Embed Size (px)
Citation preview

Frequency of Hereditary Nonpolyposis Colorectal Cancer A Prospective Multicenter Study in Finland Jukka-Pekka Mecklin, M.D.,* Heikki J. J~irvinen, M.D.,t Antti Hakkiluoto, M.D.,:~ Hannu Hallikas, M.D.,~ Kari-Matti Hiltunen, M.D., H Niilo H~irk6nen, M.D.,q[ Ilmo Kellokumpu, M.D.,# Seppo Laitinen, M.D.,** Jari Ovaska, M.D.,-H- Jukka Tulikoura, M.D.,#, Erkki Valkamo, M.D.,~ From the Surgical Departments of*Jyvdskyld Central Hospital, Jyv~skyld, Finland, t Second Department of Surgery, Helsinki University Hospital, Helsinki, Finland, tSatakunta Central Hospital, Pori, Finland, ~South- Karelia Central Hospital, Lappeenranta, Finland, II Tampere University Hospital, Tampere, Finland, 7[Mikkeli Central Hospital, Mikkeli, Finland, #Fourth Department of Surgery, Helsinki University Hospital, Helsinki, Finland, **Oulu University Hospital, Oulu, Finland, tt Turku University Hospital, Turku, Finland, *tKotka Central Hospital, Kotka, Finland, and ~Savonlinna Central Hospital, Savonlinna, Finland
PURPOSE: Hereditary nonpolyposis colorectal cancer (HNPCC) is an autosomal dominant cancer syndrome char- acterized by early onset of colorectal carcinomas (CRC). Recently, two HNPCC genes have been mapped and cloned, one in the short arm of chromosome 2 and another in the short arm of chromosome 3. There has been a major controversy about the frequency of HNPCC. The few esti- mates available have been based on series selected by age or series representing local area. The purpose of the present study was to design a nonselected, prospective, multicenter study, taking into account the family background and other risk factors of CRC. METHODS: The proportion of HNPCC of all (N = 406) CRC cases was evaluated in a prospective multicenter study. Family history and other risk factors were investigated over a 12-month period for all new CRC patients in ten hospitals. These cases constituted 23 percent of all CRCs diagnosed in Finland dut~g the study period. RESULTS: Three (0.7 percent) cases of verified and seven (1.7 percent) cases of suspected HNPCC were identified, following the evaluation of all families with features indic- ative of susceptibility to cancer. The proportion of identifi- able risk factors of CRC was 5.8-7.5 percent CHNPCC, 0.7-2.4 percent; previous CRC, 3.4 percent; ulcerative co- litis, 1.0 percent; familial adenomatous polyposis coli, 0.7 percent). CONCLUSION. This prospective multicenter study revealed that the frequency of hereditary colorectal cancer is lower than in some previous studies, when diag- nosis is based on extensive pedigree analysis. This result with recent findings of common ancestral founding muta- tion in Finnish HNPCC families indicates that there may be geographic differences in the occurrence of HNPCC. How- ever, this does not change the fact that identification of HNPCC--perhaps one of the most common inherited dis- eases identified in humans--has become a question of vital importance now when diagnosis of the syndrome and large- scale screening of gene carriers using specific tests are on the horizon. [Key words: Hereditary cancer; Hereditary colorectal cancer; Hereditary colon cancer, frequency]
Supported by grants from the Finnish Cancer Society-, the Finnish Foundation for Gastroenterological Research, the Sigrid Juselius Foundation, and the Academy of Finland, Helsinki, Finland. No reprints are available.
Mecklin J-P, Jhrvinen HJ, Hakkiluoto A, Hallikas H, Hilmnen K-M, H~irk6nen N, Kellokumpu I, Laitinen S, Ovaska J, Tu- likoura J, Valkamo E. Frequency of hereditary nonpolyposis colorectal cancer: a prospective multicenter study in Fin- land. Dis Colon Rectum 1995;38:588-593.
