Embed Size (px)
Citation preview

Genetic Predisposition to Breast Cancer
HENRY T. LYNCH, MD,’ WILLIAM A. ALBANO, MD,t B. SHANNON DANES, MD, PHD,$ MICHAEL A. LAYTON, BA,’ WILLIAM J. KIMBERLING, P H D , ~ JANE F. LYNCH, BSN,’
S. C. CHENG, PHD.11 KAREN A. COSTELLO. BSN,* GABRIEL M. MULCAHY, MD,T CINDY A. WAGNER, MSW,’ AND SYLVIA L. TINDALL, BSN’
Breast cancer risk factors are closely intertwined with the patient’s cultural background, which may contribute to breast cancer aggregations within families. The difficult questions are: (1) does a truly hereditary breast cancer subset exist; (2) which familial aggregations are hereditary; and (3) is the hereditary form distinctive from its sporadic counterpart? These queries will be resolved once biomarkers are identified that show high sensitivity and specificity with genotype. The authors provide a review of this subject and will focus on their recent discovery of increased in vitro hyperdiploidy in cultured skin fibroblasts from patients with or at risk for hereditary breast cancer. The authors discuss findings from their study of family histories in 225 consecutively ascertained patients with verified breast cancer from the Creighton University School of Medicine Oncology Clinic. Findings consistent with an hereditary breast cancer syndrome were identified in 5% of the patients. Given the 112,000 new cases of breast cancer in the United States in 1982, the authors estimate that with a confidence coefficient of 0.95 between 2410 and 8790 of these individuals will manifest hereditary breast cancer. Specific surveillance/ management programs should be geared to high-risk members of these families in which cancer yield will be predictable.
Cancer 53:612-622, 1984.
AMILIAL CLUSTERING of breast cancer was first re- F corded in the Roman medical literature around 100 AD.’ However, in spite of this long historic precedent, we remain perplexed as to its public health magnitude
Presented at the American Cancer Society National Conference: Breast Cancer, Boston, Massachusetts, May 19-21, 1983.
From the Creighton University School of Medicine and the Institute for Familial Cancer Management and Control, Inc., Omaha, Nebraska. Cornell University Medical College, New York, New York, University of Medicine & Dentistry of New Jersey, New Jersey Medical School, Newark, New Jersey, Department of Otolaryngology, Boys Town In- stitute, Omaha, Nebraska.
Supported by the Council for Tobacco Research, grant # 1297-AR 1. * Department of Preventive Medicine/Public Health, Creighton Uni-
t Department of Surgery, Division of Oncology. Creighton University. 4 Department of Medicine, Section of Cell Biology, Cornell University
(i Department of Otolaryngology, Boys Town Institute, Omaha, Ne-
)I Department of Mathematics, Creighton University. ll Department of Pathology, University of Medicine & Dentistry of
New Jersey, New Jersey Medical School. Address for reprints: Henry T. Lynch, MD, Department of Preventive
Medicine, Creighton University School of Medicine, California @ 24th Street, Omaha, NE 681 78.
William Alexander Albano, MD, a surgical oncologist and coauthor of this article, was steadfastly dedicated to the development of surveil- lance/management protocols for patients with hereditary breast cancer. He died on July 7, 1983, at the age of 37. We wish to dedicate this article to the memory of our dear friend and colleague.
versity School of Medicine.
Medical College.
braska.
Accepted for publication August 31, 1983.
and significance. A major concern pertains to the extent that chance alone may explain breast cancer clustering in families. Obfuscating elucidation of familial clustering is the fact that breast cancer is extremely common, par- ticularly among hi&er socioeconomic-educational groups where the effect of social class gradient becomes most pronounced at postmenopausal age^.^.^ This in turn may influence other risk factors such as early age at menarche,’ and increased height and weight. ’.* Collectively, these are closely intertwined with the patient’s cultural background. Thereby, they clearly are more apt to be “familial.”’ Given these facts, it is not. surprising that such familial clustering of breast cancer are frequently encountered. What is needed is more knowledge of the magnitude of the prob- lem, and an easy and efficient screening strategy to identify which familial clusters of breast cancer involve primary genetic factors, thereby inordinately predisposing family members to this disease.
Anderson’ has shown that when a woman’s mother or sister is affected, her breast cancer risk is increased. However, when early onset and/or bilaterality is present, the risk becomes even more significant and may be con- sonant with hereditary breast cancer. However, these es- timates fail to consider cancer of other anatomic sites and the relationship to relatives within the context of hereditary breast cancer syndromes. As will be shown,
612

No. 3 BREAST CANCER GENETICS Lynch et a/. 613
approximately 5% of all breast cancer-affected patients show clinical and pedigree findings which fulfill our op- erational criteria as being consistent with hereditary (au- tosomal dominant) breast cancer syndromes.
Our purpose is fourfold: ( 1 ) to document the observed frequency of “hereditary” breast cancer in a consecutive series of patients treated at the Creighton Cancer Center; (2) to discuss biomarkers in hereditary breast cancer with major attention given to the significance of our obser- vation of increased in vitro hyperdiploidy in hereditary breast cancer; (3) to describe distinctive features of he- reditary breast cancer; and (4) to discuss surveillance/ management strategy in concert with public health im- plications for hereditary breast cancer.
