Embed Size (px)
Citation preview
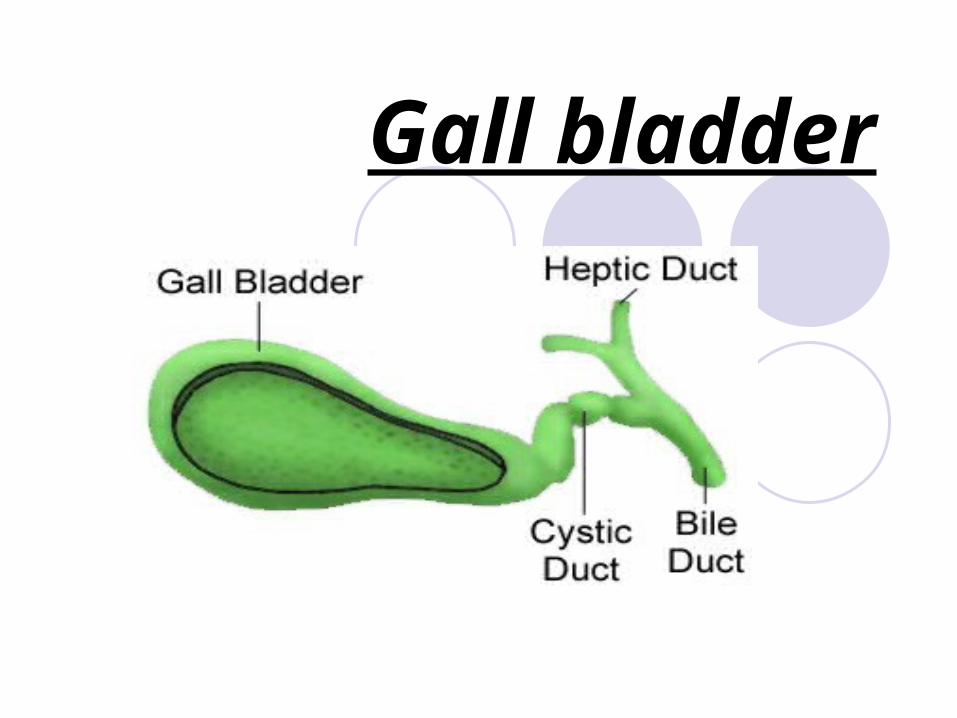
Gall bladder
Size = 7.5 x12.5 cmCapacity= 50 mlsCystic duct= 2.5cm which contains the spiral valve of
HeisterC.H.D =2.5 cmC.B.D= 7.5 cm 1-supraduodenal 2-retroduodenal 3-infradudenal 4-intraduodenal which open in ampulla's of
of Vater.
Composition of Bile:
1- 97% water
2- 1-2% bile salts