H ereditary nonpolypos i s colorectal cancer
(HNPCC) is an autosomal dominan t cancer syn-
drome characterized by early onset of colorectal car-
c inomas (CRC), proximal tumor excess, high risk of
me tachronous disease, and excess of other cancers
(especially endometrial , gastric, uroepithelial, and bil-
iopancreatic tumors) in kindred. 1-3 HNPPC has also
b e e n referred to as the Lynch syndrome 4 or as cancer
family syndrome. 5 Identification of HNPCC has great
practical impor tance both in relation to adapt ing
methods of treating affected gene carriers to the life-
long risk of metachronous mal ignancies and because
asymptomatic high-risk family member s are ideal sub-
jects for cancer screening.
Estimates of the propor t ion of HNPCC of all CRC
patients vary b e t w e e n I and 10 percent. Most apprais-
als indicate a propor t ion of 2 and 5 percent of all
CRCs. However, there have b e e n few studies in this
field. Most of these are retrospective and based on
series from one insti tution < 7 or on series selected by
age. 8'9 Two popu la t ion -based s t u d i e s - - o n e retro-
spective and one p rospec t ive - -have b e e n publ ished,
both of which represent areas with about 0.25 mil l ion
inhabitants.10, 11 Genetic l inkage to loci on chromo-
somes 2p a nd 3p was recently demons t ra ted in
HNPCC families, ~2'13 and the respective genes,
hMSH2 and hMLH1, were later c l one dJ 4-17
The purpose of the present study was to design a
588

Vol. 38, No. 6
nonselected, prospective, multicenter study, taking into account family background and other risk factors of CRC. The situation in Finland is favorable to this kind of study. The population (5 million) is ethnically homogenous, and the country has been divided into hospital districts with a population-based responsibil- ity for health care. Nationwide and complete registers for death certificates and cancer patients enable reli- able verification of cancer cases. In the present study family history and other risk factors of all new CRC patients were studied during a 12-month period in six district hospitals and in four university hospitals lo- cated in different parts of the country. Patients com- prised 23 percent of all CRCs diagnosed in Finland during the study period.
METHODS
S t u d y Protocol
Over a 12-month period (September 1, 1990 to Au- gust 31, 1991) a local surgeon belonging to the study group interviewed all patients with new primary ad- enocarcinoma of the colon or rectum. A one-page questionnaire was filled in. Known risk conditions of CRC (ulcerative colitis, familial adenomatous polypo- sis, and previous malignancies) were evaluated for the proband. Occurrence of malignancies in first-de- gree and second-degree relatives was elicited by in- terviewing the patient. Questionnaire and copies of the hospital records were sent to the responsible in- vestigator (J-P. M.), who analyzed the material and took charge of obtaining any further records and genealogic data required. Altogether, 406 new colo- rectal cancer patients were included in the study.
Classification of Family History
Families were divided into three categories accord- ing to cancer status among family members: 1) neg- ative family history, 2) positive family history, and 3) patients with ulcerative colitis or familial adenoma- tous polyposis coli (FAP). 1) Negative family history group (375 probands; 92.4 percent) comprised fami- lies with no family members affected by cancer and families with one or two first-degree/second-degree family members with malignancies of any type, al- though age of patients and/or tumor spectrum was not indicative of any inherited cancer syndrome. In- formation contained in response to questionnaires was supplemented only occasionally.
2) Positive family history group (24 probands; 5.9
FREQUENCY OF HEREDITARY COLON CANCER 589
percent) included families with three or more first- degree relatives with a malignancy or families with features--such as early onset, multiple metachronous tumors, or a typical tumor spectrum--indicative of hereditary cancer syndrome in first-degree and/or second-degree relatives. In this group, family history and verification of cancer were completed by obtain- ing documents when available. In total, 126 family members with malignancy (mean, 5.3 per family) were identified by questionnaire in these 24 families. Only one-half of these cases could be verified by documents. However, in verified or suspected HNPCC families and in families with a middle-aged (under 50-60 years of age) proband, documents could be obtained in almost all cases. 3) The third group comprised seven (1.7 percenO probands with UC or FAP, all of whom had clinical and histologic documentation of their disease.