Methods
A modified nuclear family history (FH) is routinely compiled on all patients seen at the Creighton Cancer Center.7 This FH protocol focuses on the proband’s sib- lings, parents (first-degree relatives), and both maternal and paternal aunts, uncles, and grandparents (informative second-degree relatives). The proband’s siblings and chil- dren, while at risk, are generally uninformative because of their relatively young age. Hereditary breast cancer may show paternal as well as maternal transmission. Thus, the need to acquire information about these informative relatives on both sides of the family.
A detailed explanation of the goals and objectives of the study is provided the patient. She is advised that she may freely decline further involvement in the study at any time. Signed permission for participation in the study and for release of medical documents is then requested.
Those patients referred for purposes of genetic eval- uation are excluded from the consecutive series in order to avoid ascertainment bias.
Family histories were collected from 225 consecutively ascertained patients with verified breast cancer. Primary medical and pathology documents were secured whenever possible so that cancer (all anatomic sites) could be ver- ified. Pedigrees were then constructed and reviewed with the patients. This enabled them to recall specific genelogic relationships with greater accuracy and detail; in some cases, to clarify cancer occurrences within their family.
Research interests of our group during the past 2 de- cades have led to continuous refinement of our cancer genetic protocols as well as to the establishment of rapport with countless medical records departments, pathology laboratories, and practicing physicians. This has enabled our family studies to be performed expeditiously with maximum efficiency and an excellent yield of vital medical information. Recognition of cancer-prone families of many varieties has provided powerful models for the study of biomarkem8
Dejnition of Terms
We operationally define familial breast cancer as the occurrence of two or more breast cancer-affected relatives within the modified nuclear pedigree inclusive of the pro- band. Breast cancer not fulfilling our familial cntena is classified sporadic. This determination is efficiently ac- complished in a primary care setting. Within the familial aggregation lies the subset of putative hereditary breast cancer. It is difficult to operationally define hereditary breast cancer in the absence of specific physical signs and/ or biomarkers which correlate significantly with genotype. Unfortunately, today genotype can only be inferred by the expression of phenotype (cancer). However, the oc- currence of an alleged syndrome cancer within a familial clustering may not always be associated with genetic etiology. It is important that this serious limitation be acknowledged when assessing the concept of hereditary breast cancer. The pedigrees must be extended and doc- umented to confirm putative hereditary cancer syn- dromes.
The hereditary form includes those familial clusterings which on a modified nuclear pedigree demonstrate one or more of the hereditary breast cancer cardinal features:’ (1) young age of onset’; (2) bilaterality”; (3) vertical transmission’,*; or (4) specific tumor associations con- sonant with genetic heterogeneity.’ ’ The expertise of a cancer geneticist, to interpret an extended pedigree, will be advantageous for hereditary syndrome identification.
Limited family size, problems in pathology verification, early death of key relatives prior to phenotype (cancer) expression, lack of compliance, absence of markers of cancer-prone genotype, and countless other presently un- controllable factors materially limit one’s ability to make these judgments with greater precision. These consider- ations must be carefully weighed when invoking criteria for classification of pedigrees.
We define in vitro tetraploidy as a numerical chro- mosome complement of 92 and/or 92 minus a few chro- mosomes. Tetraploidy is considered by us to be a normal event.
We define in vitro hyperdiploidy as the chromosome number per metaphase over 46, exclusive of 92 or 92 minus a few chromosomes. We are not comparing te- traploidy with hyperdiploidy in this article. Rather, this article is based on our findings of hyperdiploidy exclusive of tetraploidy.
In Vitro Hyperdiploidy
The detection of in vitro cancer-prone gene expressions requires study of three components: the experimental model based on extended pedigrees of hereditary breast cancer kindreds, including affected and high-risk relatives;

614 CANCER February 1 Supplement 1984 Vol. 53
Biopsy cut - E x p l a n t s just c o v e r e d by medium 2 x 6 m m 4 into 4 p o r t s - (pH 7 4 ) d u r i n g f i r s t c u l t u r e week
Skin biopsy
s p l i t th ickness
4-6 c u l t u r e w e e k in o n h u m i d i f i e d a t m o s p h e r e of 5 % COe in a i r .
t TI
Cells d i s p e r s e d wi th E p i t h e l i a i d s h e e t a n d Monolayer v e r s e n e - trypsin so lu t ion f i b r o b l a s t i c cells sur rounding
c u l t u r e p r i m a r y e x p l a n t
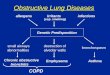
FIG. I . Methodology used for the establishment of monolayer (mixed fibroblastic and epithelioid) cultures from human skin biopsies (From Lynch H, Albano WA, Danes BS PI a/. Precursor conditions and monitoring of high-risk colon cancer patients. In: Stroehlein JR, Romsdahl MM, eds. Gastrointestinal Cancer. New York; Raven Press, I98 I; 297-325).
the test system-dermal monolayer fibroblast cultures established from split-thickness skin biopsies (Fig. 1); and the assay system for the incidence of alterations in chro- mosome complement (percent of different alterations in chromosome complement in metaphase preparations).
