Embed Size (px)
Citation preview

125 West Orchard Street
Itasca, Illinois 60143-1764
Phone: 800-724-7668 Fax: 630-773-2560 E-mail: [email protected]
FSA Claim Reimbursement & Communication Kit
Please read through this carefully as there are many changes to the
FSA Law that could affect how you make your FSA Election or
receive your FSA Reimbursement for the next plan year.
New Software. New Features. New BBP.
Online Claim Entry
Participants can now enter claims directly online into BBP’s system. After entering the claim online you will be able to upload your
claim to be adjudicated.
To enter your claim online log into the BBP system and on the left hand side under ‘My Accounts’ click ‘Reimbursement Request’ and
follow the online instructions.
E-mail Communications
By putting your e-mail into the BBP system you will now automatically receive the following communications:
1. Manual Claim Entered – Sent based on when a claim is submitted
2. Account Balance Statement – Sent Monthly (only available through email)
3. Year End Reminder – Sent 60 days before the end of the plan year
4. Run out Date Reminder – Sent 30 days prior to the last day to submit claims
5. IRS Grace Period Reminder – (Depends on Employer/ check with BBP to see if your employer offers the grace period) – Sent
14 days prior to the start of the grace period
6. Denied Transaction – Sent every time a claim is denied
7. Account Balance Alert – Sent when your account has under $100.00
All these communications are also available to receive by Mobile Phone. Just register through your online BBP account.
Online Participant Portal
BBP has always offered 24/7 online account viewing access. New features to the online account include:
1. Important Announcements
2. Download Document and Forms
3. Change Personal Information
4. Change of Address
5. View Reimbursements
6. View Pending Claims
7. Viewing claims by provider name
8. Viewing claims by employee/dependent name
9. Opt In/Out of communications
10. Sign Up for Text/Mobile Alerts
11. Frequently Asked Questions
12. Direct Deposit Information (if applicable)
Foreign Language Interpretation
If English is not your first language do not worry. BBP has the capability of answering questions in over 150 languages. Please do
not feel that you cannot call BBP to have your question answered. If you are calling and would like someone to speak the language
you are more comfortable speaking just ask BBP for an interpreter.
Mailed Communications
BBP has changed printing vendors and all BBP mailings will be mailed from Dallas, Texas. The address in the BBP system is where all
mailed correspondence will go about your account. BBP sends out 2 mailed statements a year.
Reimbursement Information
BBP or your employer handles reimbursement. Please check online or with BBP for reimbursement information and options.

Keep up-to-date with BBP!
Become a Friend on Facebook – https://www.facebook.com/BetterBusinessPlanning
Follow us on Twitter – https://twitter.com/BBP_Inc
BBP is available for your convenience Monday – Friday from 8:30am – 5:00pm (CST)
Contact BBP:
Phone: 800-724-7668
Fax: 630-773-2560
Email: [email protected]
Instant Mesenger: www.bbp-dac.comwww
Physical Address: 125 West Orchard Street, Itasca, IL 60143
Healthcare Flexible Spending Account Participation Guidelines
A healthcare Flexible Spending Account (FSA) is a reimbursement account offered by your employer as part of your benefits package.
Participating in the FSA plan saves you money by allowing you to use pre-tax dollars to pay for qualifying expenses not covered by insurance.
Participation is voluntary, and you must satisfy any healthcare FSA eligibility requirements established by your employer in order to participate.
• Only eligible expenses can be reimbursed under the plan. Eligible expenses are defined by Internal Revenue Code 213(d) and your
employer’s plan.
• Expenses must be incurred by you, your spouse, or your eligible dependent(s) during the current plan year and while you are an active
participant in the plan. Medical expenses are incurred when you (or your spouse or dependents) are provided with the medical care that
gives rise to the medical expenses, and not when you are formally billed, charged for, or pay for the medical care.
• Only “out-of-pocket” expenses are eligible for reimbursement. Expenses previously reimbursed by your healthcare FSA or covered by any
other plan or program are not eligible for reimbursement.
• Generally, eligible expenses include items that are meant to diagnose, cure, mitigate or treat illness or disease.
• Expenses such as cosmetic surgery, insurance premiums, vitamins or items for your general well-being are not eligible for
reimbursement.
• A comprehensive list (FSA Eligible Expenses) of eligible expenses, including certain over-the-counter items, can be found in the ‘Forms’
dropdown list at www.bbp-dac.com.
• Expenses reimbursed under the healthcare FSA may not be used to claim any federal income tax deduction or credit.
• Minimum (if any) and maximum election amounts are determined by your employer.
• Your election is irrevocable during the plan year unless you experience a qualifying change in status event. Rules regarding status changes
and other qualifying events are defined by IRS regulations. Not all plans recognize all of the permissible changes. For more information
regarding eligible status change events under your plan, please review your Summary Plan Description.
• Your contributions are subject to the “use-it-or-lose-it” rule. Any unused contributions are forfeited to the plan at the end of the plan
year.
• Your annual healthcare FSA election amount is available to you at any time during the plan year.
• All requests for reimbursement are subject to review and approval based on IRS guidelines. If your request is denied, you will receive an
explanation from BBP including the reason for the denial.
