-expression quantitative trait loci (cis-eQTL). eQTL analy-ses are based on the hypothesis that risk loci may containvariants located within regulatory elements, thereforemodulating expression levels of nearby genes, as suggestedby evidence of enrichment of genome-wide phenotype-associated SNPs in cis-eQTLs [81]. Recently, Grisanzioet al. [82] reported 5 cis-eQTLs in prostate tissue that alter

F. Demichelis, J.L. Stanford / Urologic Oncology: Seminars and Original Investigations ] (2014) 1–10 7
expression of nearby genes. Similarly, Xu et al. [83] testeda total of 586 transcript-genotype associations while con-sidering a set of 59 risk loci and a prostate tissue transcriptdata set from men of European ancestry. The iroquoishomeobox protein 4 (IRX4) was identified as the strongesteQTL's gene target for the rs12653946 variant located on5p15.33 and previously detected by Nguyen et al. [84] in aJapanese cohort. An additional eQTL signal was detectedfor NCOA4, a known androgen receptor coactivator [85],and for NUDT11 [82], a diphosphoinositol polyphosphatephosphohydrolase.
A more direct approach to pinpoint the role of candidatefunctional risk variants has been adopted to characterizelong-range interactions of variants within the 8q24 haplo-type block. Multiple common SNPs within the 8q24genomic region have been associated with colon, breast,and prostate cancer susceptibility and presumed to beimplicated in the regulation of the MYC oncogene locatedon 8q24.21. Chromatin conformation capture (3C) experi-ments [86] allow for the detection of physical interactions(looping interactions) between genes and their regulatoryelements that may be located megabases away from theirtarget genes. Relevant to prostate cancer, Meyer et al. [87]focused on the rs378854 SNP as prioritized by in silicoanalysis and demonstrating prostate cancer–specific activity.3C and allele-specific experiments nominated PVT1 as theoncogene involved in the rs378854 contribution to prostatecancer risk. Although still uncommon owing to the technicalchallenges of the technique and the requisite of an a priorihypothesis, 3C-like experiments hold promise for decipher-ing the role of intergenic cancer–associated risk variants.
Perspectives and future directions
To date, a large number of studies with different designshave investigated genetic variants as risk markers for prostatecancer, providing a solid backbone for functional
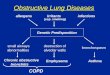
hypothesis driven (gene or mechanism based)
family-based (linkage or association)
genome-wide association study (GWAS)
short repeats (e.g. CAG in the AR gene)
SNPs, SNVs
inherited CNVs
prostate cancer
aggressive/lethal prostate cancer
molecular events (e.g. ETS rearrangment)
array (aCGH, SNPs)
Next Generation Sequencing (WES/WGS) qPCR
Genetic Variants
Study Design
Endpoint/Phenotype
Technology/Platform
Fig. Key components in cancer risk studies. (Color version of figure isavailable online.)
investigations aimed at understanding the etiology of thedisease. Most prostate cancer–risk studies were not designed(Fig.) to adequately evaluate aggressive (e.g., Gleason sum 8–10) or lethal prostate cancer, but rather to query susceptibilityto the disease overall, which is weighted toward the inclusionof cases with more indolent disease. Given the mountingevidence of the molecular heterogeneity of prostate cancer ashighlighted in multiple publications (reviewed by Barbieriet al. [88]), risk studies designed to identify germ-line variantsassociated with molecularly distinct subclasses of prostatecancer (i.e., TMPRSS2-ERG fusion positive prostate cancer orSPOP mutant prostate cancer) are also warranted; under thehypothesis that prostate cancer is a collection of distinctsubtypes for which molecular-specific end point risk studiesmight lead to more informative results.
Population diversity has not been significantly addressedin most prostate cancer germ-line studies. Without consid-ering ethnic variability, it will be difficult to identifyuniversal risk factors and to apply findings in diversepopulations. Future studies need to address individualethnicity information, preferentially inferred from popula-tion informative SNPs [89] rather than from questionnairesand self-declarations to allow for optimal populationstratification on a genome-wide scale. Any significant riskmarker needs to be verified in multiple cohorts representingdifferent at-risk populations and ethnic backgrounds toascertain validity and potential clinical utility.