3- 1% pigments, fatty acids, cholesterol
Liver excretes bile at rate of 40 ml/hr
Functions of gall bladder:
1-Reservoir of bile
2-Cocentration of bile 5-10 times by active absorption of water, Na+, Cl-, Bicarbonate
3-Secration of mucin (20 ml per day)
Investigation of the biliary tree:
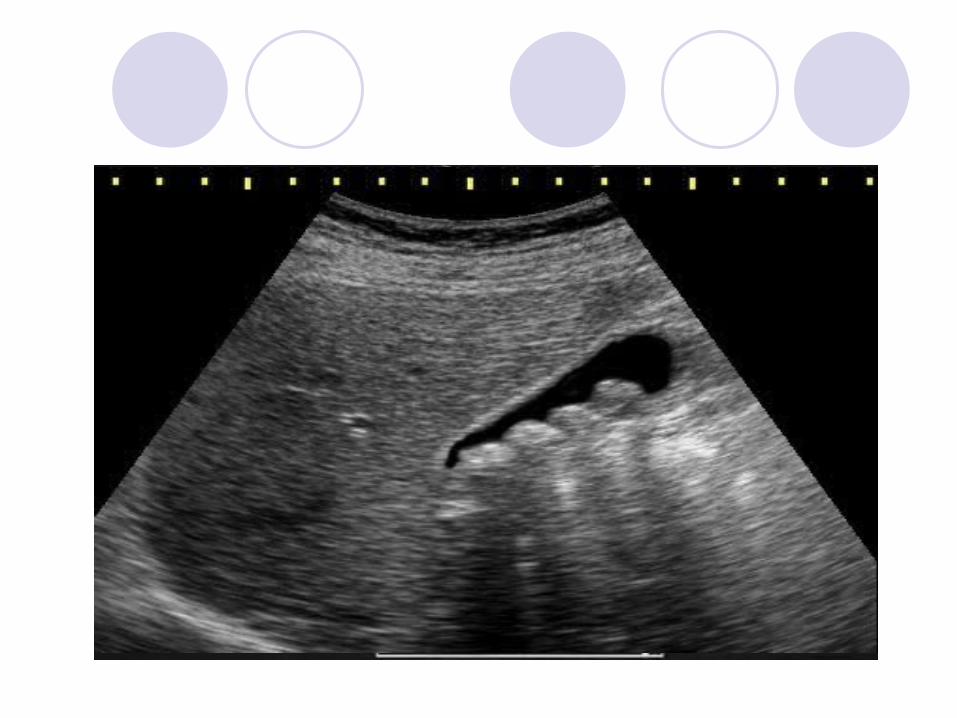
1-US: sones & size2-Plain Xray: calcification3-MRCP: anatomy & stones4-CT