Embed Size (px)
Citation preview
Journal of Plastic, Reconstructive & Aesthetic Surgery (2007) 60, 583e587
Free anterolateral thigh flap versus free forearmflap: Functional results in oral reconstruction
F. Farace a,*, V.E.E. Fois b, Andrea Manconi a, A. Puddu a, F. Stomeo b,A. Tullio c, F. Meloni d, G. Pisanu b, C. Rubino a
a Plastic SurgeryeBurn Unit Department, University of Sassari, V.le S. Pietro 43/b 07100 Sassari, Italyb ENT Department, University of Sassari, V.le S. Pietro 43/b 07100 Sassari, Italyc Maxillofacial Department, University of Sassari, V.le S. Pietro 43/b 07100 Sassari, Italyd ENT Department, University of Ferrara, Via Savonarola 9, Ferrara, Italy
Received 16 March 2006; accepted 14 November 2006
KEYWORDSFree anterolateralthigh flap;Free radial forearmflap;Functional results inoral reconstruction;Microsurgery in oralcavity
Summary Nowadays, microsurgery performed for oral reconstruction of cancer patients, hasbecome the standard treatment in restoring oral functions. The free radial forearm flap (FRFF)is still apparently the first reconstructive choice in oral cavity cancers. Recently the anterolat-eral thigh flap (ALTF) seemed to challenge the superiority of FRFF. The lack of functional dataon which to base this recent supposition is the reason for this new research. Twenty recon-structed patients were enrolled for this study. Speech, swallowing, and donor site complica-tions were studied to assess differences between the two techniques. Results show thatdifference in function between ALTF and FRFF groups is statistically insignificant. Donor siterisks and complications seem to be the only variables among groups. These variables may beused as indicators when making a surgical choice.ª 2007 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published byElsevier Ltd. All rights reserved.
Surgery remains the main procedure for oral cavity cancertreatment. Immediate reconstruction should be performedafter complete excision of the tumour. The aim ofreconstruction is to maximise oral functions and aestheticswith less morbidity, preserving speech, swallowing andreducing donor site morbidity. The current theories aboutintraoral reconstruction advocate microsurgery as thestandard treatment for restoring oral functions. Even the
* Corresponding author. Tel./fax: þ39 079 228013.E-mail address: [email protected] (F. Farace).
1748-6815/$-seefrontmatterª2007BritishAssociationofPlastic,Reconstrdoi:10.1016/j.bjps.2006.11.014
comparison of direct and indirect costs in oral reconstruc-tion by pedicled and free flaps reveals a modest difference,justifying microsurgery.1
For years, the free radial forearm flap (FRFF) has beenthe first choice to restore soft tissue ablation in oralcavity2e4 despite several disadvantages, such as the sacri-fice of the most important artery of the hand.5 FRFF is stillsupposed to be the first reconstructive choice in oral cavitycancer because of the thickness of the anterolateral thighflap (ALTF), although thickness and volume can be adjustedto the extent of the defect.6,7 Recently, ALTF has chal-lenged the superiority of FRFF. ALTF can be thinned, it
uctiveandAestheticSurgeons.PublishedbyElsevierLtd.All rightsreserved.
584 F. Farace et al.
does not need a skin graft and does not risk damage to ten-dons or hands.8,9 The lack of functional data in the litera-ture about this recent trend prompted the present study.To assess the differences between the two techniques,this paper compares oral cavity function before and aftersoft tissue reconstruction with FRFF and ALTF.
Patients and methods
Twenty patients underwent primary oral cavity reconstruc-tion after intraoral soft tissue ablation, from June 2001 toJune 2005 at the University of Sassari’s Department ofPlastic Surgery. Reconstructions were all performed by thesenior plastic surgeon (CR). The oral cancer excisions wereperformed by an ENT surgical team or by a maxillofacialteam from the same university.
All the patients were afflicted with squamous cellcarcinomas without mandibular involvement (Table 1).Ten patients were reconstructed using a FRFF (group A)and 10 employing an ALTF (group B).