The greatest utility for prostate cancer germ-line bio-markers may be in the setting of targeted screening assuggested by the IMPACT study preliminary results [79]and at the time of treatment decision. Aggressive or lethalprostate cancer–associated germ-line variants may improvethe ability to predict which patients are at a higher risk ofdisease progression when ascertained at the time ofdiagnosis and help stratify patients eligible for aggressivetreatment vs. active surveillance protocols. Based on multi-ple independent studies [15,25,26,90], we expect that futurerisk models useful in the clinical setting will incorporateseveral risk loci (i.e., panels of genetic markers) rather thansingle variants and may be dependent on an individualpatient's ethnic background.
One can foresee progression risk models that willcombine germ-line variants, somatic lesions detectable indiagnostic tissue biopsies or surgical samples, and clinico-pathological features (e.g., Gleason score) as part of aPrecision Medicine approach. Large prospective studies arenecessary to formally compare the performance of com-bined risk models with models currently utilized in theclinical setting to predict risk of prostate cancer progression.
References
[1] GLOBOCAN 2008 (IARC) Section of Cancer Information.[2] Howlader NNA, Krapcho M, Garshell J, Neyman N, Altekruse SF,
Kosary CL, et al. SEER cancer statistics review, 1975-2010.Bethesda, MD: National Cancer Institute, 2013.

F. Demichelis, J.L. Stanford / Urologic Oncology: Seminars and Original Investigations ] (2014) 1–108
[3] Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CACancer J Clin 2012;62:10–29.
[4] Boorjian SA, Eastham JA, Graefen M, Guillenneau B, Karnes RJ,Moul JW, et al. A critical analysis of the long-term impact of radicalprostatectomy on cancer control and function outcomes. Eur Urol2012;61:664–75.
[5] Thompson I, Thrasher JB, Canby-Hagino ED, Cookson MS,D0Amico AV, Dmochowski RR, et al. Guideline for the managementof clinically localized prostate cancer: 2007 update. J Urol2007;177:2106-31 [PMID: 17509297].
[6] Morganti G, Gianferrari L, Cresseri A, Arrigoni G, Lovati G. Clinico-statistical and genetic research on neoplasms of the prostate. ActaGenet Stat Med 1956;6:304–5.
[7] Carter BS, Beaty TH, Steinberg GD, Childs B, Walsh PC. Mendelianinheritance of familial prostate cancer. Proc Natl Acad Sci U S A1992;89:3367–71.
[8] Ostrander EA, Stanford JL. Genetics of prostate cancer: too manyloci, too few genes. Am J Hum Genet 2000;67:1367–75.
[9] Langeberg WJ, Isaacs WB, Stanford JL. Genetic etiology ofhereditary prostate cancer. Front Biosci 2007;12:4101–10.
[10] Qaseem A, Barry MJ, Denberg TD, Owens DK, Shekelle P. Screen-ing for prostate cancer: a guidance statement from the clinicalguidelines committee of the American College of Physicians. AnnIntern Med 2013;158:761–70.
[11] Hjelmborg JB, Scheike TH, Holst KK, Skytthe A, Penney KL, Graff RE,et al. The heritability of prostate cancer in the Nordic twin study ofcancer. Cancer Epidemiol Biomarkers Prev [in press] Published OnlineFirst May 8, 2014; Available at: http://dx.doi.org/:10.1158/1055-9965.EPI-13-0568.
[12] Lichtenstein P, Holm NV, Verkasalo PK, Iliadou A, Kaprio J,Koskenvuo M, et al. Environmental and heritable factors in thecausation of cancer—analyses of cohorts of twins from Sweden,Denmark, and Finland. N Engl J Med 2000;343:78–85.
[13] Varghese JS, Easton DF. Genome-wide association studies incommon cancers—what have we learnt? Curr Opin Genet Dev2010;20:201–9.