• If you elect to participate in the plan, your employer will provide a Summary Plan Description outlining the complete rules and
regulations of your plan.
This document provides basic information regarding participation in your employer’s FSA plan. This document does not contain all of the
rules governing your employer’s plan. For complete rules and plan information, please review the plan’s Summary Plan Description.
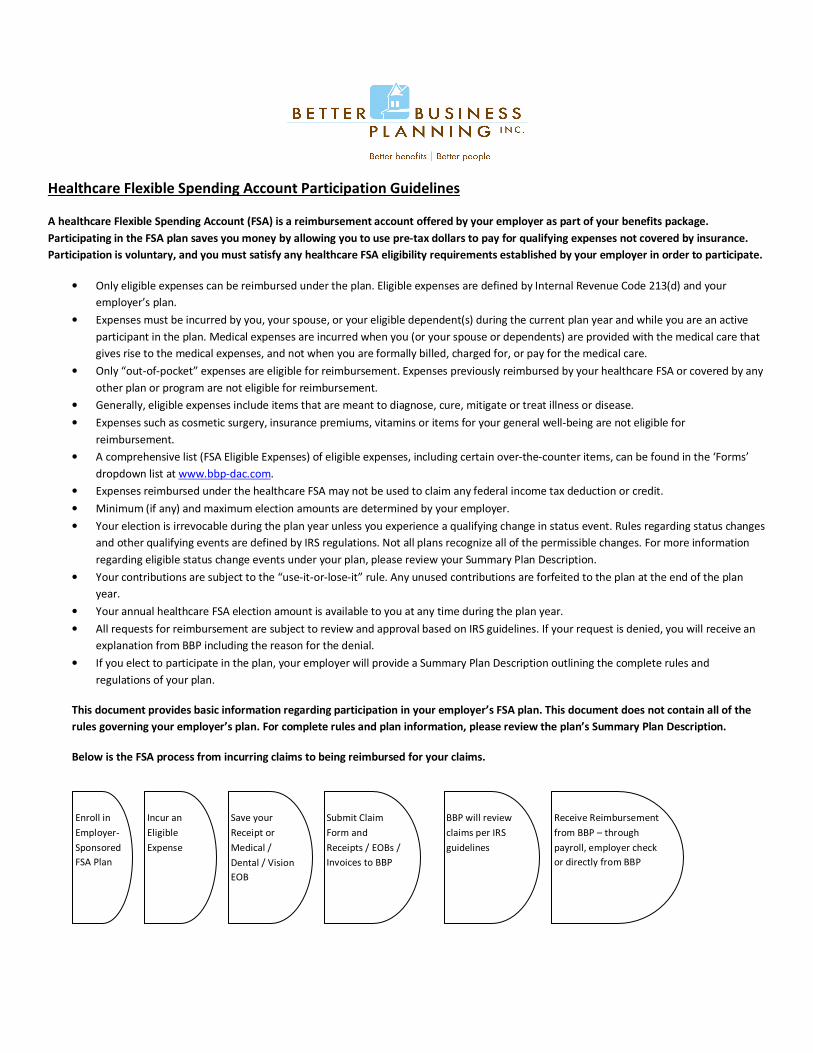
Below is the FSA process from incurring claims to being reimbursed for your claims.
Enroll in
Employer-
Sponsored
FSA Plan
Save your
Receipt or
Medical /
Dental / Vision
EOB
Incur an
Eligible
Expense
Submit Claim
Form and
Receipts / EOBs /
Invoices to BBP
BBP will review
claims per IRS
guidelines
Receive Reimbursement
from BBP – through
payroll, employer check
or directly from BBP

Dependent Care Flexible Spending Account Participation Guidelines
A dependent care Flexible Spending Account (DCAP) is a reimbursement account offered by your employer as part of your benefits package.
Participating in the DCAP plan saves you money by allowing you to use pre-tax dollars to pay for qualifying expenses such as day care or before
and/or after school care. Participation is voluntary, and you must satisfy any dependent care FSA eligibility requirements established by your
employer in order to participate.
• Only eligible expenses can be reimbursed under the plan. Dependent care expenses must be incurred to enable you (and your spouse, if
married) to work, look for work or attend school full time during the plan year. Work may include actively looking for work, but does not
include unpaid volunteer work. Expenses must be incurred during the plan year.
• Any incurred expenses must be for the care of a qualified individual. A qualified individual is a child age 12 and under or a spouse or other
tax dependent who is physically or mentally incapable of self-care. The individual must also reside in the same household for more than
half of the year.
• Per IRS regulations, a child is a qualified dependent of the “custodial parent.” Therefore, only the custodial parent may participate in a
dependent care FSA.
• Expenses reimbursed under the dependent care FSA may not be used to claim any federal income tax deduction or credit.
• Expenses related to before and after school care or nursery school are eligible expenses, if the care is primarily custodial in nature.
• Fees associated with kindergarten as well as tuition for school programs are not eligible for reimbursement.
• All requests for reimbursement are subject to review and approval based on IRS guidelines. If your request is denied, you will receive an
explanation from BBP including the reason for the denial.
• The minimum election amount (if any) is determined by your employer. The pre-defined maximum election amount is $5,000 per IRS
regulations ($2,500 if married and filing separately). The amount of reimbursement that you receive on a tax-free basis during the plan
year cannot exceed the lesser of your earned income or your spouse’s earned income.