Reconstruction with FRFF was performed from June 2001to March 2003, whereas those with ALTF were performedfrom April 2003 to June 2005.
All the subjects enrolled in this study were evaluated bya phoniatrics specialist and a speech therapist before andafter ablative surgery. Preoperative examination was neces-sary to exclude any functional difficulty. The rehabilitativeteam and the observers were blinded to the type of flap used.The patients started the swallowing and speech rehabilita-tion programme as soon as their clinical condition allowedcorrect receptivity, usually 3 weeks after the reconstruction.The outcome was assessed 6 months after reconstruction andthe rehabilitative team collected data.
Rehabilitative procedure
All the patients were treated by the same rehabilitativeteam. First, generic exercises were administered to obtaincorrect breathing. Then head and neck muscle relaxationexercises were also performed. Then praxis exercises, toimprove lips, tongue, velum palati, and pharynx muscula-ture functioning, were performed. Patients were made todo specific exercises to further improve swallowing (correctposture with head anteriorly flexed, neck extended, andhead flexed on the healthy side), oral competence (diet-
device and manoeuvres to protect airways), and speechintelligibility (TA/KA/CIA pronunciation).
Video fluoroscopic examination
No video fluoroscopic images were recorded due to the lackof an appropriate machine on the island.
Rhinopharyngolaryngoscopy
Employingaflexible rhinopharyngolaryngoscopeandadigitalvideo camera, the second swallowing phase was recorded.This test integrated the clinical swallowing exam (for the firstswallowing phase): oro-pharynx morphological and func-tional examination focusing on pharyngeal tone, mobility,and symmetry during respiration, apnoea, and voluntary/reflex cough.
Both oral transit and pharyngeal transit time weremeasured to identify the amount and location of anyresidue remaining in the oral cavity or pharynx. From videoframes and temporal data, transit time and the amount offood residuals were obtained. This procedure was repeatedafter food administration of different consistencies.
Speech tests
Speech articulation was tested with an Italian, phonemi-cally balanced sentence: ‘Il ramarro della zia’ (the greenlizard of the aunt). All the subjects were asked to read thissentence 6 months from the reconstruction, after rehabil-itative protocol administration.
Global intelligibility was valued by six nonpreparedobservers (four point value scale); articulation was valuedby a speech therapist and an ENT phoniatric specialistemploying diadocohokinesis tests (five point value scale).
Donor site
Donor site morbidity was assessed for each patient.
Statistical methods
Data from intelligibility and swallowing were analysed bytwo tail Fisher’s exact test. Articulation was analysed by c2
trend test.
Table 1 Patients (initials) enrolled for this study
FRFF patients db pg cc va gg fb gd cv gv nm
Age 52 55 64 56 63 46 55 68 51 62TNM T2N0Mx T2N0Mx T2N0Mx T2N0Mx T2N2bMx T3N1Mx T3N1Mx T3N1Mx T3N2bMx T3N2cMx
Tumorectomya hpg hpg hpg hpg hpg hpg hpg þ ap hpg þ ap hpg þ ap hpg þ ap
ALTF patients pa sf fg ss vm df sa rt gt tr
Age 67 48 54 59 61 64 53 60 63 57TNM T2N0Mx T2N0Mx T2N0Mx T2N0Mx T2N0Mx T2N0Mx T2N2bMx T3N2bMx T3N2bMx T3N2bMx
Tumorectomy hpg hpg hpg hpg hpg hpg hpg þ ap hpg þ ap hpg þ ap hpg þ apa hpg, hemipelviglossectomy; ap, anterior pavement ablation.
