Embed Size (px)
Citation preview

Eur. Radiol. 4, 341-346 (1994) © Springer-Verlag 1994
European Radiology
Musculoskeletal radiology
Fracture healing: direct magnification versus conventional radiography T. M. L i n k 1 , T. K e s s l er 2, T. L a n g e 1 , J. O v e r b e c k 2, M. F i e b i c h 1 , P. E . Pe ters I
1 Department of Clinical Radiology, Westf~ilische Wilhelms-Universit~it, Albert-Schweitzer-Strasse 33, D-48129 Mttnster, Germany 2 Department of Traumatic and Hand Surgery, Wesff~ilische Wilhelms-Universitfit, Albert-Schweitzer-Strasse 33, D-48129 Mfinster,
Germany
Received 8 October 1993; Revision received 21 February 1994; Accepted 15 March 1994
I n t r o d u c t i o n
Modern orthopaedic and traumatological procedures such as Ilizarov distraction [1-3] require diagnostic methods for detecting callus formation at an early stage in order to monitor osseous union. Conventional radiol- ogy is not sensitive enough to demonstrate the minerali- sation processes in immature fracture callus. The de- monstration of early mineralisation, however, is of great value as an absolute indicator of progressing os- seous union [4]. The mineralisation of immature bone correlates with its structural stability; these changes in callus formation occur 4-6 weeks after fracture [4]. In recent years several techniques for assessment of frac- ture healing have been developed, including quantita- tive radiography [4] and CT [5-7]. Scintigraphy [8] has been used to monitor the metabolism of fracture heal- ing by fracture site activity and ultrasonography [1, 9] to detect as yet uncalcified new bone formation.
Direct MAgnification radiography (DIMA), using a newly developed microprocessor-controlled microfocal X-ray tube [10], together with CT, offers new possibili- ties for detecting mineralised callus at an early stage and thus monitoring fracture healing. The purpose of this study was to analyse its potentials in diagnosing fracture healing and its clinical implications as com- pared with conventional radiography.
Correspondence to: T. M. Link
M e t h o d s
Subjects
This prospective study was conducted between May 1992 and August 1993. Seventy-one patients (mean age 33 years) were examined with both conventional and magnification radiography. As 10 patients were exam- ined twice and 1 three times, altogether 83 radiographs were analysed. Patients referred for magnification radiography had undergone osteotomy or suffered a fracture 15-100 days prior to the examination (mean

342 T. M. Link et al.: Direct Magnification vs Conventional Radiography in Fracture Healing
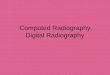
large source small focal spot size
ob!ect t
@ </ ~ ~ mia;~i~fieed r ~~ Fig. 1. Magnification geometry, showing increasing focal spot pe- numbra with magnification. Penumbra is reduced by a small focal spot size. SID, source-image distance; SOD, source-oNect dis- tance
54 days). Fixation was performed in 58 patients, includ- ing 26 with Ilizarov procedures. Reasons for referral were evaluation of osseous union (49/83), complica- tions of fracture healing (9/83) and detection of first cal- lus formations (15/83). Informed consent was obtained from all patients. Locations radiographed included the phalanx of the hand (34/83), tibia (13/83), metacarpal (10/83), scaphoid (9/83), radius (8/83), ulna (7/83), hu- merus (1/83) and metatarsal (1/83).
justed image). The other was subjected to filtering algo- rithms with unsharp masking (edge-enhanced image). Both images were required since edge-enhanced views provide excellent contrast of bone and soft tissue struc- tures but may produce so-called overswing artefacts in border areas of bone or metallic fixation with high steps in contrast fixation [16].
In the past the high radiation dose has been a major limiting factor of the magnification technique. In this study radiation dose was decreased by using computed radiography due to absence of reciprocity failure (long exposure times causing disproportionately less blacken- ing of films with conventional film-screen combina- tions) and the elimination of retakes resulting from ex- posure error. Additionally the detector dose was re- duced (1.25 ~Gy in the film plane) and the kVp values increased. Because of digital image processing contrast was not decreased by higher kVp. All of these steps re- sulted in a radiation dose, measured with a dosemeter (ionisation chamber, type 7733, PTW, Freiburg, Germa- ny), that was 1.35-fold higher in magnification radiogra- phy compared with the conventional technique.
Conventional radiography
For conventional radiography standard film-screen sys- tems (S = 100) were chosen. Focal spot size was 600 ~m in smaller objects and 1200 ~tm in knee and femur.
Magnification radiography
In direct magnification radiography the source-image distance is increased while maintaining or decreasing the source-object distance. Since this causes a magni- fied focal spot penumbra, a very small focal spot has to be used (Fig. 1) [10-13].