• Your election is irrevocable during the plan year unless you experience a qualifying change in status event or the cost of care increases or
decreases significantly. Rules regarding status changes and other qualifying events are defined by IRS regulations. Not all plans recognize
all of the permissible changes. For more information regarding eligible status change events under your plan, please review you Summary
Plan Description.
• Your contributions are subject to the “use-it-or-lose-it” rule. Any unused contributions are forfeited to the plan at the end of the plan
year.
• Dependent care FSA reimbursements are issued as contributions (payroll deductions) are posted to your account.
• If you elect to participate in the plan, your employer will provide a Summary Plan Description outlining the complete rules and
regulations of your plan.
This document provides basic information regarding participation in your employer’s FSA plan. This document does not contain all of the
rules governing your employer’s plan. For complete rules and plan information, please review the plan’s Summary Plan Description.
Below is the DCAP process from incurring claims to being reimbursed for your claims.
Enroll in
Employer-
Sponsored
DCAP Plan
Save your
Receipt or
Invoice
Incur an
Eligible
Expense
Submit Claim
Form and
Receipts /
Invoices to BBP
BBP will review
claims per IRS
guidelines
Receive Reimbursement
from BBP as funds
become available –
through payroll,
employer check or
directly from BBP
Instructions
1) You MUST complete the Enrollment Form to be able to participate in your Employer Sponsored FSA Benefit Plan.
2) Complete the Claim Form in its entirety when submitting a claim(s). Please ensure your supporting documentation clearly indicates the
requested amount. BBP Claim Forms can be found online upon logging into your Participant Portal at www.mybenefitfunds.com/dac
under the ‘My Accounts’ drop down menu then ‘Forms & Documents’. 3) Attach supporting documentation as described below.
a) Explanation of Benefits (EOB) from your insurance carrier; or
b) Itemized statement or bill from you provider including:
- Provider name
- Patient name
- Description of service
- Original date of service (the date of service, NOT the statement date or date of payment. The service MUST fall within the
plan year for which you are enrolled and while you are a participant in the plan)
- Patient portion of charge(s); or
c) Pharmacy statement including:
- Patient name
- Prescribing physician
- RX number
- Name of the drug
- Date the RX was filled
- Co-payment amount
*Unacceptable Documentation includes the following:
- Cancelled checks
- Credit / cash receipts (An itemized cash register receipt is acceptable ONLY for eligible over-the-counter expenses)
- Balance forward statements are NOT acceptable.
4) Sign and date at the bottom of the claim form
5) Submit Claims to: BBP
By Fax: (630) 773-2560
By Email: [email protected]
By Mail: 125 West Orchard Street
Itasca, Illinois 60143
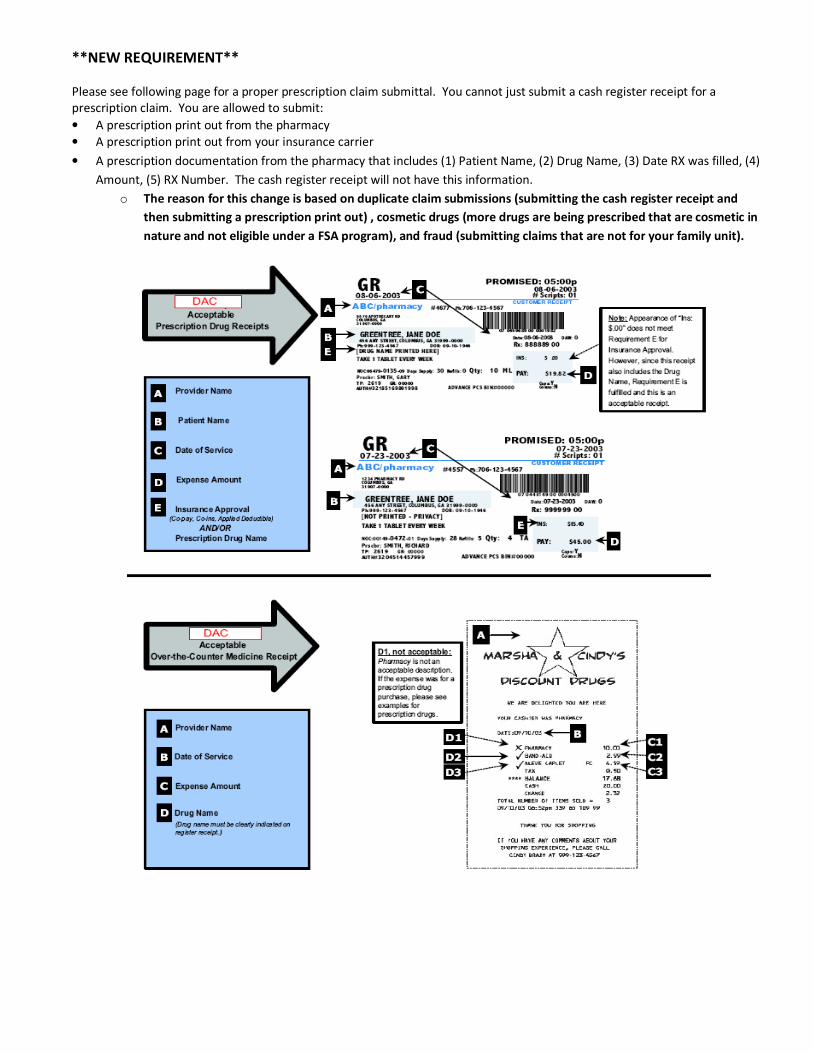
**NEW REQUIREMENT**
Please see following page for a proper prescription claim submittal. You cannot just submit a cash register receipt for a
prescription claim. You are allowed to submit:
• A prescription print out from the pharmacy
• A prescription print out from your insurance carrier
• A prescription documentation from the pharmacy that includes (1) Patient Name, (2) Drug Name, (3) Date RX was filled, (4)
Amount, (5) RX Number. The cash register receipt will not have this information.