[14] Goh CL, Schumacher FR, Easton D, Muir K, Henderson B,Kote-Jarai Z, et al. Genetic variants associated with predispositionto prostate cancer and potential clinical implications. J Int Med2012;271:353–65.
[15] Eeles RA, Al Olama AA, Benlloch S, Saunders EJ, LeongamornlertDA, Tymrakiewicz M, et al. Identification of 23 new prostate cancersusceptibility loci using the iCOGS custom genotyping array. NatGenet 2013;45:91e1–2.
[16] Al Olama AA, Kote-Jarai Z, Schumacher FR, Wiklund F, Berndt SI,Benlloch S, et al. A meta-analysis of genome-wide association studiesto identify prostate cancer susceptibility loci associated with aggres-sive and non-aggressive disease. Human Mol Genet 2013;22:408–15.
[17] Haiman CA, Chen GK, Blot WJ, Strom SS, Berndt SI, Kittles RA,et al. Genome-wide association study of prostate cancer in men ofAfrican ancestry identifies a susceptibility locus at 17q21. Nat Genet2011;43:570–3.
[18] Takata R, Akamatsu S, Kubo M, Takahashi A, Hosono N, Kawaguchi T,et al. Genome-wide association study identifies five new susceptibility locifor prostate cancer in the Japanese population. Nat Genet 2010;42:751–4.
[19] Akusuke A, Takata R, Haiman CA, Takahashi A, Inoue T, Kubo M,et al. Common variants at 11q12, 10q26 and 3p11.2 are associatedwith prostate cancer susceptibility in Japanese. Nat Genet 2012;44:426–9.
[20] Xu J, Mo Z, Ye D, Wang M, Liu F, Jin G, et al. Genome-wideassociation study in Chinese men identifies two new prostate cancerrisk loci at 9q31.2 and 19q13.4. Nat Genet 2012;44:1231–5.
[21] Duggan D, Zheng SL, Knowlton M, Benitez D, Dimitrov L, Wiklund F,et al. Two genome-wide association studies of aggressive prostatecancer implicate putative prostate tumor suppressor gene DAB2IP.J Natl Cancer Inst 2007;99:1836–44.
[22] Fitzgerald LM, Kwon EM, Conomos MP, Kolb S, Holt S, Levine D,et al. Genome-wide association study identifies a genetic variantassociated with risk for more aggressive prostate cancer. CancerEpidemiol Biomarkers Prev 2011;20:1196–203.
[23] Penney KL, Pyne S, Schumacher FR, Sinnott JA, Mucci LA, KraftPL, et al. Genome-wide association study of prostate cancer mortality.Cancer Epidemiol Biomarkers Prev 2010;19:2869–76.
[24] Lin DW, FitzGerald LM, Fu R, Kwon EM, Zheng SL, Kolb S, et al.Genetic variants in the LEPR, CRY1, RNASEL, IL4, and ARVCFgenes are prognostic markers of prostate cancer-specific mortality.Cancer Epidemiol Biomarkers Prev 2011;20:1928–36.
[25] Lindstrom S, Schumacher FR, Cox D, Travis RC, Albanes D, AllenNE, et al. Common genetic variants in prostate cancer risk prediction—results from the NCI Breast and Prostate Cancer Cohort Consortium(BPC3). Cancer Epidemiol Biomarkers Prev 2012;21:437–44.
[26] Agalliu I, Wang Z, Wang T, Dunn A, Parikh H, Myers T, et al.Characterization of SNPs associated with prostate cancer in men ofAshkenazic descent from the set of GWAS identified SNPs: impact ofcancer family history and cumulative SNP risk prediction. PLoS One2013;8:e60083.
[27] Craig-Holmes AP, Moore FB, Shaw MW. Polymorphism of humanC-band heterochromatin. I. Frequency of variants. Am J Hum Genet1973;25:181–92.
[28] Sebat J, Lakshmi B, Troge J, Alexander J, Young J, Lundin P, et al.Large-scale copy number polymorphism in the human genome.Science 2004;305:525–8.