Criteria for HNPCC
A family meeting the Amsterdam criteria 5 was con- sidered a HNPCC family. Families with a dominant cancer trait and features indicative of HNPCC but not meeting the Amsterdam criteria were considered sus- pected or putative HNPCC families.
I n c i d e n c e of Colorectal Cancer in F i n l a n d
CRC is the third most common malignancy in Fin- land after carcinoma of the breast and lung. Finland is a low-incidence area for CRC, even though the total number of cases is strongly on the increase because of the aging population. In 1988, the age-specific inci- dence of CRC in Finland (males 18, females 15.5/10 • 105 ) was, for example, one-half that in Denmark (males 35.9, females 29.3/10 • 105). 18
Reg i s t e r s U s e d
Parish Registers. A very exact and reliable popula- tion register has been kept in local parishes in Finland since the 1600s. In addition to general biographic data, these registers also file the cause of death for each parish member. This information, originally based on diagnoses by clergy, became more reliable after 1936 when a medical death certificate became mandatory throughout the country.
Register of the Cause of Death. Since 1936, all death certificates have been preserved in the Central Statis- tical Office of Finland and are available for research purposes. The death certificate also includes informa- tion about hospitalization and consulting physicians,

590 MECKLIN
thus enabling hospital records to be obtained when they have been preserved or filed on microfiche.
Finnish Cancer Registry. The Finnish Cancer Reg- istry was established in 1952. Since 1961 reporting of cancers has been compulsory, so that the registration of cancers in Finland is virtually complete. 19 The reg-
ister, which is data-based, is accessed by means of an individual's social security number, which makes it possible to check whether that person has had a
malignancy during the last 30 to 40 years.
Patients
Reliable data on status of first-degree relatives was obtained by interview for all 406 patients with new, primary CRC treated during the study period in the ten participating hospitals. According to statistics of the
Finnish Cancer Register, the number of new CRCs in Finland in 1990 was 1,738. Thus, our probands rep- resent 23 percent of all CRCs diagnosed in Finland during the study period.
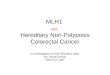
Mean age of patients was 66.6 (range, 29-91) years. Age distribution is shown in Figure 1.
Regional Health Care in Finland
Finland has been divided into 22 health care dis- tricts, each with one central hospital that has respon- sibility for the population in that district. Some addi- tional local hospitals share responsibility for health care in densely populated areas. Five of the central
hospitals are university hospitals, with more extended responsibility in demanding and uncommon health care.
Six of the central hospitals with a mean population
of 165,000 (range, 72,000-250,000) and four of the
N
80 :- ....
: , '~ F e m a l e 7 0 : ~ I . . . . . . . .
6 0
5 0
4 0
3 0
20
10
69
0 0 - 3 9 4 0 - 4 9 5 0 - 5 9 6 0 - 6 9 70 -79 80+
y e a r s
Figure 1. Age and s e x distribution of 406 patients with colorectal cancer.
ETAL Dis Colon Rectum, June 1995
university hospitals situated in different parts of the country participated in the study. Patients (N = 200; 49 percent) in the six central hospitals represent a nonselected, population-based series, whereas pa-
tients (N = 206; 51 percent) in university hospitals are more or less selected.
RESULTS
A negative family history was observed in 375 (92.4 percent) patients. However, two patients in this group
had had multiple metachronous intestinal malignan- cies at a young age without polyposis. A male patient had colonic cancer at ages 28 and 44, and another
male patient had colonic cancer at ages 43 and 63 and synchronous adenocarcinoma of the rectum and jeju-
num at age 67. The remaining 31 patients were di- vided as shown in Table 1. Fourteen (3.4 percent) had three or more first-degree relatives with a malignancy, but family history, tumor spectrum, and/or age distri- bution were not indicative of HNPCC.