The radiographic unit is specially designed for direct magnification radiography in a clinical setting [14, 15]. The prototype (Microfox G10, Feinfocus Medical Sys- tems, Garbsen, Germany) is microprocessor-controlled and performs at variable focal spot sizes between 20 and 130 ~m. Magnification up to x 9 can be achieved. The micofocus X-ray tube is demountable, allowing easy replacement of filament and target. A two-stage pump system produces the operational vacuum.
The patients in our study were examined using 5-fold magnification. Focal spot size and kVp were chosen ac- cording to the region examined: hands and feet, 60 ~m and 50 kVp; lower leg and forearm, 80 ~m and 60 kVp; femur and humerus, 100 ~m and 70 kVp. Radiation dose was chosen to be equivalent to a S = 800 film-screen sys- tem, i.e. 1.25 ~Gy in the film plane. Average exposure time was 0.75 s and the average mAs value was 1.6.
For the imaging system computed radiography was used employing a storage phosphor technique (AC-1, Fuji, Tokyo). Each of the 83 radiographs was digitally processed and for each exposure two processed images were obtained. One image was preprogrammed to simu- late the characteristics of a conventional film (X-ray ad-
Analysis
Altogether 83 radiographs in conventional technique and the corresponding magnification radiographs were analysed. The findings were correlated with the pa- tients' follow-up studies, which served as a reference.
In the first part of our study we compared pairs of magnification and conventional radiographs. The addi- tional information obtained by DIMA was analysed. As an objective judgement the first detection of minera- lised callus formation was used. The osseous union was also evaluated. Clinical implications and complications of fracture healing were assessed.
In the second part of our study two experienced radiologists and two traumatologists were asked to eval- uate anatomical and pathological structures in all films. For statistical evaluation an "inter-observer analysis" of the 166 images was performed, classifying each of the anatomical and pathological structures into one of four grades. The significance of differences between in- dividual and pooled observer performance with the two methods was tested with the paired Wilcoxon test for small samples.
Results
The magnification technique proved superior to con- ventional radiography in 39 cases (47 %). Callus forma- tion could be delineated earlier and better in 26 cases

T. M. Link et al.: Direct Magnification vs Conventional Radiography in Fracture Healing 343
Fig.2a, l~. Conventional radiograph (optically magnified) a and magnification radiograph (edge- enhanced image) b of a 39-year old man with a limb lengthening procedure carried out 30 days previously (ring finger partially amputated in a chain-saw accident). The structure of the first mi- neralised callus is depicted with a higher resolu- tion in magnification radiography. Note also the differences in trabecular bone structure
Fig. 3 a-e. Magnification radiographs (edge-en- hanced images) 29 days after fracture a and 42 days after fracture b and a conventional radio- graph (optically magnified) 42 days after fracture e of a 25-year old man with fracture of the proxi- mal phalanx (fifth finger). In the magnification radiographs there is depiction of periosteal callus after 29 days (proximal end of fracture) and blur- ring of the fracture line due to endosteal callus formation after 42 days. By conventional radiog- raphy the first callus is delineated after 42 days
(Figs.2-4). Osseous un ion was eva lua ted with grea ter certainty, due to be t te r depic t ion of the t rabecular pat- tern and the new bone format ion , in 33 cases. Compl ica- t ions such as osteitis, de layed union, non-un ion and os- teonecrosis were assessed with grea te r cer ta inty in 8 cases. In I l izarov p rocedures D I M A p roved super ior in 54 % (14/26) of cases, which was due to de tec t ion of first mineral ised callus in 10 cases after an average t ime of 26 days.
In 3 (4 %) cases the magnif ica t ion rad iographs were eva lua ted as inferior and in 41 cases (49 %) as equal to the convent iona l radiographs.
Using D I M A first mineral ised callus fo rma t ion was d iagnosed after 15-49 days (average 31 days). In 50 % of cases per iosteal callus fo rma t ion (at the site of the per ios teum), in 33 % endostea l and in 17 % bo th types appea red first. Callus could be de tec ted 10-18 days ear- lier than with convent iona l radiography.

344 T. M. Link et al.: Direct Magnification vs Conventional Radiography in Fracture Healing
In those cases only the fractured areas were depicted and no information concerning alignment, angulation or rotation was obtained.