san: cancer & anatomy5-HIDA Scan: function6-ERCP: stones & strictures7-PTC:proximal obstruction
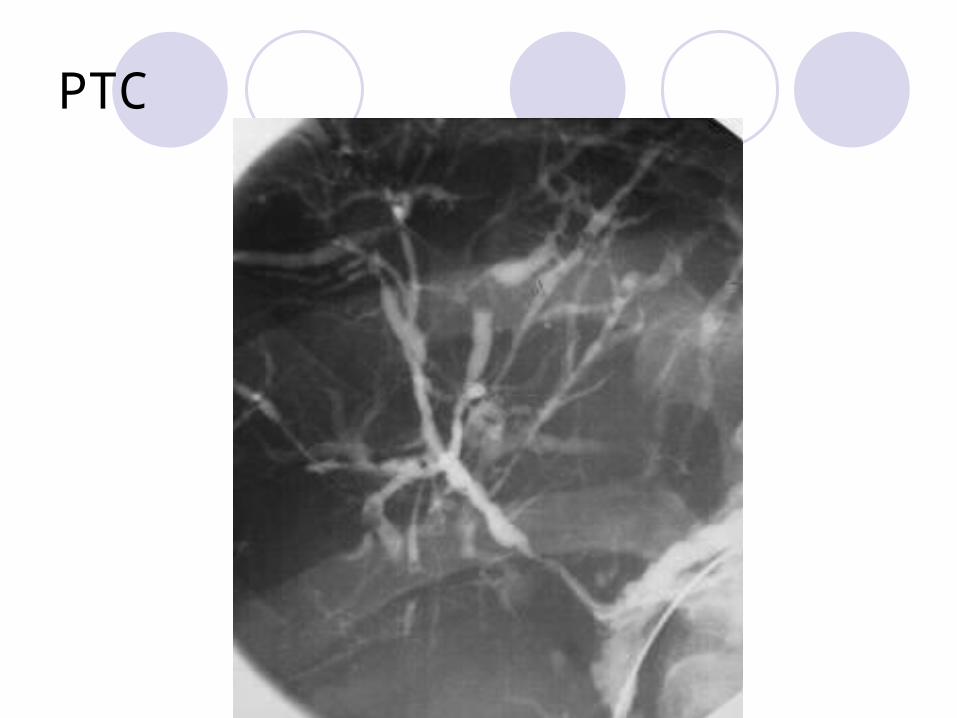
PTC
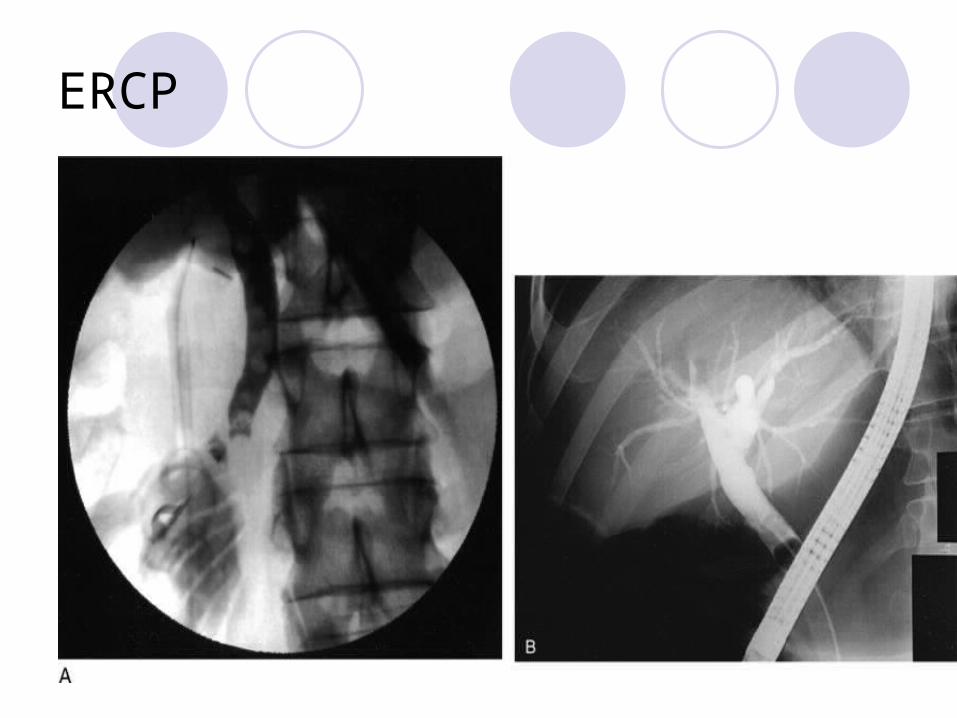
ERCP
Congenital abnormalities of Congenital abnormalities of GB & bile ducts:GB & bile ducts:
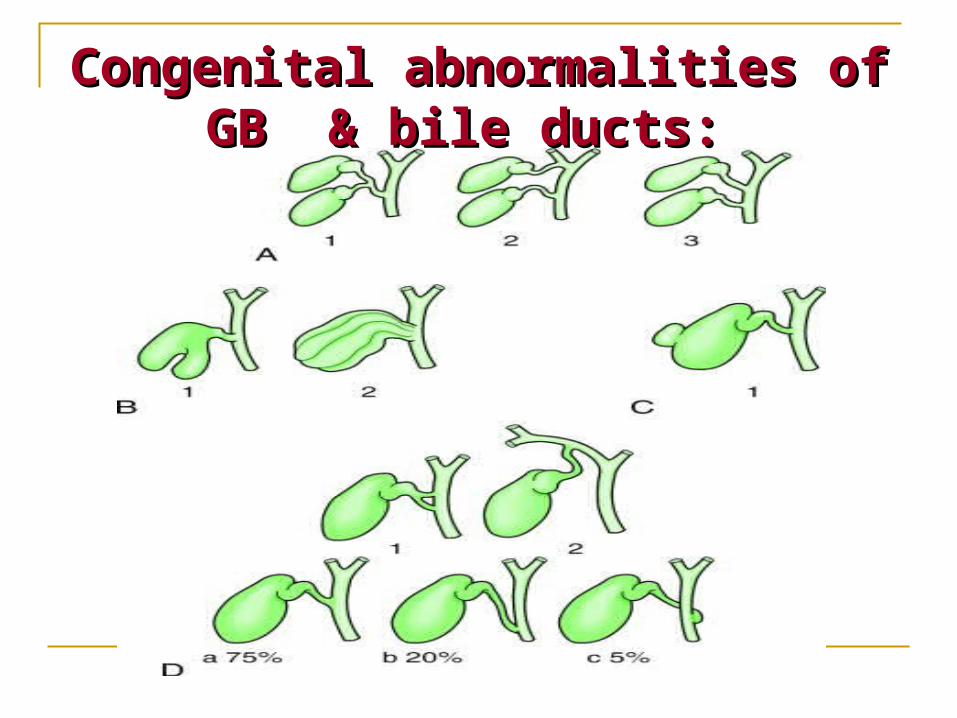
Congenital abnormalities of GB & bile ducts:
1-absence of GB.