Free anterolateral thigh flap versus free forearm flap 585
Results
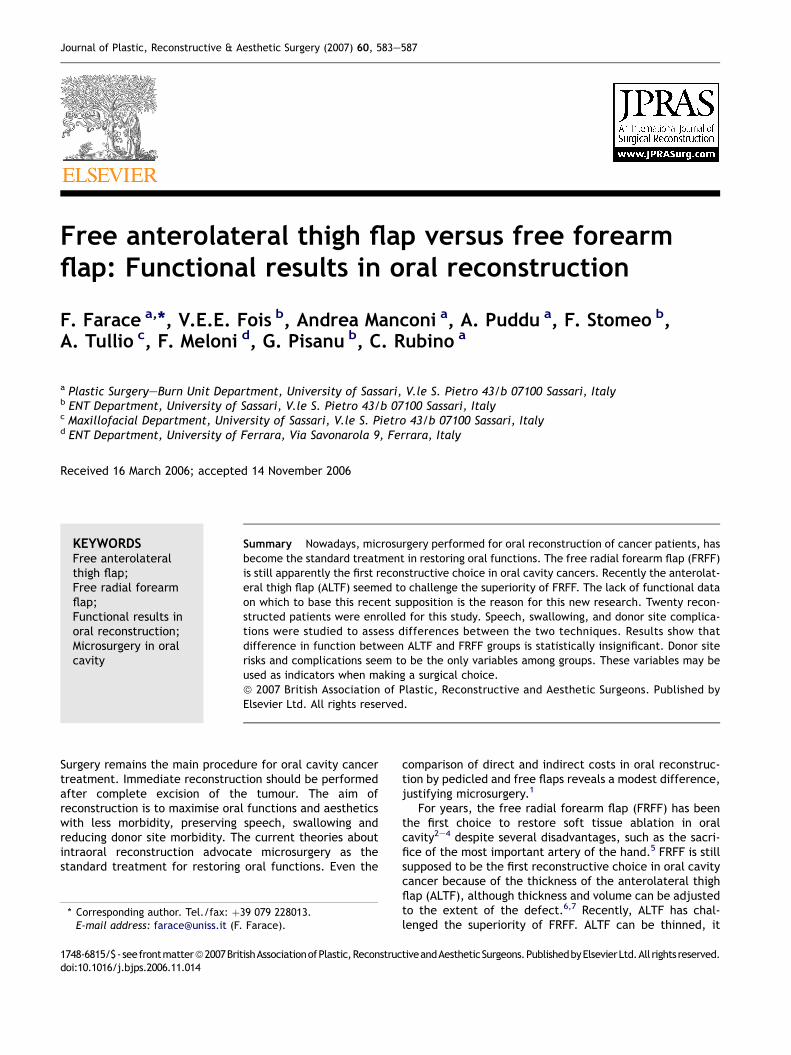
The age of the patients ranged from 46 to 68 years, witha median age of 58 years (Table 1). Table 2 shows speechintelligibility values for patients who underwent FRFF andALTF reconstruction. Eighty per cent of the two groupsachieved top values. Fisher’s exact test analysis (P Z 0.5)showed that there was no statistically significant differenceamong the groups. Table 2 shows values for articulationtests. Most of the patients reached mild to moderate resultswith all consonants targeted. Only one case (an ALTF one)reached normal limits, 10% (ALTF) to 20% (FRFF) presenteda lower scale value. c2 trend test value (P Z 0.2) showedthat the trend is statistically not significant. Swallowingand oral transit time results were within normal limits forall reconstructed patients (Table 2). After rehabilitativecare all the patients were able to assume solid diet andthe oral transit time was 10 or less than 10 s. No residualfood was recorded in any case with rhinofibrolaryngoscopy(Table 2). No complications afflicted the donor site forALTF (Fig. 1). Two weeks was the mean time for completehealing of the thigh donor area. Suction drains wereremoved on Day 1 postoperatively. Mean time for healingfor the forearm donor site area was 3 weeks (rangingfrom 2 to 5 weeks). The grafted area healed without com-plication in 2 weeks (70%). One patient had an infection andhealed in 3 weeks, responding normally to topic antibiotics.