[29] Iafrate AJ, Feuk L, Rivera MN, Listewnik ML, Donahoe PK, Qi Y,et al. Detection of large-scale variation in the human genome. NatGenet 2004;36:949–51.
[30] Freeman JL, Perry GH, Feuk L, Redon R, McCarroll SA, Altshuler DM,et al. Copy number variation: new insights in genome diversity. GenomeRes 2006;16:949–61.
[31] Feuk L, Marshall CR, Wintle RF, Scherer SW. Structural variants:changing the landscape of chromosomes and design of diseasestudies. Hum Mol Genet 2006;15 Spec No 1:R57–66.
[32] Abecasis GR, Auton A, Brooks LD, DePristo MA, Durbin RM,Handsaker RE, et al. An integrated map of genetic variation from1,092 human genomes. Nature 2012;491:56–65.
[33] Banerjee S, Oldridge D, Poptsova M, Hussain WM, Chakravarty D,Demichelis F. A computational framework discovers new copy numbervariants with functional importance. PLoS One 2011;6:e17539.
[34] Schlattl A, Anders S, Waszak SM, Huber W, Korbel JO. RelatingCNVs to transcriptome data at fine resolution: assessment of the effectof variant size, type, and overlap with functional regions. GenomeRes 2011;21:2004–13.
[35] Ledbetter DH, Riccardi VM, Airhart SD, Strobel RJ, Keenan BS,Crawford JD. Deletions of chromosome 15 as a cause of the Prader-Willi syndrome. N Engl J Med 1981;304:325–9.
[36] Nelis E, Van Broeckhoven C, De Jonghe P, Lofgren A, Vanden-berghe A, Latour P, et al. Estimation of the mutation frequencies inCharcot-Marie-Tooth disease type 1 and hereditary neuropathy withliability to pressure palsies: a European collaborative study. Eur JHum Genet 1996;4:25–33.
[37] Wise CA, Garcia CA, Davis SN, Heju Z, Pentao L, Patel PI, et al.Molecular analyses of unrelated Charcot-Marie-Tooth (CMT) diseasepatients suggest a high frequency of the CMTIA duplication. Am JHum Genet 1993;53:853–63.
[38] Stankiewicz P, Lupski JR. Structural variation in the human genomeand its role in disease. Annu Rev Med 2010;61:437–55.
[39] Zhang F, Gu W, Hurles ME, Lupski JR. Copy number variation inhuman health, disease, and evolution. Annu Rev Genomics HumGenet 2009;10:451–81.
[40] Kathiresan S, Voight BF, Purcell S, Musunuru K, Ardissino D,Mannucci PM, et al. Genome-wide association of early-onsetmyocardial infarction with single nucleotide polymorphisms andcopy number variants. Nat Genet 2009;41:334–41.

F. Demichelis, J.L. Stanford / Urologic Oncology: Seminars and Original Investigations ] (2014) 1–10 9
[41] McCarroll SA, Bradner JE, Turpeinen H, Volin L, Martin PJ,Chilewski SD, et al. Donor-recipient mismatch for common genedeletion polymorphisms in graft-versus-host disease. Nat Genet2009;41:1341–4.
[42] Frank B, Bermejo JL, Hemminki K, Sutter C, Wappenschmidt B,Meindl A, et al. Copy number variant in the candidate tumorsuppressor gene MTUS1 and familial breast cancer risk. Carcino-genesis 2007;28:1442–5.
[43] Shlien A, Tabori U, Marshall CR, Pienkowska M, Feuk L, NovokmetA, et al. Excessive genomic DNA copy number variation in the Li-Fraumeni cancer predisposition syndrome. Proc Natl Acad Sci U S A2008;105:11264–9.
[44] Diskin SJ, Hou C, Glessner JT, Attiyeh EF, Laudenslager M, BosseK, et al. Copy number variation at 1q21.1 associated with neuro-blastoma. Nature 2009;459:987–91.