Figure 2 shows am example of in vitro hyperdiploidy in a cell at metaphase.
Skin biopsy specimens were obtained from 16 breast cancer patients, 13 family members, and 1 spouse of a breast cancer patient, as well as 20 clinically normals
FIG. 2. Metaphase preparation of cells showing diploid (A) and hyperdiploid (B) chromosome complement from a monolayer skin culture

No. 3 BREAST CANCER GENETICS - Lynch et al. 615
TABLE 1 . Occurrence of In Vitro Hyperdiploidy in Dermal Monolayer Cultures From Individuals With Breast Cancer add Family Members
Firstdegree relative of breast cancer affectedt
Total individuals Clinically affected Clinically affected spouse of Putative genetic risk status studied (breast) (other) Unaffected affected
Occurrence of Hyperdiploidyg + - + - + - + - Hereditary breast cancer 14 6 1 0 0 3 3 I 0 Nonhereditary breast cancer 8 1 3 0 0 1 3 0 0 Possible hereditary breast cancer 8 3 2 I 0 0 2 0 0 Controlst 20 (all negative for hyperdiploidy)
A metaphase scored hyperdiploid if chromosome number was greater than 46, exclusive of 92 (tetraploid).
t Determined by family pedigrees.
4 Normals without a family history of solid tumors. g 76-1 18 chromowmes/metaphase Present = +, Absent = -, exclusive
of tetraploidy.
without a history of solid tumors (Table I). Dermal monolayer cultures were established from these split- thickness biopsy specimens by standard culture methods (Fig. l ) . '* Cultures were grown in plastic petri dishes in Eagle's minimum essential medium (EMEM) with 15% volume (vol) fetal bovine serum in an atmosphere of 5% C02 in air, pH 7.0-7.4. Cultures were routinely checked for bacterial contamination and mycoplasma, and found to be uncontaminated.
Cells were grown in culture 15 to 25 weeks (5-10 sub- cultures by trypsinization after the primary explant cul- ture) before assays were performed. Prior to the assays, a coded number was assigned to each culture so that its identify would not be known until completion of the assays.
In order to determine the incidence of alterations in numerical chromosome complement, each cell sample was plated at an initial cell concentration of 1 X 104 cells into multiple 28 cm2 plastic petri dishes containing me- dium with 15% (vol) fetal bovine serum. After 48 hours growth, the medium was completely changed. Approxi- mately 24 hours later, when a burst of mitoses was ob- served, chromosome preparations were made and eval- uated for the incidence of alterations in chromosome complement (hyperdiploidy including tetraploidy). Only if more than 100 mitoses were counted per slide was the preparation considered to reflect the mitotic activity of that culture.
Results
Figure 3 is a schematic drawing showing a breakdown of the 225 patients with respect to the percent of those showing familial or sporadic breast cancer within their family pedigrees. One hundred fifty-five patients were 50 years or older, and 70 patients were under the age of 50. Of the total patients evaluated, 18% demonstrated familial aggregation. Their further genetic evaluation enabled as- signment to two subsets: familial aggregation (but lacking fulfillment of our hereditary criteria, 13%), and hereditary
(fulfilling our operational criteria, 5%). A 95% confidence interval for the true proportion of the hereditary breast cancer subset was calculated to be equal to 2.25% to 7.84%
Figure 4 shows those pedigrees that were judged by us to best fit the category of hereditary breast cancer. It is important to notice that these are not extended pedigrees, although extension of the pedigrees (to include third and fourth generations) is in progress but may take as much as a year or more for completion. These pedigrees exhibit multiple breast cancer occurrences with disease trans- mission through paternal (SJ347) or maternal (SJ389) lineages. In some circumstances, cancer occurred in both maternal and paternal lineages. Notice markedly early age at onset (SJ389, SJ255) in some pedigrees and/or bilaterality in others (SJ347, SJ389, SJ255). Differing tu- mor combinations, particularly breast and gastrointestinal cancer (SJ301, SJ267), were also observed. The limited number of our sample, and thereby the relatively small yield of informative pedigrees, necessarily restricted the full phenotypic expression of tumor heterogeneity which we and others have encountered in larger series of breast cancer-prone families.'.' '
Hyperdiploidy in dermal monolayer cultures (Table 1 ) from the 20 controls (clinically normal without a family history of solid tumors) was solely tetraploidy, whose in- cidence was 0% to 6%. Hyperdiploidy (with the exception of tetraploidy) was not observed.