Table 2 Functional results from both reconstructedgroups
Speech intelligibilityscore
0 I II III
ALTF patients 1 9FRFF patients 2 8
Articulation score 0 I II III IVALTF patients 2 7 1FRFF patients 1 9
Diet score 0 I II III IVALTF patients 10FRFF patients 10
Dietoral transit time <10 s >10 sALTF patients 10FRFF patients 10
Residual food score Presence AbsenceALTF patients 10FRFF patients 10
Speech intelligibility scale: 3, no sound errors in continuousspeech; 2, speech is intelligible with some error; 1, speech is in-telligible with careful listening; 0, speech is unintelligible.Articulation scale: 4, within normal limits; 3, mild to moderate,all consonants targeted; 2, moderate to marked, consonantsand vowels both affected; 1, marked, uses adaptive compensa-tory articulations for all lingual; 0, severe, does not use effec-tive compensatory articulation.Diet results: swallowing scale: 4, solid diet; 3, semisolid diet; 2,semiliquid diet; 1, liquid diet; 0, tube feed.Oral transit time: normal transit time 10 s or less.Residual food presence or inhalation after food ingestion.
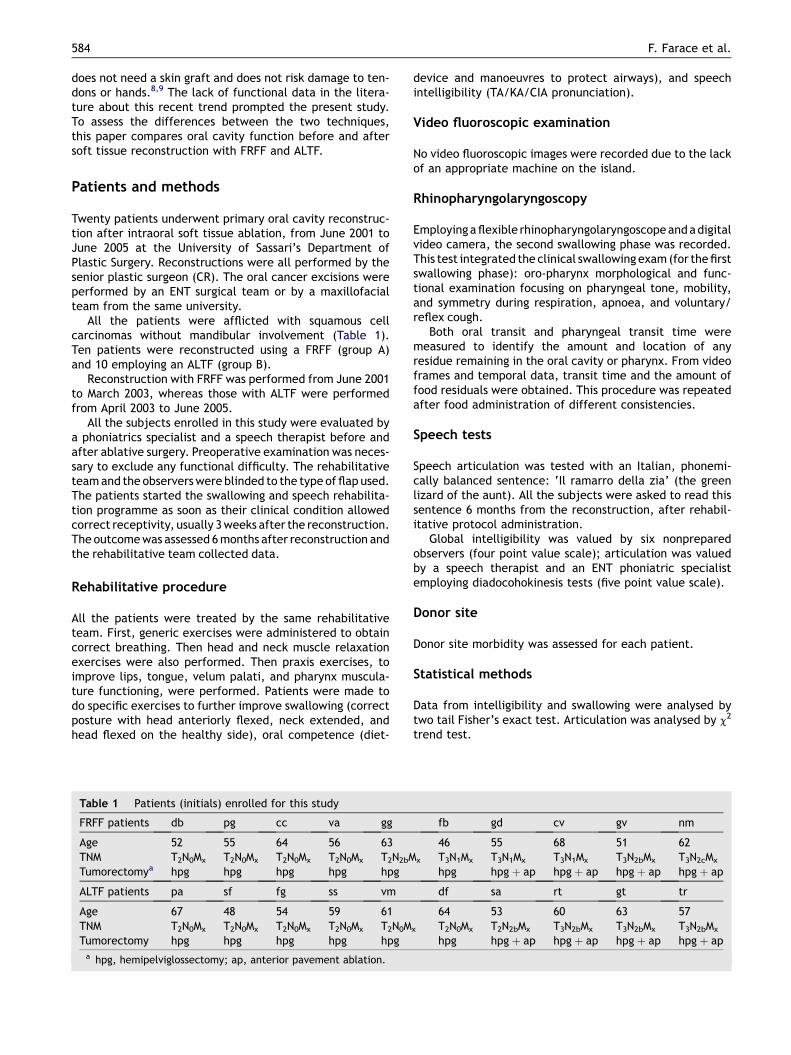
Three forearm donor sites healed for second intention inmore than 30% of the grafted area, probably due to intensetendon mobility (Fig. 2). One FRFF that was closed with anulnar fasciocutaneous VeY transposition flap developed hy-pertrophic scarring, maybe because of strong tension alongthe suture line (Fig. 3). No single patient complained aboutloss of hand stiffness. One subject suffered from superficialnumbness on the dorsal first metatarsal area, probably dueto a small radial superficial branch nerve injury.