In seven (1.7 percent) cases HNPCC could be sus- pected, but the families did not meet the Amsterdam criteria. In three of these, there was no person with CRC diagnosed who was under 50 years of age (so- called late onset family). In two families, a patient
with an extracolonic malignancy (uterus, esophagus) prevented the Amsterdam criteria from being met. In
one small family with two affected members, the proband had had three metachronous malignancies (colon, bilateral breast cancer) before age 50, and her father had died of CRC at the age of 35. In another family, the proband had had two CRCs at age 75 and breast cancer at age 72. Her only son had CRC at age 28. These seven families were considered to be puta- tive HNPCC cases.
In three cases (0.7 percent) the Amsterdam criteria were fulfilled. Two of the families with 6 and 33 affected family members in two and four generations, respectively, were typical HNPCC families according
Table 1. Distribution of Hereditary and Other Risk Conditions in
406 Patients with Colorectal Cancer
Risk Condition No. of Patients (%)
Putative HNPCC 7 (1.7) Verified HNPCC 3 (0.7) Ulcerative colitis 4 (1.0) Familial adenomatosis 3 (0.7)
polyposis Previous colorectal 14 (3.4)
cancer

Vol. 38, No. 6
to age distribution and tumor spectrum. In the third
family, only one of five patients had been under 50
years of age at the time cancer was diagnosed.
A colorectal carcinoma was complicating ulcerative
colitis in four (1.0 percent) patients and familial ad-
enomatous polyposis was found in three (0.7 percent)
patients. A synchronous colorectal neoplasia was ob-
served in 30 (7.4 percent) patients (adenoma(s) in 27,
carcinoma in 3). A previous malignancy was diag-
nosed in 28 (6.9 percent) patients. The most common
metachronous tumors were CRC (14 cases) and en-
dometrial carcinoma (5 cases).
D I S C U S S I O N
This prospective multicenter study gives an esti-
mate of frequency of HNPCC in Finland, which is
lower than our previous estimate based on a retro-
spective analysis in one hospital district. In retrospec-
tive analysis of all CRC patients (N = 468) treated
within a ten-year period (1970-1979) in the province of Central Finland, proportion of verified HNPCC was
3.8 percent and 5.5 percent when putative HNPCC cases were also included. 1~ In the present multicenter
analysis, corresponding figures were 0.7 and 2.4 per-
cent.
The present study is geographically more represen-
tative, and probands comprise 23 percent of all CRCs
diagnosed in Finland during the 12-month period.