In the second part of our study an inter-observer analysis was performed in which two experienced radi- ologists and two trauma surgeons were asked to evalu- ate all 166 images and to classify anatomical and patho- logical structures into one of four grades. Anatomical structures were evaluated in areas of the radiographs where no pathological changes were detected. The qual- ity of depiction was classified as excellent ( = 4), good ( = 3), satisfactory ( = 2) or poor ( = 1). For soft tissue structures the average grading was 3.7 (SD 0.68) using DIMA and 2.5 (SD 0.71) in conventional radiographs (P < 0.012). In cortical bone average grading was 3.7 (SD 0.51) and 2.9 (SD 0:58) respectively (P < 0.012); for trabecular bone pattern 3.7 (SD 0.49) and 3.3 (SD 0.64) respectively (P < 0.012); and for depiction of bone adjacent to fracture or osteotomy 3.3 (SD 0.87) and 2.9 (SD 0.84) respectively (P < 0.012).
The evaluation of pathological structures was classi- fied as being detected with high certainty ( = 4), low cer- tainty (= 3), as uncertain (= 2) and definitely not de- tectable (= 1). In all structures assessed (osseous union, delineation of callus, endosteal and periosteal callus) DIMA proved to be superior. Average grading in evaluation of osseous union was 2.7 (SD 1.02) for magnification radiography and 2.2 (SD 0.91) for the conventional technique (P < 0.012), and average grad- ing in delineation of callus was 2.6 (SD 1.1) and 1.9 (SD 0.87) respectively (P < 0.012). Each of the four readers awarded better average gradings to the magnification radiographs; however, because of the small number of readers a better P value was statistically not possible. Edge-enhanced views were described as superior in 67 % of all magnification radiographs evaluated.
Fig.4a, b. Conventional radiograph (optically magnified) a and mag- nification radiograph (edge-enhanced im- age) b of the proximal tibia of a 20-year-old man with a limb lengthening procedure carried out 32 days previously. Minera- lised callus is shown only on the magnifica- tion radiograph
In 12 cases the DIMA findings entailed clinical con- sequences, such as changing distraction rates in limb lengthening techniques and continuous immobilisation or mobilisation.
In 56 cases DIMA alone was sufficient (smaller ob- jects, such as phalanx, metacarpal, metatarsal and car- pus), while in 37 cases conventional radiographs were still needed to image large bones (e. g. tibia, femur), since magnification reduced the field size significantly.
Discuss ion
Fracture healing is a complex process in which a number of events take place resulting in the re-formation of the bone necessary for structural stability [17-22]. In the first, inflammatory stage the accumulation of necrotic material (marrow, periosteum, adjacent soft tissue) in- cites an acute inflammatory response with associated vasodilatation, plasma exudation and infiltration by leu- cocytes. The second, reparative stage (after 3 weeks) en- tails invasion of fibroblasts from the adjacent soft tissue. The fibroblasts and osteoprogenitor cells from the peri- osteum or endosteum produce primary callus, i.e. im- mature fibrous bone. The primary callus mineralises and immobilises the fracture fragments; the mineralisa- tion corresponds to its stability [23]. In the third, remo- delling stage the immature fibrous bone is replaced by adult lamellar bone.
Conventional radiography is not very sensitive in the early diagnosis of callus formation in the reparative stage [23, 24]. With modern orthopaedic and surgical procedures, however, early detection of callus forma- tion is essential in order to monitor osseous union:

T. M. Link et al.: Direct Magnification vs Conventional Radiography in Fracture Healing
1) The high rates of complications such as osteomyeli- tis, non-union and refracture after plating have chang- ed the techniques in trauma surgery. Locked nailing and dynamic external monofixators that entail axial mi- cromovements and fracture haematoma are used more and more frequently. These techniques are less trauma- tising to soft tissue and promote callus formation [3].
2) The success of the Ilizarov distraction technique has resulted in a marked increase in the number of limb lengthening and limb straightening procedures perform- ed for the correction of short and deformed limbs [1, 2].
The success of these procedures can not be determined for many weeks, because of the limitations of plain radiographs in detecting small amounts of new bone for- mation that occur at the site of fracture or of distraction in the early stages of healing [1]. More sensitive meth- ods of monitoring new bone production are required to, for example, adjust the distraction rate to the callus formation process: slow bone formation requires a de- crease in distraction rate and vice versa.
Various techniques to image callus formation at an early stage have been developed:
1) Sonography [1, 9]: The first appearance of bone for- mation is seen sonographically after 1-3 weeks in Ilizar- ov limb lengthening procedures [1] as compared with 6- 24 weeks in conventional radiography. The problem is, however, that early mineralisation of callus, which cor- relates with its stability, can not be monitored [4].