o The reason for this change is based on duplicate claim submissions (submitting the cash register receipt and
then submitting a prescription print out) , cosmetic drugs (more drugs are being prescribed that are cosmetic in
nature and not eligible under a FSA program), and fraud (submitting claims that are not for your family unit).

Personal Planning Worksheet
Use this worksheet to estimate expenses for you, your spouse, and eligible dependents. If you participate in your employer’s insurance plan(s),
premiums will automatically be deducted pre-tax, unless you notify your Human Resources Department to do differently.
Health Related Expenses Dependent Care Expenses
Medical co-pays Day-care centers
Deductibles Elder care
Routine physical Family child care
X-Rays Day camps
Dental co-pays Preschool
Dental deductibles After-school care
Non-cosmetic dental services Nanny/au pair
Orthodontia $ Dependent Plan Year Total
Dental Surgery Ineligible dependent expenses include:
Dental x-rays Meals – Overnight camps – diapers – educational
Contact lens & supplies expenses including kindergarten – incidental fees
Laser eye surgery such as activity fees, field trips
Eye glasses Important: You must list your dependent care
Vision x-rays provider’s tax ID number on Form 2441 for your taxes
Vision exams each year. ($5,000 maximum for married and head
Medical miles, paid according to IRS annual Limits of household filers or $2,500 if married filing
Alcoholism treatment separately). Please refer to the Summary Plan
Ambulance Description if your spouse is a student or disabled.
Care for handicapped Also, you and your spouse (if applicable) must both be
Diabetic supplies/insulin gainfully employed to participate.
Acupuncture
Drug addiction treatment
Guide animal care
Eligible hospital charges not covered by insurance
Lab fees
Learning disabilities care
Over-the-counter drugs
Prescription expenses (co-pays)
Prosthesis
Wheelchairs
Holistic healing services (medically necessary), not
including holistic remedies or supplements
$ Health Plan Year Total
Please see the following pages for a list of FSA Medical items.

What Are My Eligible Medical Expenses?
The IRS has defined a list of expenses that you can purchase with your tax-free dollars. A general rule of thumb is that if a doctor deems an item
medically necessary, it is considered an eligible expense. The items on the following list are approved; if you have a question regarding an item that
does not appear on the list, contact BBP, or go to www.bbp-dac.com under the ‘Forms’ dropdown list.
DENTAL SERVICES PRACTITIONERS
Crowns/Bridges Allergist
Dental X-Rays Chiropractor
Dentures Christian Science
Exams/Teeth Cleaning Dermatologist
Extractions Homeopath
Fillings Naturopath
Gum Treatment Osteopath
Oral Surgery Physician
Orthodontia/Braces Psychiatrist
INSURANCE-RELATED ITEMS Psychologist
Co-pay Amounts OTHER MEDICAL TREATMENTS/
Deductibles PROCEDURES
Pre-existing Condition Expenses Acupuncture
Private Hospital Room Differential Alcoholism (inpatient treatment)
LAB EXAMS/TESTS Drug Addiction
Blood Tests Hearing Exams
Cardiographs Hospital Services
Diagnostic Infertility
Laboratory Fees In-vitro Fertilization
Metabolism Tests Norplant Insertion or Removal
Spinal Fluid Tests Patterning Exercises
Urine/Stool Analyses Physical Examination (not employment related)
X-Rays Physical Therapy
MEDICATIONS Pregnancy Tests
Insulin Smoking Cessation Programs
Prescribed Birth Control Speech Therapy
Prescribed Vitamins Sterilization
Prescription Drugs Transplants (includes organ donor)
OBSTETRIC SERVICES Treatment for Handicapped
Mid-Wife Expenses Vaccinations/Immunizations
OB/GYN Exams Vasectomy
OB/GYN Prepaid Maternity Fees Well Baby Care
Post-Natal/Pre-Natal Treatment
Pre-Natal Vitamins
(list continued on next page)

OTHER MEDICAL EQUIPMENT,
SUPPLIES and SERVICES Transportation Expenses
Abdominal/Back Supports (essential to medical care)
Ambulance Services Tuition Fee at Special School for
Arches/Orthopedic Shoes Disabled Child
Contraceptives Wheelchair
Counseling Wigs (hair loss due to disease)
Crutches VISION SERVICES
Guide Dog (for visually/hearing impaired person) Artificial Eyes
Hearing Aids & Batteries Contact Lenses
Hospital Bed Eye Examinations
Learning Disability (special school/teacher) Eyeglasses
Medic Alert Bracelet or Necklace Laser Eye Surgeries
Oxygen Equipment Optometrist / Ophthalmologist
Prosthesis Prescription Sunglasses
Splints/Casts Radial Keratotomy
Syringes
Ineligible Expenses
The following is a list of expenses not eligible for payment with your tax-free FSA dollars. Of course, this list is in no way complete, and is included
as a quick reference regarding commonly questioned expenses.