Cultures derived from three of the four clinically af- fecteds, aged 25 to 34 years old (the fourth patient was 58 years old), from families without hereditary breast cancer had a normal occurrence of tetraploidy (0%-6%) and no hyperdiploidy exclusive of tetraploidy. Of the 12 clinically affecteds from the hereditary and possible he- reditary breast cancer families studied, 9 patients, aged 25 to 71 years, showed increased hyperdiploidy with a normal occurrence of tetraploidy, and 3 patients, aged 38 to 64 years, had only a normal occurrence of tetraploidy and no increased hyperdiploidy. Figure 5 shows hyper-

616 CANCER February I Supplement 1984 VOl. 53
BREAST CANCER PATIEUTS
275
100% -. 50% RISK
1 I MODIFIED NUCLEAR PEDIGREE I EMPLOY CARDINAL
I SPORADIC 1 FEATURES OF HEREDITARY I
I BREAST CANCER I \ \ \ \ \
I,
HEREDITARY FAMILV NIEMBERS
10% (111 daprse
..aq.n.ou(l."doq.n.ou,) b) pen* l O c ~ l ~ l m l i ~ n (9.0. I nkaqe
DNA polvmorphism DNA D!OD@> ~ 0 d ~ n q lor $P.CIIIC 1 I.( ~ n r o q ~ n . i l
d c y i o q e n t i ~ c ~ d) mdOrrinOlOqy
1 r------_--------- I SPECIFIC
r---------- 1 I
L ---------- A
I EXTENDED I S U R V E I I U N C E I M A Y A G E M E N T I I ANALYSIS I I I I PEDIGREE GENETIC I PAOTOCOL 5
SYNDROME IDENTIFICATIDN
5 5 * 2 8%
I
: (11.3.000CASESBREA$TCANCER I N U S DURING 198.3) ! I
2 4 l O A N 0 8 7 9 0 PATIENTSIFAMILIES IN 198.3
FAMILIAL AGGREGATION BUT DOES NOT FULFILL HEREDITARY CRITERIA
t - --_-------- -_--- --- i PueLic HEALTH SIGNIFICANCE
I THEREFORE. BETWEEN I
1
FIG. 3. Schematic diagram based on assessment of family histories in 225 consecutive patients with verified breast cancer
diploidy in one of the hereditary breast cancer families while Figure 6 shows its absence in a sporadic breast cancer setting.
Of the eight clinically normal members of hereditary and possible hereditary breast cancer families studied, five, aged 15 to 37 years, showed the same incidence of tetraploidy as in controls and no other hyperdiploidy. The other three, aged 17, 28, and 30 years, respectively, showed increased hyperdiploidy with a normal Occurrence of tetraploidy, as did one daughter, aged 28 years, with intraocular melanoma whose mother has breast cancer. A spouse, aged 43 years, from a hereditary breast cancer family showed increased in v i m hyperdiploidy. The status of his family history is unknown. Three women, aged 3 1, 52, and 60 years, respectively, who were first-degree relatives of breast cancer-affected patients from the spo- radic families, were negative for hyperdiploidy. A fourth woman, aged 29 years, in this category, was positive for h yperdiploidy .
Age of patient at cancer diagnosis or chemotherapy treatment at the time of the biopsy did not influence these incidences. There was a wide distribution in the total number of chromlosomes per cell (76 to 117 per meta- phase; average, 96 k 10 chromosomes per metaphase). No consistent changes were identified in chromosome constitution within such hyperdiploid metaphases.
Discussion
With the exception of autosomal dominantly inherited Cowden's disease,' reliable identifiable physical signs in- dicative of cancer-prone genotypes are lacking in hered- itary breast cancer. Nevertheless, mounting evidence has accrued during the last decade supporting the role of primary genetic factors in its etiology. This has emanated in part from linkage studies where the glutamate-pyruvate transaminase (GPT) locus has been putatively associated with a breast cancer susceptibility gene,I3 from hormonal

No. 3 BREAST CANCER GENETICS - Lynch el al. 617
044 836 847
50
8 2 i 33 25 827
2 9
d76
'854 d55
Y I35 Q-$
d56
/ 0 3 2 J Z 40
Skin a m Bone H B S l 851 855.55
66 d52 d57
SJ372 -1
68
H3 I d36
Y JbV 4TJP o y s g e m i n o u l 4
dl 4
I 848 5 4
1 SJ 267 q I 1 1 1
S t 4 2 S t d 1 9
Lung79 C85
A A d d 837 C45 56 ThyroldZ5 & & 834 f 835
41 41 55 52 64
SJ 214
8 674 d68
42 36 37
SJ-Y82 "r". 834 d20 8 Lung CSU
64 d42 d60s d73
15
~~
LECtND
0 0 b 1 e or female unaffected
Cancer v e r i f i e d by pathology
Be54 Cancer mica and bga when dimPomad d.60 Age l i v i n g or decabmad
CC43 56
0 b l t i p l e pr iur iam v e r i f i d by parhology
@ @ ::;;;;i;z;;fied by death
Cancer reported by fam11y 0 hlarory
Nvlber of proseny
/ Proband
8 Breast
81 Urinary bladder
C Colon
CSU Cbncer S i t e U I h a n
Cx Uterine c e r v i x
En E n d a e t r i u
Pa Pancreas
Pr P m s t a t e
S t S t o u c h
FIG. 4. Pedigrees from the putative hereditary subset (5%) of patients evaluated for breast cancer, as shown in Figure 3.

