Embed Size (px)
Citation preview

[ 367 1
FURTHER OBSERVATIONS ON THE GENETIC BASIS OF PRIMARY HYPEROXALURIA
BY E. F. SCOWEN, R. W. E. WATTS AND E. G. HALL The Medical Unit, St Bartholomew’s Hospital, London, E.C. 1
and The Adler Hey Children’s Hospital, Liverpool
Primary hyperoxaluria (Archer, Dormer, Scowen & Watts, 1957) is characterized by a con- tinuous high urinary oxalate excretion, resulting in urolithiasis which begins in childhood. The renal parenchyma is progressively destroyed by the combined effects of nephrocalcinosis, recur- rent attacks of pyelonephritis, and renal hypertension ; early death from renal failure appears to be invariable, and widespread extrarenal deposits of calcium oxalate monohydrate are found at post-mortem (Scowen, Stansfeld & Watts, 1959). The nature of the underlying biochemical lesion is obscure, but direct evidence that glycine is the precursor of at least a considerable proportion of the oxalate which these patients excrete has been obtained (Scowen et al. 1958; Watts, Scowen & Crawhall, 1958). The results of a survey which was undertaken in order to determine whether an hereditary pattern is demonstrable in primary hyperoxaluria has been reported from one of our laboratories (Archer et al. 1958). In that survey, evidence of an elevated urinary oxalate excretion and of any morbidity or mortality which might be attribut- able to urolithiasis was sought among the relatives of three proven cases of the disease which had arisen in different families; it was tentatively concluded that the findings were ‘compatible with primary hyperoxaluria being due to the operation of a rare recessive character’. We are unwilling to accept as completely conclusive, a diagnosis of primary hyperoxaluria which is unsupported by chemical measurement of the urinary oxalate excretion and in the only family in which there was any evidence for the occurrence of the disease in a relative (a sib) this measure- ment was not available on the sib concerned. We were therefore obliged to make the reservation that in the absence of more evidence for the occurrence of the disease among sibs, our findings could not be regarded as offering clear-cut support for the hypothesis that primary hyperoxaluria is due to the operation of a rare recessive character.
The present paper records in detail a further similar investigation of four previously un- reported families in which cases of primary hyperoxaluria have arisen; reference will also be made to a fifth family which has been studied in less detail. This brings the total number of families which we have studied to eight and enables us to draw more definite conclusions on the genetic aspects of the disease.
METHODS Many of the 24 hr. urine collections were made under out-patient conditions, and it is possible that, in spite of careful instructions in the collection technique, some of the specimens may have been incomplete. Our results are therefore expressed in terms of the urinary oxalate/urinary creatinine ratio, as well as the weight of oxahte excretd per 24 hr. The analytical procedures employed were identical with those used in the previous investigation (Archer et al. 1958); and the families have been numbered 4 to 8, numbers 1 to 3 being those previously studied (Archer et al. 1958).

368 GENETIC BASIS O F PRIMARY HYPEROXALURIA
RESULTS Furnily 4 (Fig. 1 and Table 1). Study of this family provides evidence for the occurrence of the disease in sibs. Of ten sibs of the propositus (IV. 36) surviving infancy, two (IV. 45, IV. 46) are alive with urinary calculi and have high urinary oxalate excretion values, one (IV. 38) died from renal failure associated with bilateral renal calculi at the age of 7 years and retrospective clinical appraisal suggests strongly that this child also suffered from primary hyperoxaluria. One other sib (IV. 37) is alive and well (aged 13 years) without clinical or radiological evidence of renal calculi, but has a urinary oxalate excretion which is of the same order of magnitude as that of the members of the family who have developed calculi. There is no history of parental con- sanguinity in this family.