[45] Fernandez-Rozadilla C, Cazier JB, Tomlinson I, Brea-Fernandez A,Lamas MJ, Baiget M, et al. A genome-wide association study oncopy-number variation identifies a 11q11 loss as a candidatesusceptibility variant for colorectal cancer. Hum Genet 2014;133:525–34.
[46] Cybulski C, Wokolorczyk D, Huzarski T, Byrski T, Gronwald J,Gorski B, et al. A large germline deletion in the Chek2 kinase gene isassociated with an increased risk of prostate cancer. J Med Genet2006;43:863–6.
[47] Setlur SR, Chen CX, Hossain RR, Ha JS, Van Doren VE, Stenzel B,et al. Genetic variation of genes involved in dihydrotestosteronemetabolism and the risk of prostate cancer. Cancer EpidemiolBiomarkers Prev 2010;19:229–39.
[48] Gallagher CJ, Kadlubar FF, Muscat JE, Ambrosone CB, Lang NP,Lazarus P. The UGT2B17 gene deletion polymorphism and risk ofprostate cancer. A case-control study in Caucasians. Cancer DetectPrev 2007;31:310–5.
[49] Karypidis AH, Olsson M, Andersson SO, Rane A, Ekstrom L.Deletion polymorphism of the UGT2B17 gene is associated withincreased risk for prostate cancer and correlated to gene expression inthe prostate. Pharmacogenomics J 2008;8:147–51.
[50] Olsson M, Lindstrom S, Haggkvist B, Adami HO, Balter K, Stattin P,et al. The UGT2B17 gene deletion is not associated with prostatecancer risk. Prostate 2008;68:571–5.
[51] Park J, Chen L, Ratnashinge L, Sellers TA, Tanner JP, Lee JH, et al.Deletion polymorphism of UDP-glucuronosyltransferase 2B17 andrisk of prostate cancer in African American and Caucasian men.Cancer Epidemiol Biomarkers Prev 2006;15:1473–8.
[52] Bartsch G, Horninger W, Klocker H, Pelzer A, Bektic J, Oberaigner W,et al. Tyrol prostate cancer demonstration project: early detection,treatment, outcome, incidence and mortality. BJU Int 2008;101:809–816.
[53] Oberaigner W, Horninger W, Klocker H, Schonitzer D, Stuhlinger W,Bartsch G. Reduction of prostate cancer mortality in Tyrol, Austria,after introduction of prostate-specific antigen testing. Am J Epidemiol2006;164:376–84.
[54] Demichelis F, Setlur SR, Banerjee S, Chakravarty D, Chen JY, ChenCX, et al. Identification of functionally active, low frequency copynumber variants at 15q21.3 and 12q21.31 associated with prostatecancer risk. Proc Natl Acad Sci U S A 2012;109:6686–91.
[55] Smith JR, Freije D, Carpten JD, Gron̈berg H, Xu J, Isaacs SD, et al.Major susceptibility locus for prostate cancer on chromosome 1suggested by a genome-wide search. Science 1996;274:1371–4.
[56] Carpten J, Nupponen N, Isaacs S, Sood R, Robbins C, Xu J, et al.Germline mutations in the ribonuclease L gene in families showinglinkage with HPC1. Nat Genet 2002;30:181–4.
[57] Johanneson B, McDonnell SK, Karyadi DM, Quignon P, McIntosh L,Riska SM, et al. Family-based association analysis of 42 hereditaryprostate cancer families identifies the Apolipoprotein L3 regionon chromosome 22q12 as a risk locus. Hum Mol Genet 2010;19:3852–62.
[58] Ewing CM, Ray AM, Lange EM, Zuhlke KA, Robbins CM, TembeWD, et al. Germline mutations in HOXB13 and prostate-cancer risk.N Engl J Med 2012;366:141–9.
[59] Sboner A, Demichelis F, Calza S, Pawitan Y, Setlur SR, Hoshida Y,et al. Molecular sampling of prostate cancer: a dilemma for predictingdisease progression. BMC Med Genomics 2010;3:8.