Baby-sitting & Child Care Insurance Premiums
Breast Pumps* Marriage Counseling
Calcium Supplements Massage Therapy**
Contact Lens Insurance Maternity Clothes
Cosmetic Surgery/Procedures Personal Trainer
Custom Fitovers (clip-ons) Prescription Drug Discount
Diaper Service Retin-A*
Electrolysis Rogaine*
Exercise Equipment* Special Foods*
Eyeglass Insurance Swimming Lessons
Fitness Programs* Tattoo Removal
Hair Loss Medication Teeth Whitening/Bleaching
Hair Transplant Toiletries, Toothpaste, etc.
Health Club Dues Varicose Vein Treatment*
Herbs & Herbal Medicines Vision Discount Program
Homeopathic Drugs Vitamins*
Insurance Premium Interest Weight Loss Programs*
* Eligible only with doctor’s certification identifying the medical condition and length of treatment program.
** Eligible only with doctor’s certification identifying the physical nature of the medical condition and length
of treatment program. Massage therapy for the sole purpose of relief of tension/stress or depression (even
with a doctor’s statement) does not qualify as an eligible expense.

How About Over-the-Counter Drugs? - NEW OTC RULE STARTING 01/01/2011
The IRS also allows over-the-counter drugs (items that can be purchased at your pharmacy without a prescription) as eligible expenses. This ruling
stretches the savings power of your FSA even further allowing you to save money on the routine items your family always keeps on hand, such as
pain relievers, allergy medication, and cold medications.
Eligible Over-the-Counter Expenses • Band-Aids / Bandages
• Saline / Contact Solution
Over-the-Counter Expenses Requiring
Letter of Medical Necessity • Acne treatments
• Allergy medicines
• Antacids
• Anti-diarrhea medicines
• Bactine
• BenGay, Tiger Balm and similar products for muscle or joint pain
• Bug bite medications
• Calamine lotion
• Cold medicines
• Cough drops, throat lozenges
• Dietary supplements or medicines to treat a specific condition
• Fiber supplements to treat a specific medical condition for a
limited time
• First aid creams
• Glucosamine/chondroitin for arthritis or other medical conditions
• Lactose intolerance pills
• Laxatives
• Menopause treatments for hot flashes or night sweats
• Menstrual cycle products for pain and cramp relief
• Motion sickness pills
• Nasal sinus sprays
• Nasal sprays for snoring
• OTC hormone therapy
• Pain relievers
• Pedialyte for ill child’s dehydration
• Prenatal vitamins
• Sleeping aids
• Special diaper rash ointments
• Special ointments for sunburn
• Sunscreens – must be SPF 30 or higher
• Suppositories and creams for hemorrhoids
• Sinus medications
• St. John’s wort for depression
• Visine and other such eye products
• Wart remover treatments
• Weight-loss drugs to treat obesity
Ineligible Over-the-Counter Expenses
• Chapstick
• Deodorants
• Eye and facial makeup preparations
• Face creams
• Feminine hygiene products
• Fingernail polishes
• Hair colors
• Hand lotions
• Lipsticks
• Medicated shampoos
• Medicated soaps
• Perfumes
• Permanent waves
• Shaving creams
• Shaving lotions
• Skin moisturizers
• Suntan lotions
• Toothpaste
• Vitamins

Employer Name: ______________________________________________________________
20___ MILEAGE REIMBURSEMENT REQUEST FORM Employee Name: __________________________________________________________________________
Daytime Phone # or E-Mail Address: __________________________________________________________
□Please check this box if your address on file with BBP has changed. New Home Address________________________________
This worksheet will help you expense your mileage traveled to and from your house for eligible medical expenses. *Mileage Reimbursement Rates – Please see current rate under the announcement tab
Mileage Report - Account for miles traveled to and from medical visits.
Date Destination
(Hospital, Clinic,
etc.)
Beginning
Mileage
Ending Mileage Total Mileage
Traveled (Ending
– Beginning)
Amount
Reimbursed
Total Amount Claimed for this Claim Form - $____________________________
Please submit proof of medical visit with every claim for mileage above. Also, submit driving directions from your house to
medical provider through an online map service; i.e., MapQuest, Yahoo Maps, Google Maps, etc.
PLEASE READ CAREFULLY
Participant’s Statement & Signature
I, the undersigned participant in the Plan, certify that all expenses for which reimbursement or payment is requested by
submission of this form were incurred during a period while I was covered under the Company’s Flexible Spending Account Plan with
respect to such expenses and that the mileage expenses, if applicable, have not been or are not reimbursable under any other plan.
I, the undersigned, certify that a federally recognized dependent or I incurred these expenses and the expenses are eligible under
federal law.