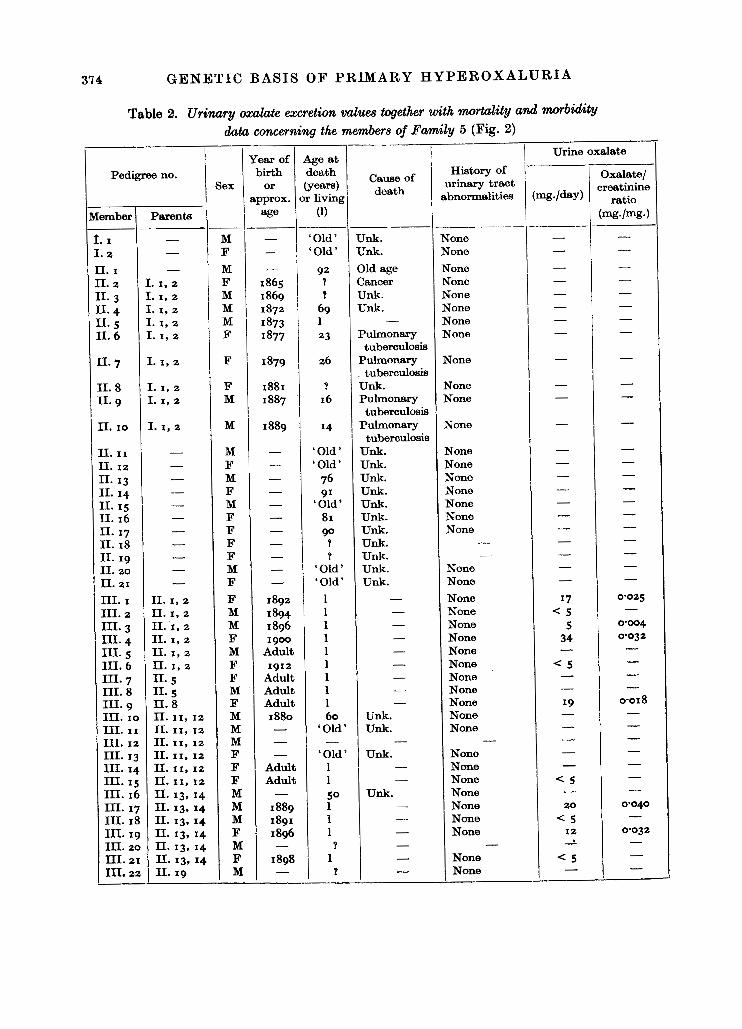
Fumily 5 (Fig. 2 and Table 2). Two sibs (V. 5, V. 6) are affected in this family. There are no unaffected sibs and no history suggesting parental consanguinity.
Family 6 (Fig. 3 and Table 3). In this family, one sib (IV. 10) out of four is affected, and the parents of the propositus are h t cousins.
Furnily 7 (Fig. 4 and Table 4). Except for the propositus (111. 13), who is one of two sibs living beyond infancy, no abnormally high levels of urinary oxalate were encountered in this family and there is no history of parental consanguinity.
FurniZy 8. In this family, only the propositus (male aged 2 years 9 months), with bilateral renal calculi, his new-born sister, parents and maternal grandmother were available for study. The propositus alone had a high urinary oxalate excretion (68-110 mg. (COOH),. 2H,0/24 hr., 0-388-0-412 mg. (COOH),. SH,O/mg. urinary creatinine). There is no history of parental con- sanguinity and the parents are not aware of any relatives with a history of urinary tract disorders.
DISCUSSION The clear-cut evidence which we have obtained for the occurrence of primary hyperoxaluria among sibs in the absence of any detectable abnormality in the parents, together with the finding of one family in this small series in which the parents of the propositus were first cousins, strongly suggests that the disease is due to the operation of a rare recessive character. Shepard (1958), Shepard, Krebs & Lee (1958) have briefly reported the occurrence of hyperoxaluria in the members of three successive generations in one family. In this family, the mother and maternal grandfather of the propositus, neither of whom display evidence of renal calculi, excreta 105-185 mg. oxalate/24 hr. and 61 mg. oxalate/24 hr., respectively, compared with a ‘top normal for 24 hr. urine oxalate of around 55 mg.’ (Shepard, 1958). Here, the mode of inheritance may be dominant so that the condition differs from the one which we have studied; there is also apparently a diminished liability for the affected members to develop urinary calculi. We have so far encountered only one subject (family 4, subject IV. 37) with a high urinary oxalate excretion but no detectable calculi or nephrocalcinosis, and this girl is only 13 years old. Oigaard & Sijderhjelm (1957) reported a family in which two sibs had died from renal failure at the ages of 17 and 27 years, respectively, and had been found to have post- mortem evidence of calcium oxalate nephrocalcinosis, another sib had died at the age of 13 years from renal failure of undetermined mtiology, and a fourth sib was alive aged 32 years, but was suffering from bilateral renal calculi and chronic renal failure. Two other sibs, the parents and the two children of one of the unaffected sibs were said to be healthy. It may well be that these