[60] Xu J, Lange EM, Lu L, Zheng SL, Wang Z, Thibodeau SN, et al.HOXB13 is a susceptibility gene for prostate cancer: results from theInternational Consortium for Prostate Cancer Genetics (ICPCG). HumGenet 2013;132:5–14.
[61] Shang Z, Zhu S, Zhang H, Li L, Niu Y. Germline homeobox B13(HOXB13) G84E mutation and prostate cancer risk in Europeandescendants: a meta-analysis of 24,213 cases and 73, 631 controls.Eur Urol 2013;64:173–6.
[62] Karlsson R, Aly M, Clements M, Zheng L, Adolfsson J, Xu J, et al. Apopulation-based assessment of germline HOXB13 G84E mutationand prostate cancer risk. Eur Urol 2014;65:169–76.
[63] Stott-Miller M, Karyadi DM, King T, Kwon EM, Kolb S, StanfordJL, et al. HOXB13 mutations in a population-based, case control studyof prostate cancer. Prostate 2013;73:634–41.
[64] Schroeck FR, Zuhlke KA, Siddiqui J, Siddiqui R, Cooney KA, WeiJT. Testing for the recurrent HOXB13 G84E germline mutation inmen with clinical indications for prostate biopsy. J Urol 2013;189:849–53.
[65] FitzGerald LM, Kumar A, Boyle EA, Zhang Y, McIntosh LM, KolbS, et al. Whole-exome sequencing and genotyping in 289 hereditaryprostate cancer families and a case-control study implicate mis-sense mutations in BTNL2. Cancer Epidemiol Biomark Prev2013;22:1520–8.
[66] Xu J, Zheng SL, Komiya A, Mychaleckyj JC, Isaacs SD, Hu JJ, et al.Germline mutations and sequence variants of the macrophagescavenger receptor 1 gene are associated with prostate cancer risk.Nat Genet 2002;32:321–5.
[67] Tavtigian SV, Simard J, Teng DH, Abtin V, Baumgard M, Beck A,et al. A candidate prostate cancer susceptibility gene at chromosome17p. Nat Genet 2001;27:172–80.
[68] Leongamornlert D, Mahmud N, Tymrakiewicz M, Saunders E,Dadaev T, Castro E, et al. Germline BRCA1 mutations increaseprostate cancer risk. Br J Cancer 2012;106:1697–701.
[69] The Breast Cancer Linkage C: Cancer risks in BRCA2 mutationcarriers. J Natl Cancer Inst 1999;91:1310–6.
[70] Edwards SM, Kote-Jarai Z, Meitz J, Hamoudi R, Hope Q, Osin P, et al.Two percent of men with early-onset prostate cancer harbor germlinemutations in the BRCA2 gene. Am J Hum Genet 2003;72:1–12.
[71] Agalliu I, Karlins E, Kwon EM, Iwasaki LM, Diamond A, OstranderEA, et al. Rare germline mutations in the BRCA2 gene are associatedwith early-onset prostate cancer. Br J Cancer 2007;97:826–31.
[72] Agalliu I, Kwon EM, Zadory D, McIntosh L, Thompson J, StanfordJL, et al. Germline mutations in the BRCA2 gene and susceptibility tohereditary prostate cancer. Clin Cancer Res 2007;13:839–43.
[73] Wilkens EP, Freije D, Xu J, Nusskern DR, Suzuki H, Isaacs SD, et al.No evidence for a role of BRCA1 or BRCA2 mutations in AshkenaziJewish families with hereditary prostate cancer. Prostate 1999;39:280–4.
[74] Sinclair CS, Berry R, Schaid D, Thibodeau SN, Couch FJ. BRCA1and BRCA2 have a limited role in familial prostate cancer. CancerRes 2000;60:1371–5.
[75] Gayther SA, de Foy KA, Harrington P, Pharoah P, Dunsmuir WD,Edwards SM, et al. The frequency of germ-line mutations in thebreast cancer predisposition genes BRCA1 and BRCA2 in familialprostate cancer. Cancer Res 2000;60:4513–8.