2) CT [5-7]: By 3 weeks callus was visible with both CT and conventional radiography in an experimental frac- ture healing study but at 6 weeks a trabecular pattern was seen on plain films and not on CT [6]. Another study [7] found an earlier detection of callus by CT as compared with conventional radiography. Both studies agree that CT is a good method of determining osseous union in later stages of fracture healing. Due to arte- facts, however, CT cannot be performed in patients with standard fixations.
Direct magnification radiography (DIMA) has the potential to image early callus formation as demonstrat- ed in our study; it depicts the trabecular structure of the callus, which is linked to the stability of the bone [5].
In 47 % of films analysed DIMA proved superior to conventional radiography as regards detection of callus and evaluation of osseous union. Magnification radio- graphs are most useful in the early stages of fracture healing to detect mineralised callus (superior in 66 % of cases 3-5 weeks after fracture or osteotomy), while in later stages it can sometimes be difficult to deter- mine osseous union due to superimposition of large mi- neralised callus formations. In those cases other meth- ods such as CT are probably more useful.
Using DIMA mineralised callus was first seen 2- 6 weeks after fracture or osteotomy, while in conven- tional radiography it needed another 2-4 weeks to de- monstrate callus. Young et al. [1] detected first callus using conventional radiography 6-8 weeks after an Ili-
345
zarov procedure. We found DIMA useful in monitoring new bone formation in callus distraction to determine distraction rates.
Complications of fracture healing include osteitis, de- layed union and osteonecrosis. Early detection of those complications is difficult using conventional radiogra- phy [25]. In our study complications occurred in 6 cases (osteitis in 3, osteonecrosis in 1 and delayed union in 2 cases). DIMA detects erosive and proliferative bone changes at an early stage [13, 26-28]. In our study de- structive cortical bone lesions could be demonstrated only with magnification radiography in 2 cases.
All 166 radiographs were evaluated by two experi- enced radiologists and trauma surgeons and classified into one of four grades. In this inter-observer analysis DIMA proved superior in all the anatomical and patho- logical structures evaluated. Best results were obtained in evaluation of soft tissue structures and depiction of bone adjacent to fracture and osteotomy. Osseous un- ion and delineation of callus were assessed with higher certainty.
In addition to fracture healing, DIMA was found to be a valuable tool in other fields of traumatology, such as detection of fractures and evaluation of osteitis [13, 26]. Small fissures in the cortical bone or avulsion frac- tures can be depicted better than by conventional radi- ography, while due to superimposition there is usually no additional information in intramedullary fracture lines. The radiological signs in osteitis and osteomyeli- tis are proliferation and bone resorption, both of which can be demonstrated well in the early stages by DIMA. Erosion of the cortical white line in arthritis is seen ear- lier in magnification radiographs [28].
DIMA was used in conjunction with computed radi- ography. In conventional radiography the spatial resolu- tion of computed radiography is inferior to that of film- screen imaging systems. The resolution of computed radiography with magnification, however, equals that of conventional film-screen systems. The reason for this is that in DIMA (more than 5-fold magnification) the overall resolution is determined by the geometrical setting (focal spot size) and not so much by the imaging system [16]. Thus the advantages of computed radiogra- phy [29, 30], such as image processing (e.g. unsharp masking technique to obtain edge-enhanced films), re- duction of radiation dose and the possibility of digital communication and storage, can be used without de- creasing image resolution.
In conclusion, magnification radiography proved to be a valuable method of monitoring fracture healing. Compared with conventional radiography, callus forma- tion was detected earlier and osseous union could be evaluated with greater certainty. With a new microfocal X-ray tube magnification radiography can be used in day-to-day clinical work to predict fracture stability and determine the distraction rates in limb lengthening procedures.
Acknowledgement. We thank Patricia A.K. Set, Department of Radiology, University of Cambridge, UK for assistance with the manuscript.