E. F. SCOWEN, R. W. E. WATTS A N D E. G. HALL 369
,Ii- -E

370 GENETIC BASIS O F PRIMARY HYPEROXALURIA
Table 1. Urinary oxalate excretion dua together with mortality and morbidity data concerning the members of Family 4 (Fig. 1)
Member
I. I I. 2 1- 3 1. 4 11. I 11. 2 11. 3 11.4 11. 5
II. 7
II. 9
11. 6
II. 8
11. I 0 11. I1
11. I 2 11. 13 11. 14 11. I5 11. 16 II. 17 II. I8 11. 19 11. 20 11.21 11.22 11.23 11.24 III. I III. 2 111. 3 111.4 III. 5
III- 7 m. 8 111. 9 III. I 0 III. I1 III. 12 III. 13 III. 14 m. I5 III. 16 111. 17 111. 18
111. 6
Parenta
- - - - - - - - - -
1. I, 2
1. I, 2 1. I, 2 c. I, 2
r. I , 2
I. I, 2 I. I, 2 I. I, 2 I. I, 2 I. I, 2 I. I, 2 I. I, 2 I. I, 2 I. I, 2 1. 31 4 - - -
11. I, I1 11. I, I 1 11. I, I1 11. I, I1 11: I, I1 11.7
11. 7 11. 7 11. 8 11. 8 II. 8 11. 9 II. 9 11. I 2 II. I2 11. I 2 11. 12 11. 13
-
sex
M F M F M M M M M F M F F M F
F M F F F - - - - M F F F M M F M M M
M F F F M M F M M M M F
YeeS of
birth or
'ppmx. age - - - - 1882 - - - - - - I893 -
Adult I 898
1901 Adult 1916 1917 1919 - - - - - 1888 - - I 920 I923
Adult I930 I932 -
1926 Adult I924
Adult Adult Adult Adult I924 1926
Adult Adult Adult
Age at death (y-1
or living
(1)
50 9dult , Old ' 'Old'
Adult Adult Adult Adul t Adult
-
65 - 60 1 1
1 1 1 1 1
Infant: Infctnc. Infane. Infanc:
50 1
Adult Adult
1 34 1 1 1
Child- hood 4
1 1 1 1 1 1 1 1 1 1 1
c a w of death
Cancer Dysentery Unk. Bronchitis
Unk. Unk. Unk. Unk. Unk. Carcinoma
Unk.
-
-
- -
- - - - -
Unk. Unk. unk. *
Unk. Killed
Unk. Unk.
Killed
-
-
- - -
Killed
Convulsions - - - - - - - - - - -
History
tract abnor-
malities
of urinary
Tone gone Tone gone Vone Yone Xone None None None None None None None Chronic uri- nary infec- tion no calculi
None None None None None - - - -
None None None None None None NonB None None None
None None None None None None None None None None None None

E. F. SCOWEN, R. W. E. WATTS AND E. G. HALL 37 1
Pedigree no.
Member
11. 19 11.20 11. 21 11.22 11.23 11.24 11.25 111. 26 .II. 27 :11. 28 111. 29 31. 30 XI. 31 [II. 32 [II. 33 111. 34 [V. I cv. 2 [V. 3 [V. 4 cv. 5 CV. 6 cv. 7 [V. 8 cv. 9 cv. I 0 IV. 11, I 2 IV. 13, 14 tv. 15 W . 16 W . 17 tv . I8 IV. 19 IV. 20 IV. 21 IV. 22 IV. 23
IV. 28 IV. 29 IV. 30 IV. 31 IV. 32
33 34
IV. 35 IV. 36
m. 24-27
Parents
[I. 14 [I. 14 [I. 15 [I. 15 [I. 16 [I. 16 [I. 21, 22 [I. 21, 22 [I. 2 1 , 22 11. 21, 22 [I. 21, 22 11. 21, 22 11.21, 22 11. 21, 22 11. 21, 22 11.21, 22 111. 2 III. 2 111.3 111.3 III. 3 111. 3 111.8 111. 8 111. 8 111. 8 111. I 0 III. I1 111. I 2 III. 12 111. 14 111. 14 111. 15 111. 17 111. 17 III. 17 11;. 17 111. I8 III. 19 III. 19 III. 20 111.21 III. 21 rn. 22 III. 22 III. I , 28 111. I, 28
sex
__ F M F M M M M F M F F M M F M F M M F &I F F M M F F
Unk. Unk.