I fully understand that I alone am responsible for the sufficiency, accuracy, and truthfulness of all information relating to
this request and that unless an expense for which payment or reimbursement is requested is an eligible expense under the plan
and IRS law, I may be liable for payment of all related taxes including federal, state, and/or city income tax and penalties on
amounts paid from the plan which relate to the taxation of ineligible expenses.
A copy or electronic copy of this form and all supporting documentation shall be deemed as valid as the original.
X________________________________________________________ _______________________ Plan Participant’s Signature (You must sign this form to be reimbursed.) DATE
Mail, Fax, or Email Completed Form to:
125 West Orchard Street - Itasca, Illinois 60143-1764
Phone (800)724-7668– Fax (630)773-2560 – E-mail [email protected]
Employer Name: ______________________________________________________________
20___ DCAP REIMBURSEMENT REQUEST FORM Employee Name: __________________________________________________________________________
Daytime Phone # or E-Mail Address: __________________________________________________________
Please check this box if your address on file with BBP has changed. New Home Address________________________________
Instructions: Complete the information below for Dependent Care Expenses incurred by you or your Spouse for which you request
reimbursement. (For information as to what Dependent Care Expenses can be reimbursed, see the Salary Reduction Plan Summary Plan
Description.) You must provide bills, receipts, or other evidence from your dependent care provider or other evidence that the Expenses
were incurred (no canceled checks). Be sure to provide all information requested by this Form. If the Form is incomplete, it will be
returned to you. Please date and sign the Form then send it along with your supporting documentation to BBP at Support@bbp-
dac.com or 630-773-2560 or 125 West Orchard St. – Itasca, IL, 60143-1764. Example Expense #1 Expense #2 Expense #3 Expense #4
Date(s) dependent care service was actually provided
03/01/2011 to 03/31/2011
__________ to __________
__________ to __________
__________ to __________
__________ to __________
Name & age of dependent Fred Jones Age 4
Name, Employer Identification Number (Social Security number for an individual), and address of service provider
Sue Smith 376-13-7753 123 Day St. Chicago, IL 60606
Proof of expense attached? X YES □ NO
Reimbursement requested $250
□ This is a recurring clam for the current plan year – please enter for the entire plan year. If my recurring charge changes, I will notify BBP.
TOTAL REIMBURSEMENT REQUESTED $______________________________
I authorize the above expenses to be reimbursed from my DCAP Account. To the best of my knowledge, my statements in this form are true and
complete. I certify all of the following: My family member has received the services described above on the dates indicated, and the expenses
qualify as valid Dependent Care Expenses as defined in the Salary Reduction Plan document ("the Plan"). The expenses listed are for a Qualifying
Individual as defined in the Plan. These expenses have not previously been reimbursed under the DCAP or any other plan, and I will not seek
reimbursement for them under insurance or any other plan. I understand that the expenses reimbursed may not be used to claim any federal
income tax deduction or credit (such as the Dependent Care Tax Credit). I agree to file IRS Form 2441 with my tax return and provide any required
taxpayer identification numbers. I also understand that any reimbursement I receive for these expenses cannot be excluded from my income to
the extent that the reimbursement, when added to excludable reimbursements to date for Dependent Care Expenses incurred during the same
calendar year (from any plan), exceeds the statutory limits described in the Salary Reduction Summary Plan Description. I have read, understand,
and make the certifications contained in the Certificate of Qualifying Dependent Care Expenses on the reverse side of this Form.
Employee Signature:___________________________________________________________ Date:__________________________
Claim Confirmation: You can easily view your claim status 24 hours a day by checking BBP’s website at www.bbp-dac.com. If you choose to fax your claim, PLEASE DO
NOT MAIL THE SAME CLAIM. Keep the fax confirmation for your records. If faxed, allow 24 hours before checking the website or calling for the status of your claim.

20___ PLAN YEAR - FSA CLAIM FORM FAX FORM to (630) 773-2560 - Number of pages including this claim form:
Employer Name: _________________________________________________
Employee Name: _________________________________________________ Daytime Phone #: _________________________________________________
E-mail address: _________________________________________________ (Provide a phone number or e-mail address in case there is a problem with your claim)
□ Please check this box if your address on file with BBP has changed.
New Home Address: _______________________________________________________________________________ PAYMENT OR REIMBURSEMENT OF HEALTH CARE FLEXIBLE SPENDING ACCOUNT AND/OR DEPENDENT CARE FLEXIBLE SPENDING ACCOUNT
CLAIMS ARE SUBJECT TO THE PROVISIONS OF YOUR EMPLOYER’S PLAN DOCUMENTS AND APPLICABLE LAWS AND REGULATIONS
□ Please check this box if you participate in a Health Savings Account or Health Reimbursement Account.
(Please note you cannot be double reimbursed)
HEALTH CARE FSA All FSA claims must be submitted with documentation that verifies the following: (1) Name of Patient, (2) Name of Provider, (3) Expense Incurred (See Expense Code Types), (4) Date of Incurred Expense AND NOT DATE CLAIM IS PAID, and amount of the expense. If the request is for an over-the-counter drug, YOU MUST INDICATE THE NAME OF THE DRUG AND ITS PURPOSE TO TREAT THE PATIENT. All claims for over-the-counter drugs need a receipt attached to the form indicating the date of purchase, name or description of item purchased, the amount of the expense, and the item circled on the receipt if purchased with other item not eligible for reimbursement. If you have insurance and a claim is being administered please attach a copy of the Explanation of Benefits (EOB) form to this claim form with all of the supporting documentation.