Discussion
Difference in function between ALTF and FRFF groups wasnot statistically significant in our data. Swallowing andspeech seemed to have been restored in the same way afterhemi-tongue resection and reconstruction with ALTF orFRFF (Table 2). Intelligibility was judged as clearly compre-hensible in 90% of FRFF and 80% in ALTF cases by six nonpre-pared people (none of them was a team member).Articulation values were more than adequate in 80% ofthe groups and in one ALTF case, results were normal.
Figure 1 ALTF donor site: 6 months postoperative view;healing without hypertrophy or dehiscence.
Figure 2 FRFF donor site: 1 month postoperative view. Notethe split thickness skin graft double central necrotic area,probably related to tendon movement.

586 F. Farace et al.
Rhinopharyngolaryngoscopy, an alternative method tovideo fluoroscopic examination, presented absence ofresidual food, even in valleculae or pyriform fossae, inboth reconstructed series. Rhinopharyngolaryngoscopydoes not expose the patient to any further X-rays; it iseasily performed by trained hands, and the entire exami-nation is in the out-patient clinic by the same physician whousually does the follow up of patients.
Food aspiration or laryngeal penetration in both groupswas never observed and each patient enrolled in this studywas able to resume a solid diet.
In both microsurgically reconstructed patient series,there are no obvious functional differences that predisposea patient towards a particular surgical treatment. Similarly,ALTF and FRFF have comparable characteristics such as,soft and pliable tissues with a long pedicle and large calibrevessel allowing comfortable microanastomosis; they seemideally suited to provide intraoral lining. Not all intraoralsoft tissue defects are equal and hemiglossectomy patientsare perhaps not the most sensitive cases for comparing thepliability and thinness of the two types of flap. The ALTF issupposed to be thicker than FRFF but usually, the bodyadiposity in oral cancer patients is reduced. In this series,only one flap had to be thinned intraoperatively. Further-more, the ALTF may be thinned primarily or a few monthsafter surgery.10 Consequently, donor site risks and compli-cations were the only variables among the groups. Thesevariables may be used as indicators to make a surgicalchoice.
The distal third of the forearm may be subject tofunctional problems when mobile tendons are exposed,even if the paratenon is preserved or lateral skin edge hasbeen advanced to partially bury the brachioradialis tendonand radial nerve. Moreover, infection of the forearm donorsite graft, although uncommon, is dangerous, even leadingto a frozen hand.11 Immediate direct closure of the FRFFdonor site can be achieved by using an ulnar fasciocutane-ous VeY transposition flap.12 This flap allows better aes-thetic results and reduces donor site morbidity avoidingthe risk of infection or tendon adhesions.13 However, thistechnique is suitable only for intraoral defects smallerthan 6 � 4 cm and may lead to hypertrophic scarring.
Figure 3 FRFF donor site: 6 months postoperative view. Notethe hypertrophic scar because of an ulnar fasciocutaneous flapemployed to close the donor site.
Recently, some authors have shown that the ulnar arteryis dominant at the elbow, but after originating its collateralbranches, the radial artery becomes the dominant artery inthe distal forearm and, consequently, is the major source ofvascularization to the hand.5 Consequently, FRFF alwayssacrifices the major artery of the limb and leads to unat-tractive scars in the forearm region. This may producenot only objective complications like stiffness, pain ornumbness, but also subjective complaints such as bad cos-metic intolerance.14
Intraoral hair growth in unirradiated patients maycomplicate both flaps, especially in male patients.
The ALTF learning curve is undoubtedly longer than forthe FRFF, mainly because the intramuscular perforatordissection is more challenging. Even if in this small seriesno complications afflicted the ALTF donor site, quadricepsdysfunction, disto-lateral thigh anaesthesia/paraesthesiaand pain are all described as potential complicationsfollowing ALTF dissection. Nevertheless, when ALTF isemployed for intraoral lining, the donor site can be closedprimarily. ALTF elevation does not involve harvesting themain vessels of the thigh; the severity of donor sitedysfunction seems to be related to the degree of damageof the vastus lateralis muscle15 and data from large tosmaller ALTF series state that donor site morbidity islimited.16,17
Therefore, based on our functional data, experience,and literature on donor site morbidity, ALTF is consideredas the first choice in intraoral reconstruction.