M M
Unk. Unk
F M M M M
Unk F M F M F F M F M'
__
Yf3al. of
birth or
Lpprox. age
I929 1931 I932 I935 - I946
Adult 1916 1919 1922
Adult Adult Adult Adult Adult I935
1 947
19-50 1951 1952 I953 I955
1946
I946
1956 I958
Child Child Child Child '956 1958 I954 1951 I952 I955 1956
1948 -
1951 I954 I953 I953 1954
1941 I943
I958
Table 1 ( cmt . )
kge at death Y-)
or living
(1)
1 1 1 1
1 1 1 1 1 1 1 1 1
1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
4
-
History of urinary
tract abnor-
malities
Tone Tone Tone gone gone gone gone gone gone gone gone Hone Hone Hone
Tone None None None None None None None None None None None
None None None None None None None None None
None None None None None None None None Bilateral rend calculi
-
-
-
Urinary oxalata
- 0.014 - - -
0.020
0'01 I 0.013 0.016 0'012 -
0.021 0.017 - -
0'02 I
- -
0.057 0.061
0.036 0.047'
- - - - - - - - - - 0.039 0.028 0.049 0.040 - -
0.025 0-017 0.036 0.039 0.035 - -
0.010
0.324 0'347 0.301
* Propositus.

37 2 GENETIC BASIS O F PRIMARY HYPEROXALURIA
Pedigree no. r . Member
- IV. 37
IV. 38
IV. 39 IV. 40 IV. 41 IV. 42 IV. 43 IV. 44 IV. 45
IV. 46
IV. 47
IV. 49 IV. 5 0 IV. 51 IV. 5 2 IV. 53 Is7* 54
IV. 48
55 IV. 56
57 IV. 58
IV. 60 IV. 61 IV. 62 IV. 63 IV. 64.65 IV. 66 IV. 67 IV. 68 N. 69
IV. 59
Parents
111. I , 28
III. I, 28
111. I, 28 111. I, 28 111. I, 28 111. I, 28 III. I, 28 111. I, 28 111. I, 28
111. I, 28
111. 25 111. 26 111. 26 111. 26 III. 26 III. 26 111. 26 III. 26 III. 27 111.27 111.27 111.29 111.29 III. 29 III. 31 III. 31 111. 31 111. 32 111. 33 III. 34 III. 34 111.34
-
sex
__ F
F
M M F F F F M
F
M F M F F M M M F F M M M M F F M
unk Unk
M F F -
YeCrr of
birth or
tpprox. age
I945
I946
1948 1949 1950 1951 1951 I953 I954
1956
1937 I937 I 944 1946 1948 1950 '953 I954 I940 I945 I949 I 947 1949 '954 I944 I 949 I953 - - 1955 1957 I957
Table 1 (crmt.)
Age at h t h :Years)
or living
(1)
1
7
1 1 1 1
1 1
D W00h
1
1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
1 1 1
-
cause of death
Histol=y of urinary
tract abnor-
malities ~ _ _ None
Bilateral renal calculi
None None None None None None Bilateral renal calculi
Unilateral renal calculi
None None None None None None None None None None None None None None None None None
- -
None None None
Urinary oxalate
Oxdate/ creatinine (mg-lmg.)
0' I93 0.213 -
- 0.015 0.013 0.015 - - 0.528 0.46 I
0.830 0.569 0.669 0.802
0.030 0.026 0.036 0.030 0.064 o-oqq 0.032 0.028 0.056 0.067 0.038 0-015 0.030
0.006
0.01 I
0.010
0.020 - - - - -

KEY
0 H
yper
oxal
uria
\ P
ropo
situ
s, -
a $
Hyp
erox
alur
ia w
itho
ut i
ncid
ence
of
sto
nes
pl 's
\ Stil
lbor
n o
r di
ed i
n in
fanc
y d
Dea
d
Figu
re u
nder
is
urin
ary
oxal
ate
excr
etio
n m
g./d
ay
u e
I,
,*
I 13
d
14
15
I <
..
..
I
14
96
-202
-
I 20,0
,
V (c
ont.)
24
27
48Q
9
m 4
rLJ cz 0
M 8 "W
Fig
. 2.
Pedi
gree
of
Fam
ily 6
.
0 4
0
37 4 G E N E T I C BASIS O F P R I M A R Y H Y P E R O X A L U R I A
data concerning
Year of Pedigree no. birth
sex Or approx.