I
I1
I 1 1
I V
V
0
EB
1
C@4 3 56
m
LEGEND
0 Male or female unaffected
2 Pedigree code v # Cancer v e r i f i e d by pathology
B@54 Cancer s i t e and age when diagnosed d .60 Age l i v i n g or deceased
@ Cancer v e r i f i e d by death
@ h i s t o r y
c e r t i f i c a t e
Cancer reportled by family
Number o f progeny
Proband # H+ Hyperdiploidy present
H- Hyperdiploidy absent
FIG. 5 . Pedigree of a family with hereditary breast cancer demonstrating hyperdiploidy in breasi.-cancer-affected mother (111-3) and her daughter (fV-2). and in the high-risk daughter (IV-6) of a breast-cancer-affected aunt (111-5) of the proband.

BREAST CANCER GENETICS - Lynch et a/. 619 No. 3
I
I1
I11
I V
d s l P r o s t a I e
I H-
I 6o
D O 1 2
C@43 B@54 56 d.60
a / H+ H-
d 60 O v a r y
LEGEND
Male or female unaffected
Pedigree code Cancer v e r i f i e d by pathology
Cancer s i t e and age when diagnosed Age l i v i n g or deceased
Cancer v e r i f i e d by death c e r t i f i c a t e
Cancer reported by family h is tory
Number of progeay
Proband
Hyperdiploidy present
Hyperdiploidy absent
FIG. 6 . Pedigree of a sporadic family showing negative findings for hyperdiploidy in a breast-cancer affected patient ( 1 1 1 - 1 ) and in her unaffected mother (11-3).
studies in which low urinary estrone and estradiol gluc- uronides have correlated with high genetic risk for he- reditary breast ~ a n c e r , ' ~ . ' ~ from a statistical analysis of high-risk females where cumulative lifetime breast cancer risk estimates were consonant with autosomal-dominant inheritance,I6 and from male-male transmission of breast cancer (discussed below). Our observation of increase in vitro hyperdiploidy in hereditary breast cancer affecteds and high-risk relatives is novel, and merits verification in a larger number of well-documented kindreds. This biomarker is of particular interest when one considers that to date, this tissue culture aberration has been ob- served only in certain specific putative cancer-prone genotypes"-'' (Table 2).
Hypothesis
in vitro research on cancer-prone genes has been based on the hypothesis that a cell, such as those derived from a skin biopsy, considered normal by all criteria, when grown in culture would demonstrate such a mutant can-
cer-prone genotype through specific changes in cellular functions. Incidence of such an in vitro cellular abnor- mality in consecutive generations; that is, vertical trans- mission from a clinically affected to his offspring, would be considered evidence of an in vitro expression of a cancer-prone gene. One of these cellular abnormalities, presumably due to in vitro expressions of germinal mu- tations, is an alteration in chromosome complement; namely, hyperdiploidy with a normal occurrence of te- traploidy .
Diploidy with a low (0%-7%) incidence of tetraploidy has been a constant feature in monolayer cultures derived from dermal biopsies from individuals without a family cancer history; the incidence of increased tetraploidy being approximately I .4% in this group," whereas hyperdiploidy (chromosome number over 46 per metaphase excluding tetraploidy) was rarely observed in such cultures irre- spective of genotype.
Two alterations in chromosome complement (increased tetraploidy and hyperdiploidy with a normal occurrence of tetraploidy) in dermal monolayer fibroblast cultures

620 CANCER February 1 Supplement 1984. VOl. 5 3
TABLE 2. In V i m Chromosome Complements in Dermal Monolayer Cultures for Heritable Cancer Syndromes
Alterations in chromosome no. per metaphase Normal chromosome no. per metaphase
Increased in v i m tetraploidy’ Hyperdiploidyt exclusive of tetraploidy Diploidy
Colonic cancer with discrete polyps FAMMM Familial osteomas Cancer family syndrome Hereditary breast Familial polyposis coli Gardner syndrome Hereditary melanoma Juvenile polyposis Malignant rhabdoid tumor Hereditary ovarian cancer Neurofibromatosis Oldheld syndrome Hereditary pancreatic cancer Peutz-Jegher syndrome Site-specific colon cancer (pancreatic family clusters) Turcot syndrome Teratocarcinoma Xeroderma pigmentosum
Established on clinical phenotypes and family pedigree data. * Chromosome number per metaphase 92.
have been considered in vitru expressions of certain can- cer-prone genes. In the autosomal-dominant colon cancer syndromes,20 this hyperdiploidy has been solely tetra- ploidy (92 chromosomes per metaphase) which appears to reflect a critical alteration in the cell cycle.2’
The in vitru data presented in Table 1 substantiated the occurrence of this alteration in heritable breast cancer. Thus, in virru hyperdiploidy with a normal occurrence of tetraploidy was not specific for any one of the cancer genotypes for heritable solid tumors studied, but appeared to be an in v i m expression of a group of cancer genes associated with certain heritable solid tumors.