The method used to investigate family history and obtain documents was identical in both studies. How-
ever, the study period (12 months) is short and may
predispose to an underestimate caused by chance. In
addition, it is probable that systematic screening for
CRC initiated in 1983 in about 60 Finnish HNPCC
families has prevented the formation of some CRC cases in HNPCC patients. Effectiveness of this screen-
ing has been analyzed in a series of 22 Finnish
HNPCC families, and a remarkable reduction in oc- currence of CRC could be demonstrated because of
polypectomies in screened subjects, z~
Another possible bias, which cannot be excluded in retrospective analysis, is the possibility of local over-
presentation of HNPCC in the province of Central Finland (population, 0.25 million). In fact, a certain
concentration of HNPCC cases in this previous study was observed simply because affected members of two large HNPCC families (Nos. 1 and 2) constituted
6 of 18 definitively diagnosed hereditary cases. 1~ Sub- sequently, it has been possible to demonstrate the
FREQUENCY OF HEREDITARY COLON CANCER 591
presence of a widespread, single ancestral founding
mutation in central and eastern Finland. 21
It is also worth noting that the Amsterdam criteria
had not become available in 1987. Two of 13 families
(15 and 18) did not meet the Amsterdam criteria
because there were no affected family members un-
der 50 years of age. According to present criteria these
families would be classified as putative HNPCC fam-
ilies. Even if these two cases were excluded, the
proportion of cases meeting the Amsterdam criterion
was 3.4 percent of all CRCs. 1~
Ponz de Leon et aL 1~ evaluated family history of
389 consecutive patients with CRC in the Modena
district (population, 0.26 million) in Italy. The authors
found that 15 (3.9 percent) probands had two or more
relatives with CRC. Unfortunately, these families were
not presented or classified in detail, and no age cri-
terion was used. These families have subsequently
been re-evaluated, with the final proportion of iden-
tified HNPCC cases representing 3.4 percent of all G i g s . 22
Westlake et al. s found HNPCC in 3.1 percent of 318
patients with CRC under 50 years of age and listed on
the Alberta Cancer Registry in Canada. Family history
was studied using a questionnaire. However, the pro-
portion of HNPCC was only 0.3 percent of all CRC
cases listed on the cancer registry. Kee and Collins 9 retrospectively investigated all pa-
tients with nonpolyposis CRC under age 55 years
(N = 205) diagnosed within a three-year period in Northern Ireland. The vital status of all first-degree
relatives was established. They found 13 probands
with two or more relatives affected with CRC, i.e., 6
percent of the study patients and 1 percent of all CRC
patients. On the basis of their results, the authors
estimated that the proportion of HNPCC might be
between 1 and 2.6 percent. Stephenson et al. 6 found four (4 percent) cases with
verified or putative HNPCC when family history of 100 patients with apparently sporadic CRC was eval-
uated. Ages of the probands and affected family mem-
bers were not presented. Aaltonen et aL 23 used a novel approach to estimate
the frequency of HNPCC. All CRC patients (N = 227) under 45 years of age diagnosed over a five-year period in Finland comprised the probands. Pedigrees
of the probands were constructed by combining in-
formation from the Finnish Population Register Center and Finnish Cancer Register, using automatically pro-
cessed data. On the basis of their results, the authors

592 MECKLIN
suggested that the proportion of HNPCC of all CRCs
would be between 0.5 and 0.9 percent. The crucial weakness in all studies evaluating prev-
alence of HNPCC has been the fact that a specific
phenotype or biomarker has not been available for identification. In an attempt to standardize publica-
tions in this field, the International Collaborative
Group on HNPCC agreed in 1990 that the Amsterdam
criteria should be used as the minimum criteria for inclusion of HNPCC families in publications. 5 How-
ever, the Amsterdam criteria are not definitive for
HNPCC; rather they are useful tools, ensuring that
families in publications and collaborative studies are
comparable with each other. For practical reasons, it
has been impossible, for example, to include all pos-
sible extracolonic malignancies belonging to the tu-
mor spectrum of HNPCC in the criteria, even though
they might be important in diagnosing the syndrome.