2-phrygian cap 2-6%
3-Floatting GB
4-Double GB
5-Absence of cystic duct
6-Low insertion of cystic duct
7-accessory cholecystohepatic duc
8-Atresia
9-choledocal cyst
Biliary Atresia
Might be due to viral infection
Correctable 10%
Uncorrectable 90%
CF:
*1\3 jaundice at birth
*all jaundice by the end of 1st week
Differential diagnosis
1-alpha one antitrypsin deficiency2-choledocal cyst3-insspissated bile syndrome4-neonatal hepatitis
Diagnosis:
*liver function tests*radioactive isotope scan---failure of the
isotope from reaching the intestine*Laparoscopy\laparotomy---liver biopsy
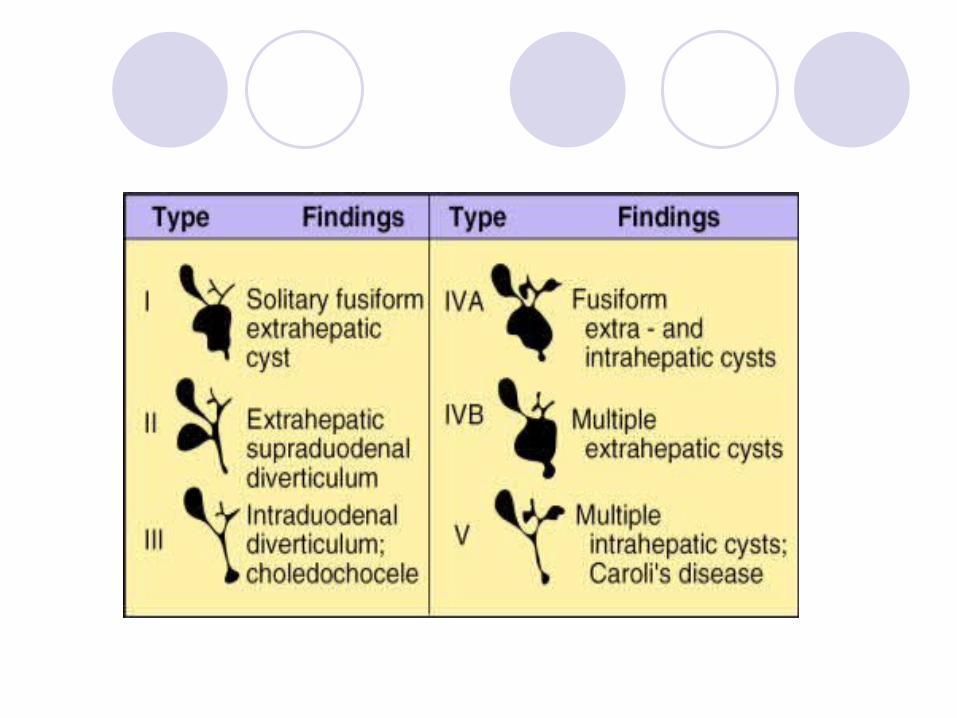
Choledocal cyst
Due to specific weakness in a part or whole wall of CBD
*female > male
*at age of 6 months
CF
*attacks of obstructive jaundice
*Cholangitis \ abdominal singns
*fever
*upper abdominal swelling.
Diagnosis:
CF+ US +MRI
Treatment:
*radical excision if possible
*choledochocystojujenostomy.

Gall stones
Gall stones
Types of gallstones
1-Pure cholesterol (10%). Often solitary, large (> 2.5cm), round.
2-Pure pigment (bile salts; 10%). Pigment stones are of two types:*black (associated with haemolytic disease);
*brown (associated with chronic cholangitis and biliary parasites).