346 T. M. Link et al.: Direct Magnification vs Conventional Radiography in Fracture Healing
References
1. Young JW, Kostrubiak IS, Resnik CS, Paley D (1990) Sono- graphic evaluation of bone production at the distraction site in Ilizarov limb-lengthening procedures. AJR 154:125-128
2. Giebel G (1993) Kallusdistraktion. In: Hierholzer G, Weller S (eds) Traumatologie aktuell, vol 5. Thieme, Stuttgart
3. Brug E, Winkler S (1991) Zuriick zur Kallusheilung durch dy- namisierbare Osteosyntheseverfahren. Radiologe 31:165-171
4. Aro HT, Wippermann BW, Hodgson SF, Wahner HW, Lewal- len DG, Chao EYS (1989) Prediction of properties of fracture callus by measurement of mineral density using micro-bone densitometry. J Bone Joint Surg [Am] 71:1020-1030
5. Braunstein EM, Golstein SA, Ku J, Smith R Matthews LS (1986) Computed tomography and plain radiography in experi- mental fracture healing. Skeletal Radiol 15:27-31
6. Schnarkowski R Weidenmaier W, Mutschler W, Arand M (1992) Erste Erfahrungen zur Quantifizierung der Frakturhei- lung mittels Computertomographie. R6ntgenpraxis 45: 380- 384
7. Nutz V, Uexkttll-Gt~ldenband V (1988) Computertomographi- sche Untersuchungen der Frakturheilung. Fortschr R6ntgenstr 149:396-401
8. Wallace AL, Strachan RK, Blane A, Best A, Hughes PF (1992) Quantitative early phase scintigraphy in the prediction of heal- ing tibial fractures. Skeletal Radiol 21:241-245
9. Hanneschlfiger G, Reschauer R (1990) Sonographische Ver- laufskontrolle der sekundfiren Frakturheilung. Fortschr R6nt- genstr 153:113-119
10. Takahashi S, Sakuma S (1975) Magnification radiography. Springer, Berlin Heidelberg New York
11. Zimmer EA (1953) Die praktische Anwendung und die Ergeb- nisse der radiologischen Vergr/3sserungstechnik. Fortschr R6ntgenstr 78:164-169
12. Rao GUV, Soong AL (1973) Physical characteristics of modern microfocus X-ray tubes. AJR 111:628-633
13. Sugiura Y (1958) Clinical application of enlargement radiogra- phy in orthopedic surgery:I. Nagoya J Med Sci 21:333-338
14. Gebureck P, Fredow G, Sperner W (1991) Anlagenkonzept ei- ner Mikrofokusr6hre ffir die klinische Anwendung. Radiologe 31:407-412
15. Kronholz H-L (1991) Direktradiographische Vergr6sserung und Strahlenexposition. Radiologe 31:413-417
16. Reuther G, Kronholz HL (1991) Direktradiographische Ver- gr6sserung in Kombination mit digitaler Radiographie ftir die Skelettdiagnostik. (Direct radiological magnification with digi- tal radiography for skeletal imaging.) Radiologe 31:424-429
17. Miiller ME, Allg6wer M, Schneider R, Willenegger H (t977) Manual der Osteosynthese. Springer, Berlin Heidelberg New York
18. McKibbin B (1978) The biology of fracture healing in long bones. J Bone Joint Surg [Br] 60:150-162
19. Weissman BNW, Sledge CB (i986) Orthopedic radiology. Saunders, Philadelphia
20. Aegerter E, Kirkpatrick JA (1975) The repair of fractures. In: Orthopedic disease: physiology, pathology, radiology. Saun- ders, Philadelphia, chap 8
21. Heppenstall RB (1980) Fracture treatment and healing. Saun- ders, Philadelphia
22. McClements R Templeton RW, Pritchard JJ (1961) Repair of a bone gap. J Ana 95:616
23. Nicholls PJ, Berg E, Bliven FE, Kling M (1979) X-ray diagnosis of healing fractures in rabbits. Clin Orthop 142:234-236
24. Miiller-Miny H, Erlemann R, Baranowski D, Roos N, Peters PE (1991) Radiologische Beurteilung von Osteosynthesen. Ra- diologe 31:179-185
25. Rosenthal H, Freier W, Galanski W (1991) Komplikationen der Osteosynthese im R6ntgenbild. Radiologe 31:186-191
26. Freyschmidt J, Fr{3hlich H, Rittmeyer K, Behrens S (1976) Neue Aspekte zur Vergr6sserungstechnik in der chirurgischen R6ntgendiagnostik. Arch Orthop Unfall-Chir 84:67-76
27. Matsuda T (1955) Evaluation of direct enlargement radiogra- phy applied to the examination of the bone structure of adults. Studies on enlargement radiography. Nippon Acta Radiol 14: 767-774
28. Link TM, Gaubitz M, Lenzen H, Mtiller-Miny H, Schneider M, Peters PE (1993) Klinische Anwendung der Vergr6sserungsra- diographie bei rheumatologischen Fragestellungen. Z Rheu- matol 52:161-166
29. Tateno Y, Iinuma T, Takano M (1987) Computed radiography. Springer, Berlin Heidelberg New York
30. Lehmann KJ, Busch H-R Sommer A, Georgi W (1991) Die Wertigkeit digitaler Bildaufnahmeverfahren bei der Skelettdia- gnostik. Fortschr R6ntgenstr 154:286-291