In the present study, the proportion of identifiable
risk factors of CRC was 5.8 to 7.5 percent (HNPCC, 0.7-2.4 percent; previous CRC, 3.4 percent;
ulcerative colitis, 1.0 percent; FAP, 0.7 percent). Pro-
portions of both ulcerative colitis and FAP are over-
estimates because of centralization of these diseases
in university hospitals participating in the study. The
real proportion of cancer caused by ulcerative colitis
might be one-half of the observed 1 percent and of cancer caused by FAP about 0.2 to 0.3 percent when
more than one-half of new FAP cases are now iden-
tified by family screening and treated prophylac- tically. 24
Our study demonstrates that it is difficult to give an
indisputable answer to the question of prevalence of
a cancer syndrome, which cannot be diagnosed until
several family members have been affected. Based on
the present study and previous analysis, it may be
concluded that the proportion of classical HNPCC
diagnosed by family history of all CRCs varies be- tween i and 4 percent in different studies, depending
on study protocol, selection of patients, and criteria
used for hereditary cases. Recently, a HNPCC gene was mapped to the short
arm of chromosome 2 by linkage analysis in two large kindreds 12 and possibly also c lonedJ 4' 15 A second
locus predisposing to HNPCC was found in chromo-
some 3 in two kindreds by Lindblom e t aL, 13 and this has also recently been cloned. 16' 17 Synchronously, an analysis of fresh frozen tumor specimens of HNPCC patients provided evidence for a novel mechanism of carcinogenesis, a tendency to microsatellite instability at multiple random loci throughout the genome. 25
E T A L Dis Colon Rectum, June 1995
This abnormality referred to as the replication error
phenomenon was found in approximately 15 percent
of sporadic CRCs, and it may offer a screening assay
for selection of patients with increased risk of hered- itary cancer. 25-27
Use of specific gene tests or replication error phe-
nomenon would enable more exact est imates--for
example, identification of so-called new muta-
t i o n s - i n the future. However, what is still obscure is
whether the occurrence of HNPCC is equal in all
geographic areas. Recent studies have shown that
there are remarkable differences in the occurrence of
HNPCC, even in a small country such as Finland.
Many apparently unrelated HNPCC families share a common ancestral founding mutation, 21 and cases
with "new mutation" are not as common as expected,
at least in Finland.
However, it is worth noting that even when accept-
ing the lowest estimate (about 1 percent) for the
proportion of HNPCC it would mean, for example, in
the United States more than 1,500 new cases of
HNPCC every year. Therefore, HNPCC, which is pos-
sibly one of the most commonly inherited diseases
identified so far, has great practical importance in
prevention of CRC in younger age groups. 2~ Its sig-
nificance will still increase as the use of specific gene
tests will, within a short time, enable highly targeted
prevention among persons with 100 percent risk of CRC.28, 29
REFERENCES
1. Lynch HT, Kimberling W, Albano WA, et al. Hereditary nonpolyposis colorectal cancer (Lynch syndromes I and II). Cancer 1985;56:934-8.
2. Mecklin J-P, JSlwinen HJ. Tumor spectrum in cancer family syndrome (hereditary nonpolyposis colorectal cancer). Cancer 1991;68:1109-12.
3. Vasen HF, Offerhaus GJ, den Hertog-Jager FC, eta l . The tumour spectrum in hereditary non-polyposis colorectal cancer: a study of 24 kindreds in the Netherlands. Int J Cancer 1990;46:31-4.
4. Lynch HT, Lanspa SJ, Boman BM, et al. Hereditary nonpolyposis colorectal cancer: Lynch syndromes I and II. Gastroenterol Clin North Am 1988;17:679-712.
5. Vasen HF, Mecklin J-P, Meera Khan P, Lynch HT. The International Collaborative Group on Hereditary Non- polyposis Colorectal Cancer (ICG-HNPCC) [Special communication]. Dis Col Rectum 1991;34:424-5.
6. Stephenson B, Finan PJ, Gascoyne J, Garbett F, Murday VA, Bishop DT. Frequency of familial colorectal cancer. Br J Surg 1991;78:1162-6.

Vol. 38, No. 6
7. Houlston RS, Collins A, Slack J, Morton NE. Dominant
genes for colorectal cancer are not rare. Ann Hum
Genet 1992;56:99-103. 8. Westlake PJ, Bryant HE, Huchcroft SA, Sutherland LR.
Frequency of hereditary nonpolyposis colorectal cancer in Southern Alberta. Dig Dis Sci 1991;36:1441-7.
9. Kee F, Collins BJ. How prevalent is cancer family syn-
drome? Gut 1991;32:509-12. 10. Mecklin J-P. Frequency of hereditary nonpolyposis
colorectal carcinoma. Gas t roen te ro logy 1987;93: 1021-5.