Person Receiving Service
Relationship to Plan Participant
Provider of Service
Expense Type Code *
If OTC – Purpose to treat patient
Date Expense Incurred
Amount Paid by Any Insurance Plan
Reimbursement Request Amount
DO NOT COMPLETE IF YOUR RECEIPTS ALREADY CONTAIN THIS INFORMATION – SIMPLY PUT DOLLAR AMOUNT BELOW AND SIGN FORM
$ $
$ $
$ $
$ $
$ $
$ $
$ $
TOTAL HEALTH CARE FSA EXPENSE REQUEST (this page only, use as many forms as needed): $_______________________ Please keep your originals and either e-mail, fax, or mail copies of your bills or receipts for the health care expenses included on this form. *Expense Type Codes: D = Dental H = Hearing HC = Health Care MH = Mental Health MS = Medical Supplies OTC = Over-the- Counter Drugs P = Prescription Drugs T = Travel for Health Care V = Vision Participant’s Statement & Signature (PLEASE READ CAREFULLY)
I, the undersigned participant in the Plan, certify that all expenses for which reimbursement or payment is requested by submission of this form were incurred during a period while I was covered under the Company’s Flexible Spending Account Plan with respect to such expenses and that the health care expenses, if applicable, have not been or are not reimbursable under any other health plan coverage. I, the undersigned, certify that a federally recognized dependent or I incurred these expenses and the expenses are eligible under federal law. I fully understand that I alone am responsible for the sufficiency, accuracy, and truthfulness of all information relating to this request and that unless an expense for which payment or reimbursement is requested is an eligible expense under the plan and IRS law, I may be liable for payment of all related taxes including federal, state, and/or city income tax and penalties on amounts paid from the plan which relate to the taxation of ineligible expenses. A copy or electronic copy of this form and all supporting documentation shall be deemed as valid as the original. Furthermore, (1) IMPORTANT: Use TWO Forms if expenses are from different plan years, (2) Requests for the current plan year must be received by the dates specified in your SPD, (3) Please Keep All Originals and either e-mail, fax, or mail copies of bills or receipts for the expenses included on this form together with this form, (4) Listed Over-the-Counter drugs are to treat a medical condition, (5) Please Note: an eligible receipt must include ALL of the following: Provider’s Name, Date of Service, Type of Service, and Cost of Service.
Plan Participant’s Signature: X_________________________________________________________ Date: ____________________ (You must sign this form to be reimbursed):
Claim Confirmation: You can easily view your claim status 24 hours a day by checking BBP’s website at www.bbp-dac.com. If you choose
to fax your claim, PLEASE DO NOT MAIL THE SAME CLAIM. Keep the fax confirmation for your records. If faxed, allow 24 hours before
checking the website or calling for the status of your claim.
Instructions for Completing the FSA Claim Form & HIPAA Statement of Privacy Practices To prevent delays in processing your claim, please complete this form correctly. (1) Name and Address (if changed) – enter your
name and address as it appears on your employer’s payroll records. (2) Daytime Telephone Number – enter number so that BBP can call if there is a problem with your claim. (3) Provider of Service – enter the name of the person or facility that provided the service. (4) Person Receiving Service – enter your name, or if
your spouse or dependent child, his or her name. (5) Birth Date – IRS required if submitting Dependent Care FSA. (6) Relationship – enter the dependent’s relationship to you: for example, your daughter, son, or spouse. (7) Date Expense Incurred – enter the date the expense was incurred, not the date it was paid. For Medical Supplies and Over-the-Counter (OTC) Medicines and Drugs, the incurred date may be the date the expense was paid. (7) Expense Type – enter the code as listed on the front for expense type. (8) Reimbursement Request Amount – enter the amount of the incurred expense that is eligible for reimbursement. (9) Total Reimbursement Requested – add the amounts of reimbursement requested and enter the total. (10) Signature and Date – sign and date the form. (11)
Documentation Required – YOU must attach copies of the required documentation to receive reimbursement. For Health, Dental, or Vision Care Expenses – attach a copy of the Explanation of Benefits “EOB” form, denial letter or other documentation you received from the insurance company(ies) or the provider of service, if insurance is not involved. The documentation must include the name of the provider, the name of the person receiving service, the type of service, the incurred date and the provider’s charge for the service. (NO VISA/MC RECEIPTS OR CANCELLED CHECKS.) For Prescription Drug Expenses – co-payments or full payment, submit a copy of the prescription payment receipt showing the patient name, drug name, date of the prescription was filled, and payment amount. Cash register prescription receipts or charge slips showing the prescription and the amount cannot be accepted, as BBP need to verify the patient name and type of drug.