Member Parents age
I. I - M - I. 2 - F - II. I - M -
-_______
II. 2 I. I, 2 F 1865 11.3 I. I, 2 M 1869
11.6 I. I , 2 F 1877
II .7 I. I, 2 F 1879
11.9 I. I, 2 M 1887
11.4 I. I, 2 M 1872 II. 5 I. I, 2 M 1873
11.8 I. 1, 2 F 1881
11. I 0 I. I, 2 M 1889
11. I1 - M - 11. 12 - F - 11. 13 - M - 11. 14 _- F - 11. I5 - M - 11. 16 - F -
- F - II. 17 11. 18 - F - 11. 19 - F 11.20 - M - 11.21 - F - III.1 I I . I , 2 F 1892 111.2 11. I, 2 M 1894 III. 3 11. I, 2 M 1896 111.4 11. I, 2 F 1900
111. 6 II. I, 2 F 1912
-
111.5 11. I, 2 M Adult
III. 7 11. 5 F Adult 111.8 11.5 M Adult 111.9 II. 8 F Adult 111. 10 II. 11, 12 M 1880 111. 11 II. 11, 12 M - 111. 12 11. 11, 12 M - 111. 13 11. 11, 12 F - III. 14 II. 11, 12 F Adult 111. 15 II. 11, 12 F Adult III. 16 II. 13, 14 M - 111. 17 11. 13, 14 M 1889 III. 18 11.13, 14 M 1891 111. 19 11. 13, 14 F 1896 111. 20 11. 13, 14 M - III.21 II. 13, 14 F 1898 III.22 11.19 M -
the members of Family 5 (Fig. 2 )
Age at I I urineoxaM,e
Oxdate/ urinary tract creatinine History of
Cause of death
(years) death or living abnormalities (mg./day) ratio
(1) (mg./mg*) - _.
- - ‘Old’ Unk. None ‘Old’ Unk. None
92 Oldage None
- - - -
- ? Cancer None - ? unk. None - -
- - 69 Unk. None 1 - None
tuberculosis
tuberculosis 4 unk. None
tuberculosis
tuberculosis
- - 23 Pulmonary None - -
26 Pulmonary None - -
16 Pulmonary None - -
14 Pulmonary None - -
- -
- - ‘ Old ’ Unk. None ‘Old’ Unk. None
76 Unk. None 91 Unk. None
‘ Old’ Unk. None 81 Unk. None 90 Unk.
4 unk. - ? Unk.
- - - - - - - - - -
- None - - - - - - - - ‘Old’ Unk. None
‘ Old ’ Unk. None - - 0.025 - None 17
None < 5
None 34
None -=5
1 - 1 - 1 - None 5 0.004
0’032 1 - 1 - None 1 - 1 - None 1 - None 1 - None I9 0018 60 Unk. None
‘ Old ’ Unk. None
‘ Old ’ Unk. None
- - - - -
- -
- - - - - - - - - - -
- 1 - None - None < 5 1 -
50 unk. None - 1 - None 20 0.040
None < 5 1 - 1 - None I 2 0.032
None < 5 1 - - None -
- -
-
- - - - ?
?
- -

375 E. F. SCOWEN, R. W. E. WATTS AND E. G. HALL
Pedigree no.
aember
III. 23 111.24
111. 26 111. 27 111. 28 111. 29 111. 30
111. 32
111.25
111. 31
111.33 III. 34 IV. I
IV. 2
IV. 3
IV. 4 IV. 5
IV. 7
IV. 9
IV. I0 IV. 11 IV. I2 IV. 13 IV. 14 IV. 1.5 IV. 16 IV. 17 IV. I8 IV. 19 IV. 20 IV. 21 IV. 22 IV. 23 IV. 24 N. 25 IV. 26 IV. 27 IV. 28 N. 29 IV. 30 N. 31 IV. 32 IV. 33 IV. 34 IVI 35
IV. 6
IV. 8
Parents
11. 19 11. 19 11.19 11. 20, 21 II. 20,21 11. 20, 21 11. 20, 21 11. 20, 21 11. 20, 21 11.20, 21 11.20, 21 II. 20,21
III. 2,15 m. 2,'s 111. 2, 15
111.2, I5
111.7 III. 7 111.7
III..6
111. I0
111. 10
III. I1 III. I1 III. I1 III. I1
111. I1
III. I1 III. 13 ID. 13 ILT. 13 III. 13 111. 13 111. 13 III. 16 III. 16 III. 16 III. 16 III. 16 III. I8 III. I8 III. I8 III. I8 111. 19 III. 19 111. 19 III. 19
-
Sex
M F F M M M M M F F F F M F M
F F M M M M
M M F F M M F M M M F F M M M F F M F M F M M F M M -
Year of birth or
Bpprox. age
- -
Adult - -
1891 I897
1898
Adult
-
-
- 1925 1926 I 928
I929 1 946 - - - -
I913 Adult Adult Adult Adult Adult
Adult
Adult Adult Adult Adult Adult Adult Adult Adult Adult 1913
Adult Adult 1928 1916 1918 1921 I923
-
-
Table 2 (cont.)
? ?
1 50 50 1 1
Adult 60
Adult 1
1 1 1
1 1 1 1 1 31
1 1 1 1 1 1 I7 1
Adult 1 1 1 1 1 1 1 1 1 1 1 r 1 1 1 1 1
-
History of u&aq tract abnormalities
~
None None None None None None None None None None None
None None None
None None None None None None
None None None None None None None None
None None None None None None None None None None None None None None None None None
-
-
Urine oxalate

376 GENETIC BASIS O F PRIMARY HYPEROXALURIA
btember
Pedigree no.