[76] Agalliu I, Gern R, Leanza S, Burk RD. Associations of high-gradeprostate cancer with BRCA1 and BRCA2 founder mutations. ClinCancer Res 2009;15:1112–20.
[77] Kote-Jarai Z, Leongamornlert D, Saunders E, Tymrakiewicz M,Castro E, Mahmud N, et al. BRCA2 is a moderate penetrance gene

F. Demichelis, J.L. Stanford / Urologic Oncology: Seminars and Original Investigations ] (2014) 1–1010
contributing to young-onset prostate cancer: implications for genetictesting in prostate cancer patients. Br J Cancer 2011;105:1230–4.
[78] Castro E, Goh C, Olmos D, Saunders E, Leongamornlert D,Tymrakiewicz M, et al. Germline BRCA mutations are associatedwith higher risk of nodal involvement, distant metastasis, and poorsurvival outcomes in prostate cancer. J Clin Oncol 2013;31:1748–57.
[79] Bancroft EK, Page EC, Castro E, Lilja H, Vickers A, Sjoberg D, et al.Targeted prostate cancer screening in BRCA1 and BRCA2 mutationcarriers: results from the initial screening round of the IMPACTstudy. Eur Urol 2014:Jan 15 [pii: S0302-2838(14)00004-9], Availableat: http://dx.doi.org/10.1016/j.eururo.2014.01.003.
[80] Bernstein BE, Birney E, Dunham I, Green ED, Gunter C, Snyder M.An integrated encyclopedia of DNA elements in the human genome.Nature 2012;489:57–74.
[81] Nicolae DL, Gamazon E, Zhang W, Duan S, Dolan ME, Cox NJ.Trait-associated SNPs are more likely to be eQTLs: annotation toenhance discovery from GWAS. PLoS Genet 2010;6:e1000888.
[82] Grisanzio C, Werner L, Takeda D, Awoyemi BC, Pomerantz MM,Yamada H, et al. Genetic and functional analyses implicate theNUDT11, HNF1B, and SLC22A3 genes in prostate cancer patho-genesis. Proc Natl Acad Sci U S A 2012;109:11252–7.
[83] Xu X, Hussain WM, Vijai J, Offit K, Rubin MA, Demichelis F, et al.Variants at IRX4 as prostate cancer expression quantitative trait loci.Eur J Hum Genet 2014;22(4):558–63.
[84] Nguyen HH, Takata R, Akamatsu S, Shigemizu D, Tsunoda T,Furihata M, et al. IRX4 at 5p15 suppresses prostate cancer growththrough the interaction with vitamin D receptor, conferring prostatecancer susceptibility. Hum Mol Genet 2012;21:2076–85.
[85] Pomerantz MM, Shrestha Y, Flavin RJ, Regan MM, Penney KL,Mucci LA, et al. Analysis of the 10q11 cancer risk locus implicatesMSMB and NCOA4 in human prostate tumorigenesis. PLoS Genet2010;6:e1001204.
[86] Dekker J. The three ‘C’ s of chromosome conformation capture:controls, controls, controls. Nat Methods 2006;3:17–21.
[87] Meyer KB, Maia AT, O0Reilly M, Ghoussaini M, Prathalingam R,Porter-Gill P, et al. A functional variant at a prostate cancerpredisposition locus at 8q24 is associated with PVT1 expression.PLoS Genet 2011;7:e1002165.
[88] Barbieri CE, Bangma CH, Bjartell A, Catto JW, Culig Z, Gronberg H, et al.The mutational landscape of prostate cancer. Eur Urol 2013;64:567–76.
[89] Price AL, Patterson NJ, Plenge RM, Weinblatt ME, Shadick NA,Reich D. Principal components analysis corrects for stratification ingenome-wide association studies. Nat Genet 2006;38:904–9.
[90] Cybulski C, Wokolorczyk D, Kluzniak W, Kashyap A, Golab A,Slojewski M, et al. A personalised approach to prostate cancerscreening based on genotyping of risk founder alleles. Br J Cancer2013;108:2601–9.