The frequency of hyperdiploidy in the sample ofwomen affected with hereditary breast cancer is both remarkable and significant when compared with the 20 control sam- ples (Table 1). The fact that four of nine first-degree rel- atives also show hyperdiploidy suggests genetic control and, possibly, an autosomal-dominant mode of trans- mission.
The one affected spouse is puzzling. When the hered- itary sample was compared with the nonhereditary breast cancer cases, no statistically significant difference in the frequency of hyperdiploidy could be found (P = 0.067). However. the sample size is limited, and with a larger sample we may indeed find a difference. The age and sex of the skin donors did not influence the occurrence of metaphases with abnormal chromosome number (hy- perdiploidy).
From the pathogenetic standpoint, as in any clinical laboratory evaluation, one anticipates encountering false- positives and false-negatives. This is particularly prob- lematic in a disease such as breast cancer, where short of a marker of high specificity to genotype, we remain unable to signify with certainty the genetic form versus its sporadic counterpart.
Distincrivt. Features o f Herediturv Breast Cuncer
That hereditary breast cancer is a distinctive disease, when compared with its sporadic counterpart, is now
t Chromosome number greater than 46 exclusive of 92 (tetraploid). FAMMM: familial atypical multiple mole melanoma syndrome.
strongly supported by its different natural history.’.’-’ I
In addition, strong support for its autosomal-dominant genetic etiology has recently been revealed from a statis- tical analysis of 6138 females at 50% putative “genetic” risk from our breast cancer family resource. The cu- mulative lifetime risk for breast cancer in these families was calculated to be 56% f 5.7% standard error (SE), which is consonant with dominant inheritance. Exclusion of sex linkage, and, therefore, support of autosomal dom- inant, is made by aobservation of male-male breast cancer transmission.16 With respect to the latter, one such family was recently called to our attention for consultation. This family contained two brothers with verified adenocarci- noma of the breast. One of the affected brothers had a son and a daughter affected with adenocarcinoma of the breast. The observation of male-to-male transmission of breast cancer is of cogency to breast cancer genetics, and is consonant with our conviction that hereditary breast cancer is inherited as an autosomal dominant.
A priuri, one would anticipate that its pathology might also be distinctive. Given current methods of examination, however, specific morphologic stigmata of hereditary breast cancer have not been identified. In fact, there are several lines of evidence that militate against the possibility that there is a close relationship between hereditary oc- currences of breast cancer and the pathologic patterns that are manifested by this neoplasm: the histopathology of familial breast cancer is quite similar to that of breast cancer of nonfaniilial the pathologic pattern within a single breast cancer is often of a heterogeneous nature24; different histopathologic types have been en- countered among breast cancers occurring within indi- vidual families2’; and bilateral breast cancers are often of different pathologic types.26 Nevertheless, in studies of multiple case families and of series of patients with par- ticular forms of breast cancer, certain morphologic find- ings of interest have been observed, including an excess of medullary breast cancer among familial cases2’; intra- familial concentrations of similar neoplasms, such as the occurrences of lobular carcinoma in sitzt, that have been

No. 3 BREAST CANCER GENETICS - Lynch et al. 62 1
reported recently in each member of a pair of identical twins,28 and an association between tubular carcinoma of breast and a family history of breast cancer.*’ These observations must be tested further, using sufficiently large numbers of familial cases, as well as meticulously matched control individuals who are affected by breast cancers of sporadic occurrence.
Further evidence for a basic difference in the hereditary form of breast cancer has been observed in terms of an apparent paradoxical response to the alleged “protective” effect of early age at first term pregnan~y.~’ We studied 162 hereditary patients from the Creighton Hereditary Breast Cancer Family Resource, and in contrast to the previous observation in the population at large, we found no significant increased frequency of breast cancer with a later age at first pregnancy (t = 1.1, not significant [NS]). In addition, we investigated 72 of these females who eventually developed breast cancer, and in whom data relevant to age at first pregnancy was available. ,4ge at diagnosis was plotted against age at first pregnancy, and analyzed for statistical significance with the t-lest. For comparison, we performed the same analysis on 197 patients with breast cancer from the Creighton-St. Joseph Oncology Clinic. Whereas females consecutively ascer- tained from the Oncology Clinic demonstrated a signif- icant earlier age at diagnosis with an early first pregnancy (t = 2.66, P < 0.05), the hereditary cohort did not illustrate a correlation (t = I .6, NS). This finding is in accord with Woods and associates, who also documented an early age at diagnosis with an early first pregnancy in 34 1 unselected patients with breast cancer.” In addition, they also dem- onstrated that the mean age of breast cancer presentalion was 5.2 years lower in parous as opposed to nulliparous women (P < 0.001). The investigators concluded iihat reproductive history influences not only breast cancer risk, but in addition, the latent interval in a proporlion of breast carcinoma^.^^ Observations in our hereditary cohort, however, illustrate no significant differences in age of breast cancer onset and parity (N = 78, t = 1.17, NS).