For OTC Medicine and Drug Claims – The following documentation is required for medicines and drugs that either (a) were available previously only by prescription, such as, Claritin, or (b)are commonly recognized as medicines or drugs, such as antacids, pain relievers, allergy medicines, cold medicines, etc. Documentation for an OTC medicine or drug claim must include – (1) a participant statement indicating whether the medicine or drug was purchased for the employee, spouse, or dependent; AND (2) an adequate receipt that includes the name of the medicine or drug or the medicine or drug category such as antacid,
pain reliever, etc., the date purchase, and amount paid. For OTC Medicine and Drug Claims that could be Dual Purpose – The following documentation is required for medicines and drugs that could be for personal, as well as, medical purposes – (1) a statement from physician that establishes that the individual has a medical condition and that the medicine or drug expense is for a medicine or drug that treats the individual’s medical condition, (2) a participant statement indicating whether the medicine or drug was
purchased for the employee, spouse, or dependent, and (3) an adequate receipt that includes the name of the medicine or drug or the medicine or drug category, such as, antacid, pain reliever, etc., the date of purchase, and the amount paid. An example is vitamins. An individual would need to provide a note from a physician stating that the individual had/has a disease that requires vitamins to prevent or aid in treating this disease. The physician’s note would establish the existence of a medical condition.
Orthodontia – For orthodontia expenses, please submit a copy of the Truth in Lending Statement, orthodontia contract of financial agreement with your initial submission itemizing the treatment period, down payment, monthly payment amounts and the amount covered by insurance, if any. Submit a copy of your monthly payment coupon and/or an itemized receipt each time you request reimbursement for ongoing treatment. Note: The plan cannot reimburse for future service or for the portion of treatment occurring in another plan year. Any additional fees such as x-rays, molds, etc., are reimbursable when incurred. The
banding fee (attaching bracket/bands on teeth) can be paid in full when incurred. Down Payments are reimbursable after they have been made. Please submit an itemized receipt showing all payments.
Claim Appeals – If your claim is denied please consult your company’s summary plan document in order to follow the
procedure on how to appeal the claim.
Please mail, fax, or e-mail completed claim form to the following address:
125 West Orchard Street Itasca, Illinois 60143-1764 Fax: (630) 773-2560 E-Mail: [email protected]
Summary of Privacy Practices This Summary of Privacy Practices summarizes how medical information about you may be used and disclosed by Better Business Planning, Inc., hereinafter “BBP” or others in the administration of your claims, and certain rights that you have under Federal and State Law. For a complete, detailed description of all privacy practices, as well as, your legal rights, please refer to the accompanying Notice of Privacy Practices.
Our Pledge Regarding Medical Information BBP is committed to protecting your personal health information. BBP is required by law to (1) make sure that any medical information that identifies you is kept private; (2) provide you with certain rights with respect to your medical information; (3) give you a notice of our legal duties and privacy practices; and (4) follow all privacy practices and procedures currently in effect.
How We May Use and Disclose Medical Information About You BBP may use and disclose your personal health information without your permission to facilitate your medical treatment, for payment for any medical treatments, and for any other health care operation. BBP will disclose your medical information to employees of your company for plan administration functions; but those employees may not share your information for employment-related purposes. BBP may also use and disclose your personal health information without your permission as allowed or required by law. Otherwise,
BBP must obtain your written authorization for any other use and disclosure of your medical information. BBP cannot retaliate against you if you refuse to sign an authorization or revoke an authorization you had previously given to BBP.
Your Rights Regarding Your Medical Information
You have the right to inspect and copy your medical information to request corrections of your medical information and to obtain an accounting of certain disclosures of your medical information. You also have the right to request that additional restrictions or limitations be placed on the use or disclosure of our medical information, or that communications about
your medical information be made in different ways or at different locations. How to File Complaints
If you believe your privacy rights have been violated, you have the right to file a complaint with BBP or with the Office of Civil Rights. BBP will not retaliate against you for making a
complaint.
Questions or Submitting a Claim for Reimbursement? Contact BBP using one of these convenient methods.
Visit: www.bbp-dac.com Fax: (630)773-2560 E-mail: [email protected] Call: (800)724‐7668, Monday - Friday, 8:30 am to 5:00 pm (CST)
Letter of Medical Necessity
Please include this letter of medical necessity in order to be reimbursed for Medical
claims that have been deemed ineligible by the IRS, such as certain OTC items, vitamins or gym memberships. This signed letter will only be valid for the current plan year. Employee Name__________________________________________________________________
Employer_________________________________________________________________________
Email or phone number______________________________________________________________ Physician Signature:______________________________________ Date: _____________________ Printed Physician Name: __________________________________ Phone Number:________________
Address: _______________________________________________________________________________
Better Business Planning, Inc.
125 West Orchard Street
Itasca, Illinois 60143-1764
Phone: 800‐‐‐‐724‐‐‐‐7668 Fax: 630-773-2560 email: [email protected]
To be completed by your physician
Describe the diagnosed condition to be treated: ____________________________________________________________________________________________________________________________________________________________________ Describe the recommended treatment: __________________________________________________________________________________ _________________________________________________________________________________
Indicate the duration of the treatment: __________________________________________________________________________________ Please read the following and sign & date: This treatment is medically necessary to treat the medical condition(s) listed above. The treatment listed is not for general health purposes, not to improve the patient’s appearance or for cosmetic services.





