References
1. Tsue TT, Desyatnikova SS, Delayiannis FWB, et al. Comparison ofcostand function in reconstructionof theposterior oral cavity andoropharynx. Arch Otolaryngol Head Neck Surg 1997;123:731e7.
2. Yang GF, Chen PJ, Gao YZ, et al. Forearm free skin transplan-tation. Natl Med J China 1981;61:139.
3. Soutar DS, Scheker LR, Tanner NS, et al. The radial forearmflap: a versatile method for intra-oral reconstruction. Br J PlastSurg 1983;36:1e8.
4. Soutar DS, McGregor IA. The radial forearm flap in intraoralreconstruction: the experience of 60 consecutive cases. PlastReconstr Surg 1986;78:1e8.
5. Haerle M, Hafner HM, Dietz K, et al. Vascular dominance in theforearm. Plast Reconstr Surg 2003;111:1891e8.
6. Wei FC, Jain V, Celik N, et al. Have we found an ideal soft-tissue flap? An experience with 672 anterolateral thigh flaps.Plast Reconstr Surg 2002;109:2219e26 [discussion 2227e30].
7. Nakayama B, Hyodo I, Hasegawa Y, et al. Role of the anterolat-eral thigh flap in head and neck reconstruction: advantages ofmoderate skin and subcutaneous thickness. J Reconstr Micro-surg 2002;18:141e6.
8. Chen Hung-chi, Tang Yueh-bih. Anterolateral thigh flap: anideal soft tissue flap. Clin Plast Surg 2003;30:383e401.
9. Huang CH, Chen HC, Huang YL, et al. Comparison of the radialforearm flap and the thinned anterolateral thigh cutaneousflap for reconstruction of tongue defects: an evaluation ofdonor-site morbidity. Plast Reconstr Surg 2004;114:1704e10.
10. Ross GL, Dunn R, Kirkpatrick J, et al. To thin or not to thin: theuse of the anterolateral thigh flap in the reconstruction ofintraoral defects. Br J Plast Surg 2003;56:409e13.
11. Hallock G. Complications of the free flap donor site from a com-munity hospital perspective. J Reconstr Microsurg 1991;7:331e4.

Free anterolateral thigh flap versus free forearm flap 587
12. Elliot D, Bardsley AF, Batchelor AG, et al. Direct closure of theradial forearm flap donor defect. Br J Plast Surg 1988;41:358e60.
13. Bardsley AF, Soutar DS, Elliot D, et al. Reducing morbidity inthe radial forearm flap donor site. Plast Reconstr Surg 1990;86:287e92 [discussion 293e4].
14. de Bree R, Hartley C, Smeele LE, et al. Evaluation of donor sitefunction and morbidity of the fasciocutaneous radial forearmflap. Laryngoscope 2004;114:1973e6.
15. Kimata Y, Uchiyama K, Ebihara S, et al. Anterolateral thigh flapdonor-site complications and morbidity. Plast Reconstr Surg2000;106:584e9.
16. Gedebou TM, Wei FC, Lin CH. Clinical experience of 1284 freeanterolateral thigh flaps. Handchir Mikrochir Plast Chir 2002;34:239e44.
17. Shieh SJ, Chiu HY, Yu JC, et al. Freeanterolateral thigh flap for re-construction of head and neck defects following cancer ablation.Plast Reconstr Surg 2000;105:2349e57 [discussion 2358e60].




















![HFM Free Flap Versus Fat Grafting[1]](https://img.dokumen.tips/doc/110x75/54f83fc94a7959fe478b459b/hfm-free-flap-versus-fat-grafting1.jpg)