11. Ponz de Leon M, Sassatelli R, Sacchetti C, Zanghieri G, Scalmati A, Roncucci L. Familial aggregation of tumors in the three-year experience of a population-based colorectal cancer registry. Cancer Res 1989;49:4344-8.
12. Peltomfiki P, Aaltonen LA, Sistonen P, et al. Genetic mapping of a locus predisposing to human colorectal
cancer. Science 1993;260:810-2. 13. Lindblom A, TannegErd P, Novelius B, NordenskjOld M.
Genetic mapping of a second locus predisposing to hereditary non-polyposis colon cancer. Nat Genet 1993; 5:279-82.
14. Leach FS, Nicolaides NC, Papadopoulos N, et al. Muta- tions of a routS homolog in hereditary nonpolyposis
colorectal cancer. Cell 1993;75:1215-25. 15. Fishel R, Lescoe MK, Rao MR. The human mutator gene
homolog MSH2 and its association with hereditary non- polyposis coiorectal cancer. Cell 1993;75:1027-38.
16. Papadopoulos N, Nicolaides NC, Ying-Fei W, et al.
Mutation of a mutL homolog in hereditary colon cancer.
Science 1994;263:1625-9. 17. Bronner CE, Baker SM, Morrison PT, et al. Mutation in
the DNA mismatch repair gene homologue hMLH1 is associated with hereditary non-polyposis colon cancer.
Nature 1994:368:25841. 18. Moller Jensen O, Carstensen B, Glattre E, Matker B,
Pukkala E, Tulinius H. Atlas of cancer incidence in the Nordic Countries. Helsinki: Nordic Cancer Union, 1988.
19. Hakulinen T, Kenward M, Luostarinen T. Cancer in
FREQUENCY OF HEREDITARY COLON CANCER 593
Finland in 1954-2008. Incidence, mortality and preva-
lence by region. Helsinki: Finnish Foundation for Can-
cer Research, 1989. 20. Jfirvinen HJ, Mecklin J-P, Sistonen P. Screening reduces
colorectal cancer rate in hereditary nonpolyposis colo- rectal cancer (HNPCC) families. Gastroenterology (in press).
21. NystrOm-Lahti M, Sistonen P, Mecklin J-P, et al. Close linkage to chromosome 3p and conservation of ances- tral founding haplotype in hereditary nonpolyposis colorectal cancer families. Proc Natl Acad Sci U S A
1994;91:6054-8. 22. Ponz de Leaon M, Sassatelli R, Benatti P, Roncucci L.
Identification of hereditary nonpolyposis colorectal cancer in the general population. Cancer 1993;71:3493-
501. 23. Aaltonen L, Sankila R, Mecklin J-P, Jfirvinen H, Pelto-
mfiki P, de la Chapelle A. A novel approach to estimate the proportion of hereditary nonpolyposis colorectal cancer of total colorectal cancer burden. Cancer Detect Prev 1994;18:57-63.
24. Jfirvinen HJ. Epidemiology of familial adenomatous pol- yposis in Finland: impact of family screening on the colorectal cancer rate and survival. Gut 1992;33:357-60.
25. Aaltonen LA, Peltomfiki P, Leach FS, et aL Clues to the pathogenesis of familial colorectal cancer. Science 1993;260:812-6.
26. Thibodeau SN, Bren G, Schaid D. Microsatellite insta- bility in cancer of the proximal colon. Science 1993;260:
816-9. 27. Ionov Y, Pernando MA, Malkhosyan S, Shibato D, Pe-
mcho M. Ubiquitous somatic mutations in simple re- peated sequences reveal a new mechanism for colonic carcinogenesis. Nature 1993;363:558-61.
28. Marx J. New colon cancer gene discovered. Science
1993;200:751-2. 29. Steele Y Jr. Accomplishment and promise in the under-
standing and treatment of colorectal cancer. Lancet
1993;342:1092-6.