N. 36
IV. 38
39 IV. 40 IV. 41 IV. 42 Iv- 43 IV. 44 IV- 45 IV. 46 IV- 47 IV. 48 v . I v. 2 v. 3 v . 4 v. 5
V. 6
v* 7 V. 8 v. 9 v. I 0 v. I1 v. I 2 V. 13 V. 14 v . 15 V. 16 V. 17 V. 18 V. 19 v. 20 v. 21 v. 22 v. 23 V. 24 v. 25 V. 26 v . 27 V. 28 V. 29 V. 30 V. 31
IV. 37
v. 32 v. 33
Parents
UI. 19 El. 19 m. 21, 28 [II. 21, 28 m. 25 III. 25 III. 25 III. 25 III. 26 III. 26 III. 27 III. 27 III. 29 J.V. I
4 Iv. 4 IV. 4 IV. 39 38
Iv. 3.38
N. 11 IV. 13 IV. 13 N. 13 IV. 14 Iv. 14 IT. I5 Iv. I5 IV. I5 IV. 15 IV. 15 IV. 17 IV. 17 IV. 18 IV. 19 Iv. 19 IV. 19 IV. 19 IV. 19 Iv. 21 Iv. 2 1 Iv. 21 IV. 21 N. 22 Iv. 22 IV. 22 IV. 28
3eX
- M F F
F M M F F M F M F M F M M F F*
M
M F F F - - M F M F F M F F M M M M F M M M F F M M F -
'ear of birth
or pprox. age
I934
I929
1931 Adult Adult Adult Adult Adult Adult Adult Adult Adult
'95 1
I955 1956 1958 I951
I953
-
I946
I938 I937
I947 I947 '955 I943 I943 '945 I947 '947 1931 I945
Adult 1923
Adult Adult Adult I933
Child Child 1948 I947 I949
I937
7938
1956
Table 2 (cont.)
4ge at death Y e w ) r living
(1)
1 5/12 1
1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
1
1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
History of urinary tract abnormalities
Tone
Tone
Tone Tone Tone Tone Tone Tone Tone
-
- -
Qone Tone Tone Tone Qone 3ilateral renal calculi '
?aesedurinary calculi Qone Tone gone gone gone gone gone None None None None None None None None None None None None None None None None None None None None
Urine oxalate
0.023 0.013 -
* Propsite.

E. F. SCOWEN, R. W. E. WATTS A N D E. G. HALL 377
Pedigree no.
dember
v. 34 v- 35 V. 36 v. 37 V. 38 v- 39 V. 40 V. 41 V. 42 v- 43 v. 44 v. 45 v- 47 v. 48 v. 49
V. 46
Parents
IV. 28 IV. 28 Iv. 28 rv. 29 IV. 30 IV. 33 Is7. 33 Iv- 33
33 N- 35
44 45
N. 45 N- 45 N. 48 IV. 48
sex
-- F F F M M M M F F M M M F M F F
Year of birth
spprox. age
1939 1 942 1954 1952
I942 I944
I952 1955
Adult I938 I943 I953
Or
I956
1948
- -
Table 2 (cont.)
1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
Cause of death
History of urinary tract abnormality
None None None None None None None None None None None None None None None None
~
urine oxalate
KEY 0 Hyperoxaluria B Stillborn or died in infancy d Dead
Figure under is urinary oxalate excretion mg./day
Fig. 3. Pedigree of Family 6.

37 8 GENETIC BASIS O F PRIMARY HYPEROXALURIA
Table 3. Urinary malate excretion values together with mortality and morbidity data concerning the members of Family 6 (Fig. 3 )
Pedigree no.
Member
I: I I. 2 1- 3 1- 4 1. 5
1. 7
I. 8 1- 9 I. I 0 I. I1 I. I 2 I. 13 11. I II. 2
II. 3 11.4 11. 5 11. 6 11.7 11. 8 11. 9 11. I 0 11. I1 II. I 2 11. 13
11. 18 11.19 11.20 XI. 21 11.22 11.23 11.24 11.25
11. 26 II. 27 II. 28 11.29 11. 3-32 11- 33-37 11.38-47 11.48-5 I rn. I In. 2
3
I. 6
11. 14-17
111.4
Parents
Sex
M F F F M M M
F M F F F F M M
F M F F F F M M F F M
Unk M F F F F F M M
F F F F
Unb Unk Unb Unb
M M M
M
of birth
or !ppmx.
age
I877 I879
I893 I 882
1898 - - 1881 - - - - - - -
- 1891 - - -
Adult Adult - - - -
Adult Adult Adult Adult Adult Adult Adult Adult -
Adult Adult Adult Adult Adult Adult Adult Adult 1910
Adult -
1919
4ge at
:Y-)
(1)
death
r living
1 1 1 1 1
? ?