3-Mixed (80%). Most common; usually multiple
Causes
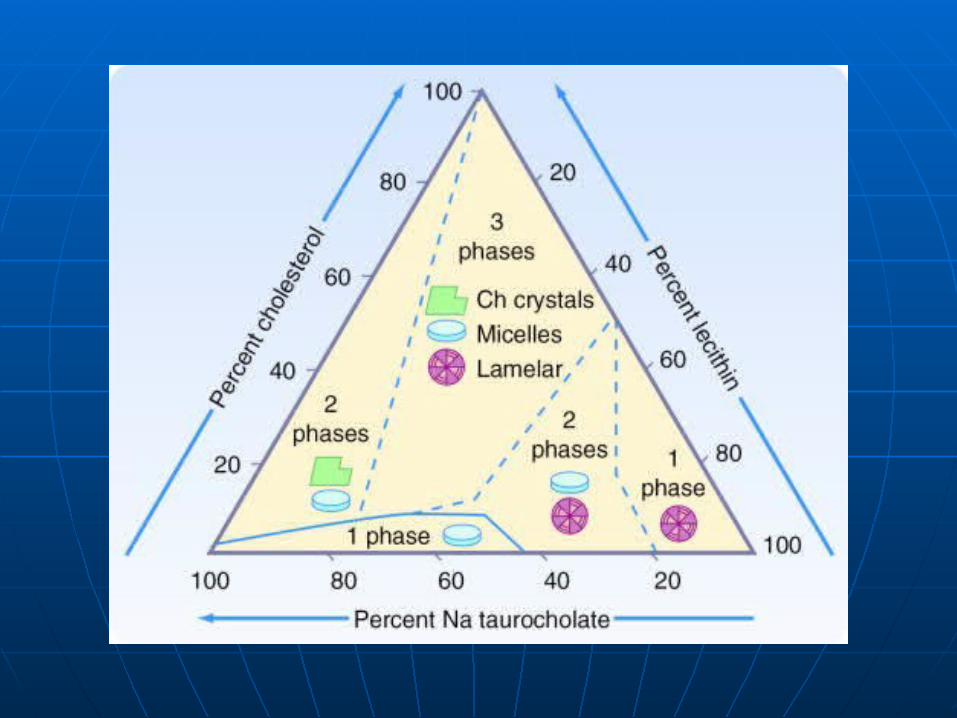
1-supersaturated bile:
*age
*sex
*genetics
*obesity
*diet
2-impaired gall bladder function:
*emptying
*absorption
*excretion
3-cholestrol nucleating factors:
*mucus
*glycoprotein
*infection
4-absorption\enterohepatic circulation of bile acids:
*deoxycholate
*bowel transit zone
*faecal flora
*ileal resection
*cholestyramine.
Other factors:
A-Metabolic
B-Infective
C-Stasis
Saint's triad
*gall stones
*diverticular disease
*hiatus hernia
Presentation & DX
*silent in 85%
*acute cholecystitis:pain ,radiation,fatty meals
*chronic cholecystitis:flatulent dyspepsia & heart burn which has to be differentiated from:(hiatus hernia, chronic pancreatitis & peptic ulcer)
DX
CF+US+X-ray
Treatment:
*NBM + IVF
*biliary pain :(analgesia,spasmolytic,antiemetic)
*antibiotic(broad spectrum)
Surgery:urgent(for complicated cases),early(next available list) & delayed
Complications & effects of gall stones
A-on GB:1-acute cholecystitis2-chronic cholecystitis3-empyema4-mucocele5-biliary colic6-CA7-gangerene8-perforation
B-on bile ducts:1-obstructive jaundice
2-cholangitis—liver abscess
3-pancreatitis
C-on the bowel:1-cholecystoenteric fistula
2-gall stone ileus.
Achalculous cholycystitis:
Needs oral cholecystogram for dx
Presence of cholesterol crystals in duodenal aspirate.high mortality eraly perforation & gangerene
Usually seen after:major trauma,burns ,in ICU or patient recovering from major surgery





