At the infrahuman level, using the rat as a model, chemically induced tumors provided an interesting par- allel to the above findings in our consecutive series. Spe- cifically, prior pregnancy rendered rat mammary tissue less susceptible to chemical carcinogene~is.’~ However, when the pregnancy followed exposure to the carcinogen, the interval between exposure and the presentation of tumors was ~ h o r t e n e d . ~ ~ . ~ ~ It would be of interest to ex- amine these parameters in an animal strain endogeneously predisposed to breast cancer.
Comprehension of the etiologic significance of this vexing issue remains obscure. However, it is of interest that Fishman and coworkers14 have shown that patients at 50% risk for breast cancer from our hereditary bneast
cancer resource showed decreased El and E2 glucuronide conjugates in their urine when compared with meticu- lously matched controls from a nonhereditary population. In addition, although increased estrone sulfate conjugates noted in the urine just escaped statistical significance, this finding suggests a possible shift from glucuronide to sulfate conjugation in high-risk females. One might speculate that this shift predisposes to cancer generation in the hereditary population, irrespective of pregnancy status, whereas in the consecutive series, fluctuating levels of estrogens at pregnancy provide the stimulus for tumor growth.
Innovative Programs
Innovative approaches toward the amelioration of he- reditary breast cancer are needed. Ideally, this should involve intensive care education, coupled with encour- agement for high-risk patients to participate in cancer control programs. We wish there was substantial evidence available demonstrating that alteration in lifestyle for those patients at risk for hereditary breast cancer would be advantageous in its control. However, this simply is not the case. Short of lifestyle alteration, specific surveillance/ management programs should be employed among high- risk members of breast cancer-prone families. Our rec- ommendation for such programs have been previously p ~ b l i s h e d . ~ ~ . ~ ~ For example, the 20-year cumulative risk to the contralateral breast is 46% among hereditary breast cancer patients.’” For this reason, intensive surveillance, or in suitable candidates, prophylactic surgery, is man- dated.35.36
All women who are at 50% risk for hereditary breast cancer should be under intensive surveillance programs beginning at age 20 to 25 years. This timely implemen- tation is recommended because of the average 15-year earlier onset which occurs in the hereditary variety of this disease. I.’ Knowledge of the cardinal features of hereditary breast cancer’.*.’-’ I should be employed as part of indi- vidualized and highly targeted surveillance/management program^.^^.^^ In addition, the recent observation of im- proved survival37 in the hereditary variety can be used advantageously in order to assuage the often crippling anxiety and fear associated with this severely emotionally stereotyped disease. This should also provide impetus to the family physician or surgeon who might otherwise be pessimistic about mounting a breast cancer control pro- gram.
Given the high predictability of cancer yield among the hereditary segment of the population, it is imperative that immediate consideration be given to these groups. What is needed for expediting these goals is the devel- opment of training and service centers, integrated with computerized registries, focusing on practical measures

622 CANCER February 1 Supplement 1984. Vol. 53
for hereditary cancer syndrome identification.’.*.’,’’ Such centers would train office nurses in the rudiments of com- piling FH. Practicing physicians could gain first-hand knowledge in logistics and strategy for the identification, surveillance, and management of hereditary breast cancer. In this overall control strategy, the highest possible priority must be given to biomarker investigations, such as in vitru hyperdiploidy.
REFERENCES
1 . Lynch HT. Genetics and Breast Cancer. New York: Van Nostrand Reinhold Company, 198 I .
2. Lynch HT. Cancer Genetics. Springfield: Charles C. Thomas Co. 1976.
3. Cuello C. Correa P. Haenszel W. Socioeconomic class differences in cancer incidence in Cali, Colombia. In! J Cuncrr 1982; 29:637-643.
4. Graham S, Marshall J. Mettlin C. Rzepka T. Nemoto T, Byers T. Diet in the epidemiology of breast cancer. Am J Lpidemiol 1982: I 16:68- 75.
5 . MacMahon B, Trichopoulos D. Brown J et a/. Age at menarche, probability of ovulation, and breast cancer risk. In! J Cancer 1982:
6. Anderson DE. A genetic study of human breast cancer. J Nut1 Cancer Inst 1972: 48:1029-1034.
7. Lynch HT, Follett KL. Lynch PM e! ul. Family history in an oncology clinic: Implications concerning cancer genetics. JAMA 1979: 242: 1268- 1272.
8. Lynch HT, Albano WA, Danes BS e! a/. Precursor conditions and monitoring of high-risk colon cancer patients. In: Stroehlein, JR, Roms- dahl MM. ed. Gastrointestinal Cancer. New York: Raven Press, 1981; 297-325.
9. Lynch HT. Guirgis H, Brodkey F et ul. Early age of onset in familial breast cancer. Arch Surg 1976; 1 I I : 126-1 3 I .
10. Hams RE, Lynch HT, Guirgis HA. Familial breast cancer: Risk to the contralateral breast. J Nu!/ Cancer Inst 1978: 60:955-960.
I I . Lynch HT, Krush AJ, Lemon HM el a/. Tumor variation in families with breast cancer. JAMA 1972; 222:1631-1635.