47 1
? P ? ?
? ?
? 1
1
1 1
38
-
I
7 5 ?
1 1 1 1 1 1 1 1
1
1 1 1 1 1 1 1 1 1 1 - 1
cause of death
- - - - -
?neumonie, Killed in adult life Killed
unk. Dnk. 2ancer Unk. bk. Killed in adult life
Sildbirth
Pneumonia
-
-
- - - -
S d d s ?
Killed weak spine
- - - - - -_ - -
Killedin adult life - - - - - - - - - -
Killed in adult life -
History of urinary tract abnormality
None None None None None None None
None None None None None None Nephrectom y None
None None . None None None None None
None None None None None None None None None None None None
None None None None None None None None None None None
None
-
Oxalate/
mg./mg.)
lreatinine ratio

E. F. SCOWEN, R. W. E. WATTS AND E. G. HALL 37 9
sex
M Unk. F F
- - - F F F F F F M M M
- F M M M F F
-
- M*
F
F
M
M M F
F F
F M M F
Table 3 (cont.) urine oxalate Year of Ageat
birth death History of OXf%late/
age (1) (mg./mg. 1
Or (Years) cause death of urinary tract creetinine approx. or living abnormality (mg./&Y) ratio
- ~ ~ - I924 1 - None 12 0.009 - - Adult 1 - None
Adult 1 - None 1920 37 chest None
- - - -
trouble - - - - Infancy unk. - - - - ? - - - Adult 1 - None
1926 I - None I 0 0.014 1928 1 - None I 2 0.007
0.006 None 7 I929 1 - - Infancy unk. - - Infancy unk. - - - 1936 1 - None 26 I939 1 I940 1
None < 5 Adult 1 - None - I947 1
Adult I - None I942 I - I944 1
- -
- - None I 0 0.004 - None 20 0.014
- -
-
- - - +
None < 5 None < 5 None ( 5
- o Still-born - - - o Birthtrauma
- -
- - 1948 1
- - - - 6/12 Congenital Congenital - 1 -
hydro- hydrone- cephalus phrosis. Py-
elonephritis. No stones - I -
Child 1 - None 1947 1958 Uraemia Recurrenturi- 0.352
C d C U l i { gi 1 0'254
{<; 1 0 z 8 - None 0.016
nephrocalci- 0.288 nosis I
1950 1 - None
- - L;
{< : I952 1
0.019 0.040
I955 1 - None
None I3
None < 5 Child 1 - None - Child 1 - None Child 1 - None Child 1 - None 1948 1 - None I 2 0.025
- None 0.028
1948 1 - 1950 1 - None I5 0.061 1952 1 - None 18 0.072 I953 1 -
- -
- - - - - -
- None 1 : - -
Pedigree no.
I Member I Pmnta
III. 5
111. 15
111.6-13 111. 14
111. 16 111. 17-26 111.27-34 III- 35 III. 36 111.37 111. 38 111. 39 III. 40 III. 41 III. 42 111.43 III. 44-46
IV. I N. 2 IV. 3 IV. 4 N. 5
111.47-50
IV. 6
IV- 7-9 N. 10
N. I1
N. I 2
IV. 13
N. 14 N. 15 IV. 16 N. 17 N. I8 N. 19 N. 20 Iv. 21 Iv. 22 N. 23 N. 24 IV. 25
11. I, 5 11. I, 5 11. I, 5 II. 6
III. 14 III. 4 9 37
In- 4 9 37
In- 41 37
III. 4* 37
"II. 35
In- 35 In- 35 111. 35
111.35 III. 35 III. 36 III. 36 lll. 40
35
35
I m-40

380 GENETIC BASIS O F PRIMARY HYPEROXALURIA
I 'ep I1
111 1
Fig. 4. Pedigree of Family 7.
Table 4. Urinary oxdate excretion values together with mortality and morbidity data umcerning the members of Family 7 (Fig. 4)
Pedigree no.