12. Danes BS. The Gardner syndrome: Increased tetraploidy in cul- tured skin fibroblasts. J Med Genet 1976; l3:52-56.
13. King M-C, Go RCP, Elston RC, Lynch HT, Petrakis NL. Allele increasing susceptibility to human breast cancer may be linked to the glutamate-pyruvate transaminase locus. Science 1980: 208:406-408.
14. Fishman J. Bradlow HL, Fukushima DK el ul. Abnormal estrogen conjugation in women at risk for familial breast cancer is confined to the periovulatory stage of the menstrual cycle. Cuncer Res 1983; 43: 1884- 1890.
15. Fishman J. Fukushima D, OConnor J, Lynch HT. Low urinary estrogen glucuronides in women at risk for familial breast cancer. Science 1979; 204: 1089- I09 1 .
16. Layton MA, Fortune JE, Albano WA, Kimberling WJ, Lynch HT. Cumulative lifetime risk for hereditary breast cancer. Presented at National Student Research Forum, 24th Annual Meeting, April 20-22, 1983, Galveston, Texas.
29:13-16.
17. Danes BS, Lynch HT. A familial aggregation of pancreatic cancer: An in vitro study. JAMA 1982: 247:2798-2802.
18. Lynch HT. Fusaro RM, Danes BS e! a/. Hereditary malignant melanoma, including biomarkers in the familial atypical multiple mole melanoma syndrome. Cuncer Gene! Cy!ogene! 1983: 8:325-358.
19. Danes BS, Lynch HT. Increased in v i t m tetraploidy in normals. Chncer Gene1 Cytogene! 1983; 8:8 1-87.
20. Danes BS. Occurrence of in vi!ro tetraploidy in the heritable colon cancer syndromes. Cancer 198 I ; 48: I 596- I60 I .
2 I . Danes BS, Deschner EE. Detection of in virro tetraploidy in the heritable colon cancer syndrome: Confirmation by 3 different assays Chncer (in press).
22. Adami HO, Jung B, Lindgren A, Rimsten A. Histopathological malignancy grading and familiality in an unselected series of 1 303 women with breast carcinoma. Ann Clin Rcs 1982: 14:76-82.
23. Erdreich LS, Asal NR, Hoge AF. Morphologic types of breast cancer: Age, bilateralil.y, and family history. South Med J 1980: 73:28- 32.
24. Qualheim RE, Gall EA. Breast carcinoma with multiple sites of origin. Cancer 1957; 10:460-468.
25. Rosen PP. Lesser ML, Senie RT, Kinne DW. Epidemiology of breast carcinoma: 111. Relationship of family history to tumor type. Cuncer 1982; 50: 17 1 - I 79.
26. Robbins GF, Berg JW. Bilateral primary breast cancers: A pro- spective clinicopathological study. Chncer 1964; 17: I50 I - 1527.
27. Mulcahy GM, l’latt R. Pathologic aspects of familial carcinoma of breast. In: Lynch HT, ed. Genetics and Breast Cancer. New York: Van Nostrand Reinhold Co., 1981. pp 65-97.
28. Holzgreve W, Nienhaus H, Beller FK. Carcinoma lobulare in si!u B in monozygotic twins. J Cuncer Res C/in Oncol 1982: 103:203- 206.
29. Lagios MD, Rcise MR, Margolin FR. Tubular carcinoma of the breast: Association wi1.h multicentricity, bilaterality. and family history of mammary carcinoma. Am J Clin Puthol 1980: 73:25-30.
30. Lynch HT, Albano WA, Layton MA, Kimberling WJ, Lynch JF. Breast cancer, genetics, and age at first pregnancy. J Med Genet (in press).
31. Woods KL, Smith SR. Momson JM. Parity and breast cancer: Evidence of a dual effect. Br Med J 1980: 28 1 :4 19.
32. Moon RC. Relationship between previous reproductive history and chemically induced mammary cancer in rats. In! J Cuncer 1969; 23:3 12.
33. Dao TL, Sunderland H. Mammary carcinogenesis by 3-meth- ylcholanthrene: 1. Hormonal aspects in tumor induction and growth. J Nut1 Cancer lnst 1959: 23:567.
34. McCormick GM, Moon RC. Effect of pregnancy and lactation on growth of mammary tumors induced by 7.12 DMBA. Br J Cunccv 1965: 19:160.
35. Lynch HT, Hams RE, Organ CH. Lynch JF. Management of familial breast cancer, Part 1. Arch Szcrg 1978: 113: 1053-1058.
36. Lynch HT, Hams RE, Organ CH, Lynch JF. Management of familial breast cancer, Part 11. Arch Szrrg 1978: I13:1061-1067.
37. Albano WA, Recabaren JA, Lynch HT e! a/. Natural history of hereditary cancer of the breast and colon. Cancer 1982; 50:360-363.
38. Lynch HT, Fain PR, Golgar D, Albano WA, Mailliard JA. McKenna P. Familial breast cancer and its recognition in an oncology clinic. Cancer 198 I ; 47:2730-2739.