[ember
[. I c. 2
1. 3 [- 4 rI. I rI. 2
3
TI. 4 tI* 5 [I. 6 II* 7 T I . 8 TI. 9 TI. I0 TI. I1
11. I2
III. I 111.2 111. 3 III- 4 111.5 III. 6 m- 7 III. 8 m. 9 m. I0 m. I1 m. 12 111. 13
III. 14
III. 16 m. 15
Parents
- - - -
I. I, 2 I. I, 2 I. I, 2
I. I , 2 I. I, 2 I. I, 2 I. I, 2 I. I, 2
1. 39 4 1. 3.4 1.3.4 1. 39 4 11. I 11. I II. I 11. 2 11. 4 11.4 II- 4 11.6 II. 6 II. 8 II. 8 11. 8 II .7, I2
11.7, 12 11. I1
11. I1
3eX
- M F M F M M M
F M F M F M F F F F M M F M M F F M F F M M*
F F M
__
felw of birth, or
bpprox. ege
I 887 I 892 1900
Adult
1913 1916 I919
1921 I923 I925 I929 1931
Adult Adult 1922 I934 1940 I944 1948 I947 I947 1950
1947 1950 1953 I955 I957 1951
I953 I944 I955
__-
I956
Ige at death Y - 4 c living
(1)
1 50 49 1 1 1
2
1
1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
1 1 1
3
cause of death
Hietory of urinary tract abnormality
None None None
None None
-
-
None
None None None
-
- -
None None None None None None None None None None None None None None Recurrent urin
None None None
ary calouli
urine ox&l&te
ox&late/
(mg./mg.)
crerttinine ratio
0'003 - - -
0'012 0.005 -
om08
0.006 0.006
-
- - - -
0'010
0.023 0.028 0'01 I
0'012 0'014 0.026 -
0'01 I 0'027 - - -
0.326- 0.48 I - - -
* Propositus.

E. F. SCOWEN, R. W. E. WATTS AND E. G. HALL 38 1
are cases of primary hyperoxaluria, although no urinary oxalate determinations were performed; and, on the available evidence, the mode of inheritance in this family appears to be recessive.
We had previously noted, in reviewing the literature (Archer et al. 1958), that reports of male cases of primary hyperoxaluria appeared to predominate, a survey of the eight families which have now been reported from our laboratories suggests that the sex incidence of the disease is in fact approximately equal.
Five previously unreported families in which cases of primary hyperoxaluria have occurred have been investigated to determine whether an hereditary pattern is apparent in this disease. The occurrence of the condition in sibs in the absence of any detectable abnormality in the parents hrts been proved in two of these families, and suggests a recessive mode of inheritance. In one family out of a total of eight which have now been reported from our laboratories the parents of the propositus are first cousins. The sex-incidence of the disease appears to be approximately equal.
SUMMARY
We are indebted to the following surgeons and physicians for permission to study the families of patients under their care: M i P. P. Rickham (families 4 and 6), Miss I. Forshall (family 6 ) , Dr W. Sheldon, C.V.O. (family 7), Dr Mary Wilmers (family 8); and to Dr H. Harris for his continued interest in this investigation. We are also pleased to acknowledge the technical help which we have received from Mr J. T. Ireland, B.Sc., and Mr L. Rawlings.
REFERENCES
ARCHER, H. E., DORMER, A. E., SOOWEN, E. F. & W A ~ S , R. W. E. (1957). Primary hyperoxaluria. k m t ,
ARC=, H. E., DORWER, A. E., SCOWEN, E. F. & WATTS, R. W. E. (1958). Observations on the possible
( 5 I a m D , H. & SODERHJELM, L. (1957). Familial oxalosis. AGta SOC. Med. UpaalierrSia, 62, 176. SCOWEN, E. F., &AWECALL, J. C. & WATTS, R. W. E. (1958). Incorporation of carboxyl-carbon atom of
glycine into oxalate in a case of primary hyperoxaluria. Lancet, ii, 300. SCOWEN, E. F., STANSFELD, A. G . & WATTS, R. W. E. (1959). Oxalosis and primary hyperoxaluria. J. Path.
Bact. 77, 195. SHEPARD, T. H. (1958). Personal communication to the authors. SHEPARD, T. H., KREBS, E. G. & LEE, L. S. (1958). Studies on familial oxa~osis. Amer. J . D&. Child. %, 490. WATCS, R. W. E., SCOWEN, E. F. & C k u - f i ~ , J. C. (1958). The metabolic lesion in primary hyperoxaluria.
Abatracta of cmmunicatiom to the IVth International Conpeas of Biochemktry. Section 13. Communica- tion number 27.
ii, 320.
genetic basis of primary hyperoxaluria. Ann. Hum. Genet., Lond., 22, 373.





























